
Abstract
Objectives
Sentinel lymph node biopsy (SLNB) is standard practice for intermediate-thickness head and neck melanoma (HNM) but remains controversial for melanomas more than 4 mm in thickness. The objectives of this study were to evaluate (1) the diagnostic accuracy and (2) the prognostic value of SLNB in patients with thick HNM.
Study Design
Case series with chart review.
Setting
Large cancer center between June 2000 and December 2012.
Subjects
77 patients undergoing SLNB for T4 HNM without in-transit, regional, or distant metastatic disease at presentation.
Methods
Univariate and multivariate analyses of prognostic factors were performed.
Results
77 patients underwent attempted SLNB for T4 HNM without in-transit, regional, or distant metastatic disease at presentation. The mean patient age was 62 years (range, 4-87 years) and there was a male predominance (80%). Mean Breslow thickness was 6.1 mm (range, 4-21 mm). Of the 77 patients undergoing attempted SLNB, 7 had no identifiable sentinel lymph node (9%). For the remaining 91% with 1 or more identifiable sentinel lymph nodes, the mean number of nodes identified was 3.3 (range, 1-13). The sentinel lymph node positivity rate was 24%. A false-negative SLNB occurred in 2 patients (3.8%). With a median follow-up of 36 months, the estimated 5-year disease-free, disease-specific, and overall survival rates were 47%, 74%, and 69%, respectively. A positive sentinel lymph node was significantly linked to shortened disease-free survival (74 vs 36 months, P = .026) and disease-specific survival (121 vs 59 months, P = .035).
Conclusion
SLNB provides accurate staging of the regional node basin and important prognostic information for patients with thick HNM.
Keywords
Introduction
The role of sentinel lymph node biopsy (SLNB) in the management of intermediate-thickness head and neck melanoma (HNM) is well-established. In contrast, for patients with thick melanomas (>4 mm), pathologic staging remains controversial. A perceived lack of benefit due to increased rates of occult distant metastatic disease at presentation and resultant difficulty in demonstrating a survival benefit from removal of regional nodes have been the principal arguments against SLNB in this population.1,2
At the same time, multiple retrospective studies have demonstrated that SLNB provides important staging and prognostic information for patients with thick melanomas of all sites.1,3-20 These series have limited numbers of patients with HNM, making interpretation of the diagnostic accuracy and prognostic value of SLNB in thick HNM difficult. One of the largest series included 293 patients with thick melanomas, of which 76 were located in the head and neck. 10 Survival was significantly improved in patients with T4 melanomas without metastases to the sentinel lymph node (SLN) (85% vs 48%), with the status of the SLN being the most significant prognostic factor. However, 23% of the HNMs in this study were classified as desmoplastic melanomas, with known lower rates of SLN positivity, thereby limiting the conclusions of this study with regard to the value of SLNB for thick HNM.
The primary objectives of this study were to evaluate the diagnostic accuracy and prognostic value of SLNB in a retrospective cohort of patients with thick HNM treated at a large cancer hospital.
Methods
Patients
This study was approved by the MD Anderson institutional review board. Patients with T4 cutaneous melanoma of the head and neck without clinical evidence of regional, in-transit, or distant metastatic spread at presentation were identified from a prospective institutional database. Tumor thickness was determined by the thickest Breslow depth from either the pretreatment biopsy or subsequent surgical excision. Patients with recurrent or second primary melanomas or those whose pathologic staging was performed outside of the study institution were excluded. Patients underwent preoperative lymphoscintigraphy and SLNB as has been previously described. 21 Medical records were reviewed for patient, pathology, treatment, and outcomes data.
Statistical Analysis
Categorical data were evaluated with the chi-square and Fisher’s exact test. Continuous data were analyzed with independent t tests and the Mann-Whitney U test for comparisons of means with variables of 2 groupings and the 1-way ANOVA and Kruskal Wallis tests for variables with more than 2 groupings. Univariate survival analysis was estimated by the Kaplan Meier method and compared with the log-rank test. Multivariate analysis was accomplished using the Cox proportional hazards model with inclusion of prognostic factors with a P value of ≤.2 identified by univariate analysis. A false-negative SLNB was defined as recurrence within an SLNB-negative nodal basin. Statistical analysis was accomplished with SPSS version 19 (SPSS Inc, Chicago, Illinois). Results were considered significant for P ≤ .05.
Results
A total of 77 patients were identified with head and neck primary melanomas greater than 4 mm in thickness without evidence of in-transit, regional, or distant metastatic disease at presentation. Of these, 70 had an SLN identified by lymphoscintigraphy and were included in the analysis ( Figure 1 ). The study population was predominately white (95%) and male (80%), with a mean age of 62 years (range, 4-87 years). The mean Breslow thickness was 6.1 mm (range, 4-21 mm). The most common histologic subtypes included nodular (40%), superficial spreading (24%), and desmoplastic variants (11%). Head and neck subsites involved, in order of decreasing frequency, included the scalp (50%), face (28.5%), neck (18.5%), and eyelid (3%) ( Table 1 ). With a median follow-up of 36 months, the estimated 5-year disease-free, disease-specific, and overall survival rates were 47%, 74%, and 69%, respectively.
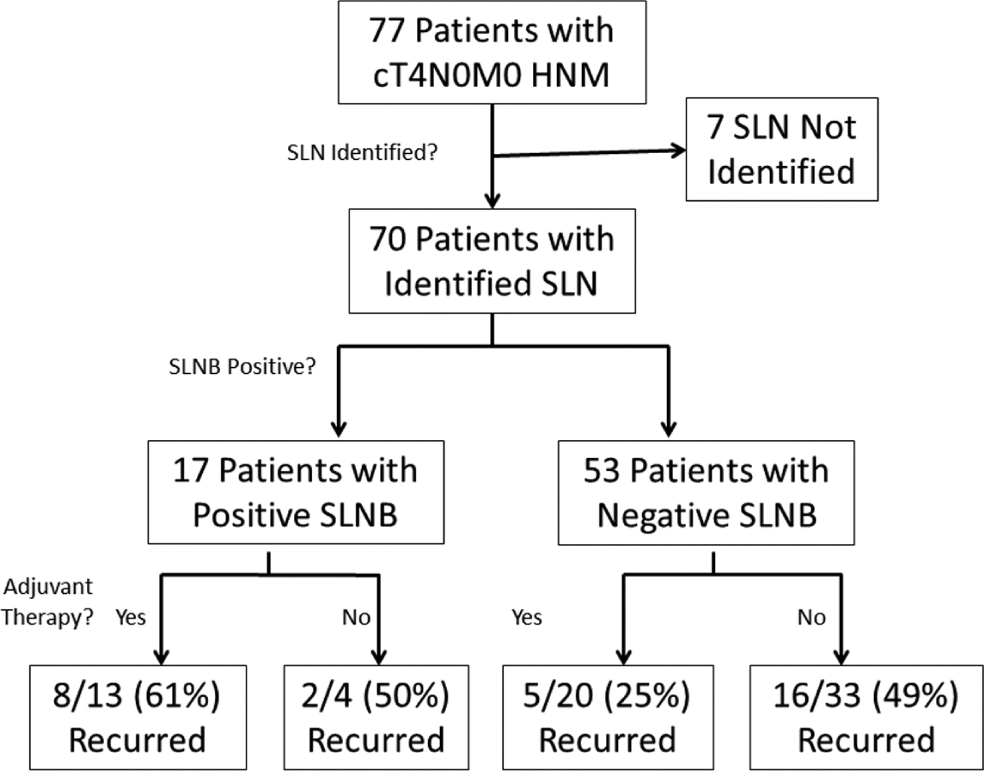
Study population flow diagram. HNM, head and neck melanoma; SLN, sentinel lymph node; SLNB, sentinel lymph node biopsy.
Population Characteristics.
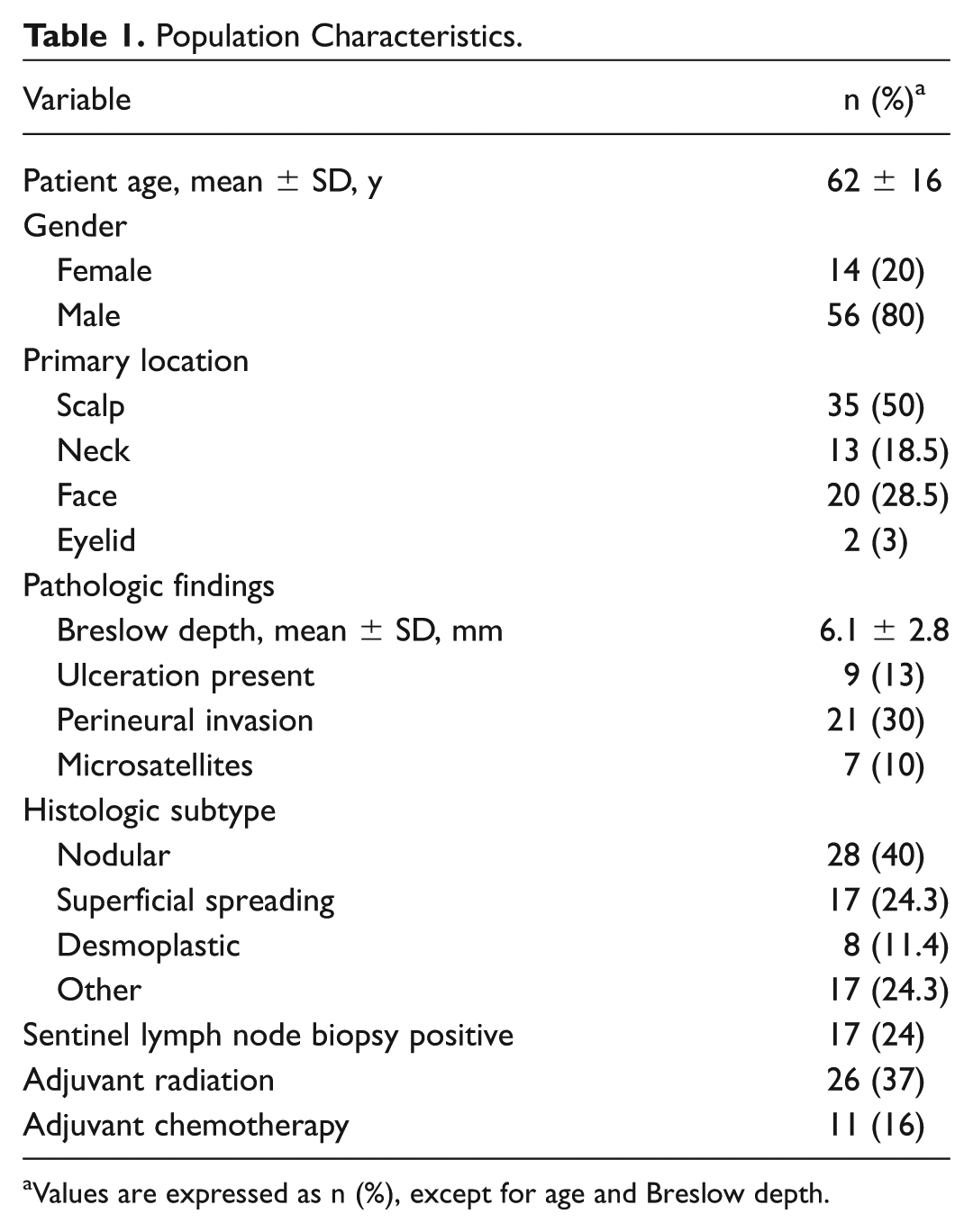
Values are expressed as n (%), except for age and Breslow depth.
Preoperative lymphoscintigraphy was attempted on 77 patients and was unsuccessful in 7 patients, for an overall identification rate of 91%. Patient age, anatomic subsite, histologic subtype, and Breslow depth did not significantly differ between patients with an identified and nonidentified SLN. Similarly, overall survival did not differ significantly between patients with an identified SLN and those in whom an SLN could not be identified (100 vs 72 months, P = .959).
Of the 70 patients who had an SLN identified by lymphoscintigraphy and underwent SLNB, a positive sentinel node was identified in 17 (24%). On univariate analysis, the presence of a positive sentinel node was significantly associated with reduced disease-free survival (74 vs 36 months, P = .026) and disease-specific survival (121 vs 59 months, P = .035). Patients with a positive SLNB demonstrated a mean overall survival of 55 months compared with 108 months in those with a negative SLNB (P = .082; Table 2 , Figure 2 ).
Univariate Survival Analysis. a
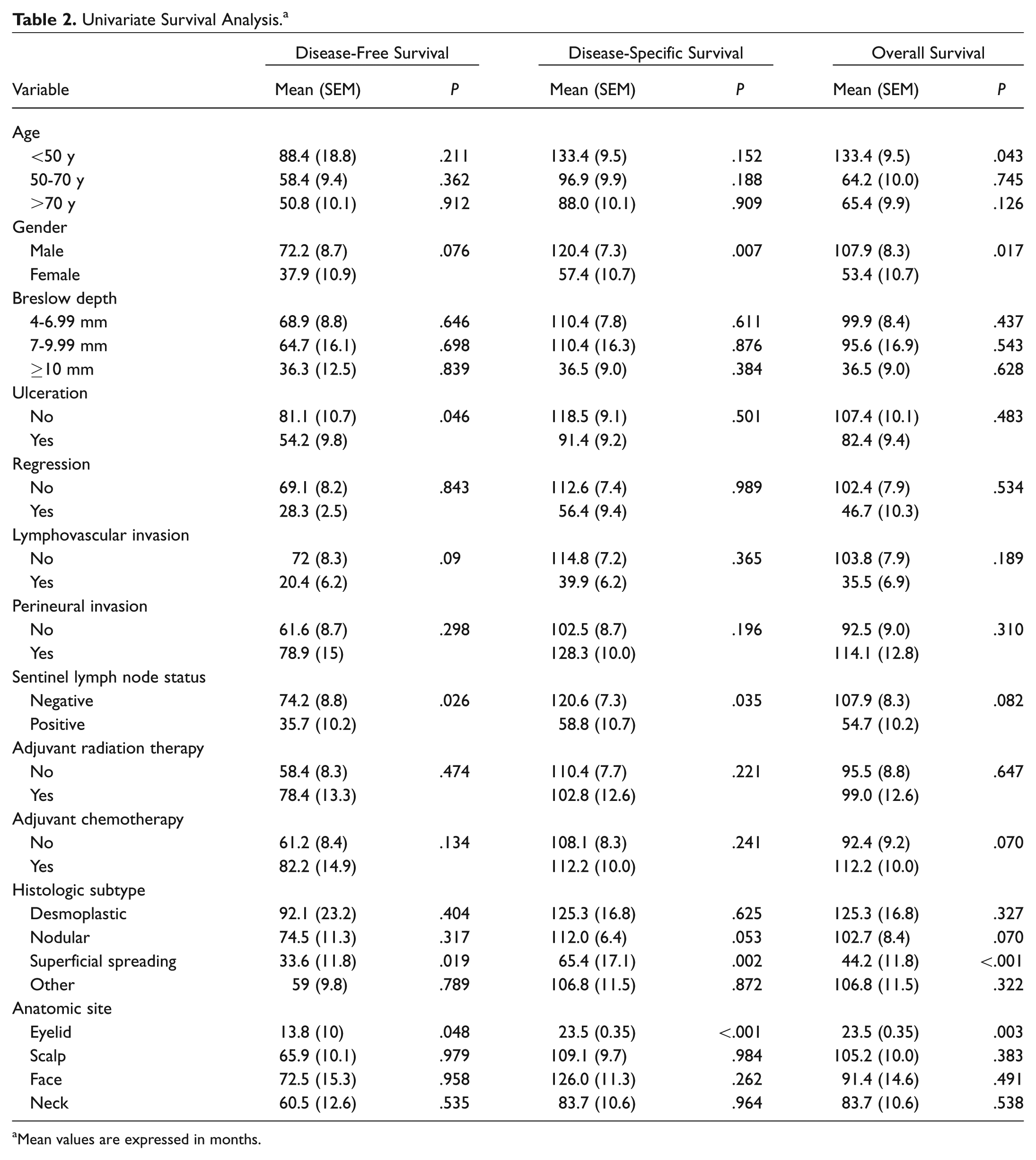
Mean values are expressed in months.
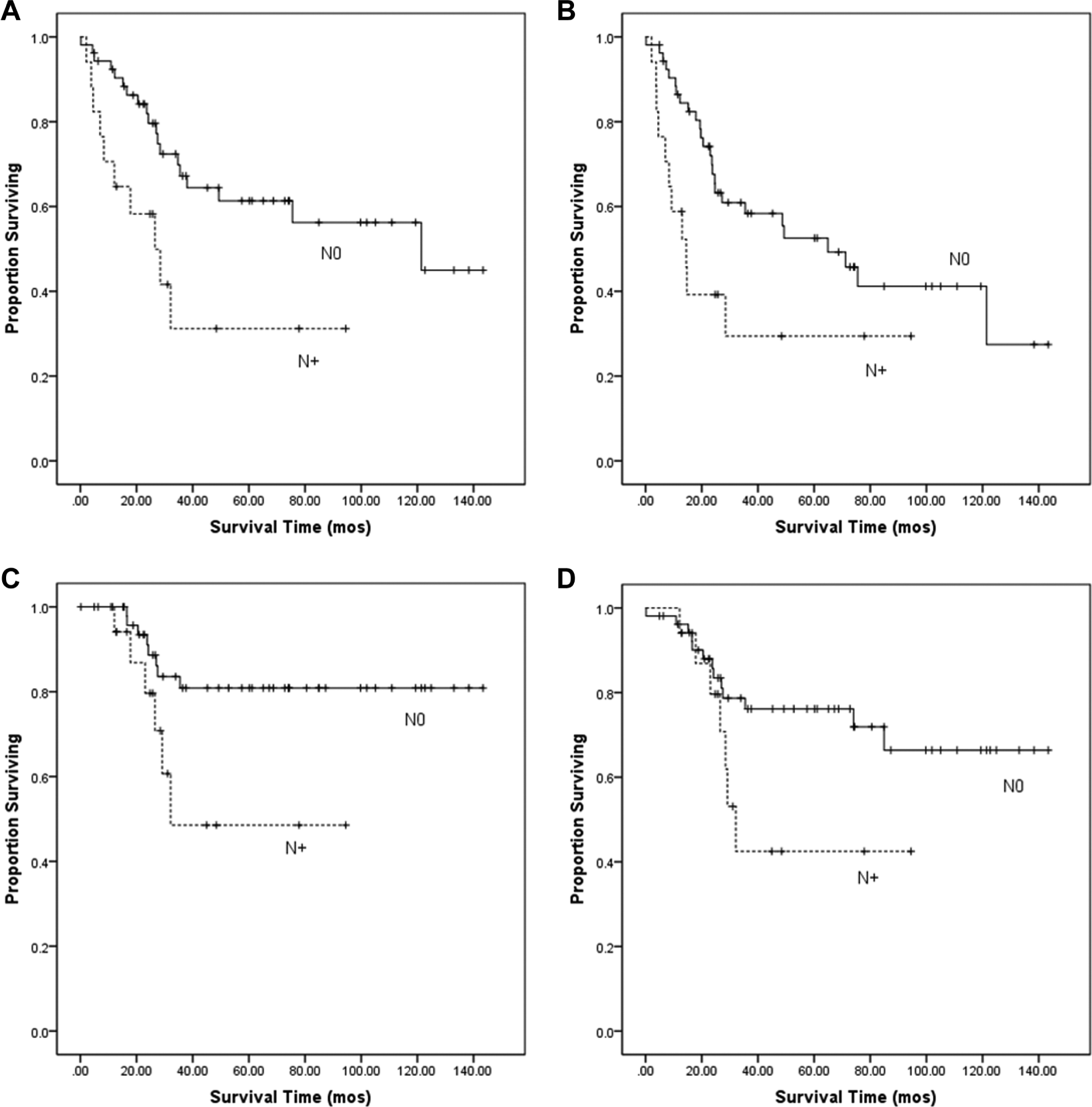
Kaplan Meier survival estimates in N0 and N+ patients. (A) Locoregional recurrence-free survival, (B) disease-free survival, (C) melanoma-specific survival, (D) overall survival.
On multivariate analysis, the status of the SLNB remained the most significant factor for reduced disease-free survival (hazard ratio [HR] 4.2; 95% CI, 1.5-11.6; P = .006). Female gender (HR 2.7; 95% CI, 1.1-6.9; P = .035) was also significantly associated with a reduction in disease-free survival. Ulceration status did not achieve statistical significance (HR 2.1; 95% CI, 0.91-4.7; P = .082). The status of the SLN was not significantly associated with disease-specific or overall survival. By multivariate analysis, female gender was also associated with a reduction in disease-specific survival (HR 7.3; 95% CI, 1.4-38; P = .017) and overall survival (HR 8.7; 95% CI, 2.0-39; P = .005). A superficial spreading melanoma subtype (HR 9.6; 95% CI, 2.1-43; P = .003) and age less than 50 years (HR 0.04; 95% CI, 0.003-0.565; P = .016) were negatively and positively associated with overall survival ( Table 3 ).
Multivariate Analyses. a
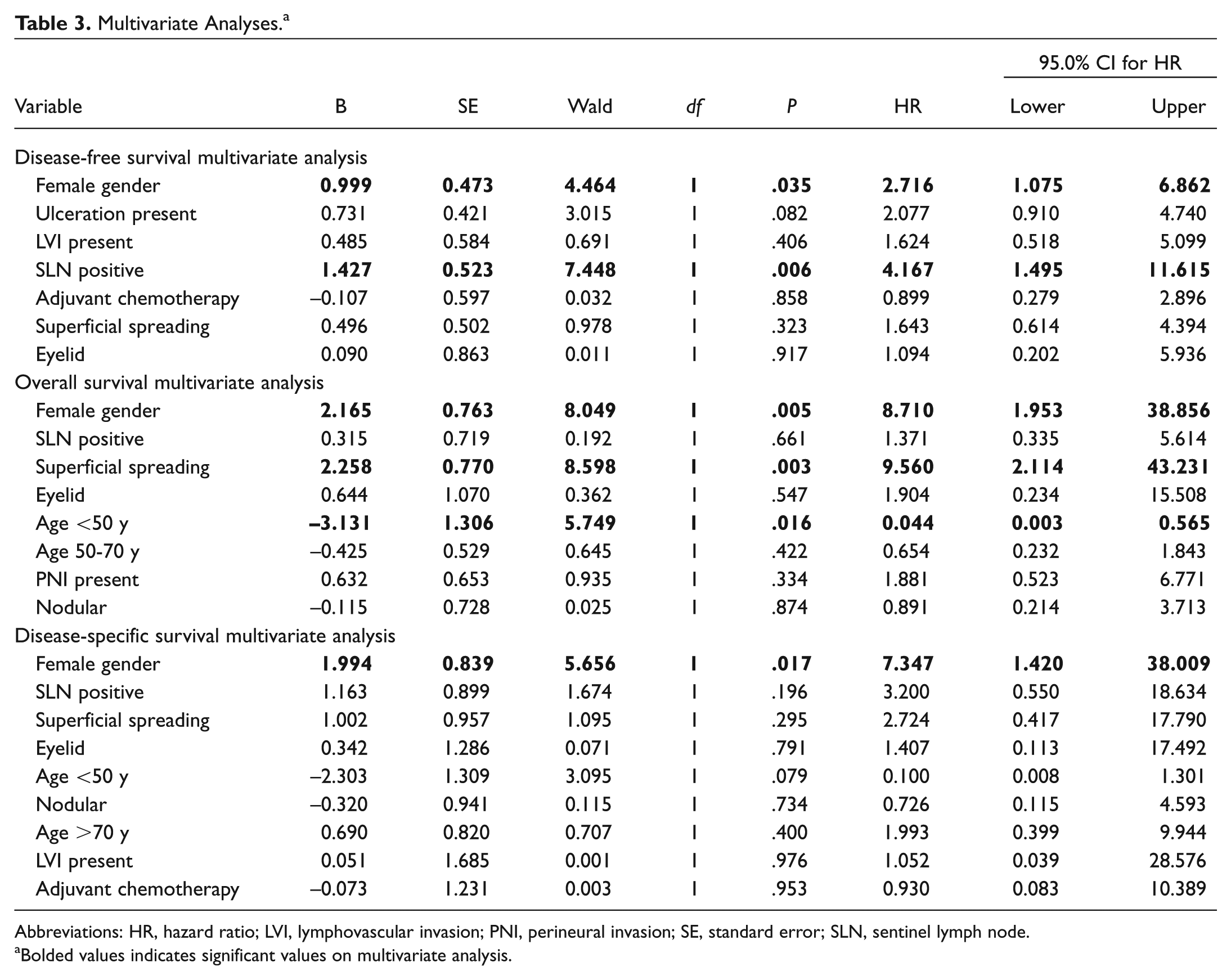
Abbreviations: HR, hazard ratio; LVI, lymphovascular invasion; PNI, perineural invasion; SE, standard error; SLN, sentinel lymph node.
Bolded values indicates significant values on multivariate analysis.
Adjuvant radiation therapy was used in 30% of patients with a thick HNM and a negative SLNB compared with 59% of patients with a positive SLNB (P = .09). Adjuvant chemotherapy was used in 11% of patients with a negative SLNB compared with 29% with a positive SLNB (P = .16). Any adjuvant treatment was used in 77% of patients with a positive SLNB and 38% of patients with a negative SLNB (P = .01). Of the 17 patients with an identified positive SLNB, 5 were observed and the remaining 11 underwent completion lymph node dissection. No patient who was observed developed a regional recurrence.
Recurrences were noted in 32 of 70 patients. In 10 patients, the first site of relapse occurred locally or in a regional nodal basin other than the one assessed by SLNB. Distant metastases as the initial site of recurrence occurred in 20 patients and in an additional 5 patients following initial locoregional relapse. Of the patients with a positive SLNB, 59% developed recurrent disease, whereas in those with a negative SLNB, 40% developed recurrent disease (P = .17). Distant metastatic disease occurred in 47% of patients with a positive SLNB and 38% with a negative SLNB (P = .51).
Of patients initially identified as SLNB negative, 2 patients recurred within the regional nodal basin (3.8% of total cases) for a false-negative rate of 10.5% and a negative predictive value of 96.2%. The 2 false-negative SLNB cases included a 12-mm ulcerated lower eyelid and an 8-mm ulcerated cheek primary that mapped to cervical lymph node levels 1 and 2, respectively.
The identification of a single SLN was significantly associated with a false-negative SLNB (P = .027), while the association between increased Breslow depth and a false-negative SLNB did not achieve significance (P = .058). Similarly, anatomic subsite, histologic subtype, ulceration status, mitotic index, lymphovascular invasion, perineural invasion, patient age, and patient gender did not display any significant association with a false-negative SLNB.
Given the survival discrepancies between genders, a comparison of male and female patients was undertaken. No significant differences were observed in rates of adverse pathologic features, use of adjuvant therapy, or histologic subtypes of melanoma. Likewise, male and female subjects did not significantly differ with respect to age or average Breslow depth. Significant differences existed in the sites of melanomas, with female subjects accounting for both of the cases of eyelid melanoma (P = .038).
Discussion
To date, large randomized trials have not demonstrated an improvement in overall survival with the use of SLNB.22,23 Despite this, SLNB has become standard practice and has been recommended as a measure of quality of care for intermediate-thickness melanomas. 24 This is due to the fact that pathologic staging adds important prognostic information that can guide treatment decisions, including the frequency and intensity of surveillance regimens as well as the use of adjuvant therapy.
For patients with thick melanomas, the use of pathologic staging remains controversial. Principal arguments against the use of pathologic staging in this population include a perceived lack of benefit due to a high rate of occult distant metastatic disease at presentation.1,2 Despite this, a growing series of retrospective studies has demonstrated the independent prognostic value of SLNB in patients with thick melanomas. Yet these studies have limited numbers of patients with thick HNM, making determination of the utility of SLNB in this population difficult.
Recently, the updated 10-year outcomes of the MSLT1 Trial comparing SLNB and observation were reported. 23 The prognostic value of SLNB in thick (>3.5 mm) melanomas was confirmed, with a reduction in disease-free survival noted for patients with a positive SLN. However, in comparison to intermediate-thickness melanomas, no significant reduction in melanoma-specific or distant-metastasis-free survival was demonstrated for patients with thick melanomas and lymph node disease who underwent SLNB compared with observation.
Here we demonstrate that the overall rate of regional lymph node involvement was only 24%, well below that reported for thick melanomas of other body sites7,11 and in line with the rate of regional disease reported in a recent study using the SEER database for thick HNM. 25 This may reflect a lower propensity for regional disease in patients with thick HNM compared with other body sites.
The presence of a positive SLN was associated with a significant reduction in disease-free survival and disease-specific survival, while no significant association was noted for overall survival on univariate analysis. Furthermore, on multivariate analysis, the presence of the SLNB remained the most significant factor associated with disease-free survival. This fact points to the important prognostic information provided by SLNB for patients with thick HNM and suggests that the status of the SLNB may be a rational method to approach treatment intensification through the use of adjuvant therapy. Adjuvant therapy was used in 77% of SLNB-positive patients compared with 38% of SLNB-negative patients (P = .01), suggestive of the impact that the SLN status may have on therapeutic decision making.
The nonidentification rate of 9% (7 of 77) in this population is higher than that commonly reported in the literature for both intermediate and thick melanomas.21,26-29 We were unable to identify any statistically significant associations that may explain this elevated rate. Additional cases will be required to determine whether this is simply a statistical anomaly due to a small sample size or whether this finding reflects a true difference from other melanoma populations. However, survival rate did not differ significantly between those patients with an identified SLN and those in whom one could not be identified.
The low false-negative rate (3.8%) in this study is in line with previously published reports on the accuracy of SLNB in HNM.21,26-29 The identification of only a single SLN was the only factor statistically associated with an increased risk for a false-negative SLNB. This association has previously been reported for SLNB in thin melanoma. 27 It can be speculated that in some cases, the identification of only a single node may signify an inadequate load of radioactive colloid reaching the lymphatic system to provide a robust and accurate signal. Theoretically, this could be due to inadequate injection or interference with the transit of radioactive marker through the lymphatics due to scarring from prior surgery.
Female gender was significantly associated with a reduction in disease-free survival, disease-specific survival, and overall survival on multivariate analysis. Others have reported findings that suggest gender disparities in outcomes for nontrunk melanomas 30 as well. However, the overall limited number of female subjects in the current study (n = 14), and the fact that both eyelid melanomas with significantly shortened survival involved female patients, cloud interpretation of these findings.
As with any retrospective study, certain limitations are inherent. Only patients who underwent SLNB were included in this study. We do not have data on the number of patients with T4 melanomas who did not undergo SLNB or the percentage of patients known to be T4 prior to definitive surgical therapy, thereby potentially introducing selection bias. Given that multiple physicians were involved in treating these patients, preoperative workup including imaging for regional or distant metastatic disease prior to surgical intervention varied, which also could have influenced patient selection for SLNB. Given the small overall sample size, statistical power is limited, making interpretation of nonsignificant relationships difficult. For example, ulceration is a well-known prognostic marker in melanoma and is included in the American Joint Committee on Cancer (AJCC) staging system; however, this particular variable was not identified as being significant in this study. Similarly, increasing tumor thickness was not identified as an independent prognostic factor for thick HNM, although it has been identified as an independent prognostic factor in thick melanomas of all sites. 10 These findings may reflect either the limited power of the study or a true difference in thick HNM. Further work is needed to help clarify these questions.
While SLNB status was not predictive of overall survival on multivariate analysis, the ability to identify patients at higher risk of disease relapse provides a strong rationale for the use of SLNB in this patient population. This knowledge has important implications regarding the consideration of adjuvant radiation and chemotherapy as well as candidacy for clinical trial enrollment.
Conclusions
The SLNB provides important prognostic information for patients with thick HNM. Patients with a positive SLN are at significant risk of shortened disease-free survival. The use of SLNB may provide a rational method of selecting patients most likely to benefit from adjuvant therapy.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the 2013 AAO-HNSF Annual Meeting & OTO EXPO; September 29 to October 3, 2013; Vancouver, British Columbia, Canada.