
Abstract
Objective
Pediatric dysphagia occurs in 500,000 children each year; however, there is not a common tool to assess these children. Our aim was to identify validated patient- or parent-reported outcome assessment tools evaluating pediatric dysphagia.
Data Sources
Scopus, EMBASE, PubMed, Cochrane Library, and CINAHL electronic databases (all indexed years through August 2014).
Review Methods
Inclusion criteria included English-language articles containing instruments evaluated in children. Two investigators independently reviewed all articles, and the review was performed according to PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-analyses).
Results
The initial search yielded 1697 abstracts; 158 studies were assessed further. Four symptom questionnaires, validated in adults, were used to report pediatric dysphagia outcomes. Four outcomes tools assessing dysphagia were validated in pediatrics in selected populations. The Dysphagia in Multiple Sclerosis questionnaire and the Dysphagia Symptom Questionnaire for eosinophilic esophagitis were validated in adolescents and adults. The Symptom Questionnaire for Eosinophilic Esophagitis was validated in children with eosinophilic esophagitis. The Pediatric Quality of Life Inventory Gastrointestinal Symptoms Module, validated in children with gastrointestinal disorders, includes 2 domains that assess swallowing function.
Conclusion
We did not identify any validated patient- or parent-reported outcome assessment tools examining dysphagia symptoms in a general pediatric population. However, we identified 4 questionnaires that have been validated in specific pediatric disease cohorts. Having a standardized assessment instrument validated in all children would allow clinicians to systematically report symptoms and compare results of pediatric clinical trials. With this in mind, we recommend establishing a standard questionnaire for the broader pediatric population.
Swallowing disorders, including both oropharyngeal and esophageal dysphagia, affect an estimated 500,000 children per year in the United States. 1 Higher rates of oropharyngeal dysphagia are reported in children with upper aerodigestive tract lesions, craniofacial syndromes, central nervous system anomalies, and developmental delays, as well as in preterm infants.2-4 With the recent increase in preterm births and the increasing survival rates of infants with complex medical conditions, the number of affected patients seen in pediatric clinical practice has also increased.2,4,5
Although a number of studies have proposed evaluation and treatment algorithms for patients with oropharyngeal dysphagia, there are currently no widely accepted protocols. Most clinical assessment focuses on identifying aspiration by radiographic studies or establishing the etiology of dysphagia, primarily through fiberoptic endoscopic evaluation of swallowing. Although these approaches evaluate the mechanics and safety of the swallow, they do not provide a robust assessment of the child’s symptoms, nor do they measure the impact of dysphagia on the physical or emotional well-being of the child.
The use of outcome assessment instruments such as symptom questionnaires or quality-of-life measures allow for direct assessment of patient symptoms and measurement of the psychosocial impact of the disease process. Such instruments have been effectively used in the assessment of health-related quality of life in general pediatric patients and in children with a broad spectrum of otolaryngologic disease, including otitis media, rhinitis, adenotonsillar disease, obstructive sleep apnea, and dysphonia.6,7
Although a number of metrics examining dysphagia have been validated in adults,8-14 there is no standard for symptom assessment in dysphagic children. Through the use of standardized assessment tools, patient symptoms, disease activity, and efficacy of treatment can easily be tracked and more rigorous clinical research conducted. With this in mind, we performed a systematic review of the existing literature to identify dysphagia-specific outcome assessment tools that included symptom assessment and were validated in children. This review serves as the first step in directing future research to establish a standardized metric for evaluating pediatric dysphagia.
Methods
This systematic review was conducted in the manner specified in the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-analyses). 15 The PRISMA flowchart can be found in Figure 1 . This study was exempt from evaluation by the institutional review board.
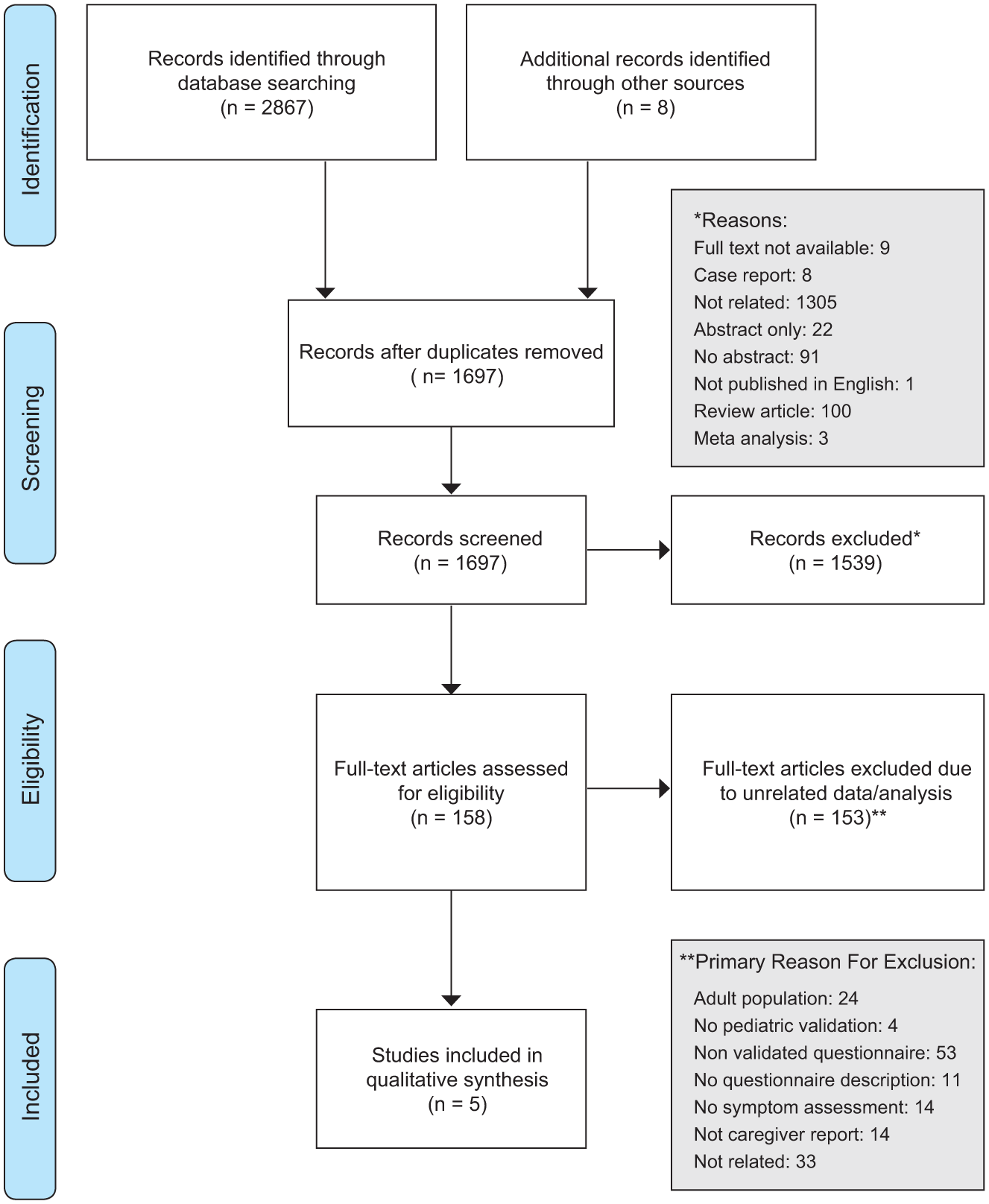
PRISMA diagram for article selection and inclusion in the systematic review of patient-reported pediatric dysphagia assessment.
Search Strategy
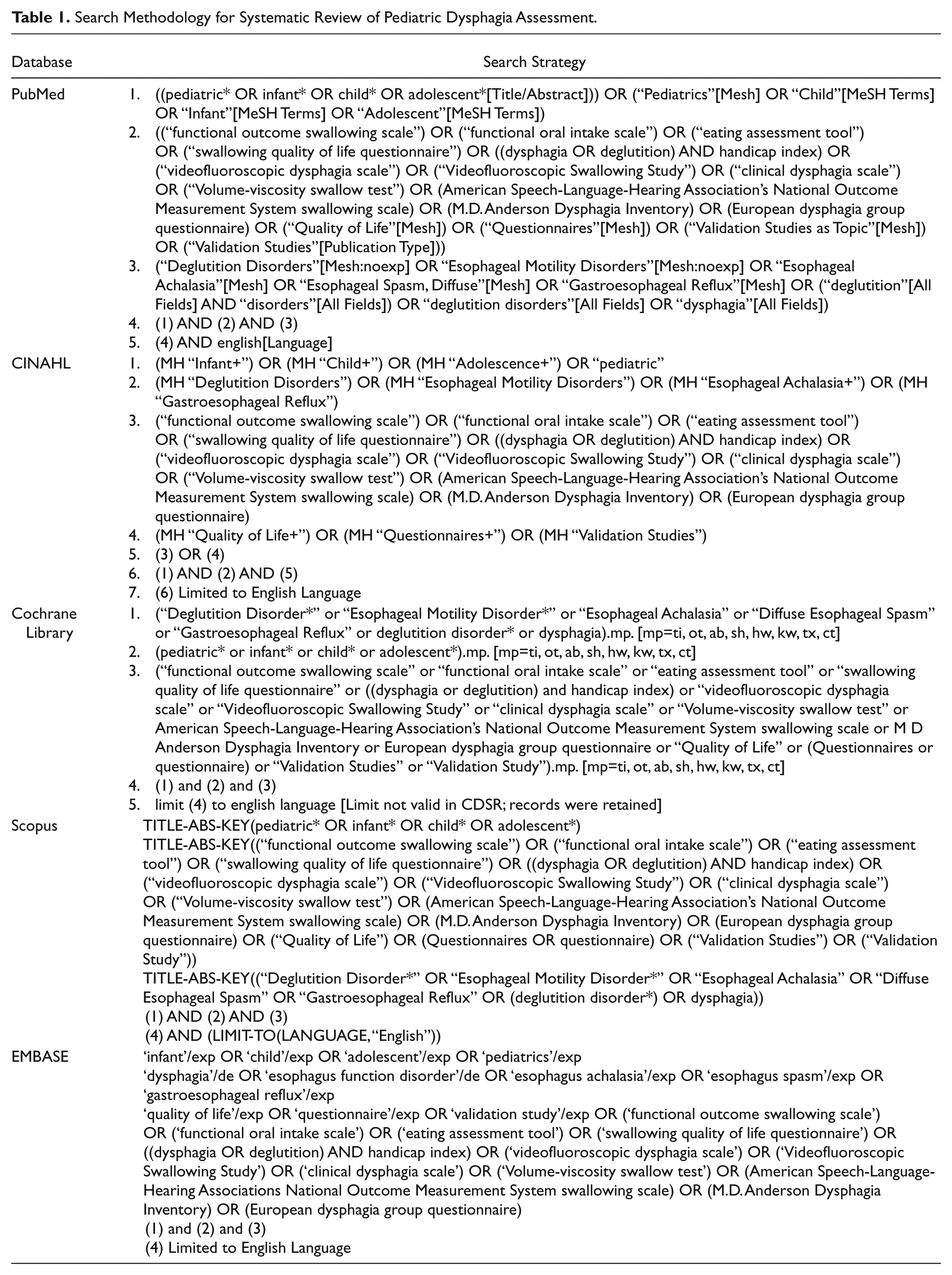
Our search was conducted in the following databases: PubMed (1950–August 26, 2014), Scopus, CINAHL (1982–August 26, 2014), Cochrane Library (2001–August 26, 2014), and EMBASE (1945–August 26, 2014). The electronic search strategy was designed and tailored for each database by a medical librarian. The search used combined key terms and Medical Subject Headings as shown in Table 1 .
Search Methodology for Systematic Review of Pediatric Dysphagia Assessment.
Study Eligibility
All identified titles, abstracts, and full-text articles were independently reviewed by 2 investigators to determine if studies met the established inclusion criteria—namely, each study must evaluate an instrument that assessed dysphagia symptoms, include children <18 years of age, contain an abstract, be published in English, and include >2 subjects. Review articles and practice guidelines were reviewed to determine if additional studies should be included in the present review. Abstracts and conference posters were excluded, as were studies that focused on the evaluation of gastroesophageal reflux disease.
For articles on which there was disagreement regarding inclusion in the study, reviewers met to reach a consensus on inclusion or exclusion.
Data Extraction and Quality Assessment
Information obtained from each article included authors, year of publication, questionnaire or instrument used, targeted patient population, study population, study design, and reported validation measures. Extracted validity and reliability measures included content validity, construct validity, discriminant validity, internal consistency, responsiveness to change, reproducibility, and test-retest reliability. Criterion validity was excluded given the absence of a “gold standard” for dysphagia. Additional searches were performed for each included questionnaire, for further validation or translation. Although guidelines for assessing the quality of measurement instruments for systematic reviews have been reported, 16 there is currently no widely used standard. As the included studies comprised heterogeneous study populations and different assessment tools, integration of the data was not performed.
Results
The initial search identified 1697 abstracts, with 158 selected for eligibility screening. Of these 158 articles, only 5 articles describing 4 questionnaires met our inclusion criteria for qualitative synthesis. Table 2 presents the key characteristics of each questionnaire. Of the excluded studies, 4 reported outcomes for pediatric patients using instruments validated only in adults.17-20
Questionnaires Included in the Systematic Review of Dysphagia-Specific Outcome Measures: Patient or Parent-Proxy Reported.
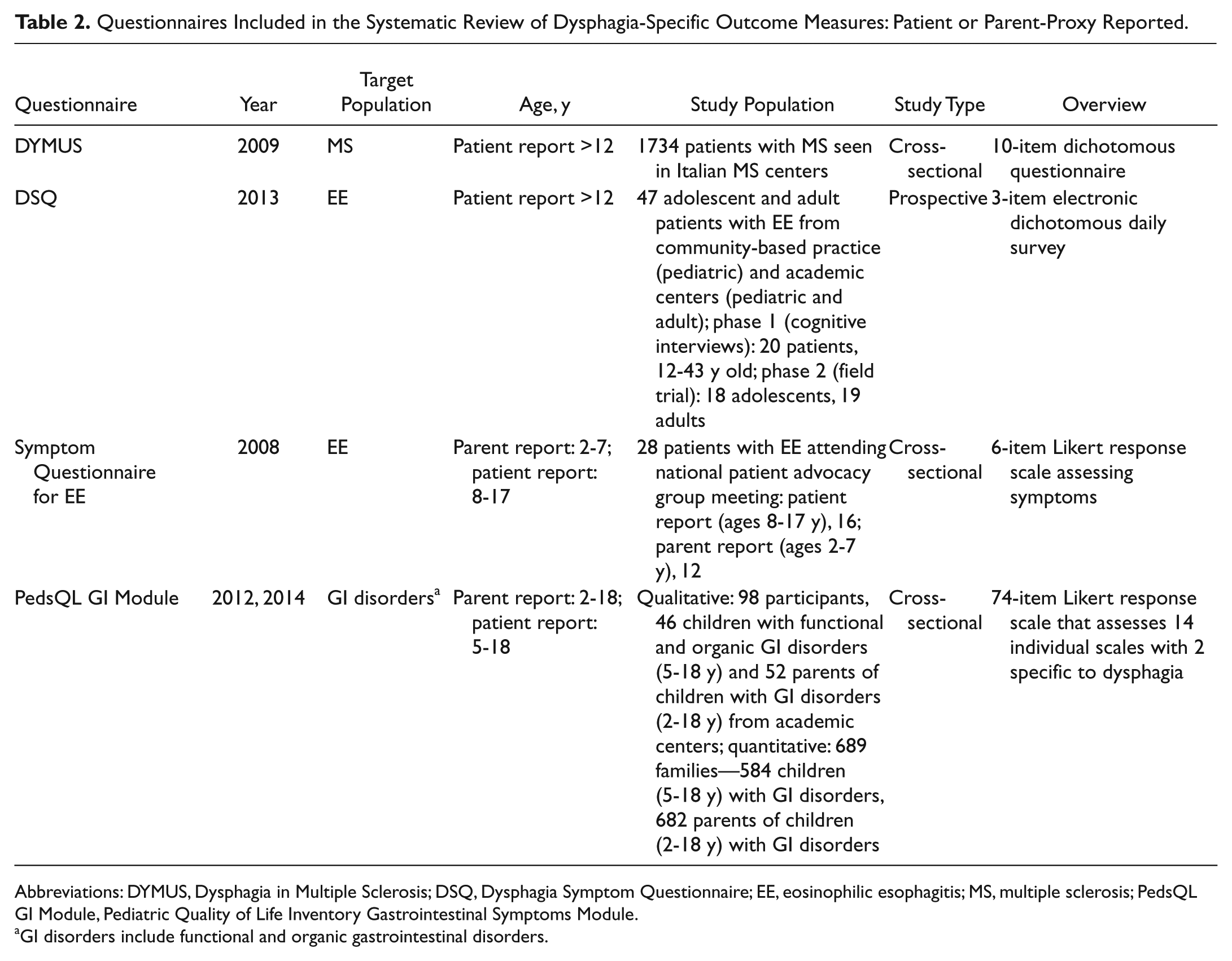
Abbreviations: DYMUS, Dysphagia in Multiple Sclerosis; DSQ, Dysphagia Symptom Questionnaire; EE, eosinophilic esophagitis; MS, multiple sclerosis; PedsQL GI Module, Pediatric Quality of Life Inventory Gastrointestinal Symptoms Module.
GI disorders include functional and organic gastrointestinal disorders.
Bergamaschi et al 21 reported on the validation of the Dysphagia in Multiple Sclerosis (DYMUS) questionnaire. This previously developed 10-item patient-completed questionnaire 22 was developed as a screening tool for dysphagia and to follow dysphagia symptoms longitudinally in patients with multiple sclerosis. The DYMUS includes questions regarding difficulty swallowing, coughing with ingestion, weight loss, and modifications to eating behavior; however, there is no assessment of psychosocial domains. Validation testing showed good internal consistency (Cronbach’s alpha = 0.914). Additionally, when the DYMUS was divided into subscales of dysphagia for liquids and dysphagia for solids, good internal consistency was maintained (Cronbach’s alpha = 0.864, 0.885, respectively). Although the study population for validation included adolescents (age range starting at 12 years), the mean age of participants was 43.4 years. No further specific information regarding the adolescent cohort was reported. The DYMUS has since been translated and validated in an multiple sclerosis cohort in Brazil 23 ; however, our search did not yield any reports of its validation in other populations.
The Dysphagia Symptom Questionnaire (DSQ) 24 is a 3-item patient-completed electronic questionnaire designed for daily reporting of oral intake. The DSQ was developed to serve as a symptom diary for patients with eosinophilic esophagitis. This questionnaire assesses dysphagia solely through queries regarding difficulty with the intake of solid food, with no assessment or measurement of psychosocial domains. The study population included adolescents and adults, with 48% of participants (18 of 37) ranging in age from 12 to 17 years. Authors reported a strong correlation of the DSQ score both with the number of days that patients reported dysphagia (P < .001) and with the Straumann Dysphagia Index (SDI; P < .001). Our search revealed no additional validation studies.
The Symptom Questionnaire for Eosinophilic Esophagitis 25 was designed to assess globus, odynophagia, and difficulty swallowing solids and liquids for patients with eosinophilic esophagitis ranging in age from 2 to 18 years; it does not include assessment of psychosocial domains. For children <8 years of age, the questionnaire is completed by the parent. This article described the development of the survey, reporting face and content validity; however, no psychometric evaluation of construct validity, internal consistency, or reliability was performed. An additional search did not identify any further validation publications.
The Pediatric Quality of Life Inventory Gastrointestinal Symptoms Module (PedsQL GI Module)26,27 consists of 74 items that encompass individual scales for stomach pain, stomach discomfort, food and drink limits, trouble swallowing, heartburn and reflux, nausea and vomiting, gas and bloating, constipation, blood in feces, worry about defecation, worry about stomachaches, medicines, and communication. Six items assess food and drink limitations, whereas 3 assess dysphagia symptoms. The PedsQL GI Module has been validated for patients with gastrointestinal disorders, with patient-reported (5-18 years old) and parent-proxy questionnaires available (2-18 years old). Authors reported high internal consistency for child- and parent-reported information (Cronbach’s alpha = 0.97) and construct validity with the PedsQL 4.0 health-related quality of life (P < .001). Each scale can be used in a stand-alone fashion.
Table 3 summarizes the reported psychometric measures for each outcome instrument. Content validity was clearly described for each tool, and construct validity was reported for the DYMUS, DSQ, and PedsQL GI module. Only the DYMUS and the PedsQL GI module measured internal consistency. No study reported responsiveness to change, test-retest reliability, or reproducibility for the described instruments.
Reported Validation Measures in the Systematic Review of Dysphagia-Specific Outcome Measures: Patient or Parent-Proxy Reported. a
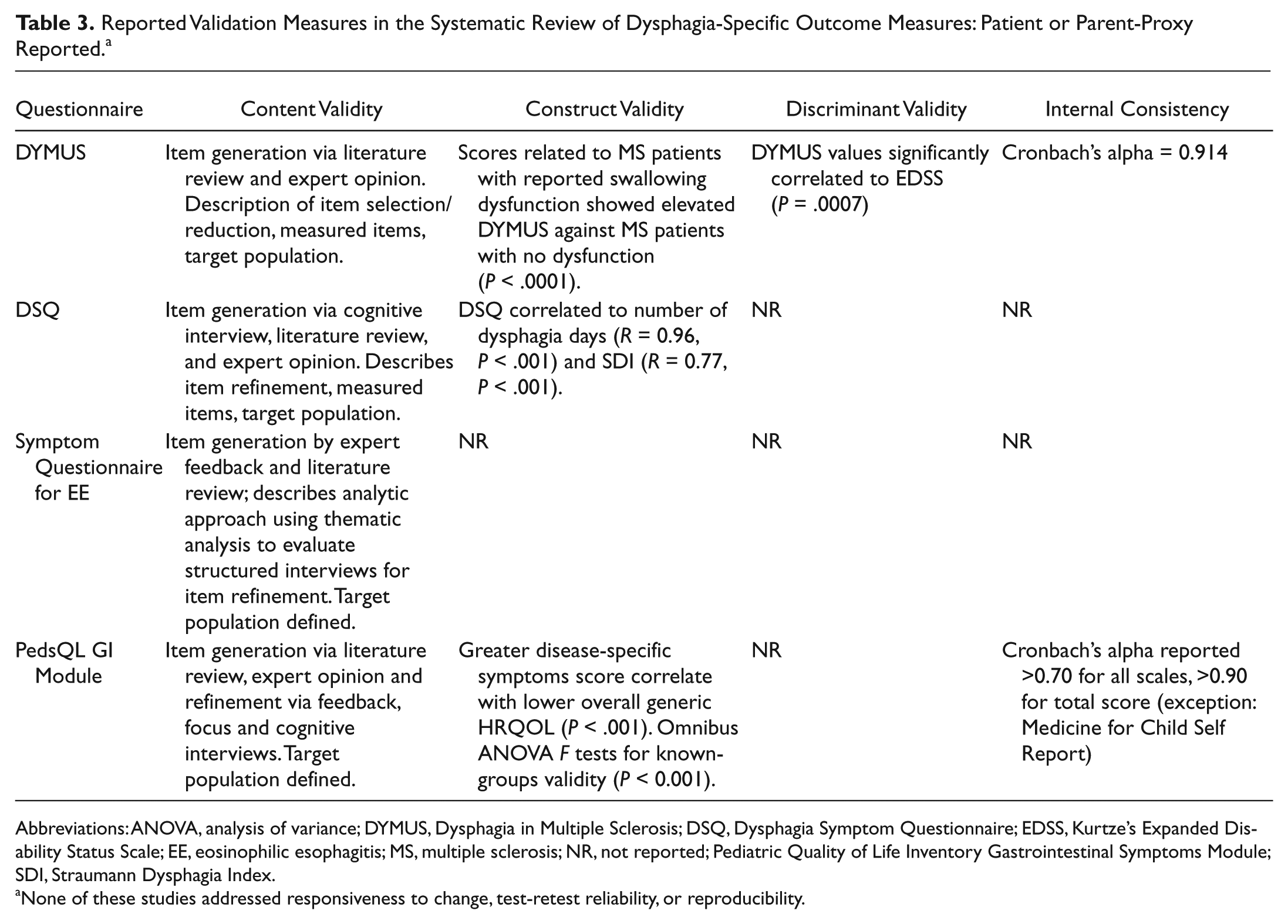
Abbreviations: ANOVA, analysis of variance; DYMUS, Dysphagia in Multiple Sclerosis; DSQ, Dysphagia Symptom Questionnaire; EDSS, Kurtze’s Expanded Disability Status Scale; EE, eosinophilic esophagitis; MS, multiple sclerosis; NR, not reported; Pediatric Quality of Life Inventory Gastrointestinal Symptoms Module; SDI, Straumann Dysphagia Index.
None of these studies addressed responsiveness to change, test-retest reliability, or reproducibility.
Discussion
Our systematic review identified 4 questionnaires for the symptomatic assessment of pediatric dysphagia that have been validated in children.21,24,25,27 With the exception of the PedsQL GI Module,26,27 these questionnaires were validated only in children with a specific disease entity. In contrast, the PedsQL GI Module was validated in a broader pediatric population, comprising children with functional or organic gastrointestinal disorders and included assessment of psychosocial domains. The utility of these identified questionnaires is unknown in the assessment of children who are not members of the disease specific cohort in which they were validated. No identified questionnaires were validated in a general pediatric population.
The ideal surgical patient-reported symptom assessment instrument would demonstrate content, construct, and discriminant validity; have internal consistency; and show responsiveness to change, with reproducibility and test-retest reliability. Of the identified questionnaires, only the DYMUS and the PedsQL GI Module reported internal consistency, indicating reliability of the questionnaire items, and no questionnaire tested responsiveness to change or test-retest reliability. Without further testing, the ability of these questionnaires to accurately assess a patient’s response to intervention is unknown.
Both the DYMUS 21 and the DSQ 24 were validated in adolescents and adults. The DSQ study population contained a comparable number of adolescents and adults and reported some results by age subpopulation. The study population for validation of the DYMUS, however, lacked additional descriptive data regarding the adolescent cohort and had a high median age (47.5 years).
The DSQ has several other limitations. The questionnaire contains assessment of only solid food dysphagia, with no clear definition of a solid. Furthermore, although the validation study of the DSQ reports construct validity with the correlation of DSQ scores to the SDI score, the SDI itself is not validated.
The number of articles utilizing questionnaires to report pediatric dysphagia outcomes that were validated only in adults points to the need for standardized pediatric metrics to assess dysphagia.17-20 Having a standardized validated assessment instrument would allow clinicians to track disease activity and symptoms longitudinally as well as compare results among pediatric clinical trials. Unlike the pediatric literature, the adult literature is replete with questionnaires aimed at symptom assessment and/or quality-of-life assessment for dysphagic patients. These include questionnaires specific to oropharyngeal9,10 and esophageal dysphagia,8,9 as well as disease-specific instruments.11,12,14
Given that outcome questionnaires validated in adults have in the past been modified for use in children (eg, Pediatric Voice Handicap Index), 28 establishing a standard assessment questionnaire for pediatric dysphagia may entail a similar modification of a preexisting metric validated in adults. Such an approach would have to consider the developmental differences among children of different ages and the need for a parental proxy in children who cannot reliably report symptoms. Further validation of a disease-specific pediatric questionnaire in a broader pediatric population could also be carried out, completing psychometric assessments as described above.
The primary limitation of our systematic review is that, despite a thorough search, we found few validated questionnaires that included a symptom assessment of dysphagia in children.
Conclusion
Our systematic review yielded no patient- or parent-reported questionnaires validated for the assessment of dysphagia symptoms in the general pediatric population. However, we identified 4 questionnaires that have been validated in specific pediatric disease cohorts. Having a standardized assessment instrument validated in all children would allow clinicians to systematically report symptoms and compare results of pediatric clinical trials. With this in mind, we recommend establishing a standard questionnaire for the broader pediatric population.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the 2015 AAO-HNSF Annual Meeting & OTO EXPO; September 27-30, 2015; Dallas, Texas.