
Abstract
Objective
Dizziness associated with vestibular schwannoma is usually ascribed to retrolabyrinthine mechanisms. The goal of this study was to determine if quantitative peripheral vestibular (labyrinthine) otopathology was present in a series of patients with vestibular schwannoma.
Study Design
Comparative human temporal bone study.
Setting
Otopathology laboratory.
Subjects and Methods
Temporal bones from 12 subjects with unilateral sporadic vestibular schwannoma were included. Based on differential interference contrast microscopy, type I and II vestibular hair cell counts were performed on each vestibular sense organ with minimal autolysis in which the neuroepithelium was oriented perpendicular to the plane of section. Hair cell densities (cells per 0.01-mm2 surface area) and the presence of endolymphatic hydrops and precipitate within the endolymph or perilymph were compared between the tumor ears and the contralateral (control) ears.
Results
Compared with the contralateral ears, vestibular schwannoma ears had significantly more endolymphatic hydrops (P = .049) and precipitate in the endolymph and perilymph (P = .005), lower densities of type I and II vestibular hair cells in the lateral canal cristae (mean differences, respectively: 25.2 [P = .001] and 10.8 [P < .001]) and utricle (mean differences, respectively: 26.8 and 10.4 [P < .001]), and lower densities of type I hair cells and the same density of type II hair cells in the saccule (mean differences, respectively: 26.5 [P < .001] and 0.9 [P = .46]).
Conclusion
Peripheral vestibular otopathology, manifested as reductions of vestibular hair cell densities, was identified in ears with vestibular schwannoma. Labyrinthine as well as retrolabyrinthine pathology may contribute to tumor-related vestibular dysfunction.
Vestibular symptoms are commonly associated with schwannoma of the eighth cranial nerve (acoustic neuroma, vestibular schwannoma [VS]). At the time of diagnosis, 30% to 75% of patients report at least 1 vestibular symptom, ranging from dizziness, disequilibrium, directional pulsion, and positioning vertigo to severe spontaneous vertigo and vestibular crisis events.1-3 Compared with hearing loss and tinnitus, vertigo has the greatest negative impact on health-related quality of life among those with VS,4,5 prompting a desire to further understand its pathogenesis and identify better management strategies. Clinicians commonly think of VS-associated dizziness as occurring because of dysfunction of the vestibular nerve. Supporting this contention is histopathologic evidence of destruction of vestibular nerve fibers from pressure atrophy or tumor invasion.6,7 Larger tumors may also cause centrally mediated vestibular symptoms by compressing the cerebellum and brainstem. 8
Pathology within the inner ear may be an upstream source of tumor-associated vestibular dysfunction. Prior histopathologic descriptions of VS of all sizes note ipsilateral inner ear changes, including endolymphatic hydrops and acidophilic-staining precipitate within the endolymph and perilymphatic compartments.6,9-13 This precipitate is considered to be the histopathologic correlate of the higher inner ear protein content present in ears with VS and may represent biochemical degradation of the inner ear fluids.7,14,15 Cochleae ipsilateral to VS have also been found to have greater losses of inner and outer hair cells and cochlear neurons when compared with unaffected ears.12,13 These findings suggest that there are cochlear as well as retrocochlear pathologies contributing to hearing loss caused by VS. 13 If analogous changes were present within the vestibular sensory organs, it would be reasonable to hypothesize that labyrinthine pathology contributes to the vestibular dysfunction and symptomatology that has been traditionally ascribed to retrolabyrinthine sources.
The goal of this human temporal bone (HTB) histopathologic study was to determine if peripheral vestibular pathology is present in a series of patients with VS. A quantitative analysis was undertaken to compare vestibular hair cell count density between ears with VS and contralateral unaffected ears. Our findings have implications for the pathogenesis and management of dizziness associated with VS.
Materials and Methods
Subjects and Specimens
The archives of the temporal bone collection at the University of Minnesota (Minneapolis, Minnesota) were searched to identify cases of VS meeting the inclusion criteria of sporadic unilateral VS with intact vestibular labyrinths. Temporal bones from subjects known to have the following conditions that might affect the vestibular system were excluded: head trauma, systemic autoimmune disorders, ototoxic drug use, and any defined otologic disease other than VS (eg, Meniere’s disease, active otitis media). Twelve eligible cases were identified. Of 12 subjects, 11 had untreated tumors. One patient died of a brainstem infarct immediately following subtotal suboccipital removal of the cerebellopontine angle component of the schwannoma (a procedure that spared the internal auditory canal [IAC] and labyrinth).
All temporal bones had been removed at autopsy, fixed in formalin solution, decalcified, and embedded in celloidin. Each bone was serially sectioned in the horizontal plane at a thickness of 20 µm. Every 10th section was stained with hematoxylin and eosin and mounted on a glass slide for light microscopy. The study was approved by the Institutional Review Board of the University of Minnesota (0206M26181).
Qualitative Histopathologic Assessment
HTBs from the affected and contralateral unaffected (control) ears were examined by light microscopy. The nerve of origin was identified for each schwannoma, and intracochlear, intralabyrinthine, and/or IAC involvement was noted. Each labyrinth was assessed for the presence or absence of precipitate within the endolymphatic and perilymphatic spaces. Hydrops was considered to be present if there was distension of the membranous walls of the saccule, utricle, or ampullae (vestibular) or of Reissner’s membrane (cochlear).
Vestibular Hair Cell Density Measurement
Quantitative assessment of the vestibular hair cells was performed as described by Merchant. 16 Accurate assessment is restricted to specimens with minimal to mild postmortem neuroepithelial autolysis and in which the plane of section is perpendicular to the surface of the sensory epithelium. 16 Based on differential interference contrast microscopy at ×1008 magnification, the cuticular plate and stereociliary bundles of the vestibular hair cells were visualized, and type I and II vestibular hair cells were morphologically distinguished from each other and from supporting cells according to the criteria described by Wersäll 17 and Merchant. 16 The type I vestibular hair cell is flask shaped with a spherical nucleus and is surrounded by an afferent nerve fiber chalice. The type II vestibular hair cell has a cylindrical shape with an ovoid nucleus and bouton nerve fibers terminating at its base. Both types have a cuticular plate and stereociliary bundle at their apices. Supporting cells have neither a stereociliary bundle nor a cuticular plate and are not innervated ( Figure 1 ).
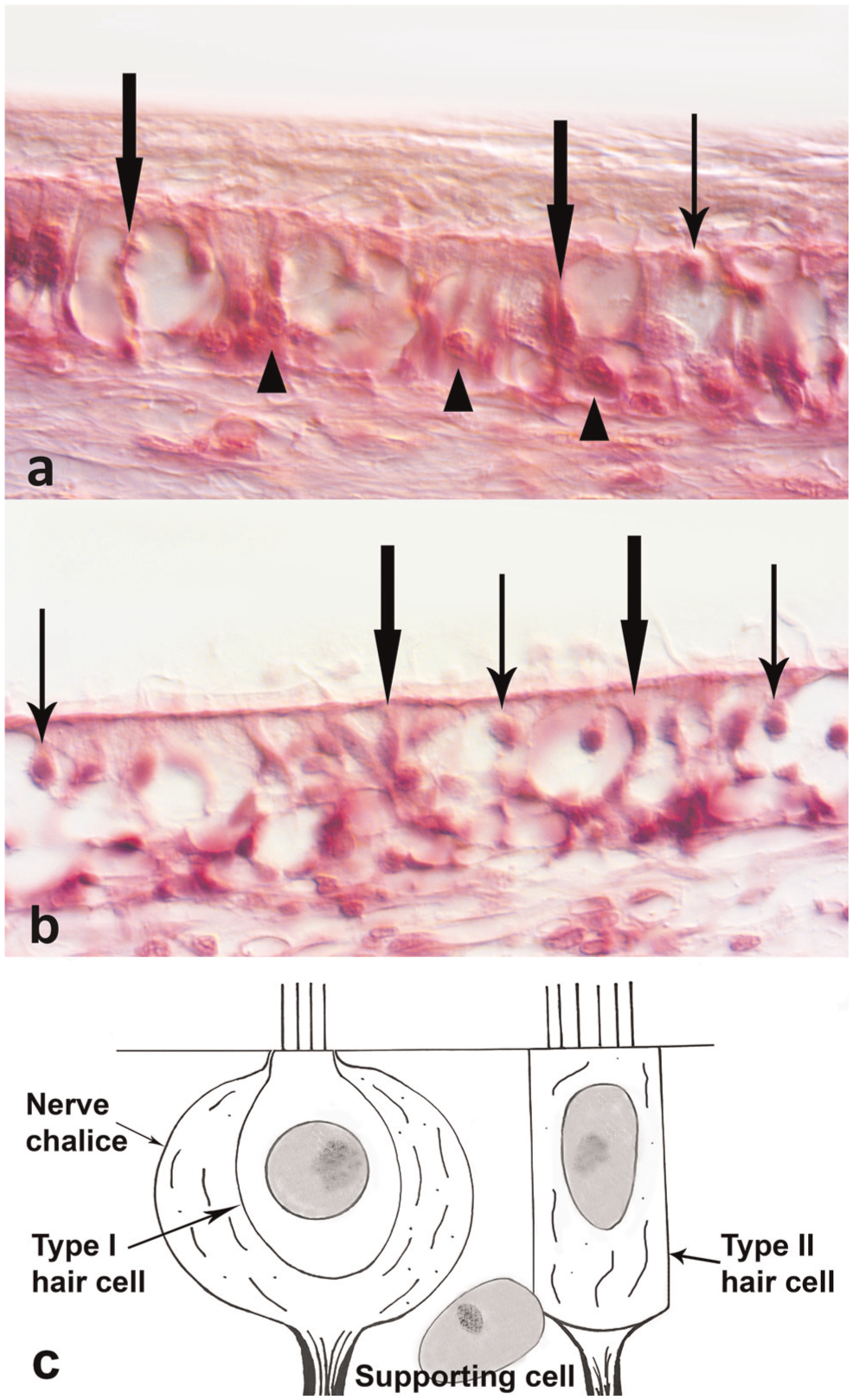
Differential interference contrast photomicrograph of saccular maculae from a 76-year-old man with an untreated unilateral vestibular schwannoma (hematoxylin and eosin stain): (a) vestibular schwannoma ear, (b) contralateral ear. Thin arrows: type I vestibular hair cells. Thick arrows: type II vestibular hair cells. Arrowheads: supporting cells. (c) Illustration of hair cell and supporting cell locations and characteristics.
Vestibular hair cell nuclei were counted in each perpendicularly sectioned macula and crista over viewable surface areas of 0.006 mm2. The results were expressed in terms of cell density (the number of hair cells per 0.01-mm2 surface area), in keeping with previous publications. 18 Surface area was determined by multiplying the thickness of the section (20 µm) by the length of the sensory epithelium where the count was made. The raw hair cell counts were corrected for double counting of cells split between 2 sections, per the formula of Abercrombie—Hi = hi ×t/(t+d), where Hi = corrected density of hair cells, hi = raw density, t = thickness of section (20 μm), and d = mean value of nuclear diameters in 250 vestibular hair cells— which results in correction factors of 0.82 for type I hair cells and 0.87 for type II hair cells.16,19
Statistical Analysis
Results are presented as mean (SD). Type I and II vestibular hair cell densities of each vestibular organ were compared between ears with VS and contralateral unaffected (control) ears. The normal distribution of data from each group were confirmed with the Kolmogorov-Smirnov test (P = .2). Statistical comparisons of binary outcomes (presence or absence of hydrops or precipitate) were performed with chi-square tests. Statistical comparisons between vestibular hair cell densities were performed with paired t tests, including subjects for whom the vestibular neuroepithelia of interest were appropriately sectioned and preserved on the affected and unaffected sides. SPSS 22.0 software for Windows (SPSS, Inc, Chicago, Illinois) was used for analysis of data. A P value <.05 was considered statistically significant.
Results
Twelve patients with unilateral VS were eligible for study (10 men, 2 women), with mean age of 70 (14) years (range, 44-86). Complete clinical historical information was not available for all subjects. Six had documented dizziness and/or episodic vertigo. The presence or absence of dizziness could not be determined from the extant case files of the remaining 6 subjects. Eleven cases were untreated. One subject died of a brainstem infarct immediately following an IAC- and labyrinth-sparing subtotal tumor resection, and peripheral vestibular changes were deemed attributable to tumor rather than surgical/postsurgical effects (supported by the absence of autolysis/ischemic changes in the operated ear and continued presence of the tumor within the IAC).
Table 1 lists the qualitative and quantitative otopathologic observations for all cases and contralateral control ears. All 12 tumors had an IAC component. Ten schwannoma originated from the vestibular nerve (4 from the superior division and 6 whose vestibular nerve division of origin could not be discerned) and 1 from the cochlear nerve, and 1 tumor filled the cochlea and the lateral half of the IAC. No tumors involved the vestibular labyrinth. The size of the cerebellopontine angle component could not be accurately estimated, as it was not preserved by traditional HTB removal and processing methods and premortem imaging was not available for review.
Vestibular Pathology in Unilateral Sporadic Schwannoma of the Eighth Cranial Nerve. a

Abbreviations: CH, cochlear hydrops; CN, cochlear nerve; D, dizziness; F, female; IC, tumor involved the cochlea and internal auditory canal; M, male; NA, not available; PR, precipitate; SC, semicircular canal crista ampullaris; SH, saccular hydrops; SVN, superior division of vestibular nerve; Sx, symptoms reported in case history file; UH, utricular hydrops; V, vertigo; VN, vestibular nerve.
For precipitate and hydrops: +, presence; –, absence. Control: contralateral control ear. Origin: tumor nerve of origin.
Subject died following surgery, described in the text.
Precipitate in the endolymphatic or perilymphatic spaces was observed in 67% of VS ears (8 cases) and in 1 contralateral control ear (χ2 = 7.99, P = .005). While no subjects had a documented diagnosis of Meniere’s disease, endolymphatic hydrops was present in 60% (7 cases) of the ears with VS and in 2 control ears (χ2 = 3.88, P = .049). Hydrops in VS ears involved the cochlea (n = 5), saccule (n = 5), and/or utricle (n = 4), and 1 subject had complete collapse of the saccular membrane. Figure 2 shows an example of temporal bone histology from 1 subject with VS with endolymphatic hydrops and precipitate in the perilymphatic spaces of the cochlea and vestibule.
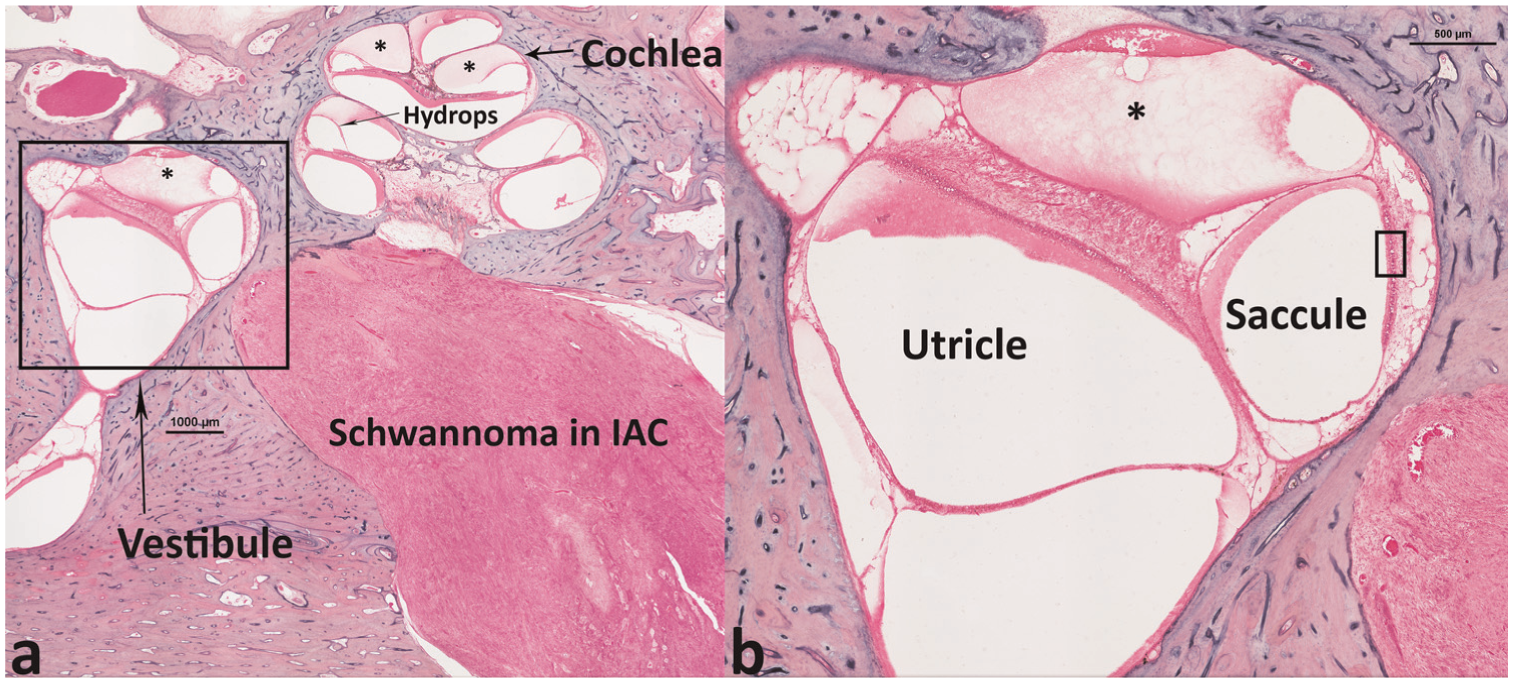
Light micrograph of the temporal bone from a 76-year-old man with left vestibular schwannoma (hematoxylin and eosin stain). (a) Tumor is present in the distal internal auditory canal. Hydrops and precipitate (*) are present in the cochlea and vestibule. (b) Magnified view of boxed area shown in panel a. Boxed area in panel b corresponds to Figure 1a. IAC, internal auditory canal.
The contralateral labyrinth was available as a control for quantitative hair cell assessment in 11 of 12 cases. The mean hair cell densities and mean difference for pairwise comparisons of vestibular hair cell density are presented in Table 2 . In some cases, the vestibular neuroepithelia were not sectioned in an appropriate plane for counting, thereby preventing a comparison between sides. The mean type I vestibular hair cell densities were approximately 60% lower on the side of the VS as compared with the contralateral ear in the lateral semicircular canal crista ampullaris (n = 9 pairs, P < .001), utricular macula (n = 10 pairs, P = .001), and the saccular macula (n = 11 pairs, P < .001). The density of type II vestibular hair cells was approximately 40% lower among ears with VS when compared with control ears in the lateral semicircular canal crista ampullaris (P < .001) and utricular macula (P < .001). There was no difference between affected and unaffected ears in the density of type II hair cells in the saccule (P = .463; Figure 1 ). The paucity of matched pairs of superior (2 pairs) and posterior (1 pair) semicircular canal cristae suitable for counting precluded statistical comparison, but the raw densities of vestibular hair cells were lower in the VS ear than in the control ears in each case.
Matched Pairs Analysis of Mean Type I and II Vestibular Hair Cell Densities.
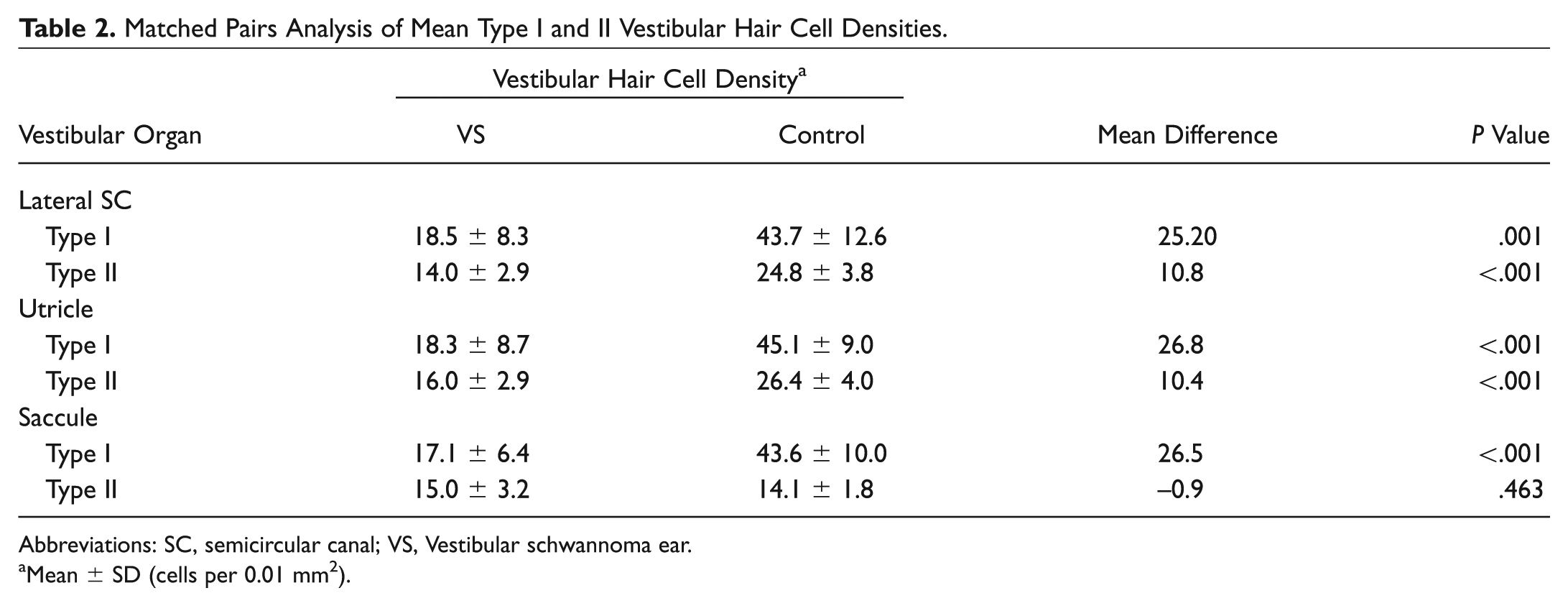
Abbreviations: SC, semicircular canal; VS, Vestibular schwannoma ear.
Mean ± SD (cells per 0.01 mm2).
Discussion
In this series of 12 VS cases, we observed that VS were associated with significant reductions (40%-60%) of ipsilateral vestibular hair cell density in the vestibular sensory neuroepithelia innervated by either division of the vestibular nerve. The potentially confounding effects of genetics, age, and systemic exposures were controlled by using the contralateral ears as the comparison group. We also observed significantly more hydrops and precipitate in the inner ear fluids among ears with VS. Our findings of vestibular labyrinthine pathology, including hair cell loss, hydrops, and inner ear fluid precipitate, are analogous to findings in the cochleae of ears with VS.12,13
Unlike previous qualitative descriptions of conventional light microscopic (LM) findings associated with VS, this study employed differential interference contrast microscopy in a quantitative analysis of the peripheral vestibular system. Hair cells and supporting cells are densely packed within the vestibular sensory neuroepithelia. Conventional light microscopy has insufficient resolution to reliably distinguish the morphologic characteristics of each cell type, including the stereociliary bundle and cuticular plate that are unique to hair cells, as well as the cell body and nuclear morphologies that distinguish type I from type II hair cells. 16 Given that all vestibular organs appeared morphologically normal in our series, it is not surprising that previous LM descriptions of the vestibular labyrinth in VS ears report normal-appearing maculae and cristae.6,9,10 While 1 LM report notes that the posterior crista appeared to be missing about 30% of its hair cells, no counts were performed. 9 In contrast, differential interference contrast microscopy permitted us to focus up and down through each slide at high magnification to create optical sections with high degrees of contrast that allowed for the differentiation of cell types. A similar series is not available for comparison, but in a chapter from a contemporary text that details the technique of quantitative peripheral vestibular otopathologic assessment, Merchant and McKenna describe the vestibular sensory epithelia in 2 cases of VS: one 94-year-old woman who had a mild decrease in hair cells in all 5 vestibular sensory organs while the density in the contralateral ear was normal for age, and an 81-year-old man in whom about 25% of the hair cells were missing in the ipsilateral cristae. 7 While the actual cell densities were not reported, our findings are consistent with their semiquantitative descriptions.
There are several potential mechanisms for the observed degeneration of vestibular sensory epithelia in ears with VS. Direct tumor invasion of any vestibular organ or the vestibular labyrinth was not observed in any of our cases and therefore is not likely to be causal. VS may compromise perfusion by blocking flow through the labyrinthine artery, thus causing ischemia and atrophy of downstream sensory organs.7,13 While we observed no occlusion of labyrinthine vessels, we cannot rule out this mechanism. Whether sensory nerve loss affects the fate of vestibular hair cells remains a matter of debate, 20 but in the single human study addressing this topic, vestibular hair cells were found to remain intact in 2 HTBs in which Scarpa’s ganglion cells had been destroyed by tumor metastases in the IAC. Hair cell degeneration occurred in a third case, but the presence of subneuroepithelial congestion caused the investigators to surmise that the loss resulted from labyrinthine ischemia rather than denervation. 21 Therefore, it is unlikely that vestibular nerve deafferentation explains our findings. The acidophilic precipitate observed in this study and others, along with increased protein concentrations detected in the perilymph,15,22 implicates VS-associated abnormalities of inner ear biochemistry. The etiology of increased protein concentrations remains unclear, with theories ranging from alterations in the blood-labyrinth barrier, 22 immune response to tumor antigens, 23 and obstruction of axonal transport of proteins through the compressed or infiltrated eighth nerve. 24 The protein appears to result in characteristic alterations in magnetic resonance imaging signal intensity in the cochlea and vestibule,25,26 and the degree of signal alteration in the cochlea is associated with pretreatment hearing levels in VS ears. 27 Given these cochlear pathologic correlates, proteins within the vestibule may contribute to (or be an epiphenomenon of another process that contributes to) hair cell loss by altering ion metabolism or through other unknown mechanisms. At the same time, we observed hair cell losses in HTBs without evidence of precipitate. Additional investigation will be necessary to further elucidate the cause of hair cell loss in the cochlea and vestibular labyrinth.
The presence of peripheral vestibular otopathology suggests that there may be labyrinthine as well as retrolabyrinthine sources of vestibular dysfunction in VS patients. Vestibular nerve compression and invasion by a slow-growing schwannoma might prompt gradual central compensation and mild symptoms. Alternately, positioning vertigo, 2 Meniere’s-like spells, 28 and severe vestibular crisis events 1 reported by some patients with VS may reflect more rapid changes in hair cell population, membrane alterations or collapse, or a mixture thereof. Peripheral pathology affecting all vestibular organs, as observed in this study, would also be expected to result in vestibular testing abnormalities regardless of the state of the afferent vestibular nerve division. Some attempts to preoperatively identify the tumor nerve of origin via caloric testing, vestibular-evoked myogenic potentials, and video head impulse testing found that the vestibular test profile does not often indicate selective nerve involvement 29 and that the pattern of test abnormalities does not always accurately predict the nerve of origin confirmed at surgery. 30 One explanation for these findings is that tumors compress or injure both divisions of the vestibular nerve as they grow. Diffuse end organ degeneration may also contribute to the level and distribution of dysfunction detected and would obfuscate nerve prediction efforts.
Our findings also have implications for the management of dizziness in VS patients with intact labyrinths. Unremitting vestibular symptoms may develop in patients who elect to observe their tumors. Labyrinth-level ablation, with intratympanic gentamicin31,32 or transmastoid labyrinthectomy without tumor removal, 33 has been reported as an effective strategy for treating disabling vertigo in such cases if vestibular rehabilitation efforts fail. Similar scenarios may arise after radiosurgery (ie, when the tumor remains in place and may still affect the peripheral vestibular system) or after partial surgical deafferentation (eg, after a hearing preservation surgery during which vestibular nerve fibers may be intentionally or unintentionally left behind in an attempt to preserve the cochlear nerve). In theory, ongoing degeneration of vestibular sensory epithelia may occur in such cases, creating an unstable peripheral vestibular lesion amenable to chemical or surgical labyrinthectomy.
This study has several limitations. Archival HTB studies are inherently limited by fixed sample sizes. Complete vestibular histories, electrophysiologic testing, and imaging results were not available for all subjects, impeding our ability to fully correlate findings with clinical manifestations. In particular, we were unable to determine if subjects with vestibular symptoms manifested greater degrees of labyrinthine pathology. Vestibular hair cell counts could be performed only in sensory organs that contained perpendicularly sectioned regions and had minimal postmortem autolysis that would otherwise obscure cell characteristics. The size of the cerebellopontine angle component of each tumor and the neuronal population in Scarpa’s ganglion could not be accurately assessed as a result of the standard HTB removal process. On the basis of the data available, we were also unable to explain the differential loss of type I versus type II hair cells in the saccule.
Conclusion
In conclusion, quantitative peripheral vestibular otopathology, manifested as reductions of vestibular hair cell densities, was identified in ears with VS. Labyrinthine as well as retrolabyrinthine pathology may contribute to tumor-related vestibular dysfunction and may be a target for ablative therapies for unremitting dizziness in patients with VS.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article
This article was accepted for presentation as a poster at the 2015 AAO-HNSF Annual Meeting & OTO EXPO; September 27-30, 2015; Dallas, Texas.