
Abstract

Introduction
Multiple variations of temporomandibular (TMJ) joint dislocation have been described, with anterior dislocation the most common. 1 Anterior dislocation occurs when the mandibular condyle becomes trapped anterior to and slightly above the articular eminence. This dislocation may occur unilaterally or bilaterally during any type of extreme mouth-opening activity. 1 The jaw muscles involved in TMJ dislocation include the masseter, temporalis, and medial (internal) pterygoid, which close the jaw, and the lateral (external) pterygoid, which relaxes or opens the jaw.
After TMJ dislocation, the individual senses malocclusion, difficulty talking, inability to completely close the mouth, and pain.
While spontaneous reduction can occur, it is commonly necessary to manually reduce the dislocation using several described techniques.1-3 Reduction is often difficult due to associated muscle spasm. The use of muscle relaxants, sedation, and general anesthetics is common.
I describe a new technique of intramuscular temporomandibular joint reduction (iTMJ reduction) where anesthetic is externally injected into the pterygoid muscles to relax the associated muscle spasm and facilitate easier manual reduction.
Case Report
A 67-year-old male began having bilateral TMJ dislocations in the 1970s.
These occurred 3 to 5 times a year and often required sedation techniques for reduction.
The patient presented 3 hours after a yawn resulted in bilateral TMJ dislocation. He stated that most past dislocations had occurred with a yawn-type motion. The patient had no history of TMJ crepitance, orthodontia, or trauma, and the surgical and medical history were noncontributory. The physical exam was significant for an open bite with inability to close the jaw bilaterally.
An informed consent was obtained. The right and left coronoid notches were palpated bilaterally. An alcohol skin cleansing was performed on the submalar eminence skin bilaterally. Three milliliters of plain 1% lidocaine was drawn into a syringe with a 1.5 inch 27 gauge needle. Through the skin overlying the right coronoid notch the 1.5 inch needle was fully inserted at a downward angle of approximately 45° in a lateral to medial direction and at an angle of approximately 45° in an anterior to posterior direction ( Figures 1 and 2 ) into the body of the right medial pterygoid muscle. Aspiration was done to assure that the internal maxillary artery had not been punctured. Then the 3 ml of 1% lidocaine was slowly injected, anesthetizing the muscle. The procedure was repeated on the left side to anesthetize the left medial pterygoid muscle. Two minutes were allowed to elapse. Standard Hippocratic technique using gloved hands was then used to easily reduce the TMJ. A Barton dressing was placed to prevent immediate recurrent dislocation and left in position for 3 hours. The patient tolerated the procedure well.
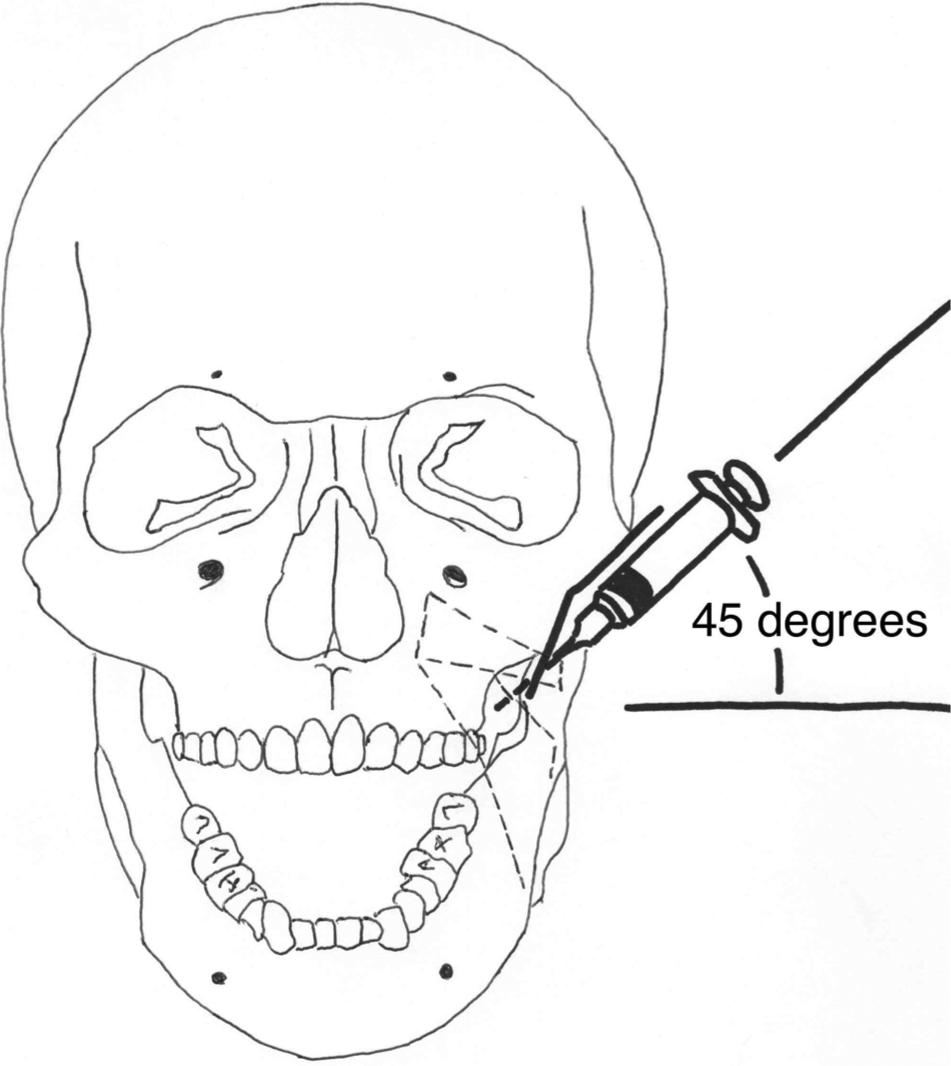
Insertion of needle for anesthesia of medial pterygoid muscle for intramuscular temporomandibular joint reduction (iTMJ) reduction—anterior view.
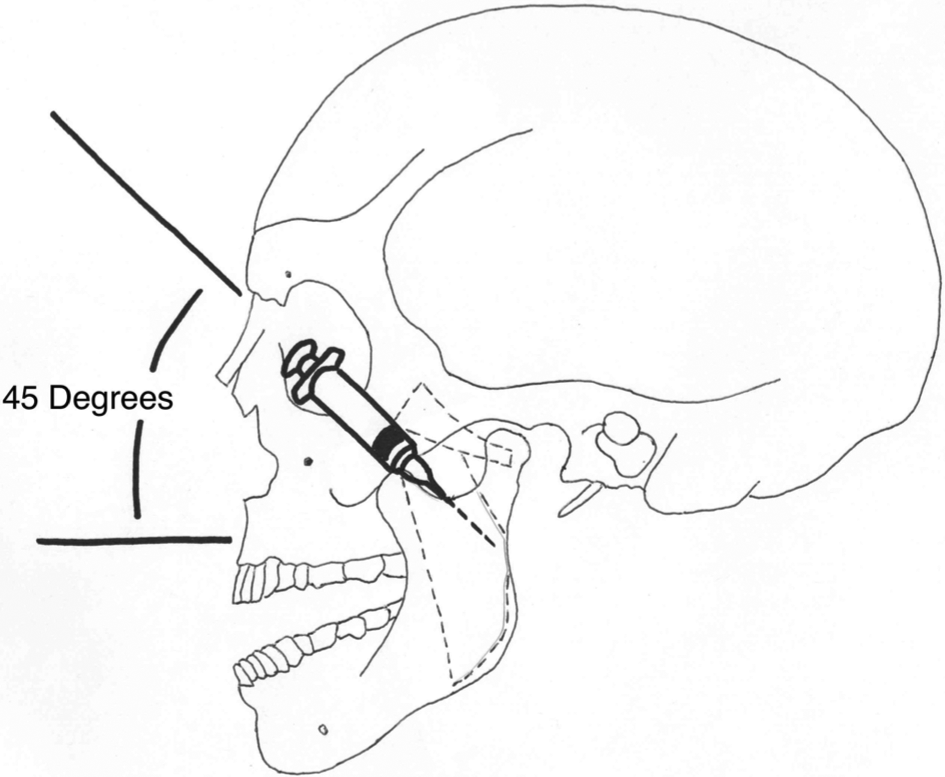
Insertion of needle for anesthesia of medial pterygoid muscle for intramuscular temporomandibular joint reduction (iTMJ) reduction—lateral view.
Discussion
Spasmodic contraction of the muscles of mastication prevents the spontaneous reduction of the dislocated temporomandibular joint.1,2 Variations of the classic Hippocratic method of reduction have been developed and are referenced by Babatunde 1 : the wrist-pivot technique, the combined ipsilateral staggering technique, the extra-oral technique, and the gag reflex procedure.
If simple reduction is initially unsuccessful at overcoming the spasmodic contraction of the muscles of mastication, the addition of anxiolytics, muscle relaxants, conscious sedation, and general anesthesia may be used in an attempt to reduce the dislocation. Local anesthesia to the temporal and masseter muscles is referenced by Babatunde, as is the progression to more aggressive techniques. 1 Anesthetic and surgical progression can place ill or elderly patients at increasing risk, so the most conservative reduction technique is always preferred.
I describe for the first time a technique whereby the powerful and spasmodically contracted pterygoid muscles are directly anesthetized and relaxed, thereby facilitating minimally invasive reduction of the anterior dislocation of the mandible. The author has utilized this iTMJ technique successfully in multiple cases. The iTMJ technique reduces the force often needed to reduce the dislocated joint and may stop the step-by-step progression to more dangerous and invasive methods of reduction.
The potential limitations of this iTMJ technique are that the angle of needle insertion and depth of insertion for application of the 1% lidocaine intramuscular injection was estimated and have not been anatomically studied to determine optimum angle or depth. The author thanks the Group Health Research Institute Institutional Review Board for their approving review manuscript.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.