
Abstract

Cholesterol granuloma (CG) of the petrous apex (PA) may be asymptomatic or enlarge to cause symptoms from compression of neural and vascular structures within the temporal bone. Surgical decompression may then be indicated. We present a case of PA-CG where the feasibility of decompression with a minimally invasive per-meatal infracochlear approach was first assessed through 3-dimensional imaging and printing technology. Exemption was granted by the hospital’s Research Ethics Board.
Case Report
PA-CG was identified as an incidental finding on magnetic resonance imaging (MRI) of a 4.5-year-old boy during investigation for a febrile seizure. Although he remained asymptomatic, serial MRI obtained 19 months later revealed enlargement of the CG. Further evaluation with computed tomography (CT) demonstrated erosion of the internal auditory meatus and the boney wall of the intrapetrous carotid artery. Given this expansile growth and neurovascular encroachment, surgical drainage was considered.
The decision to proceed with surgery was predicated on an ability to minimize morbidity. Multiple corridors were considered, but transmastoid access was impeded by a large, anteriorly placed sigmoid sinus and transsphenoidal access, by the small size of the immature sinus and adjoining marrow and growth plates. Middle fossa and retrosigmoid approaches were considered too invasive for this asymptomatic child. A pneumatized infracochlear tunnel offered the prospect of an endoscopic per-meatal infracochlear approach, but it was uncertain whether the narrow pediatric external meatus would provide sufficient access. Three-dimensional modeling was employed to verify the feasibility and safety of this approach. First, multiplanar CT imaging was analyzed to confirm that the infracochlear tunnel could indeed be accessed along a per-meatal trajectory ( Figure 1 ). Next, a 3-dimensional printer (Spectrum Z510; 3D Systems, Rock Hill, South Carolina) was used to create a synthetic model of the patient’s temporal bone (material: ZP-131; binder: ZB-60) after the CT scan was segmented (Mimics and Magics software; Materialise, Plymouth, Michigan). The approach was then successfully trialed on a printed model ( Figure 2 ).
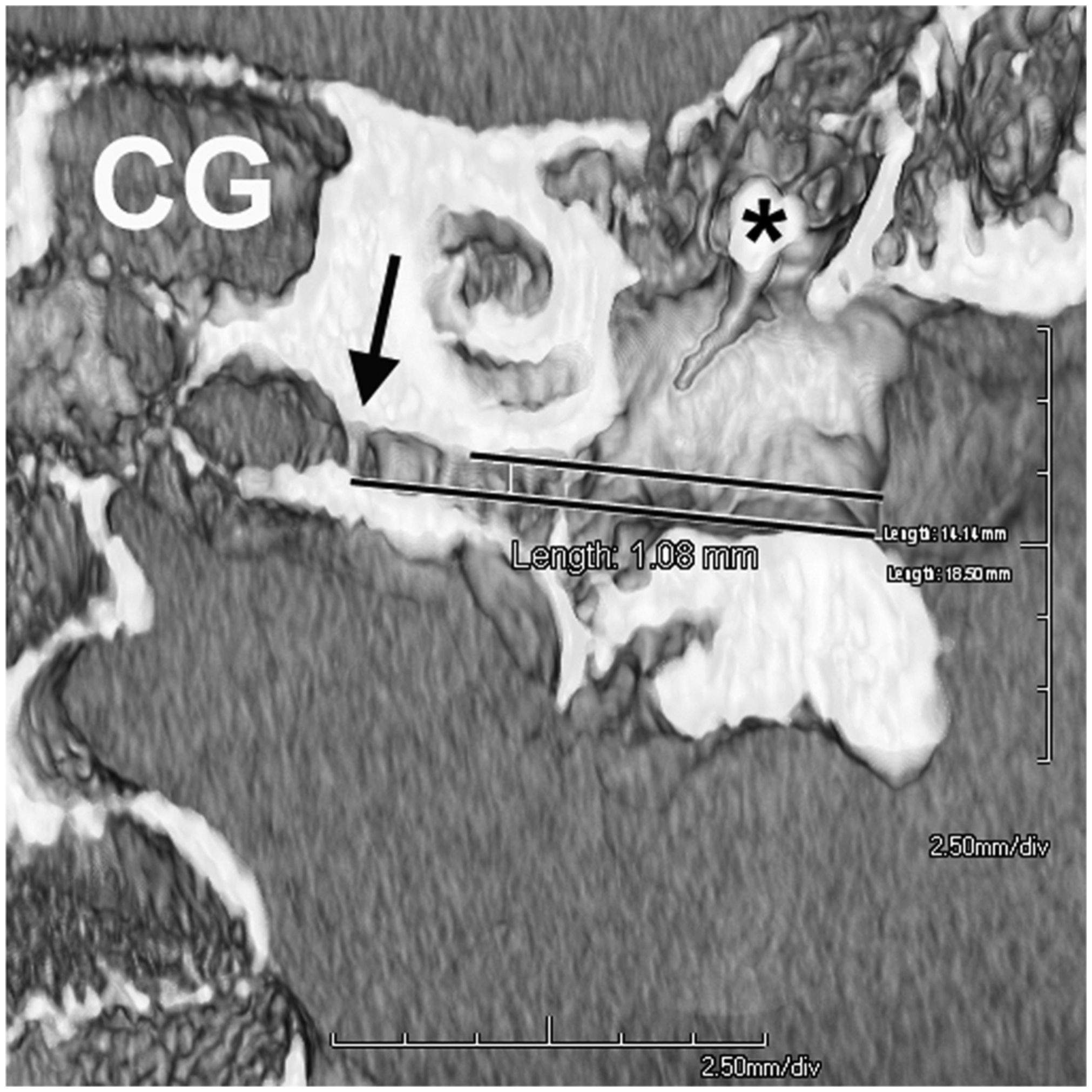
Paracoronal computed tomography reconstruction of the right temporal bone (facing anteriorly) predicting a 1-mm-wide per-meatal trajectory (parallel lines) toward the bony septation (arrow) between the infracochlear tunnel and the cholesterol granuloma (CG). Asterisk: malleus head.

View of right temporal bone model with 0
Parental consent to proceed with this approach was taken after careful explanation. A superiorly based tympanomeatal flap was elevated with a 0
The patient made a rapid recovery without complication. He remained asymptomatic, but subsequent MRI revealed reaccumulation of the CG and further expansion. At age 9 years, the procedure was repeated, again endoscopically with uncomplicated recovery, to widen the infracochlear tunnel with a Skeeter drill and insert a T-tube stent.
Discussion
Developments in endoscopic ear surgery allow the prospect of an even less invasive per-meatal approach to the PA than that provided by transsphenoidal surgery.1-3 Similarly, though, access may be restricted in children by smaller morphology, making the feasibility of this approach uncertain. Surface rendering of skull base imaging provides accurate representation 4 for preoperative evaluation (as Figure 1 ) but is not sufficient to predict the complex 4-dimensional interaction between movement of endoscope and instruments within the complex curvature of the ear canal. Three-dimensional printing provides an increasingly and widely available method of modeling temporal bone anatomy. 5 Our case demonstrates that this technology can be used to model surgery preoperatively with sufficient accuracy to confirm the feasibility of totally endoscopic pediatric ear surgery. Further study—for example, comparing measurements and interventions in cadaveric temporal bones with models—could be used to determine the limits of accuracy. This, with faster techniques for CT scan segmentation in preparation for printing and with wider clinical availability of printers, may allow 3-dimensional printing to become a valuable tool for routine preoperative planning and patient-specific preoperative training.
Conclusion
Totally endoscopic drainage through the infracochlear tunnel provides a truly minimally invasive option for PA-CG that is feasible even in childhood. As with other approaches, reaccumulation of PA-CG is a common challenge. Multiplanar image reconstruction and 3-dimensional printing can help determine feasibility of the approach in accordance with an individual’s ear canal morphology.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We thank Thomas Looi preparing the 3-dimensional temporal bone model.
No sponsorships or competing interests have been disclosed for this article.
This report was presented at the First World Congress of Endoscopic Ear Surgery; April 19, 2015; Dubai, United Arab Emirates.