
Abstract
Objective
(1) Integrate practice-based patient encounters using the Dartmouth Atlas Medicare database to understand practice treatments for Ménière’s disease (MD). (2) Describe differences in the practice patterns between academic and community providers for MD.
Study Design
Practice-based research database review.
Setting
CHEER (Creating Healthcare Excellence through Education and Research) network academic and community providers.
Subjects and Methods
MD patient data were identified with ICD-9 and CPT codes. Demographics, unique visits, and procedures per patient were tabulated. The Dartmouth Atlas of Health Care was used to reference regional health care utilization. Statistical analysis included 1-way analyses of variance, bivariate linear regression, and Student’s t tests, with significance set at P < .05.
Results
A total of 2071 unique patients with MD were identified from 8 academic and 10 community otolaryngology–head and neck surgery provider centers nationally. Average age was 56.5 years; 63.9% were female; and 91.4% self-reported white ethnicity. There was an average of 3.2 visits per patient. Western providers had the highest average visits per patient. Midwest providers had the highest average procedures per patient. Community providers had more visits per site and per patient than did academic providers. Academic providers had significantly more operative procedures per site (P = .0002) when compared with community providers. Health care service areas with higher total Medicare reimbursements per enrollee did not report significantly more operative procedures being performed.
Conclusion
This is the first practice-based clinical research database study to describe MD practice patterns. We demonstrate that academic otolaryngology–head and neck surgery providers perform significantly more operative procedures than do community providers for MD, and we validate these data with an independent Medicare spending database.
Ménière’s disease (MD) is among the more common and perplexing conditions encountered in otolaryngology, with a contemporary prevalence estimate of 190 cases per 100,000 people, or 0.20% to 0.27% of the population.1-3 The most prominent symptoms include acute episodes of vertigo lasting >20 minutes, as well as fluctuating hearing loss, tinnitus, and aural fullness. 4 These symptoms can become so severe as to incapacitate the patient, and they can recur in an unpredictable pattern. Risk factors identified include Caucasian ethnicity, female sex, age, and elevated body mass index.1,3 The treatment for MD is composed of both medical and surgical therapies. Medical management has historically consisted of maintenance or preventative therapy, as well as abortive therapy for acute attacks. Maintenance therapy consists of a low-salt diet and a diuretic. Abortive therapy includes benzodiazepines. Surgical management—which includes endolymphatic shunts, labyrinthectomy, and/or vestibular neurectomy—is reserved for medical treatment failures, often after attempt at control of vertigo with intratympanic gentamicin. Despite the pervasiveness of this condition, little has been published on possible geographic trends and health care resource utilization.
CHEER (Creating Healthcare Excellence through Education and Research) is a National Institutes of Health–funded, practice-based research network in otolaryngology–head and neck surgery comprising 30 provider sites in 19 states totaling >200 otolaryngologists, 100 audiologists, and 50 speech language pathologists. The goal of CHEER is to unite academic and community practices to facilitate practice-based research and quality improvement.
The objective of this study is to examine the CHEER network providers and their MD patients’ encounters to investigate possible local and regional variations in health care resource utilization in both academic and community settings. Specifically, we aim to determine if there are significant differences in the practice patterns between academic and community otolaryngology–head and neck surgery providers in the management of MD. A dated practice guideline exists for the evaluation and treatment of MD, 4 and we suspect that there may considerable variability in the surgical management employed in the treatment of MD. A national practice-based approach to these questions has yet to be attempted and will offer a broader scope of investigation as compared with a series from 1 center. These results would inform further research questions and studies on MD via a “big data” approach in conjunction with a practice-based network such as CHEER.
Methods
Provider Database and Patient Selection
This study was deemed research exempt by the Duke University School of Medicine Institutional Review Board. The CHEER network warehouses the Retrospective Data Collection (RDC) initiative, which contains 1 year of de-identified patient-level data from contributing sites and represents >260,000 unique patients and >650,000 unique encounters. All sites provided 1 year of patient data either from 2011-2012 or 2012-2013. A subset of MD patients from the RDC was created through International Classification of Diseases, Ninth Revision (ICD-9) and Current Procedural Terminology (CPT) code criteria that we developed. The ICD-9 codes utilized included 386.00 MD, 386.01 MD (cochleovestibular), 386.02 MD (cochlear), 386.03 MD (vestibular), and 386.04 inactive MD/MD in remission. The CPT codes utilized included 69801 transtympanic injection, 69805 endolymphatic sac decompression without shunt, 69806 endolymphatic sac decompression with shunt, 69910 labyrinthectomy with mastoidectomy, and 69915 vestibular nerve section. For patients identified as being diagnosed with MD, patient demographics, unique visits, visits per patient, and procedures per patient were tabulated. Procedures were coded first as MD-related procedures, and procedures that required invasive surgery were recoded into an operative procedures subgroup. For regional comparisons, the CHEER site locations were recoded into conventional northeast, south, midwest, and west descriptors. Moreover, site locations were further classified as “academic” if the provider site was contained within a university and as “community” if within a community or private clinic.
Dartmouth Atlas of Health Care Cross-reference
To integrate our patient-encounter level data with regional medical resource utilization metrics, each CHEER provider site was cross-referenced to a hospital service area (HSA) utilized in the Dartmouth Atlas of Health Care.5,6 The Dartmouth Atlas of Health Care utilizes a population-based small area analysis to present CMS Medicare data on a given population living in a defined geographic area or a specific hospital. For each health care service area, variables reported included total Medicare reimbursements per enrollee (2012 data) and surgeons per 100,000 HSA residents, by specialty (otolaryngology, 2006 data).
Statistical Analysis
Statistical analysis—including descriptive statistics, 1-way analyses of variance, bivariate linear regression, and Student’s t tests (2-tailed)—were conducted with the JMP Pro 11.2.1 software suite (SAS Institute Inc, Cary, North Carolina). Statistical significance was set at P < .05.
Results
Patient Population and Procedures
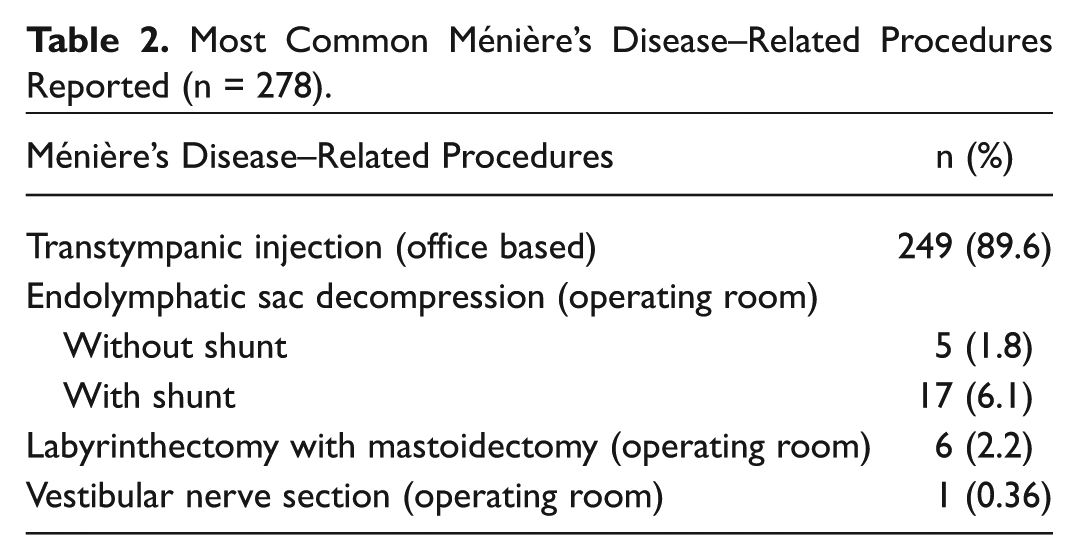
Per MD ICD-9 codes, 2071 unique patients and 6669 unique visits were identified. Only CHEER sites with MD encounters were included in subsequent analyses ( Table 1 ; n = 18). Eight (44.4%) sites were classified as “academic” and 10 (55.6%) as “community.” The average age of patients was 56.5 years. In all patients, the frequency of female sex was 63.9%, and the self-reported white ethnicity was 91.4%. There was an average of 3.2 visits per patient. A total 278 MD-related procedures were identified. The most common procedure reported was CPT 69801, transtympanic injection ( Table 2 ). We were unable to determine by CPT code if the transtympanic injection was delivery of steroid or aminoglycoside. For the purposes of analyses, operative procedures were classified as office based (intratympanic injection) or occurring in the operating room (endolymphatic sac decompression, labyrinthectomy, and vestibular nerve section).
Academic and Community CHEER Network Provider Sites and Corresponding Hospital Service Area Included in Study.
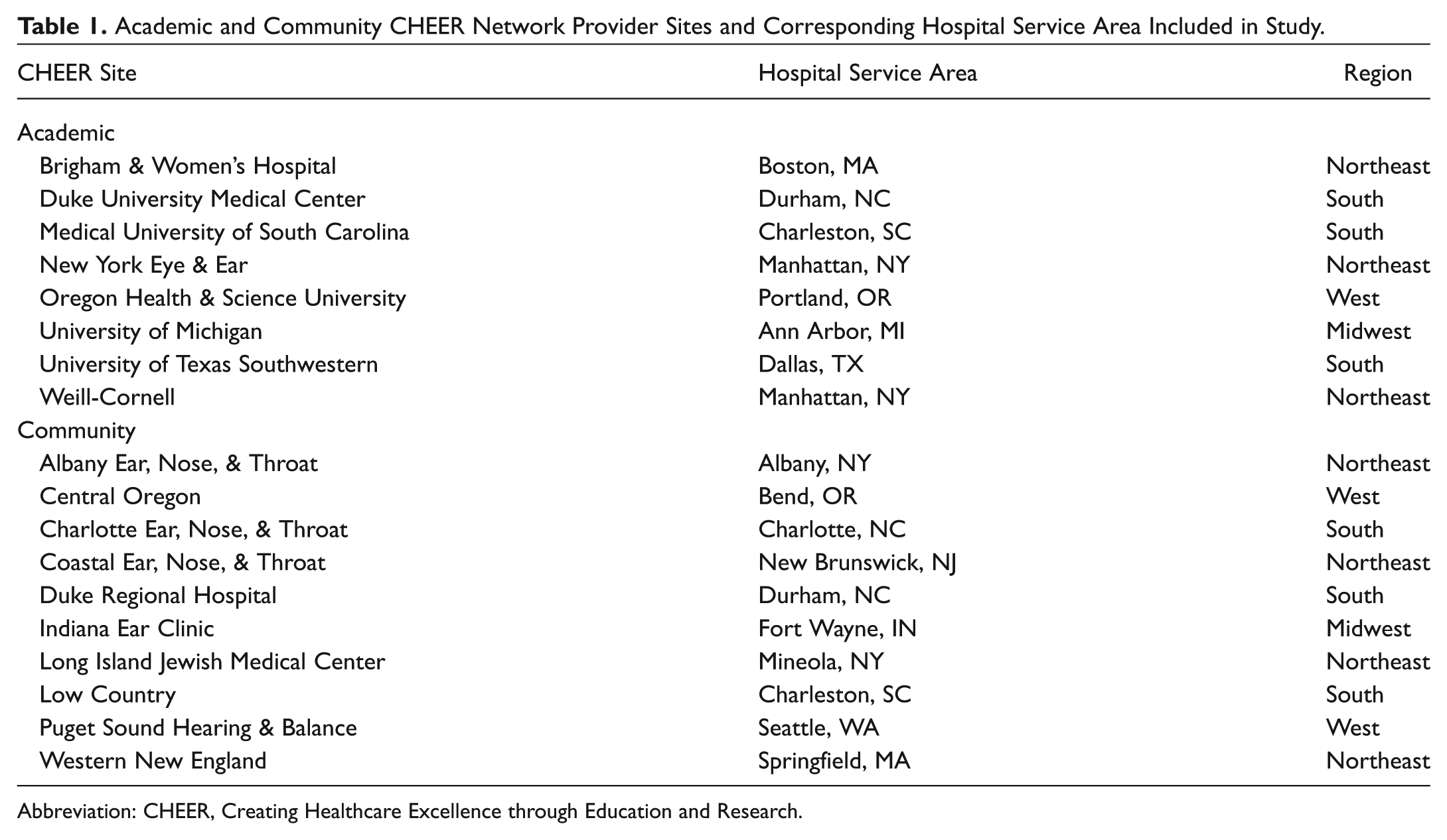
Abbreviation: CHEER, Creating Healthcare Excellence through Education and Research.
Most Common Ménière’s Disease–Related Procedures Reported (n = 278).
Academic and Community Site Trends
There was no significant difference in mean encounters per patient between community and academic sites ( Table 3 ). There were no significant differences in academic and community sites with either the number of any type of procedure per patient (0.35 vs 0.14; P = .14) or intratympanic injection procedures per patient (0.08 vs 0.10; P = .70). However, academic sites had a significantly higher number of operative procedures per site when compared with community sites (5.2 vs 0.63; P = .0002). When academic and community sites were compared with the Dartmouth Atlas variables, no significant differences were observed in total Medicare Reimbursements per enrollee and the number of Medicare enrollees who visit a primary care clinician annually. Moreover, no significant differences between site types were observed when health care physicians, surgeons, and otolaryngologists per 100,000 residents in each HSA were compared.
One-way Analysis of Variance Comparisons of Academic and Community Provider Patient Encounters: Procedures and Dartmouth Atlas Database Variables.
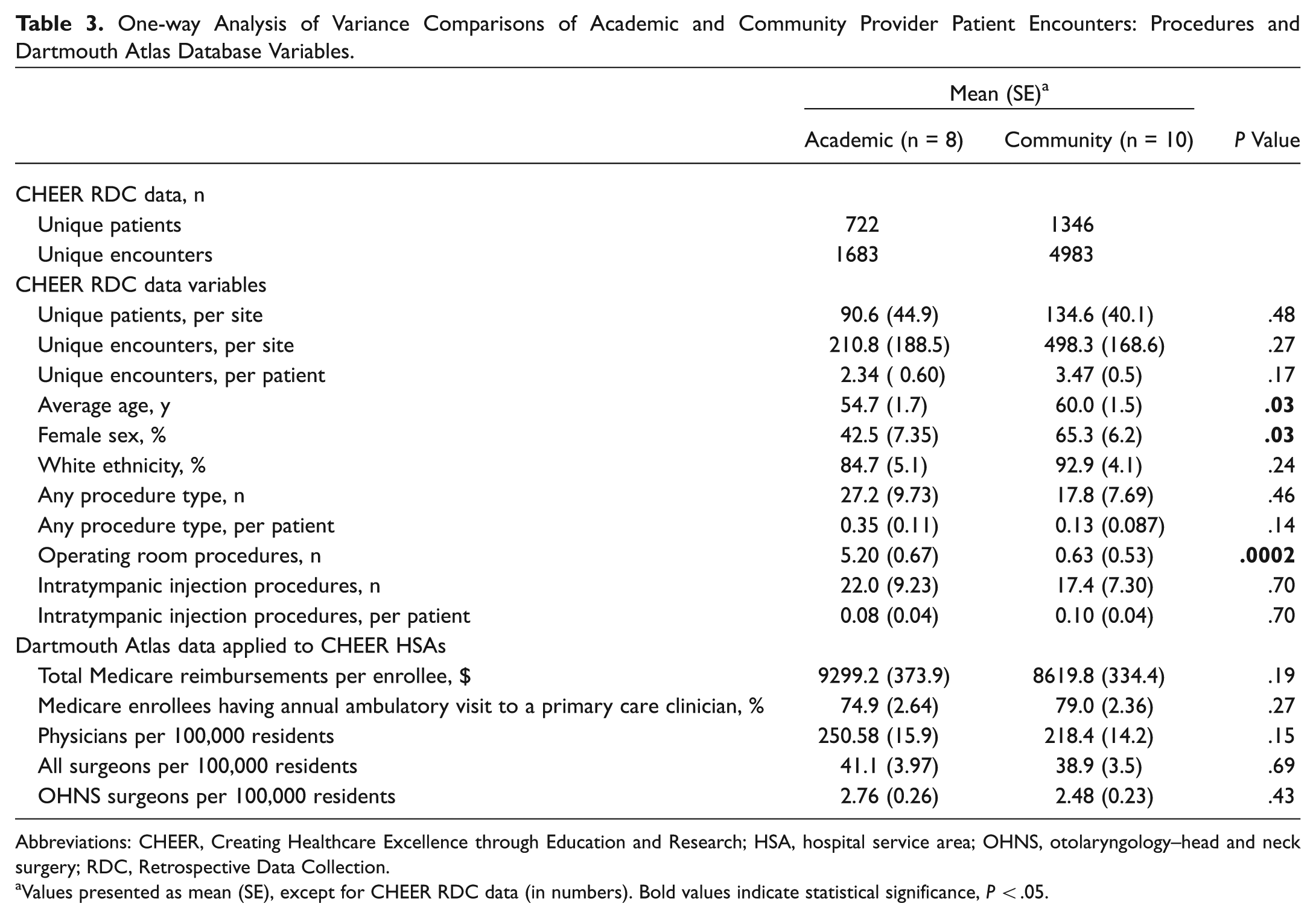
Abbreviations: CHEER, Creating Healthcare Excellence through Education and Research; HSA, hospital service area; OHNS, otolaryngology–head and neck surgery; RDC, Retrospective Data Collection.
Values presented as mean (SE), except for CHEER RDC data (in numbers). Bold values indicate statistical significance, P < .05.
Regional Site Variation
When the CHEER sites were recoded into their corresponding regions, we observed that the western region providers had the highest average visits per patient ( Table 4 ). Midwest providers had significantly higher average procedures per patient versus the next-highest procedural region (0.72 vs 0.09; P = .007). There were no other significant differences between the regions when comparing the other variables in the table (not shown). The CHEER regions were cross-referenced with Dartmouth Atlas variables, including the 2012 total Medicare reimbursements per enrollee (adjusted for price, age, sex, and race), the percentage of Medicare enrollees with an annual primary care clinician, and the number of physicians, surgeons, and otolaryngology–head and neck surgery surgeons per 100,000 residents ( Figure 1 ). There were no other significant differences among the regions when comparing these variables of a region with the lowest value and the region with the next highest value (not shown).
Descriptive statistics of regional designations of CHEER site patient encounters and procedures data.
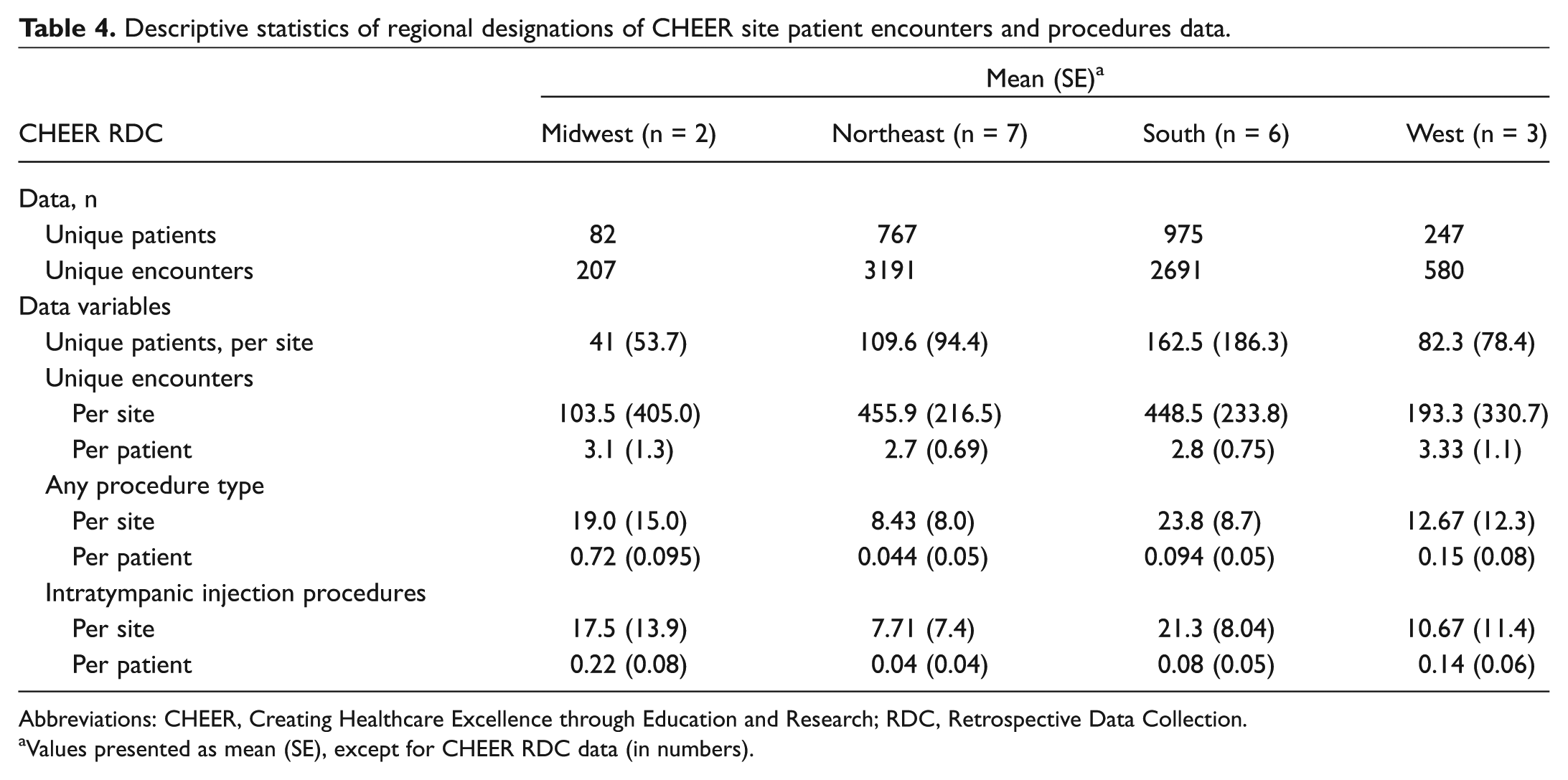
Abbreviations: CHEER, Creating Healthcare Excellence through Education and Research; RDC, Retrospective Data Collection.
Values presented as mean (SE), except for CHEER RDC data (in numbers).
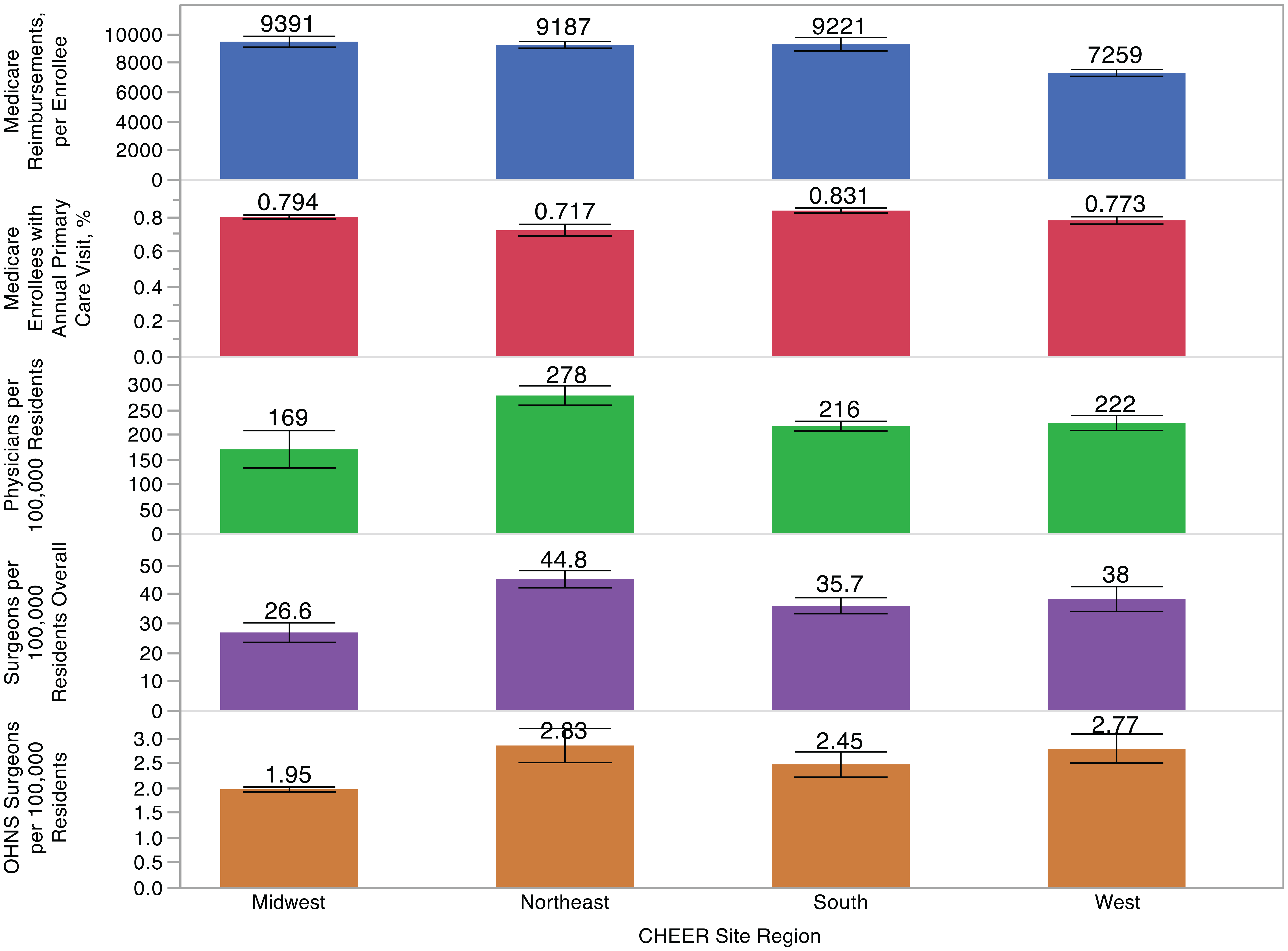
Comparisons of regional designations of CHEER sites with cross-referenced Dartmouth Atlas database variables. Error bars represent 1 measure of standard error. CHEER, Creating Healthcare Excellence through Education and Research.
Dartmouth Atlas Cross-reference
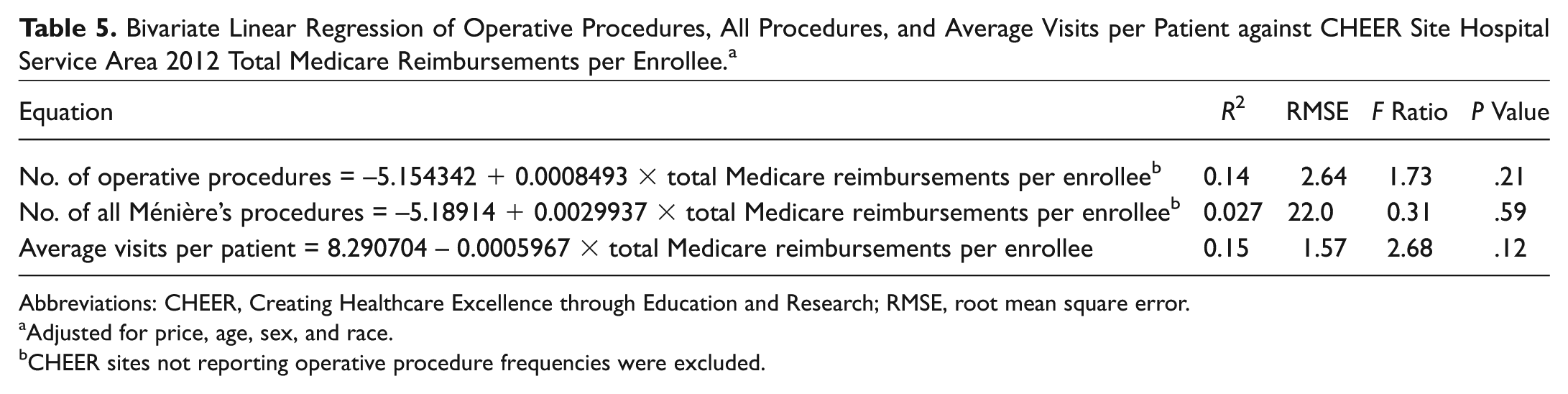
Bivariate linear regressions were performed to assess for correlation between 2012 total Medicare reimbursements per enrollee (adjusted for price, age, sex, and race) and operative procedures, all procedures, and average visits per patient for all CHEER site HSAs ( Table 5 ). Medicare reimbursement was not a statistically significant predictor of number of operating room procedures (data not shown), aggregate of both operative and procedures, and average visits per patient (data not shown).
Bivariate Linear Regression of Operative Procedures, All Procedures, and Average Visits per Patient against CHEER Site Hospital Service Area 2012 Total Medicare Reimbursements per Enrollee. a
Abbreviations: CHEER, Creating Healthcare Excellence through Education and Research; RMSE, root mean square error.
Adjusted for price, age, sex, and race.
CHEER sites not reporting operative procedure frequencies were excluded.
Discussion
The management of MD is generally composed of both medical and surgical interventions depending on the patient’s severity of illness. To date, there are no formal clinical practice guidelines focused on management of these patients, as there are with other otologic conditions, such as tinnitus, 7 acute otitis externa, 8 sudden sensorineural hearing loss, 9 and Bell’s palsy. 10 For MD, there is only a committee document that provides guidance regarding the diagnosis and evaluation of MD patients. 4 Furthering our understanding of MD practice patterns may provide an opportunity for quality improvement that may inform the discussion for development of a guideline for the management of the MD patient. To be informative, a broad and generalizable analysis of otolaryngology provider management patterns is needed. This is the first practice-based clinical research database study to describe trends in the practice patterns related to MD.
The patients reported in our database of 8 academic and 10 community provider sites had a demographic profile similar to that previously published in other contemporary reports on MD, with most being of non-Hispanic white race and female sex. 1 Our academic and community sites did not differ in the self-reported ethnicity, the number of visits, or the number of tympanic injection procedures per patient. Community sites had a significantly older and higher proportion of female patients, as compared with academic sites. The clinical significance of these demographic differences is likely inconsequential.
We discovered that academic sites had a significantly higher mean number of operating room procedures per site. Both gentamicin injection and surgical therapy for MD have been shown to be very effective in the resolution of vertigo symptoms.11-13 As such, insurance providers will reimburse gentamicin injections, endolymphatic sac decompression procedures, lateral semicircular canal plugging, sacculotomy, vestibular nerve decompression, vestibular nerve section, and labyrinthectomy in the treatment of MD. 14 Inclusion criteria that must be met include patients who have disabling vertigo and symptoms for ≥2 years and have failed conservative medical therapy. While most community otolaryngology practices have operating room privileges at an ambulatory surgery center or hospital, it is possible that this is not the case universally. It is also plausible that community providers may elect not to perform an endolymphatic sac decompression, labyrinthectomy, or vestibular nerve section and instead refer patients into academic centers for these procedures, thus concentrating their prevalence at these sites. Our data do not furnish information on disease severity, so we cannot infer about the complexity of MD cases that our community providers observed versus their academic counterparts. While we cannot specifically determine why the population is different on some constructs in these data, the differences support the need for guidelines that are unique to patients and that address provider site type, capacity, as well as specialized training for providers performing more invasive surgical therapy. These findings may reinforce emphasis of future studies of operative procedures toward academic settings, while the study of diagnoses and nonoperative procedures is pertinent to both academic and community provider settings.
The Dartmouth Atlas of Health Care is an innovative database that highlights regional trends in Medicare spending and health care utilization.5,6 In this new era of health care, analysis of health care utilization is prudent when considering priorities for resource allocation. As MD is a challenging condition with effective therapies both noninvasive and invasive, we sought to determine if health care regions of high spending are associated with a higher frequency of more expensive and more invasive therapies. To our knowledge, our study is the first to attempt to cross-reference the Dartmouth Atlas data set with an independent otolaryngology data set. When we coupled our database to the Dartmouth Atlas database, we found that CHEER sites who belong to HSAs with higher total Medicare reimbursements per enrollee did not report significantly more operative procedures being performed. There was also no significant relationship between the number of all procedures and the average number of visits with HSA total Medicare reimbursements. This may mean that (1) low-spending regions are performing as many operative procedures and/or (2) patients requiring operative intervention are not being preferentially referred to provider sites in higher-spending regions. Based on our data and the widely accepted evidence for the efficacy of surgical therapy, it is unlikely that CHEER sites in HSAs with high Medicare reimbursements are performing superfluous or “unnecessary” volumes of operative or office-based procedures.
This study has limitations that need to be considered. Our inferences on the provider sites’ data are only as strong as the data. The RDC includes the most recently available year of data from each contributing site and the maximum number of diagnosis and procedure codes that each site can provide. The earliest RDC year-start date is January 2011, and the latest year-end date is May 2013. We made no attempt to balance academic and clinical sites within a region when constructing the CHEER network. Although our network covers all geographical regions of the United States, there is variability as regard clinical or academic practices within regions. The CHEER RDC database includes a year’s worth of de-identified data from contributing sites in the CHEER network. We assume that the encounters, diagnoses, and procedures are only a subset of the total patient population. We are unable to describe the severity of MD by the ICD-9 code identification and whether patients have sought prior treatment elsewhere. We must also note that we are limited to the description of the procedures by their representative CPT codes. As stated previously, we cannot determine the therapeutic ingredient used for transtympanic injections. Although the data are from limited sites within different geographic regions, the findings suggest that there may be a shift away from more invasive surgical procedures, such as transmastoid labyrinthectomy, to a more limited invasive procedure of a transtympanic injection.
For this given study, not all sites with data in the RDC had the appropriate patient population to be included. The CHEER RDC was not developed with the goal of regional representation for all conditions, which would be difficult in otolaryngology. Additionally, CHEER comprises both community and academic sites of various sizes. The sites in the northeast and south constituted the majority of the sites included in the analysis (13 of 18). The sample sizes of sites and volumes are provided in the regional analysis. We are currently embarking on updating the RDC with more recent data and expanding and enhancing the number of the fields collected. As “big data” and registries become integrated into performance and quality metrics, studies such as ours can help educate on the limitations and methodologic approaches for analyses. Ours is an administrative data set without rigor in enforcing consistency in reporting, and it provides an appropriate source for descriptive analyses and the basis for further investigation and research. This study is also informative as we move in health care toward performance, quality, and reimbursement based on “big data.” This study appropriately identifies limitations of the database while describing potential opportunities for addressing variation in practice and treatment options for MD. As registries and other “big data” sources are being developed and utilized, limitations identified in studies like this one can be used in their development, as well as in supporting the need for multidimensional performance and reimbursement algorithms.
With regard to our health care utilization analyses, debate has been raised about the validity of the Dartmouth Atlas data. The Dartmouth Atlas seeks to highlight high-spending HSAs inferred from total Medicare reimbursements. One major argument is that certain hospital referral regions will accrue “sicker” patients, thus justifying their higher care expenditure. The Dartmouth Atlas authors have tried to mitigate this potential bias by accounting for age, race, sex, and local price of care. 15 An additional limitation is our ad hoc merge of the Dartmouth Atlas administrative data set with our practice-based CHEER network data. As the Dartmouth Atlas data have not been explicitly designed to merge seamlessly with other data sets, this could introduce an element extrapolation to our conclusions. We also cannot assume that each CHEER site is representative of the HSA and larger hospital referral regions in which they are embedded. This limits our ability to generalize health care expenditure trends to the larger geographic subdivisions that we list.
This is the first practice-based clinical research database study to describe trends in the practice patterns in MD management. We demonstrate that academic otolaryngology–head and neck surgery providers perform significantly more operative procedures for MD patients than do community providers. Reasons for this difference include possible operating room availability or access, otolaryngologist training, severity of patient illness, or possible operative case referral. As these operative procedures are reported to be very effective in the management of refractory MD, more detailed investigation into the practice patterns of academic and community providers will be fruitful in further determining drivers for this difference. It is well understood that variation in health care often leads to inefficient health care utilization of resources and waste. In demonstrating that there is a degree of variation within the management of MD across different provider centers and types, we highlight an opportunity to improve care delivery while describing potential opportunities for addressing variation in practice and treatment options for MD. Specifically, we hope that this work may inform discussion on whether a national guideline for the management of MD patients would prove useful, as this often burdensome condition can be effectively treated with appropriate medical and surgical therapy.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We acknowledge Anne Wolfley and Rhonda Roberts of the Duke Clinical Research Institute for their contribution in data acquisition and analysis. We acknowledge all of the CHEER network sites that contribute data to the Retrospective Data Collection.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.