
Abstract
Objectives
Our objective is to describe a novel operative technique for localization of parotid sialolithiasis, demonstrate the feasibility of the technique, and discuss its indications.
Study Design
Prospective study.
Setting
Tertiary-level academic center.
Subjects and Methods
Patients with symptomatic parotid sialolithiasis who had failed prior sialendoscopic extraction underwent ultrasound needle localization and open sialolithotomy. Data were prospectively collected. Independent variables included size of and location of sialoliths.
Results
Eleven patients were treated using transcutaneous ultrasound-guided needle placement and injection of methylene blue prior to external sialolithotomy. Follow-up ranged from 6 to 12 months. Ten (91.9%) patients had stones within the proximal one-third of the ductal lumen, and 1 (9.1%) had stones present within both the proximal one-third and middle one-third of the ductal lumen. The average surgical time was 53 ± 10.8 minutes. The average sialolith length was 7.6 ± 2 mm. The average sialolith width was 6 ± 1.9 mm. All 11 (100%) cases were successful for stone retrieval. Ten (91%) patients had complete symptom resolution, and 1 (9.1%) patient had partial resolution of symptoms. No patients had major complications. Three (27.3%) patients had minor complications.
Conclusion
After failing a purely endoscopic approach, sialoliths of the parotid gland pose a problem for precise localization and treatment. Ultrasound has been demonstrated to be reliable for identifying sialoliths. We propose a novel technique and assert that ultrasound-guided needle localization is a reliable aid to effective external parotid sialolithotomy, especially for larger stones >4 mm that are not amenable to sialendoscopic retrieval.
Sialolithiasis is a rare disease of unknown etiology that occurs in 1 per 10,000 to 1 per 300,000. 1 Parotid sialolithiasis accounts for 10% to 20% of all cases of sialolithiasis involving the head and neck, and diagnosis can be challenging. 2 Recently, sialendoscopy has been used as a diagnostic and therapeutic tool in the management of parotid sialolithiasis.3-10 It has the distinct ability to directly visualize parotid stones and, if amenable, extract the offending sialolith through a purely endoscopic approach. Sialendoscopy, however, is limited by its ability to diagnose and treat all parotid stones, since it is unable to effectively treat stones impacted in the secondary or tertiary ductal system. Sialendoscopy is currently limited in its ability to treat most sialoliths greater than 3 to 4 mm in a purely endoscopic fashion. 1
Modalities such as ultrasound, conventional x-ray, sialography, and computed tomography (CT) imaging have all been used with variable success to help aid identification of parotid sialolithiasis.1,11-15 Ultrasound has been used by myriad other medical specialties to not only visualize but also localize and biopsy accessible masses. Otolaryngologists have been relatively reticent about adapting this technology, although many of the disease processes that we treat are transcutaneously accessible.
In this article, we present ultrasound-guided needle localization of parotid sialolithiasis as a novel technique for the diagnosis and treatment of parotid stones that are not amenable to pure endoscopic extraction.
Methods
From August 2009 to January 2012, patients with symptomatic parotid swelling were followed and a prospective database was maintained. Approval was obtained through the George Washington University Institutional Review Board. Patients with parotid stones visualized on ultrasound examination were identified and diagnostic sialendoscopy was performed in the office under local anesthesia. An attempt was made to treat the condition using a purely endoscopic approach. Those patients who failed sialendoscopic treatment underwent ultrasound needle localization and open parotid sialolithotomy in a tertiary-level hospital setting using the technique by the senior author (A.S.J.) as described below.
Description of the Technique
The patient is intubated using a short-acting paralytic agent. A facial nerve monitor (Medtronic, Minneapolis, Minnesota) is then placed into the lower lip and upper cheek to monitor the lower division of the facial nerve, and the proper placement is confirmed. Ultrasound of the parotid gland is typically performed in a transverse axis, and the offending sialolith is visualized. At that point, a 3-mL syringe with 1 mL of methylene blue and a 23- or 25-gauge needle is used to localize the stone using ultrasound guidance ( Figure 1 ). The position of the stone is confirmed by direct palpation using the tip of the needle and the stone. Methylene blue is then injected slowly as the needle is withdrawn. Proper identification of the stone is again confirmed by visualizing methylene blue at the parotid papilla intraorally.

Short-axis ultrasound-guided localization technique for identification of parotid sialolith with methylene blue.
At that point, the patient is prepped and draped for open surgery. A modified Blair incision is commonly used for exposure. Sub–superficial musculoaponeurotic system (SMAS) flaps are raised and the parotidomasseteric fascia is then exposed. The location of the stone is suggested by the focus of methylene blue (which usually measures 5 mm), and intraparotid dissection is performed ( Figure 2 ). Depending on the location of the stone, the buccal branch of the facial nerve is usually encountered and bluntly dissected. The position of the Stensen’s duct is then identified as a punctate area of methylene blue injection, and incision through the duct is then performed in the linear/oblique axis of the duct. Ultrasound may be performed at this step to confirm the position of the sialolith, although this is not usually necessary.

Appearance of the surgical field after lifting a sub–superficial musculoaponeurotic system skin flap. After an effective injection, there is a pinpoint mark just over the location of the calculus.
The stone (often stained blue) is then delivered ( Figure 3 ). The Stensen’s duct is usually stented using a 6Fr infant feeding tube over a vascular guide wire placed through the dochotomy ( Figure 4 ). Ultrasound is performed again to confirm the absence of fragmented sialoliths. The duct is closed using a running 5-0 or 6-0 vascular suture, and the wound is closed in layers. The stent is sutured in place intraorally and removed 4 weeks postoperatively.
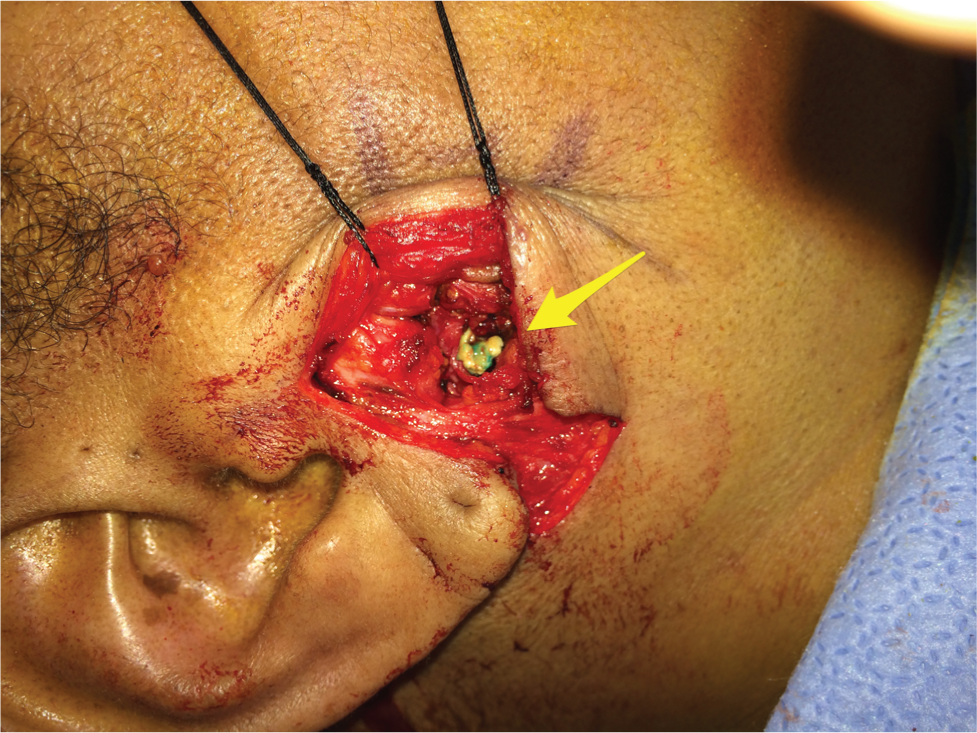
Minimal transparotid dissection for delivery of the calculus. Calculus marked with yellow arrow.

Guide wire is passed through the surgical dochotomy through the parotid papilla intraorally. The stent is then passed over the guide wire through the dochotomy into the mouth. Guide wire and stent marked with red and yellow arrows, respectively.
Patients were then followed up for a minimum period of 6 months, and outcome data were tabulated. Primary outcome measure was successful delivery of stone. Secondary outcomes included symptom resolution, presence of infection, ductal stenosis, loss of glandular function, and facial nerve paralysis. Independent variables included size and location of sialoliths.
Results
Between August 2009 and August 2012, a total of 36 patients with parotid stones were treated at the George Washington University. Eleven patients underwent transcutaneous ultrasound-guided needle placement and injection of methylene blue prior to external sialolithotomy in the operating room.
The mean age was 47.2 ± 16.1 (range, 22-72) years. Of the 11 patients, 6 (54.5%) were male, and 5 (45.5%) were female. The mean symptom duration was 33.1 (range, 1-86) months. The presenting symptoms were pain (n = 9 [81.8%]), swelling (n = 10 [90.9%]), discharge (n = 6 [54.5%]), periprandial symptoms (n = 6 [54.5%]), and xerostomia (n = 1 [9.1%]). Additional factors were antibiotic usage (n = 8 [72.7%]), smoking (n = 6 [54.5%]), occasional caffeine consumption (defined as 1-2 cups daily) (n = 5 [45.5%]), moderate caffeine consumption (3-4 cups daily) (n = 5, [45.5%]), and heavy caffeine consumption (>5 cups daily) (n = 1 [9.1%]) in our patient cohort ( Table 1 ).
Patient Demographics and Symptoms. a
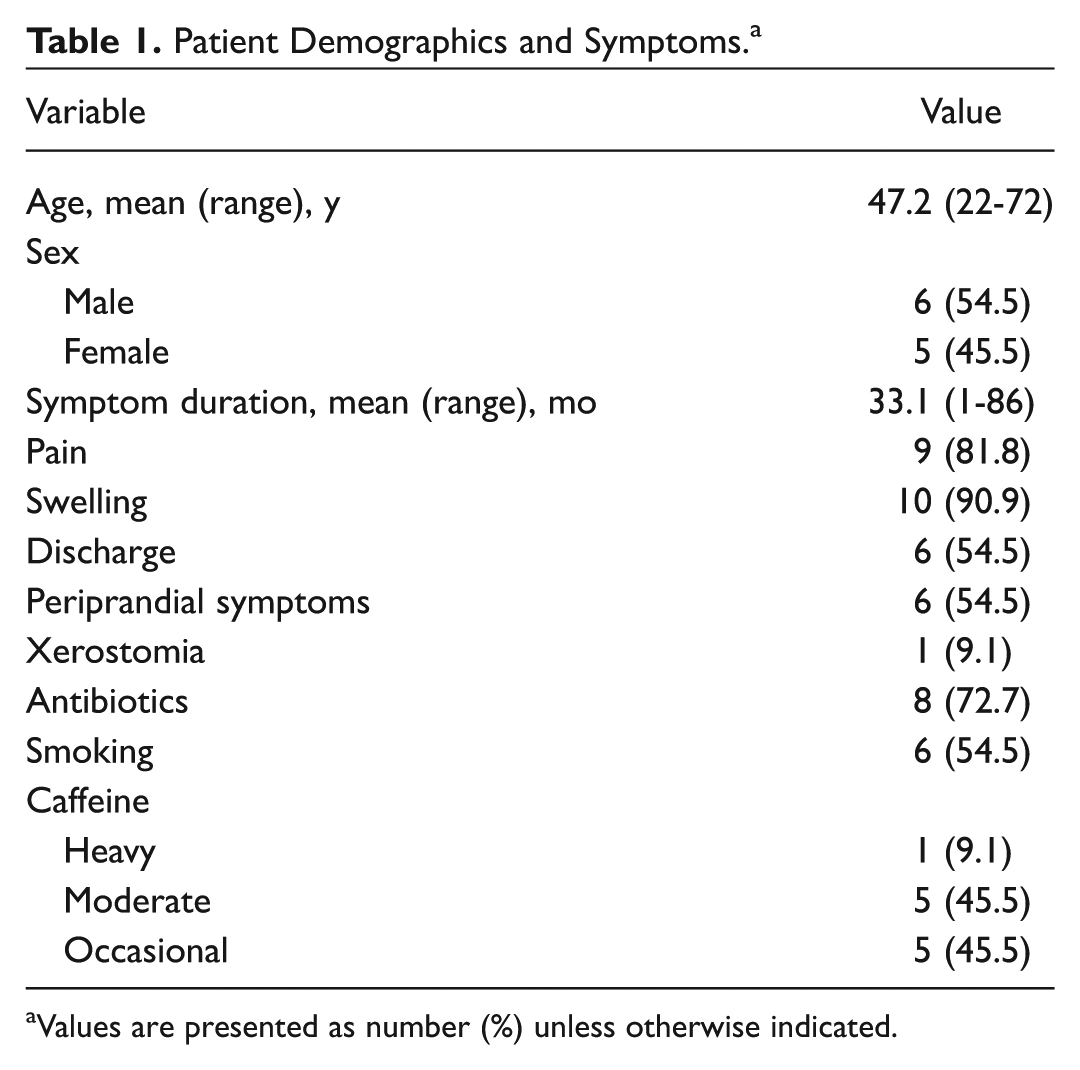
Values are presented as number (%) unless otherwise indicated.
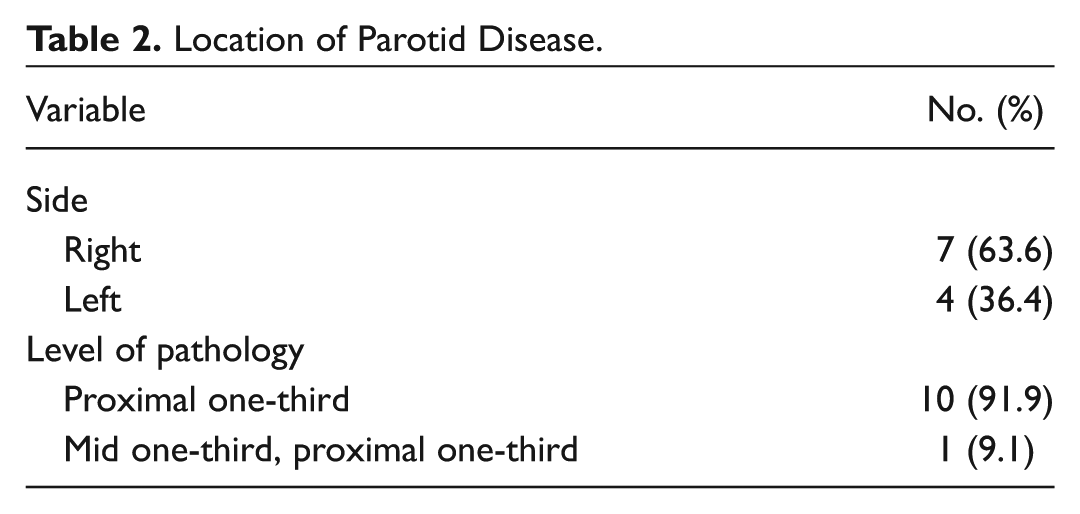
After undergoing ultrasound detection within the office setting, it was determined that 7 (63.6%) patients had right-sided parotid disease and 4 (36.4%) patients had left-sided parotid disease. Stones were defined as being in the distal one-third of the duct if distal to the anterior border of the masseter, middle one-third if between the anterior border of the masseter and the hilum, and proximal one-third if located proximal to the hilum in the secondary or tertiary ducts. Most (10/11 [91.9%]) had stones located in the proximal one-third of the ductal system, and 1 (9.1%) had stones within both the proximal one-third and middle one-third of the ductal lumen ( Table 2 ). In 8 of 11 (72.7%) patients, the calculi could not be visualized with sialendoscopy and the diagnosis was simply suggested by mucopus emanating from the secondary or tertiary ducts ( Figure 5 ). The remainder of the stones (3/11 [27.3%]) were visualized endoscopically but could not be extracted due to increased size and impaction.
Location of Parotid Disease.
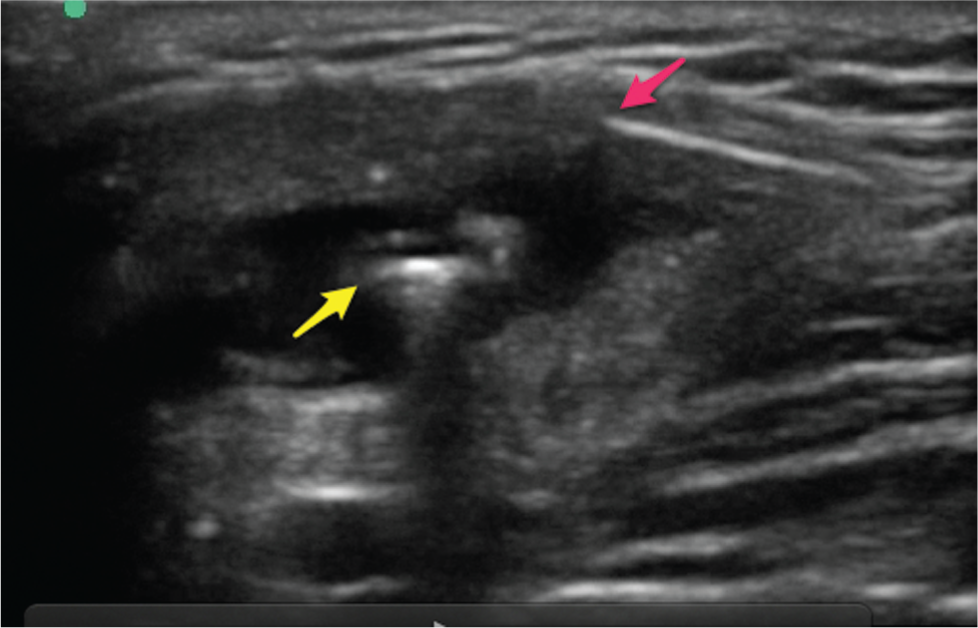
Ultrasound view of the right parotid gland. Sialendoscopy is being performed concomitantly. The stone is impacted in a tertiary duct and cannot be visualized. Tip of the scope marked with red arrow and stone marked with yellow arrow.
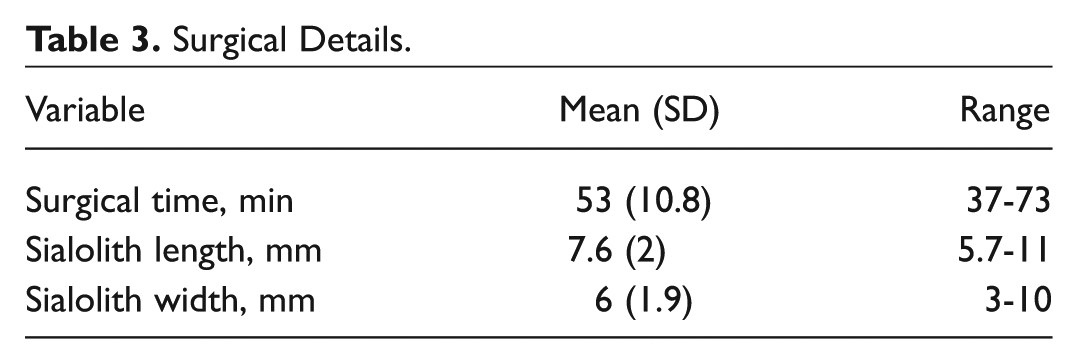
After the stones were localized using ultrasound in the operating room, patients underwent external sialolithotomy with gland and facial nerve preservation. The average surgical time was 53 ± 10.8 (range, 37-73) minutes. The average sialolith length was 7.6 ± 2 (range, 5.7-11) mm. The average sialolith width was 6 ± 1.9 (range, 3-10) mm. Stents were placed in 11 (100%) patients. Ten (91.9%) stones were irregularly shaped, and 1 (9.1%) stone was oval shaped ( Table 3 ).
Surgical Details.
Postoperative outcomes and long-term follow-up results were obtained. Average follow-up was at 8.9 ± 2.6 (range, 6-14) months. All 11 (100%) cases were successful for stone retrieval. Ten (91.%) patients had complete symptom resolution, and 1 (9.1%) patient had partial resolution of symptoms. No patients had major complications, defined as buccal facial nerve paralysis, loss of glandular function, and major ductal perforation. Three (27.3%) patients had evidence of minor complications defined as postoperative infection, sialoceles, and minor ductal perforation; 1 patient had minor ductal perforation that developed into a salivary fistula that resolved with pressure dressings, and 2 patients had sialoceles that resolved ( Table 4 ). No patients had salvage parotidectomy.
Outcomes and Complications.
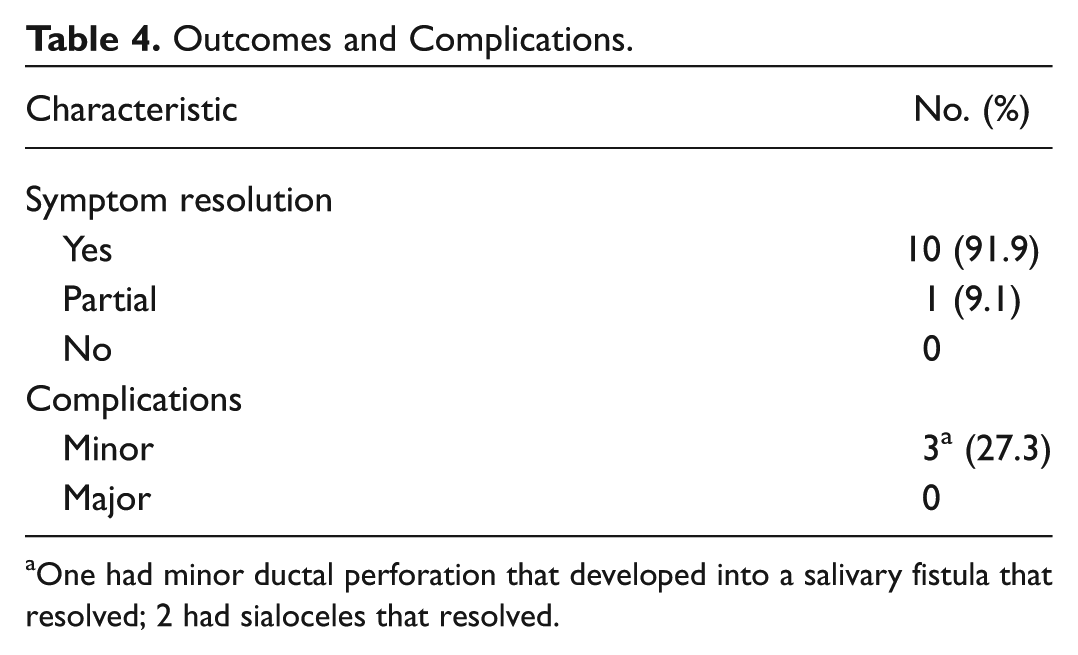
One had minor ductal perforation that developed into a salivary fistula that resolved; 2 had sialoceles that resolved.
Discussion
Parotid sialolithiasis accounts for 10% to 20% of salivary gland stones. 2 Diagnosis can be challenging for a variety of reasons. Modalities such as ultrasound, conventional x-ray, sialography, and CT scan have been used for the diagnosis of parotid sialolithiasis.1,11-15 Ultrasound has been used successfully in various specialties for transcutaneous evaluation of disease processes, and it has been proven effective for the diagnosis of parotid stones.11-13 Recent studies demonstrate a sensitivity rate of 94% and specificity of 100% for the detection of parotid sialoliths.11,13
With the recent advent of micro-instrumentation, sialendoscopy has been successfully implemented as a diagnostic and therapeutic tool for the diagnosis and management of parotid stones. Most would currently consider it the gold standard for the diagnosis of parotid sialolithiasis. Purely endoscopic treatment, however, can be limited by factors, including stone size, shape, orientation, and location of ductal pathology.1,16
In particular, sialendoscopy is limited by its ability to diagnose and treatment proximally located stones, since it is unable to effectively visualize those sialoliths impacted in the secondary or tertiary ductal system. 16 Although the percentage of stones located proximally has not been specifically addressed in the literature, our cohort of patients indicated this principle since 10 of 11 (91.9%) patients had proximally located stones and 1 of 11 (9.1%) had both proximal and middle third calculi that were not amenable to pure sialendoscopic extraction. In addition, sialendoscopy is limited in its ability to treat sialoliths greater than 3 to 4 mm through a purely endoscopic technique.1,16 Sialendoscopy is able to treat stones up to 3 mm with a 97% success rate, a value that dramatically decreases to 35% for stones greater than 3 mm. 7
These limitations of pure endoscopic extraction have encouraged others to attempt combined approaches.5,8,17 These so-called combined approaches have gained popularity for the treatment of large parotid sialoliths and involve localization of the stone with a sialendoscope as an aid during external sialolithotomy. The technique is highly reliable and effective for calculi located in the distal third, middle third, and immediately near the hilum of the parotid ductal system.
In the United Kingdom, Overton and colleagues 8 described 55 patients who underwent endoscopic-guidance localization of stones and surgical parotid sialolithectomy through an extraoral approach with subsequent ductal reconstruction to preserve glandular function. Of the patients available for follow-up, 70% were completely asymptomatic and 28% had mild residual symptoms.
Similarly, Karavidas and colleagues 5 published a 7-year prospective study in which 69 patients underwent minimally invasive surgery through a preauricular or direct transcutaneous approach after endoscopic transillumination localized the stones. Results indicated 99% complete removal of the identified stones and only 5% persistent symptomatic patients. Although the combined approaches have been successful for larger stones not amenable through pure sialendoscopic extraction, they are limited by the principle that very proximally located stones are not effectively visualized by the sialendoscope.
For example, after failing sialendoscopic treatment either due to impaction or inadequate visualization, our cohort of patients underwent successful treatment with ultrasound-guided needle localization and open parotid sialolithotomy. Diagnostic sialendoscopies were performed under local anesthesia in the office in all patients to effectively examine calculi and preoperatively counsel patients as to the approach. Sialendoscopic delivery was attempted in all cases, since we have had some limited success with removal of thin 1-cm stones in the main duct. We do not always use size as an absolute indicator for success of removal.
In our cohort, 11 (100%) patients had at least 1 stone present within the proximal one-third of the ductal lumen. One patient had stones in both the middle one-third and proximal one-third of the ductal system. The average sialolith length and width were 7.6 mm and 6 mm, respectively. We were able to visualize the sialoliths during sialendoscopy in 3 of 11 (27%) patients but were not able to treat them using a purely endoscopic technique. In the remainder of cases, calculi were suggested by mucopus emanating from a tertiary duct ( Figure 5 ).
Operative times were reasonable, averaging 53 (range, 37-73) minutes. A facial nerve monitor (Medtronic) was used in all cases. There were no major complications intraoperatively. Three patients (27.3%) had minor complications that included 1 through-and-through dochotomy that developed into a fistula and resolved with pressure dressings. Two patients developed sialoceles that resolved. There were no cases of temporary or permanent facial nerve paralysis. It has been our experience that there is a significant amount of functional redundancy in the distribution of the buccal branch of the facial nerve. Even with close nerve dissection, or with activity of the facial nerve monitor during dissection, we have not found any appreciable degree of facial dysfunction using this technique.
All stones were delivered successfully using ultrasound guidance. Average follow-up was between 6 and 14 months. Ten (91.%) patients had complete symptom resolution, and 1 (9.1%) patient had partial resolution of symptoms, which suggests that larger and proximally located stones that are not amenable to pure sialendoscopic retrieval may be effectively extracted through this technique. Furthermore, since 10 (91.9%) stones were irregularly shaped, the results suggest that shape and orientation of stones within the ductal lumen—factors that affect endoscopic extraction—do not play a significant role in stone extraction through this method.
Some advantages over a combined approach include the avoidance of additional instrumentation, which can obscure the surgical field. Sialendoscopy requires the use of additional equipment and personnel, which can be a limiting factor for some surgeons without access to these resources. Maintenance of sterility using ultrasound localization until the final portion of the case (sialodochotomy) may theoretically reduce the number of postoperative infections.
Our technique offers the ability to intraoperatively reassess the presence of residual stones without obscuring the surgeons’ view during open sialolithotomy, an important surgical consideration. For example, once detected sialoliths are removed, the sub-SMAS flap is laid back down and ultrasound is used to assess if any residual or previously unidentified stones are present. If any stones are identified, the sub-SMAS flap is reelevated and stones are retrieved using an identical technique. In our cohort of patients, 1 (9.1%) patient had a residual stone noted intraoperatively after external sialolithotomy and was successfully treated. Theoretically, intraoperative reassessment of residual stones should increase the efficacy of open sialolithotomy by decreasing the potential for both postoperative residual symptoms and number of unsuccessful cases.
The technique is safe and complication rates are low and acceptable, but there are some drawbacks. The technique is user dependent, and advanced training in head and neck ultrasound is a prerequisite. Stones that are small (1 mm) or mobile may be missed during ultrasound examination. In addition, there is a learning curve to injecting stones with methylene blue, since a forceful injection can diffuse into surrounding tissues. It is imperative to use a small volume of (0.2-0.3 mL) of methylene blue and inject lightly while removing the needle and syringe to prevent diffusion.
Unlike sialendoscopy-guided open sialolithotomy (combined approach), there is no ability to fix the position of the offending calculus during the surgery. During sialendoscopy, the stone can be trapped in the wire basket, preventing proximal migration of the sialolith during external sialolithotomy. This can be a problem, since the proximal ductal system can dilate significantly behind an obstructed sialolith, and the calculus can retrograde migrate into the proximal sac, making extraction difficult. We have encountered this issue during surgery and now control the position of the stone using transductal needle puncture proximal and prior to the dochotomy. This is typically performed with ultrasound in the parotid bed, with the SMAS flap retracted anteriorly. The needle can be placed proximal to the dochotomy into the parotid tissue and left in place to prevent retrograde migration. Other techniques that have helped us deal with this particular situation include forceful saline irrigation through the dochotomy to expel the calculus.
Conclusion
After failing a purely endoscopic approach, sialoliths of the parotid gland pose a problem for precise localization and treatment. Ultrasound has been demonstrated to be reliable for identifying sialoliths. We propose a novel technique and assert that ultrasound-guided needle localization is a reliable aid to effective external parotid sialolithotomy, especially for proximally located and larger stones (>3-4 mm) that are not amenable to retrieval through either a purely endoscopic or combined approach. The technique should be used in the armamentarium to treat parotid sialoliths.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.