
Abstract
Objectives
Fine-needle aspiration biopsy (FNAB) has a well-established role in the evaluation of an adult head and neck mass (HNM) but remains underused in children. The objectives of this study were to assess the diagnostic accuracy, safety profile, use of anesthesia, and influence on surgical decision making of FNAB of HNM in the pediatric population.
Study Design
Case series with chart review.
Setting
Tertiary care children’s hospital.
Subjects and Methods
In total, 257 consecutive patients with HNM who underwent 338 FNABs from July 2007 to July 2014 were reviewed. Patients ranged in age from 0 to 21 years (mean, 9.3 years); lesions ranged in size from 0.3 to 12.5 cm (mean, 2.4cm). Fine-needle aspiration biopsies were performed in the interventional radiology suite, operating room, clinic, or ward.
Results
The most common patient final diagnoses included reactive lymphadenopathy (n = 99, 38.5%), benign thyroid colloid nodule (n = 31, 12.1%), malignancies (n = 21, 8.2%), and atypical mycobacterial infection (n = 15, 5.8%). On surgical histopathologic and clinical follow-up, overall sensitivity of FNAB was 94.6% and specificity was 97.7%. The complication rate was 2.1%, and general anesthesia or sedation was used for 73% of FNAB. Surgery occurred only 9 times following the 191 patients with negative FNAB results, indicating that 95.3% of unnecessary surgeries were avoided with the assistance of the FNAB result.
Conclusions
Fine-needle aspiration biopsy is an accurate and safe diagnostic tool for guiding management of persistent lymphadenopathy, thyroid nodules, and other HNM in pediatric patients. Negative FNABs can often obviate the need for surgical intervention.
Keywords
Fine-needle aspiration biopsy (FNAB) dates back as far as 1857 and has been established in the diagnosis of head and neck masses (HNMs) since the late 1920s. 1 In the adult population, FNAB is widely used and accurate for diagnosis of both benign and malignant lesions throughout the head and neck region.2,3 For example, FNAB has been used with great success as the primary screening test for thyroid nodules in adults, 4 but such a structured approach has lagged in the evaluation of pediatric thyroid nodules.5,6
This diagnostic modality has gradually become more accepted in the pediatric population but remains underused. The first studies examining pediatric FNAB were published in the 1980s,7-9 and the first report dedicated to pediatric HNM FNAB was published in 1991 by Mobley et al. 10 Since that time, several publications have related the safety, accuracy, and feasibility of FNAB in pediatric HNM11-16 but have been limited by case numbers or restricted anatomic subsites.
The potential avoidance of surgery with associated scarring, complications, general anesthetic risk, recovery time, and expense have all been heralded as benefits of FNAB, especially given the high prevalence of nonneoplastic pediatric HNM. The objectives of this study were to assess the diagnostic accuracy and safety profile of FNAB in a large number of thyroid and nonthyroid pediatric HNMs. In addition, we examined the clinical application of FNAB, including the use of general anesthesia and the influence of FNAB on surgical decision making.
Methods
Institutional review board approval was obtained from the University of Pittsburgh. Patients aged 0 to 21 years were retrospectively identified in a cytopathology database for having undergone FNAB of a HNM. Consecutive subjects from July 2007 to July 2014 were included, and there were no exclusion criteria. All patients were seen in the pediatric otolaryngology or endocrinology departments where the need for FNAB was determined and consent was obtained for the procedure.
The decision to proceed with nonthyroid FNAB was typically based on persistence of a neck mass beyond 4 weeks despite treatment with antibiotics. Cases atypical for benign lymphadenopathy were referred for FNAB sooner (eg, unusual location, rapid enlargement, weight loss, night sweats, skin changes, fixed/immobile mass). All nonthyroid FNABs were performed because the patient was considered a potential surgical candidate, the mass was atypical, and/or the family or medical team desired a pathologic diagnosis. Given the high rate of malignancy in pediatric thyroid nodules, patients with lesions greater than 1 cm or smaller with concerning ultrasonographic features (hypoechogenicity, irregular margins, or increased vascularity) were offered FNAB.
Fine-needle aspiration biopsies were subsequently performed in the otolaryngology clinic or inpatient ward by the cytopathologist, the interventional radiology suite (IR) by a radiologist, or the operating room (OR) by the surgeon or cytopathologist. Topical (4% lidocaine cream), general, or topical plus sedative anesthesia was used. As a standard practice at our institution, all biopsies performed in the IR suite used image guidance, and all others were performed by palpation. Most thyroid nodules were biopsied with ultrasound guidance, consistent with current recommendations. 6
A 25- to 27-gauge needle was used, and approximately 3 to 5 passes were performed for each targeted site, representing a single FNAB. Patients with multiple FNABs therefore had more than 1 targeted HNM, multiple encounters, or both. Aspirated material was used for smear preparation, including air-dried slides stained with Diff-Quik and alcohol-fixed slides stained with the Papanicolaou stain. Residual material was submitted for ThinPrep (Hologic Inc, Marlborough, Massachusetts) processing, microbial cultures, molecular studies, flow cytometry, and/or cell block preparation, depending on the immediate interpretation. Cell block sections were stained with hematoxylin and eosin stain, and additional levels were used for immunostains, special stains, or other ancillary testing. The FNABs were interpreted by 1 of 9 cytopathologists, although most (88%) were interpreted by 1 of 2 cytopathologists with pediatric expertise. Nonthyroid cases received diagnoses with an adequacy interpretation (unsatisfactory, less than optimal, or satisfactory), a primary interpretation (nondiagnostic, negative for malignant cells, atypical cells present, suspicious for malignant cells, or positive for malignant cells), and a free text explanatory diagnosis. Thyroid cases received an adequacy interpretation, a primary interpretation using The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC), 4 and a free text explanatory diagnosis.
The determination of a nonsurgical (negative) vs surgical (positive) FNAB result was made for each patient. Final outcomes were then established either through correlation to surgical histopathology or clinical follow-up. Histopathology based on surgical biopsy (incisional or excisional) is considered the reference standard in the diagnosis of an HNM. Clinical follow-up is included as a secondary reference given that most pediatric HNMs are benign and do not undergo surgery and therefore histopathologic evaluation.
True positives were cytopathologic results that warranted surgical treatment and were confirmed as such histopathologically. True negatives were cytopathologic results that did not indicate a need for surgery and were confirmed histopathologically as such. Clinical true negatives were cytopathologically negative conditions that resolved or did not progress without surgical intervention. False positives were cytopathologic results that indicated a need for surgical treatment but histopathology demonstrated a nonsurgical condition. False negatives were cytopathologic results that did not indicate a need for surgery but were histopathologically proven to be conditions where surgery was indicated. Pathologists interpreting surgical histopathology were distinct from our cytopathologists and neither was blinded to clinical information or pathology results.
Certain conditions, such as atypical mycobacterial infection, cervicofacial abscess, lymphovenous malformations, and lymphoma, may warrant surgical diagnosis or treatment but may also appropriately proceed directly to medically therapy. These cases were all considered positive on the basis that surgery could be indicated. If surgery was pursued and histopathology confirmed the cytopathologic result, the case was a true positive. If the appropriate medical therapy was initiated and was effective, the result was a clinical true positive.
Individual diagnoses and demographic data such as age at first encounter and sex are presented on a patient level. Features unique to each encounter such as complications, FNAB venue, and level of anesthesia are presented on an encounter level. Specificity, sensitivity, and nondiagnostic results are presented on an FNAB level.
SPSS version 21 (SPSS, Inc, an IBM Company, Chicago, Illinois) was used to analyze the data. Sensitivity, specificity, and positive and negative predictive values were calculated using the definitions as detailed above. Nondiagnostic results were not included in these statistics, and no missing data were encountered. A P value <.05 was considered significant. Age at first encounter was compared between the high and low level of anesthesia and thyroid/nonthyroid groups using an independent sample t test. Age was compared between the thyroid/nonthyroid groups using Pearson’s χ2 test. Generalized estimating equations were used to compare the number of nondiagnostic results between the level of anesthesia groups. This method was used to account for the dependency of FNAB across encounters within patients. 17 The 2015 Standards for Reporting of Diagnostic Accuracy (STARD) guideline for reporting diagnostic accuracy studies was used. 18
Results
Over the 7-year study period, 257 patients who underwent at least 1 FNAB were identified. By having multiple FNABs at 1 or multiple visits, there were 338 total FNABs, with 284 specific encounters ( Figure 1 ). Baseline characteristics of the patients are shown in Table 1 . The 169 patients in the nonthyroid group were younger (mean age, 7.1 vs 13.6 years, P < .001) and had a lower percentage of females (38.5% vs 77.3%, P < .001) than the 88 patients in the thyroid group. The mean (SD) size of the 189 masses with prebiopsy imaging was 2.4 (1.73) cm (range, 0.3-12.5 cm). The average time between FNAB and surgery was 73 days (range, 0-1183 days). The volume of FNABs performed per month steadily increased from 3.2 in 2007 to 7.2 in 2014 with no seasonal variation.
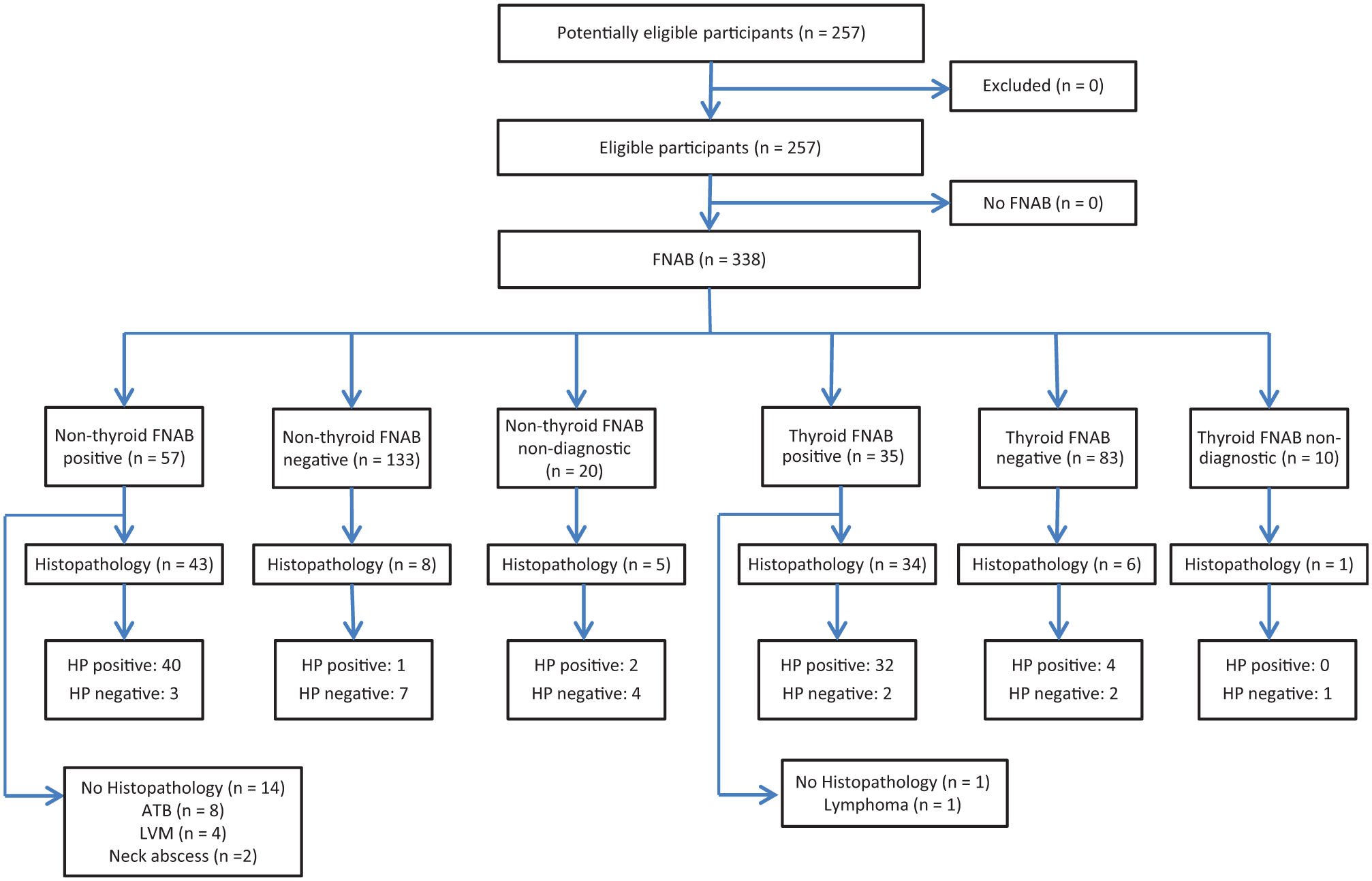
STARD flowchart of enrolled patients and FNAB. ATB, atypical tuberculosis; FNAB, fine-needle aspiration biopsy; HP, histopathology; LVM, lymphovenous malformation.
Characteristic of Patients and FNABs.
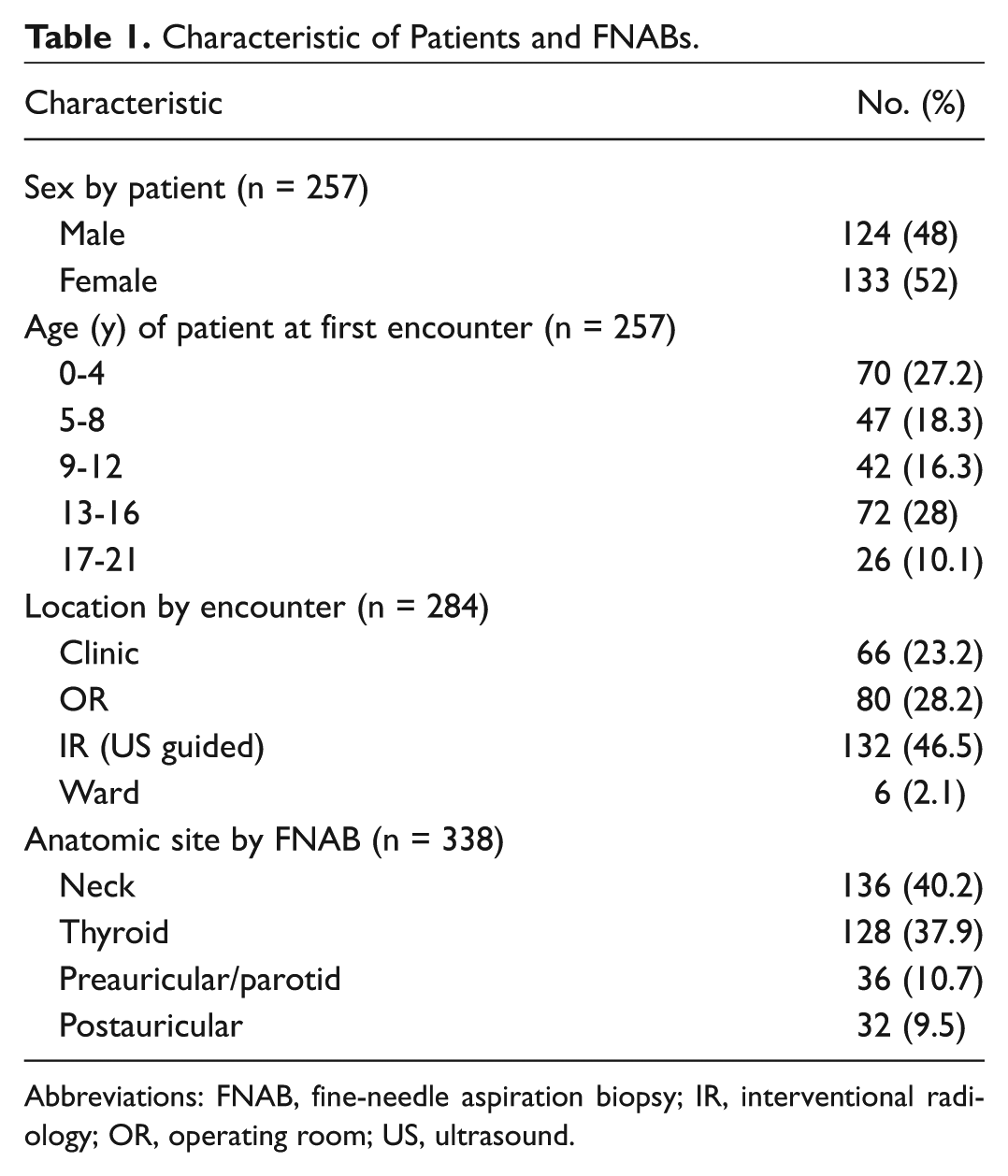
Abbreviations: FNAB, fine-needle aspiration biopsy; IR, interventional radiology; OR, operating room; US, ultrasound.
Diagnostic Accuracy
The overall pathologically confirmed sensitivity and specificity were 93.5% and 64.3%, respectively ( Table 2 ). If clinically and pathologically confirmed results are combined, sensitivity was 94.6% and specificity was 97.7% ( Table 2 ). When rapid on-site interpretation yielded a preliminary diagnosis, it correlated with final cytopathology 99.1% of the time (n = 106) and final surgical histopathology 93.3% of the time (n = 30). The false positives and false negatives are presented in Table 3 .
Sensitivity, Specificity, and Positive and Negative Predictive Values.
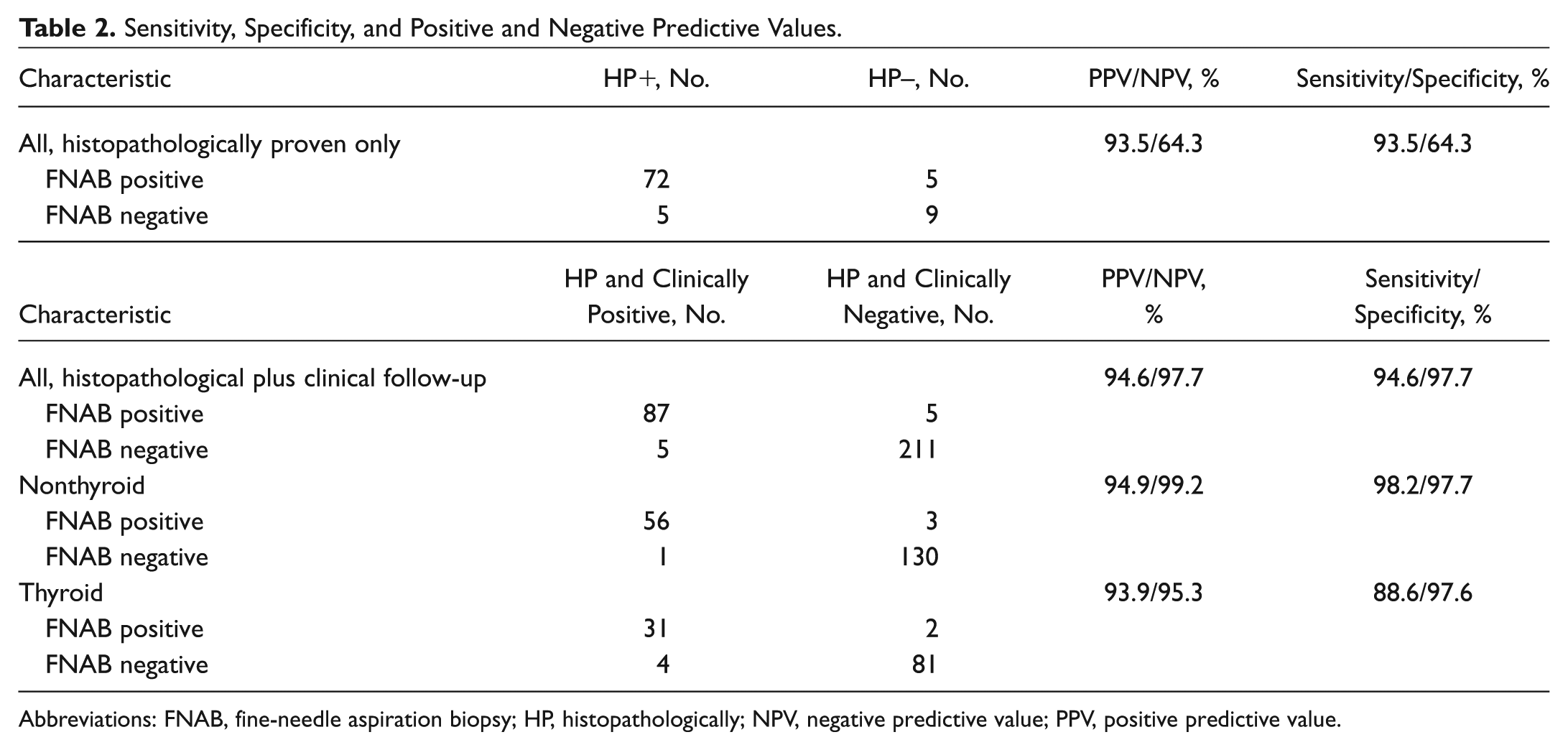
Abbreviations: FNAB, fine-needle aspiration biopsy; HP, histopathologically; NPV, negative predictive value; PPV, positive predictive value.
False-Positive and False-Negative FNAB with Final Histopathologic Result, Explanation of Error, and/or Patient Outcome.
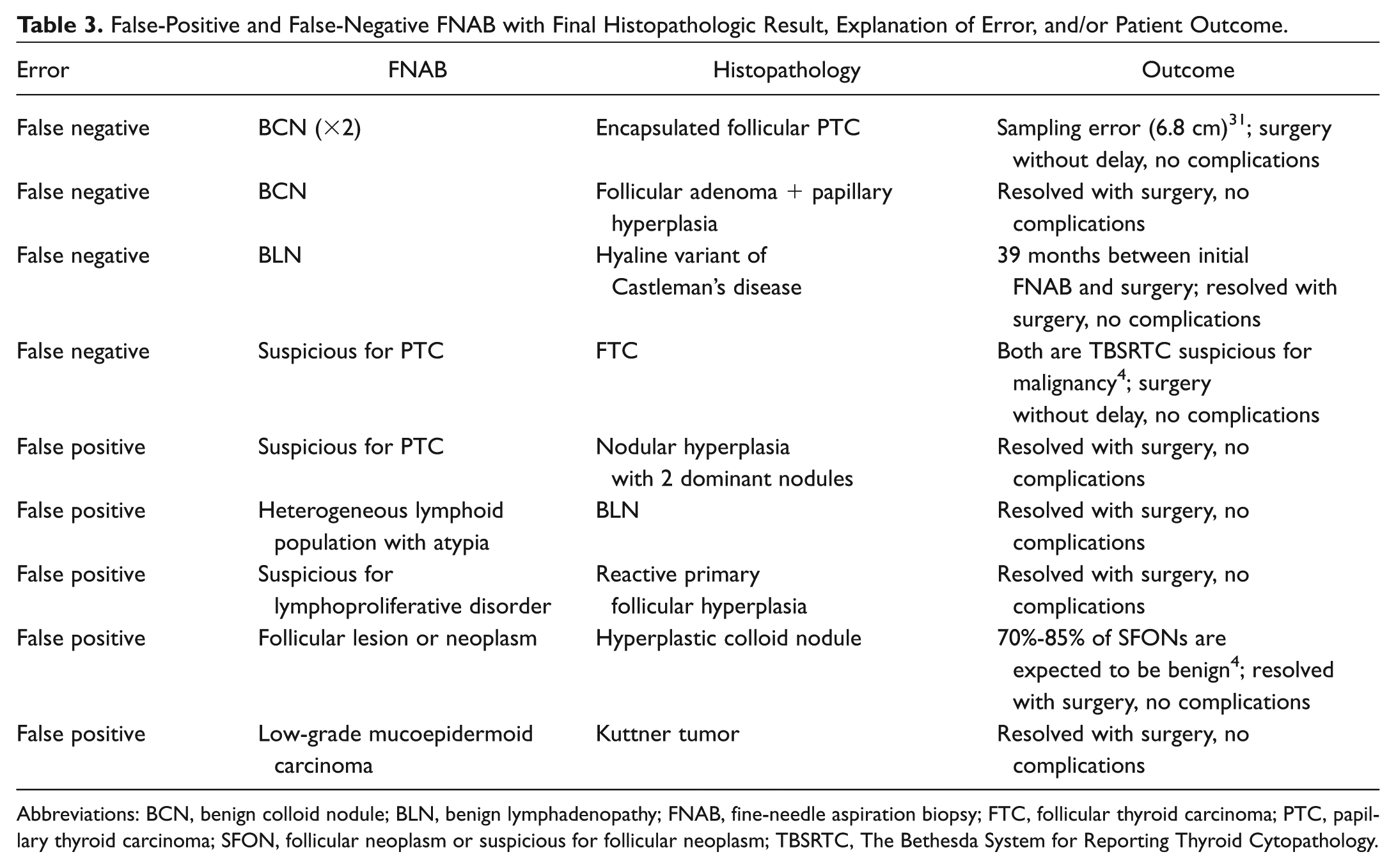
Abbreviations: BCN, benign colloid nodule; BLN, benign lymphadenopathy; FNAB, fine-needle aspiration biopsy; FTC, follicular thyroid carcinoma; PTC, papillary thyroid carcinoma; SFON, follicular neoplasm or suspicious for follicular neoplasm; TBSRTC, The Bethesda System for Reporting Thyroid Cytopathology.
The clinical nonthyroid HNM sensitivity and specificity were 98.2% and 97.7%, respectively, representing 190 total FNABs ( Table 2 ). There were an additional 20 nondiagnostic specimens (9.5%). Table 4 presents the final diagnoses, the most common of which was benign reactive lymphadenopathy (BLN), present in 99 patients. Malignancy was detected in 6 of the 169 patients (3.6%), including a metastatic medullary thyroid carcinoma that was not confirmed by thyroid FNAB prior to thyroidectomy.
Partial List of Patient Final Diagnoses.
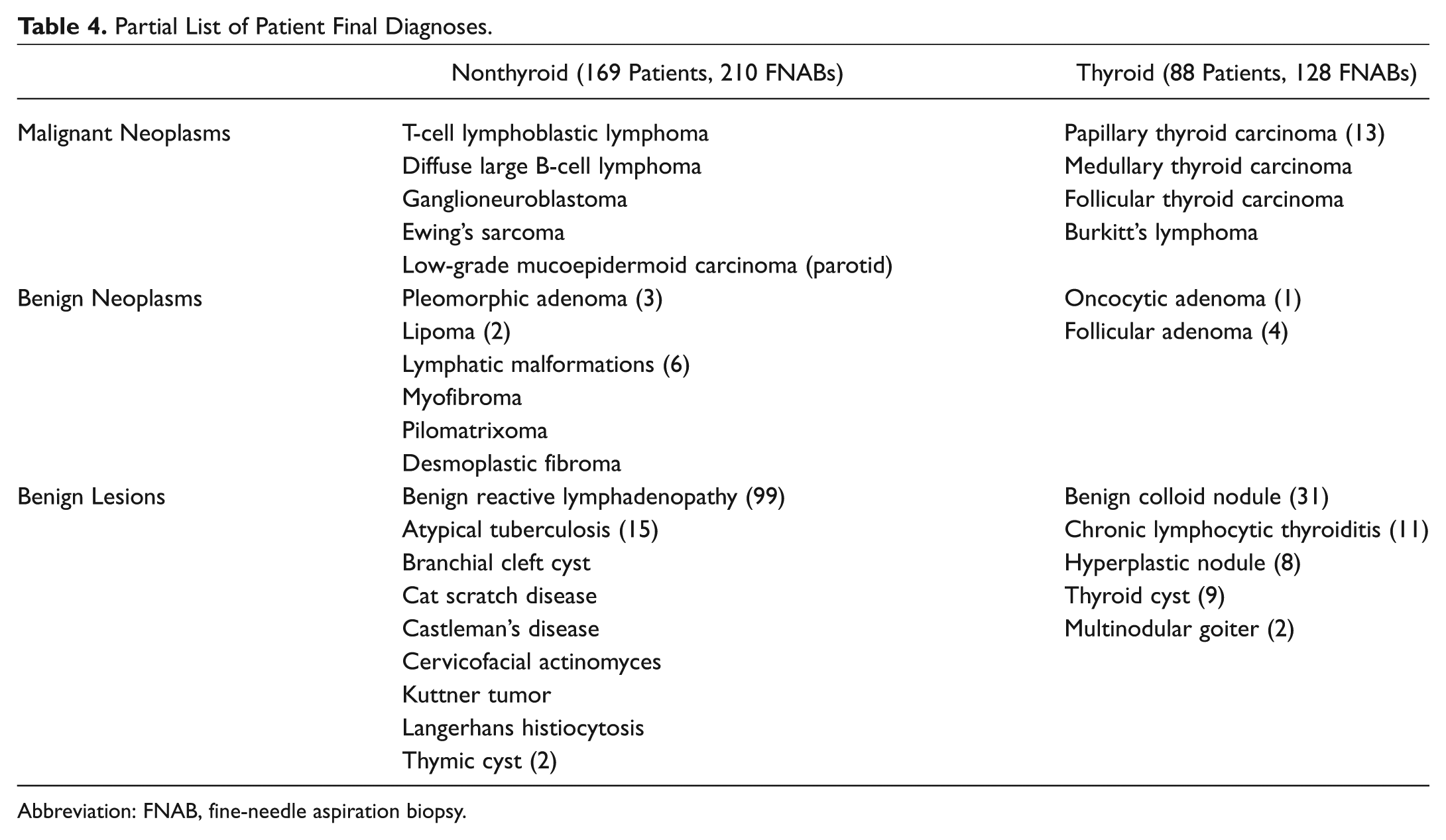
Abbreviation: FNAB, fine-needle aspiration biopsy.
There were 118 thyroid FNABs, with a clinical sensitivity of 88.6% and specificity of 97.6% ( Table 2 ). There were 10 nondiagnostic results (7.8%). The most common diagnosis was benign colloid nodule, found in 31 children. Fifteen malignancies were detected in the 88 patients undergoing thyroid FNABs (17.0%), most commonly papillary thyroid carcinoma. The rates of malignancy by are presented TBSRTC 4 category in Table 5 with comparisons to a large pediatric thyroid FNAB series. 19
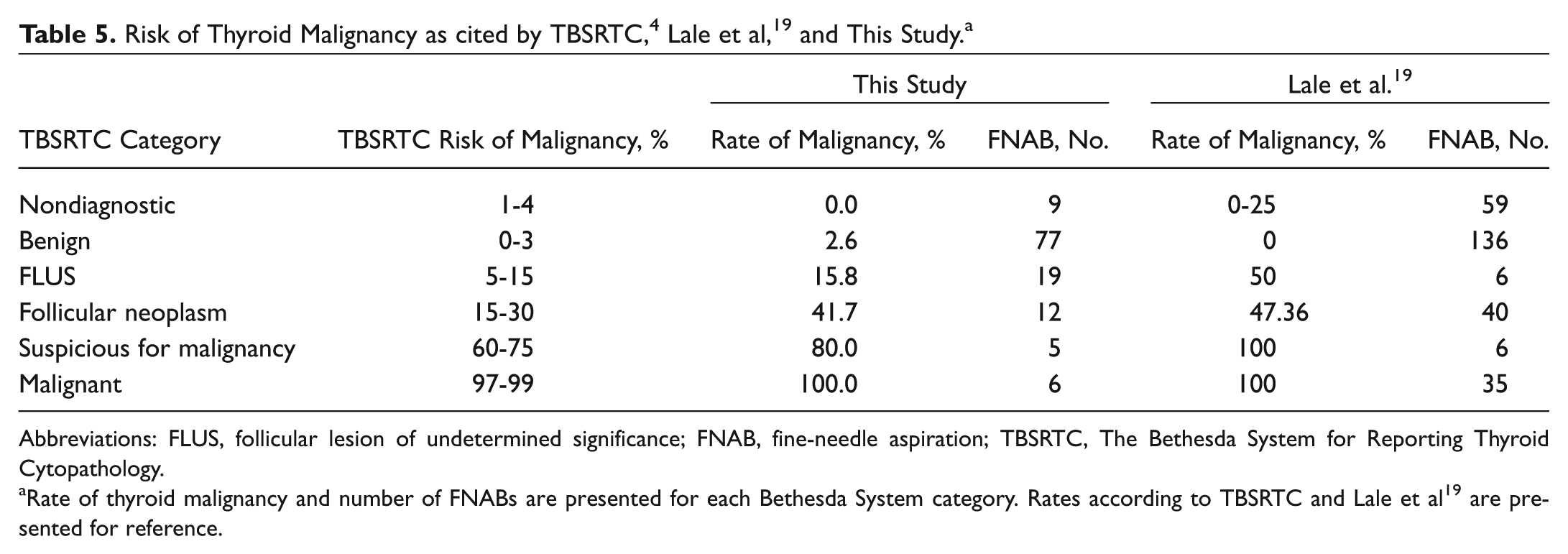
Abbreviations: FLUS, follicular lesion of undetermined significance; FNAB, fine-needle aspiration; TBSRTC, The Bethesda System for Reporting Thyroid Cytopathology.
Rate of thyroid malignancy and number of FNABs are presented for each Bethesda System category. Rates according to TBSRTC and Lale et al 19 are presented for reference.
The overall FNAB nondiagnostic rate was 8.9% (n = 30). All 10 of the thyroid nondiagnostic results were performed with image guidance and under general anesthesia (GA) or sedation. Of the 20 nonthyroid nondiagnostic results, there was no difference in the number of nondiagnostic results by anesthesia group (8 in topical/no-anesthesia group vs 12 in GA/sedation, P = .416), but only 5 of these 20 used image guidance.
Safety Profile
The overall complication rate was 2.1%. All 6 of the complications occurred in nonthyroid HNM patients undergoing FNAB in the clinic with topical anesthesia only. Vasovagal response was seen in 2 patients after successful FNAB. Both patients were discharged home in good condition from the otolaryngology clinic. Two patients (aged 5 and 9 years) could not have all FNAB passes completed due to discomfort. One procedure was terminated due to equipment failure. One lesion was too small to be successfully targeted and has been followed clinically. Mild FNAB site ecchymosis was not considered a complication but rather an expected occurrence. In comparison, there was a 9.1% complication rate in the 77 surgeries performed, including hypertrophic scar/alopecia, neck abscess, neck seroma, incomplete resection, inadvertent pharyngotomy, and Horner’s syndrome.
General Anesthesia
Of the FNABs, 73% were performed with GA or sedation. Overall, there was no statistically significant difference in the age of those requiring GA vs topical anesthesia alone (9.3 ± 5.5 vs 9.5 ± 5.6 years old, P = .410), but this finding is skewed by the use of GA for all but 3 thyroid FNABs. Excluding the thyroid and concurrent thyroid-lymph node FNAB, 66 (39%) FNAB encounters were performed with topical or no anesthesia and 105 (61%) with GA or sedation, and a younger average age was found in the heightened GA/sedation group (6.3 ± 4.8 vs 8.5 ± 5.4 years, P = .006).
Surgical Decision Making
Seventy-seven patients (27.0%) underwent surgery after an FNAB encounter, with 11.7% (n = 9) of these procedures following negative FNAB results. When combined with the nonsurgical cases, 9 of the 191 patients (4.7%) had a surgical intervention following FNAB results that did not indicate a need for surgery. Therefore, FNAB results assisted in the decision making to avoid surgery in 95.3% of patients in whom it was not considered appropriate.
Discussion
Pediatric HNMs are a commonly encountered finding with a broad differential diagnosis confronting pediatricians and otolaryngologists alike. The diagnostic challenge is distinct from the adult HNM in that only 4% to 11% of pediatric neck masses are found to be malignant, whereas in adults, this figure is over 60%.20-24 Our overall incidence of malignancy in nonthyroid FNAB was 3.6%. This does, however, likely represent an overestimate of the true incidence of pediatric nonthyroid HNM malignancy, as typically only persistent or otherwise worrisome masses undergo FNAB or surgical excision, especially at a tertiary referral hospital. Furthermore, congenital lesions such as branchial cleft anomalies and lymphatic malformations tend to not undergo FNAB given characteristic physical exam and imaging findings.
The opposite scenario is seen in pediatric thyroid nodules—namely, they are far less common than in adults but more commonly malignant. Recent studies suggest that 16% to 26% (17% in this study) of pediatric thyroid nodules are malignant, which compares to 5% in adults.6,25-27 Therefore, to ensure adequate sampling as well as increase patient comfort while undergoing a deeper FNAB, virtually all thyroid FNABs at our institution are performed under GA in the IR suite with ultrasound guidance.
Diagnostic Accuracy
Sensitivity reported in our study and others is dependent on surgical histopathologic results to validate true positives and false negatives. The overall sensitivity in this study (93.5%) is similar to previous studies, which have shown rates of 93.3% to 100%, indicating reliability in both small and large series as well as all head and neck locations.10,14,15 Specificity, however, is more limited by the fact that most “benign” or negative FNAB results will not undergo surgery. Our pathologically confirmed specificity was 64.3% but represents only 14 cases. Working under the assumption that patients who have clinical resolution or nonprogression of disease confirms a negative FNAB, our specificity was 97.7%. Slightly higher overall sensitivity and specificity were seen in nonthyroid FNABs ( Table 2 ), which is also seen in the adult population. 3
The overall sensitivity and specificity of the thyroid FNAB was 88.6% and 97.6%, respectively, which is consistent with reports within both the general and pediatric populations.19,28-30 The applicability of The Bethesda System (TBSRTC) to the pediatric population has been previously examined in the literature and is a recommendation of the 2015 American Thyroid Association (ATA) Guidelines for Pediatric Thyroid Nodules and Cancer.6,19 We found the 128 thyroid FNABs to have excellent concordance with the rates of malignancy as described by TBSRTC 4 ( Table 5 ). Similar to Lale et al, 19 there was an increased rate of malignancies in the indeterminate TBSRTC categories (III, IV, and V).
In addition to being highly accurate, FNAB offers the potential for a more rapid diagnosis when the cytopathologist can make an on-site judgment. Our study found that in the 106 instances when an initial diagnosis was offered, it correlated with final cytopathology 99.1% of the time—an improvement from 92% in the predecessor study from our institution. 14 Rapid on-site diagnosis correlated with 93.3% of histopathologic results. The ability to offer an accurate on-site diagnosis is not only helpful in treatment planning but also in alleviating patient and family anxiety.
The rate of nondiagnostic FNAB results is seemingly high (n = 30, 8.9%) but was found to be lower than in a large meta-analysis of adult HNM. 3 Current management of such a result consists of clinical follow-up with possible repeat FNAB or surgical excision. With these and all other results, it is critical to remember that neither the sensitivity nor the specificity of FNAB is 100%, and FNAB results must be taken in the context of clinical factors.
General Anesthesia
General anesthesia or sedation was used in a significant portion of the children in this study, thus nullifying one of main benefits of FNAB. Most of these cases were thyroid evaluations, where GA is employed routinely by policy at our institution. While a younger average age was seen in the nonthyroid patients undergoing FNAB with sedation or GA (6.3 vs 8.5 years, P = .006), our experience was that many children of all ages were able to successfully undergo FNAB in the clinic with topical anesthesia alone. We therefore feel that general anesthesia is unnecessarily overused and that there is even the opportunity to perform thyroid FNAB with ultrasound guidance in an awake child or adolescent, as is common practice in adults. Nevertheless, parental preference, coordination with other procedures, or a perceived inability to tolerate an awake FNAB can drive the desire for a higher level of anesthesia in the OR or IR suite.
Surgical Decision Making
If the fundamental goal of FNAB is to provide a diagnosis that will influence management, there is a significant gain to be made in avoiding unnecessary surgery and associated complications in children with benign or nonsurgical conditions. Over the course of the 7-year study, surgery occurred only 9 times following the 191 negative FNAB results. Stated alternatively, negative FNAB results assisted in avoiding unnecessary surgery in 95.3% of patients in whom it was not indicated. In these 9 cases, the decision to proceed with surgery was guided by parental concern or the clinical judgment of the treating physician. Final histopathology concurred with the initial FNAB cytopathology in all 9 of these cases. Six of the cases occurred in the first 4 years of the study, whereas only 3 were in the last 3 years, indicating a possible increased clinician (and conceivably parental) confidence in FNAB results.
Aside from the avoided morbidity and mortality of surgery, the cost savings are potentially significant. For example, our institution charges $320.00 for an FNAB and $1203.00 for a simple excisional lymph node biopsy, excluding the cost of anesthesia ($550.00/hour), OR time ($740/hour), and a hospital room ($1017.10/day). The cost differences are obviously more pronounced when the surgery being considered is a total thyroidectomy or superficial parotidectomy.
Limitations
This study has several limitations that are inherent in its retrospective nature. First, the lack of standardization of the enrolled patients is reflective of both the diversity of pediatric HNM and the variable diagnostic and treatment approaches by different physicians. For example, in the routine lateral neck mass consistent with BLN, there was significant variation in the use, duration, and timing of antibiotic treatment, making uniform indications for FNAB challenging in the retrospective study. In these instances, FNAB was only offered once the child was deemed a potential surgical candidate, had an atypical presentation, or had an unclear diagnosis. Another limitation to this study is the lack of universal follow-up. All patients with negative FNAB results are instructed to follow up if the HNM persists or concerns remain. If no follow-up in our system was pursued, the child was assumed to have resolution and was counted as a clinical true negative. Even still, if these cases are excluded from the analysis, the overall specificity of FNAB is 96.2%. Despite these limitations, this study was able to demonstrate that FNAB in children is highly accurate and safe in a wide range of head and neck anatomic locations, diagnoses, and ages.
Conclusion
Fine-needle aspiration biopsy is a safe, well-tolerated, and accurate means of diagnosing pediatric HNM of thyroid and nonthyroid origin. Given that few nonthyroid pediatric HNMs are malignant, FNAB plays an important role in providing reassurance to obviate the need for unnecessary surgery in benign HNM. Pediatric thyroid malignancies, on the other hand, are not infrequent, and TBSRTC should be applied to the pediatric population with the caveat that a higher degree of suspicion should be present when FNAB result is indeterminate. When this triage or stratification of pediatric HNM is employed, it potentially reduces both surgical morbidity and the burden on health care resources.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We thank Li Wang and Dan Winger.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.