
Abstract
Objective
Recently, a novel hydroxyapatite-coated concave bone-anchored hearing device abutment was introduced, the first designed specifically to improve outcomes in soft-tissue preservation osseointegrated hearing implant surgery. We sought to evaluate our early experience with this abutment.
Study Design
A single-center case series with planned data collection including patient-reported outcomes.
Setting
Tertiary referral center.
Subjects and Methods
The first 30 consecutive patients undergoing osseointegrated hearing implant surgery using the Cochlear DermaLock (BA400) abutment at our institution (February-September 2013) were studied. Follow-up was for a minimum of 6 months. The following data were collected: operative duration; wound healing; postoperative complications, chiefly soft-tissue reactions graded by Holger’s classification; and postintervention patient-perceived health-related quality of life, as assessed by the Glasgow Benefit Inventory (GBI).
Results
The mean operating time was 16 minutes (range, 9-22 minutes). Favorable and rapid wound healing was observed in all cases. Three patients (10%) reported transient periabutment paraesthesia. Four patients (13.3%) suffered adverse soft-tissue reactions, all of which were successfully managed conservatively and graded as follows: Holger’s grade 1 (n = 2), 2 (n = 1), and 3 (n = 1). Respective overall general health, social support, and physical health GBI mean scores were +38 (95% confidence interval [CI], 31 to 45), +51 (95% CI, 42 to 60), +19 (95% CI, 8 to 30), and +8 (95% CI, –1 to 17).
Conclusion
Our preliminary clinical and patient-reported outcomes support soft-tissue preservation surgery and indicate that the technology on which the Cochlear DermaLock (BA400) abutment is based may enhance soft-tissue outcomes in this context. We recommend further appraisal of this approach on a larger scale with more extensive follow-up.
Keywords
Since their introduction more than 30 years ago, osseointegrated hearing implants have become an established treatment option for auditory rehabilitation in patients with numerous conditions resulting in conductive, mixed, or sensorineural hearing loss.
Traditional teaching on implantation of such devices, and indeed the originally proposed surgical technique, mandates liberal subepidermal tissue reduction and hair removal in the area surrounding the percutaneous abutment to minimize soft-tissue movement around the abutment and, by association, the risk of adverse soft-tissue reactions. 1 Although techniques have continually evolved, with numerous variations described,2 -5 until recently all have remained true to this traditional surgical tenet.
However, with the common goal of averting postoperative paraesthesia and/or chronic pain in the periabutment area and to improve cosmesis, specifically prevention of permanent hair removal and “denting,” several authors have challenged this conventional dogma, reporting contemporary techniques with minimal or no soft-tissue removal.6-11 While taking advantage of the relatively recent availability of longer abutment lengths, all such techniques have continued to use traditionally shaped titanium-based implant systems not designed specifically for soft-tissue preservation. Although titanium possesses excellent biocompatibility and has the unique ability to osseointegrate with bone, it does not integrate well with soft tissues and as such lacks the ability to develop a stable soft tissue–abutment interface, thought to be a prerequisite for maintaining a healthy implant site in the context of soft-tissue preservation.12-17
In 2012, the DermaLock (BA400) abutment (Cochlear Bone Anchored Solutions AB, Molnlycke, Sweden) was introduced, the first designed specifically for soft-tissue preservation surgery. The abutment features a pronounced concavity on its lower section and is coated with a layer of hydroxyapatite, both of which are unique design characteristics to facilitate tight integration between the abutment and surrounding soft tissues.
To date, there have been no published reports in the English language literature evaluating outcomes with this novel abutment in the clinical setting. We sought, therefore, to appraise our early experience with this abutment with corresponding patient-reported outcomes.
Materials and Methods
Patients and Setting
This was a prospective study of the first 30 consecutive patients undergoing bone-anchored hearing device implantation using the DermaLock (BA400) abutment (Cochlear Bone Anchored Solutions AB) at our institution (February-September 2013), the regional tertiary referral center for adult osseointegrated hearing implant surgery in Merseyside and Cheshire, United Kingdom.
Patient demographics and the indications for implantation were extracted from hospital records, while data regarding procedure duration were collected perioperatively for each case.
Operative Technique
All implants were performed as single-stage procedures by the senior author (R.H.T.). One case was performed under general anesthetic owing to patient preference, with the remainder performed under local anesthetic.
The designated implant site was marked preoperatively; typically fixtures were positioned 55 mm from the external auditory meatus at an angle 45° postero-superior to the horizontal plane. Prior to infiltration of local anesthetic, soft-tissue thickness was measured with the aid of a small-gauge hypodermic needle, clamp, and ruler to guide selection of abutment length—available in 4 different lengths in 2-mm increments from 6 to 12 mm. The optimal abutment length was deemed to be 2 to 3 mm greater than the measured soft-tissue thickness, in accordance with the manufacturer’s instructions. Subsequently, a 2- to 3-cm linear incision was made to gain access and was extended to a small cruciate incision around the implant ( Figure 1 ). No dermal reduction was undertaken, and thereafter implant insertion was performed in a standard fashion using an Osscora hand piece and foot controller (Cochlear Bone Anchored Solutions AB).
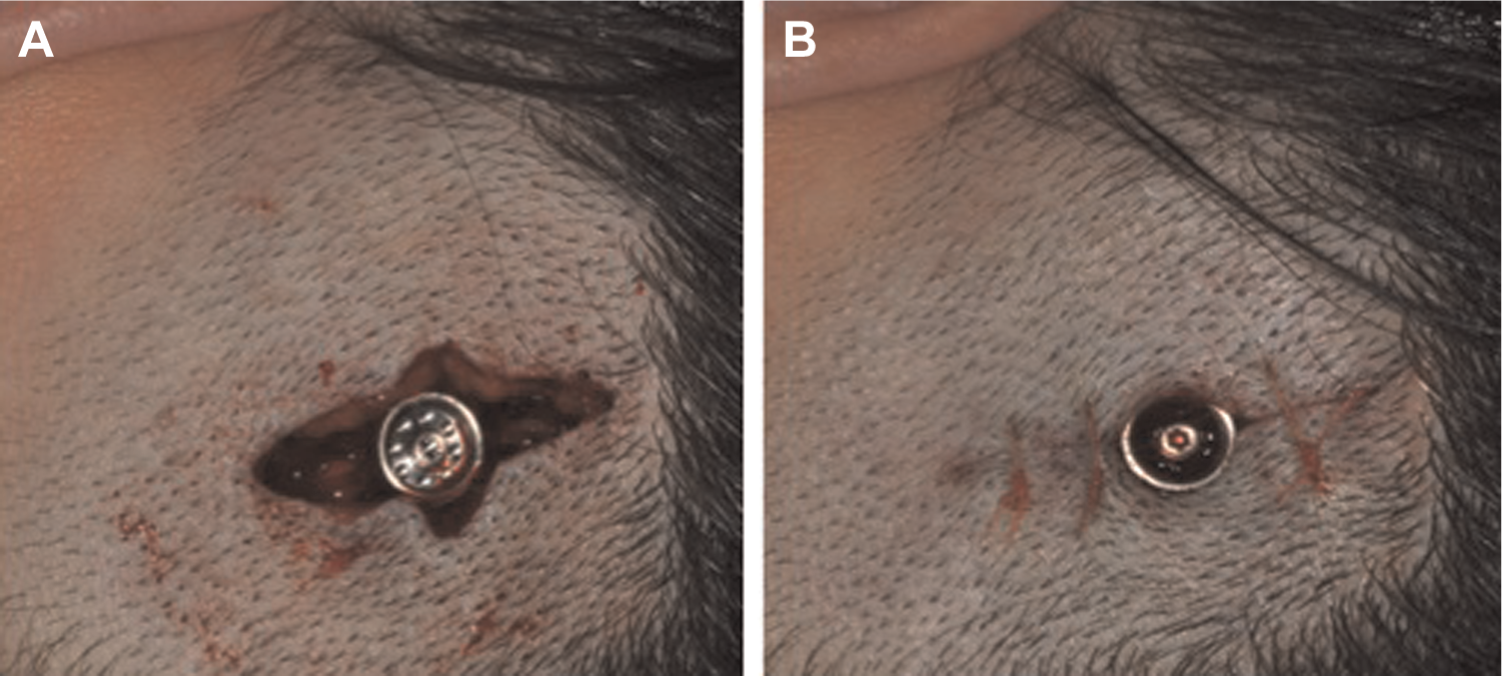
Intraoperative photographs demonstrating the cruciate incision used with no soft-tissue reduction preclosure (A) and following closure (B).
Outcomes and Analysis
Postoperatively, patients were followed prospectively for a minimum of 6 months, and any complications were recorded, chiefly periabutment soft-tissue reactions, which were graded according to Holger’s classification. 18 In addition, patients were asked specifically about periabutment paresthesia and pain. Time from implantation to fitting of the sound processor was also noted.
Four months following sound processor fitting, patients were asked to complete the Glasgow Benefit Inventory (GBI), relating to their bone-conduction hearing device, by means of postal survey. A reminder was sent 3 weeks later to those who had yet to respond by that time. The GBI is a validated postinterventional assessment tool, which comprises 18 health-related quality-of-life questions, and it is specifically designed to detect change in health status in the context of otorhinolaryngological interventions. 19 The response to each question is based on a 5-point Likert-type scale ranging from a large deterioration through to marked improvement in health status. A total score and 3 subscale scores (general subscale, social support, and physical health) are then calculated from the response scores. 19 All scores range from −100 (maximal negative benefit) to 0 (no benefit) to +100 (maximal positive benefit). 19
All data were collated in and analyzed using Excel for Mac 2011 (Microsoft Corp, Redmond, Washington). GBI scores were observed to be parametric in nature; thus, mean values were used in this study. Furthermore, presentation of mean GBI scores facilitates comparison with previous GBI studies as most, and indeed the original validation study, 19 have reported mean scores for their study cohorts.
Ethical Considerations
All data collection and analysis were carried out in accordance with our institution’s Clinical Information and Audit Department regulations and approval.
Results
The mean patient age at implantation was 61 years (range, 23-91 years), with a slight female preponderance (17 women, 13 men). Two patients were noted to suffer from diabetes mellitus, but no other medical conditions recognized to affect wound healing were identified in our study cohort. The mean duration of follow-up after implantation was 8 months (range, 6-13 months). The procedure was indicated for single-sided deafness in 8 cases (26.7%) and in the remainder for mixed loss with a significant conductive component when a conventional hearing aid was contraindicated. No patients in the study had undergone previous osseointegrated hearing implant surgery.
The mean operating time was 16 minutes (range, 9-22 minutes). The distribution of abutment lengths used, as dictated by measured skin depth (see the Materials and Methods section), was as follows: 6 mm (n = 5), 8 mm (n = 8), 10 mm (n = 10), 12 mm (n = 7). There were no intraoperative complications.
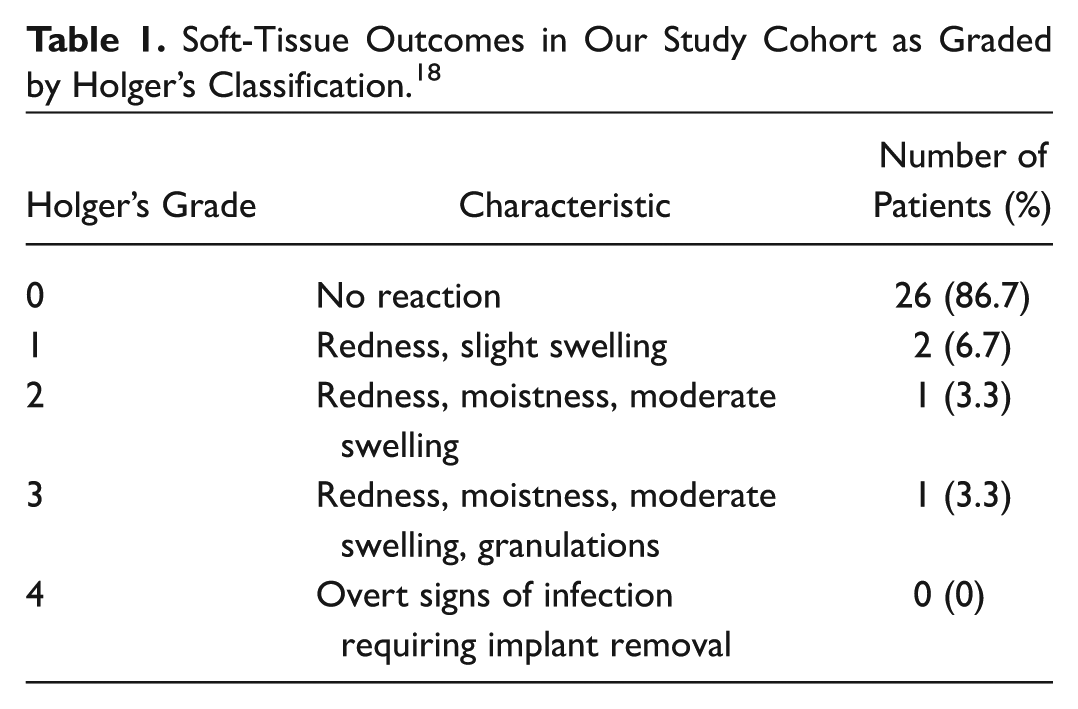
Postoperatively, favorable and expeditious wound healing was observed in all cases, with minimal surgical defect and hair loss, typical examples of which are shown in Figure 2 . Four patients (13.3%) suffered subsequent implant site soft-tissue reactions, all of which were successfully managed conservatively using varying combinations of topical steroid, silver nitrate cautery, and topical and oral antibiotics. Grading of the soft-tissue outcomes, as per Holger’s classification, 18 is detailed in Table 1 . Three patients (10%) reported periabutment paraesthesia in the early postoperative period, which resolved in all cases by 6 month follow-up, while no patients reported chronic pain. No other complications were observed in our study cohort.
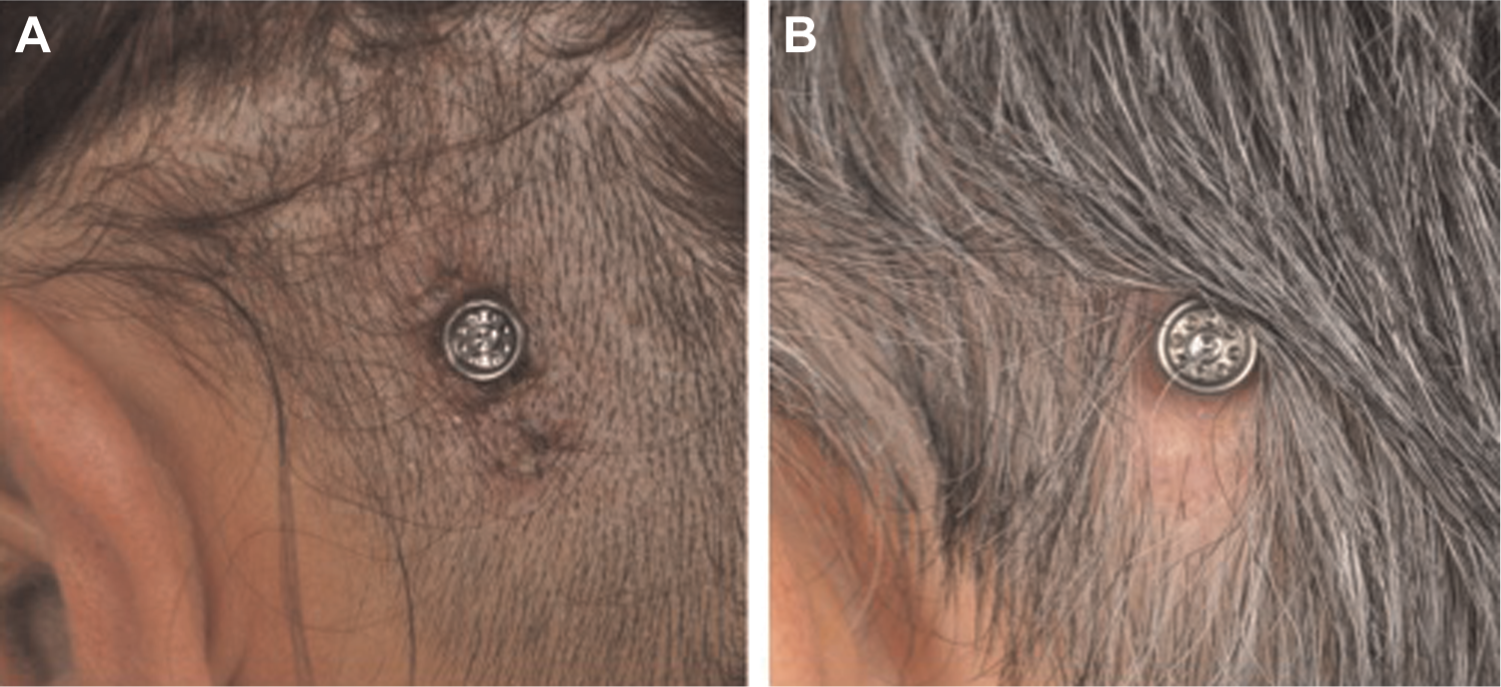
Typical wound healing and cosmetic outcomes at 1 week (A) and 8 weeks (B) postoperatively.
Soft-Tissue Outcomes in Our Study Cohort as Graded by Holger’s Classification. 18
The mean time from implantation to loading of the sound processor was 4.5 weeks (range, 2.5-9 weeks). In one instance, loading was delayed owing to a postoperative soft-tissue reaction, while the remainder were all loaded within 6 weeks of implantation.
Regarding patient-perceived outcomes, the response rate to the postal questionnaire was 86.7%. All of those who responded reported positive overall benefit scores, with a mean overall score of +38 (95% confidence interval [CI], 31-45). Respective general health, social support, and physical health subscale mean scores were +51 (95% CI, 42 to 60), +19 (95% CI, 8 to 30), and +8 (95% CI, –1 to 17). A breakdown of responses according to GBI questionnaire items with corresponding mean scores is depicted in Table 2 .
Breakdown of Responses according to Individual Questions on the GBI Questionnaire.

Items used to calculate general benefit.
Items used to calculate social benefit score.
Items used to calculate physical health benefit.
Discussion
Although the efficacy of osseointegrated hearing implants is well established in a variety of patient populations, adverse soft-tissue reactions remain a common complication, and extensive soft-tissue reduction frequently results in transient or permanent numbness in the peri-implant area and a poor cosmetic result.7,10,20,21 The quintessential surgical approach would create a reaction-free cutaneous-implant interface as well as minimize cosmetic concerns while not compromising efficacy. Recent reports of soft-tissue preservation surgery6-11 appear to represent an important advance in this regard, and such techniques are likely to become increasingly popular among implant surgeons. It is of paramount importance, therefore, to examine factors that may assist in optimizing outcomes for patients. To this end, principal findings from our early experience with the DermaLock (BA400) abutment (Cochlear Bone Anchored Solutions AB) indicate that use of this novel abutment design in the context of soft-tissue preservation surgery is associated with encouraging clinical outcomes in adult patients.
Congruous with previous reports of soft-tissue preservation surgical techniques,6-11 we observed rapid wound healing with favorable cosmetic outcomes, specifically no hair loss or “denting,” in all patients. Importantly, such expedient would healing also enabled early loading of the sound processor in all but one of our patients, for whom loading was unfortunately delayed owing to a Holger’s grade 3 soft-tissue reaction. All remaining patients were loaded within 6 weeks of surgery, with a mean time to loading of 4.5 weeks. Moreover, we believe that loading could have been undertaken even earlier in the postoperative period for most patients but regrettably was impeded by limited audiology department resources at our institution. Indeed, one of our patients was successfully loaded at 2.5 weeks, and findings from previous studies examining implant stability in bone over time support early sound processor loading provided wound healing allows for this.22,23
In addition to favorable wound healing, no patients in our study cohort reported chronic pain around the implant site, and only 10% reported paresthesia at any time in the postoperative period, with resolution in all such cases by 6-month follow-up. This represents an important advantage of soft-tissue preservation surgery, as this can be a troublesome ramification of soft-tissue reduction,21,24 which is likely underreported. While the retrospective nature of almost all series to date reporting soft-tissue preservation techniques has precluded analysis of such a subjective outcome, in a prospective clinical trial Hultcrantz 7 noted a markedly lower incidence of postoperative numbness around the implant site with soft-tissue preservation: 14.2% versus 100% with a conventional surgical approach.
A further putative advantage of soft-tissue preservation surgery relates to operative duration. Mean reported operating times for soft-tissue preservation techniques have typically been in the order of 15 to 30 minutes,6-11 comparable to our recorded mean time of 16 minutes, while soft-tissue preservation studies including a comparator patient group implanted using a conventional surgical approach have all demonstrated significantly reduced operative times for the soft-tissue preservation method.7,9,10 Although detailed economic evaluation is beyond the scope of the current study, these data, taken together with the aforementioned faster healing times and in turn reduced clinic visits, would suggest that soft-tissue preservation surgery may confer considerable cost savings when compared with traditional techniques and certainly merits further investigation in a more robust cost-analysis study.
A fundamental concern regarding soft-tissue preservation, however, relates to the potential for adverse soft-tissue reactions. Whereas with traditional techniques a stress-free abutment–soft tissue interface is achieved through meticulous dermal reduction, in the context of soft-tissue preservation, a strong adhesion between abutment and the surrounding tissues is thought to be necessary to limit epidermal down growth and pocket formation and thereby maintain a healthy implant site.14-17 However, conventional titanium-based abutments, which have been used in all published reports of soft-tissue preservation surgery to date,6-11 do not promote such integration,12,13,15,17 and as such, higher rates of adverse soft-tissue reactions than those reported may have been envisaged. Extrapolating findings from studies of other percutaneous devices,14,17,25 and more recently from a histological animal study in the context of osseointegrated hearing implantation, 15 particular device shaping and the use of hydroxyapatite ostensibly augment integration with surrounding soft tissues. Specifically, in the latter study, Larsson et al 15 demonstrated enhanced dermal adherence and reduced epidermal down growth and pocket formation for hydroxyapatite-coated abutments implanted in sheep, with effects further optimized using hydroxyapatite-coated abutments with a concave shape. Indeed, it is such findings that underpin the DermaLock (BA400) abutment (Cochlear Bone Anchored Solutions AB) design. It is perhaps unsurprising, therefore, that our observed soft-tissue outcomes with this abutment appear, on the whole, propitious in comparison with those reported previously in other soft-tissue preservation surgery studies using traditional titanium-based abutments. Only 4 patients (13.3%) in our study group suffered from soft-tissue reactions, only 2 of which (6.7%) were Holger’s grade ≥2, and all were managed successfully by conservative means. Although Hultcrantz 7 reported a similar soft-tissue reaction rate (14%) in the earliest published study of soft-tissue preservation surgery, this was based on a small study cohort of only 7 patients, and soft-tissue reactions have been reported subsequently in up to 37.5% of adult cases, with 28.1% graded ≥2, when using conventional abutment designs in the context of soft-tissue preservation surgery. 6 It is important to point out, however, that the follow-up period in our patient group is relatively short, and an appreciable proportion of reported soft-tissue complications may occur more than 12 months postoperatively.2,3
As with any surgical procedure, it is of ever-increasing importance to assess patient-reported outcomes, particularly when new approaches are being explored. Indeed, this information is vital for surgeons to be able to provide evidence of benefit of their interventions and, more importantly, to enhance our ability to counsel patients regarding expected outcomes. Although numerous studies have examined patient-perceived benefit of osseointegrated hearing implantation, several using the GBI assessment tool,26-29 until now, none have done so when employing a soft-tissue preservation approach. In addition, the prospective nature of the current study enabled administration of the GBI at a preset time interval, avoiding a principal drawback of many of the previous GBI studies, which, owing to their retrospective nature, have administered questionnaires at varying time points after intervention, conceivably confounding responses. Within our study cohort, positive mean GBI benefit scores were observed on all domains but with least benefit noted for physical health, as would be anticipated when examining an intervention aimed at improving hearing. 19 Importantly, all patients in our study reported positive overall benefit scores, with a mean overall score of +38 (95% CI, 31-45), which compares favorably with scores reported previously following unilateral implantation in adults using traditional techniques. In the first study using the GBI to assess bone-anchored hearing devices Arunachalam et al 26 reported a mean overall benefit score of +31 (95% CI, 22-41) in 60 adult patients, while subsequent studies have noted very similar overall scores in adult patient groups implanted for a variety of indications.27-29 It is interesting to note that a relatively high proportion of our patients were implanted for single-sided deafness (26.7%), which arguably adds weight to the auspicious patient-perceived benefit observed, given that this indication tends to be associated with lower benefit scores when compared with other indications. 27 Although the GBI does not enable us to ascertain the reasons as to why patients may have reported higher levels of benefit in this study, it is intuitive to suggest that the laudable cosmetic outcomes and the rapid wound healing time, with concomitant early sound processor loading, that result from soft-tissue preservation surgery may have positively influenced patients’ perception of the clinical pathway.
Conclusions
The present report provides a unique clinical perspective on osseointegrated hearing implant surgery with soft-tissue preservation using a novel hydroxyapatite-coated concave abutment design. Frailties relating to a relatively small study cohort with limited follow-up notwithstanding, our preliminary findings lend further credence to the notion of a surgical approach avoiding dermal reduction and indicate that the technology on which the DermaLock (BA400) abutment (Cochlear Bone Anchored Solutions AB) is based may indeed translate favorably into clinical practice, possibly enhancing soft-tissue outcomes in the context of soft-tissue preservation surgery. Moreover, we have demonstrated that patient-reported quality of life may be enhanced when using a soft-tissue preservation approach. We hope that such encouraging outcomes will prompt other suitably specialized and motivated centers to consider using this novel abutment design in combination with soft-tissue preservation, which would also facilitate further larger-scale, multicenter studies with longer follow-up, which are no doubt required to corroborate this initial report.
Author Contribution
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This study was presented at the annual North of England Otolaryngology Society Spring Meeting; March 14, 2014; Liverpool, United Kingdom.