
Abstract
Objective
To test our hypothesis that general and thyroid surgery–specific complications, mortality, and postdischarge utilization for patients undergoing outpatient and inpatient thyroid and parathyroid surgery would not differ when outpatient status was defined as discharge within 8 hours of surgery completion.
Study Design
Retrospective observational cohort, 2008 to 2013.
Setting
Kaiser Permanente Northern California and Kaiser Permanente Southern California.
Subjects and Methods
We used a robust set of variables and propensity score methods to match 2362 patients undergoing hemithyroidectomy, total thyroidectomy, or parathyroidectomy surgery as outpatients to 2362 patients undergoing the same procedures as inpatients. Outcomes assessed were 30-day rates of complications, emergency department visits, all-cause hospital readmissions, and mortality.
Results
After matching, no statistically significant differences between inpatients and outpatients were found for complication rates or postdischarge utilization. After matching, there was no statistically significant difference between inpatients and outpatients in hematoma rates, which were 0.55% in both groups. In the matched-pair groups, 2 deaths occurred among inpatients (0.09%) and none occurred among outpatients (0.00%), a difference that was not statistically significant.
Conclusion
Discharge within 8 hours after completion of thyroid and parathyroid surgery is as safe as inpatient surgery.
More than half of all surgical procedures are performed in ambulatory settings. 1 In 2012, the most recent year for which multistate data are available, 62% of partial or complete thyroidectomies were performed on an outpatient basis. 1 In the 30 years since the first published account of performing thyroid surgery on an outpatient basis, 2 a growing number of peer-reviewed reports have documented the safety of outpatient thyroidectomies. In 2013, Terris et al 3 noted that studies published since 2006 included more than 4500 procedures, and the more recent use of databases such as the National Surgical Quality Improvement Program (NSQIP) and statewide ambulatory surgery databases enables analysis of even larger populations.4-6
However, existing reports have some limitations. The NSQIP data do not include individual surgeon volume, which is associated with clinical outcomes and, until 2011, did not include the thyroid surgery–specific complications of hypocalcemia and hematoma.3,6-14 Large databases may not distinguish between 23-hour and shorter stays.6,15 Many studies define outpatient status as same-day discharge,6,15-20 although others provide more precise information about shorter lengths of stay.21-31 Even recent studies using rigorous propensity score matching techniques, which can allow an observational study to approximate a randomized controlled trial, are subject to these limitations. 32
The purpose of this study was to assess the safety of outpatient thyroid and parathyroid surgery, using general and thyroid surgery–specific outcomes and postdischarge utilization, a robust set of variables in a propensity score matching model, and a definition of outpatient status as discharge within 8 hours of completed surgery. Our hypothesis was that outcomes and postdischarge utilization for outpatient and inpatient thyroid surgery would not differ.
Methods
The Kaiser Permanente Northern California Institutional Review Board approved this study. It was conducted from 2007 to 2013 in Kaiser Permanente Northern California and Kaiser Permanente Southern California, with a collective total of approximately 7.4 million members in December 2014. During the study period, 16,347 thyroid and parathyroid procedures were performed; 33.1% (5412) were hemithyroidectomies, 17.8% (2916) were parathyroidectomies, and 49.1% (8019) were total thyroidectomies. Annual procedure volumes more than doubled, from 1445 in 2008 to 3143 in 2013, and the proportion of outpatient surgeries increased from 10.4% in 2008 to 29.7% in 2013. Of hemithyroidectomies and parathyroidectomies performed in 2013, 51.5% (1056) and 64.7% (609) were performed on an outpatient basis, compared with 16% (1477) of total thyroidectomies. The proportion of surgeons performing any included procedures on an outpatient basis increased from 19.0% in 2008 to 49.1% in 2013. Surgeons comprised general surgeons with and without fellowship endocrine training and otolaryngologists.
The study population consisted of unique patients with a single thyroid or parathyroid procedure performed in 2008-2013 ( Figure 1 ). Patients were identified by International Classification of Diseases, Ninth Revision (ICD-9) codes for hemithyroidectomy (isthmusectomy [06.39], partial thyroidectomy [06.39], lobectomy [06.2]), total thyroidectomy (complete [06.4], complete with sternotomy [06.39]), and parathyroidectomy (operation on parathyroid gland [06.99], parathyroid exploration [06.99], parathyroidectomy [06.89], parathyroidectomy with minimally invasive approach [06.89]). Patients experiencing intraoperative complications, typically bleeding and recurrent laryngeal nerve injury, that required hospitalization were identified by a change from outpatient to inpatient status and excluded from the study population.
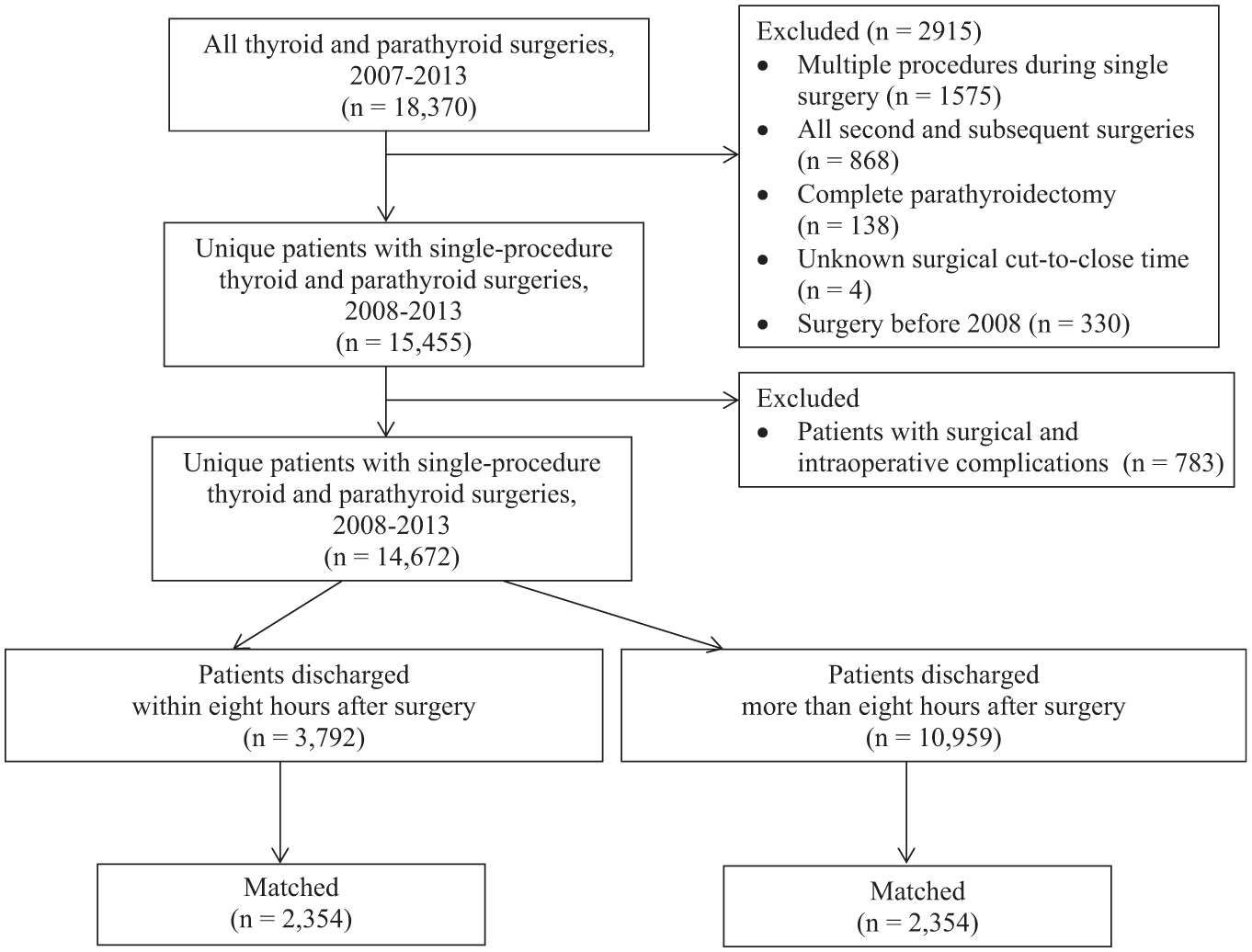
Participant flow diagram.
Outcomes studied were 30-day rates of complications, emergency department visits, all-cause hospital readmissions, and mortality. Complications were measured dichotomously as present or not during the first 30 days after surgery in 2 categories: thyroid surgery–related complications, which included hematoma, stridor, hypocalcemia, and vocal cord paralysis/paresis, and other complications, which included surgical site infection, deep incisional surgical site infection, wound disruption, pneumonia, deep vein thrombosis, pulmonary embolism, progressive renal insufficiency, acute renal failure, urinary tract infection, stroke, coma, acute myocardial infarction, sepsis, septic shock, neck swelling, seroma, chyle fistula, Horner’s syndrome, tracheal injury, esophageal injury, and other morbidity of unclear or unknown causes. The ICD-9 codes for complications are available online (Supplemental Table S1 at www.otojournal.org/supplemental). Hypocalcemia was identified by coded hypocalcemia, hungry bone syndrome, or hypoparathyroidism and was confirmed by a recorded serum calcium <8.5 mg/dL, a recorded serum ionized calcium of <4.8 mg/dL, or a serum parathyroid hormone level ≤10 pg/mL and prescribed medications of calcitriol or intravenous calcium gluconate. Postdischarge utilization was measured as 30-day rates of all-cause readmissions and emergency department visits.
The main independent variable was whether the procedure was performed on an outpatient or inpatient basis. Outpatient procedures were defined as those for which patients were discharged within 8 hours after surgery was completed.
To control for confounding factors and eliminate bias arising from patient selection, patients receiving procedures on an outpatient basis were matched to those receiving surgery on an inpatient basis using propensity scores and covariates that may have affected outcomes or the combination of choice of surgical setting and outcomes. Covariates included relative contraindications to outpatient surgery suggested by the American Thyroid Association (ATA) consensus-based guidelines for which data were available. 3 Covariates also included preoperative factors, procedure type, and annual surgeon procedure volumes. Dichotomous variables were created for region (Northern vs Southern California), sex, and comorbid conditions (Hashimoto’s disease, Graves’ disease, thyroid cancer, obstructive sleep apnea, visual impairment, hearing loss, disseminated cancer, hypertension, chronic obstructive pulmonary disease, bleeding disorders, diabetes, anxiety, asthma, dementia, depression, pregnancy, primary hyperparathyroidism, nontoxic goiter, radiotherapy within the past 90 days, chemotherapy within the past 30 days, dyspnea, steroid medication use, anticoagulant therapy, dialysis, acute myocardial infarction, stroke, and seizures). The ICD-9 codes for these conditions are available online in Supplemental Table S2 (at www.otojournal.org/supplemental). Categorical variables were created for age, ethnicity, body mass index (BMI), income, education, distance to nearest medical office building, Charlson comorbidity index, year of procedure, and DxCG risk score (Verisk Health, Inc, Waltham, Massachusetts). DxCG relative risk scores are a commercial product that assesses illness severity and predicts health care costs relative to the population mean, based on age, sex, diagnoses, and drug codes 33 ; it is a commonly used tool by the Centers for Medicare & Medicaid Services and frequently appears in peer-reviewed publications in public health literature. Prior-year utilization of office visits, hospitalization, and emergency department visits were treated as continuous variables. With the exception of income and education, data were available from KP HealthConnect, Kaiser Permanente’s integrated electronic health record (EHR), which is implemented across all settings. Data on income and education are not routinely collected and were imputed from census block–level data. 34
All covariates were used in multiple regression modeling to calculate a propensity score for the likelihood of outpatient surgery. Patients receiving surgery as outpatients and as inpatients were matched by procedure and propensity score using a greedy nearest-neighbor algorithm, within calipers set at 0.01. The balance between covariates was assessed using standardized differences in means, with a threshold of 10%. 35
Procedure-specific propensity score–matched groups and bootstrapped estimates were used to assess differences in 30-day rates of complications, postdischarge utilization, and mortality, using t tests for continuous variables and χ2 tests for categorical variables. Statistical analyses were performed with SAS version 9.2 (SAS Institute, Cary, North Carolina).
Results
A total of 14,762 adults were identified who underwent any of the listed procedures in 2008 to 2013. Inpatients were more likely to have undergone total thyroidectomy, have surgeons with lower annual procedure volumes, and have had surgery earlier in the study period; they also tended to be nonwhite and have higher Charlson comorbidity and DxCG scores, thyroid cancer, and Graves’ disease ( Table 1 ). Of adults meeting inclusion criteria, 4724, consisting of 2362 matched pairs of inpatients and outpatients, were included in the analysis. After matching, no significant differences remained between inpatients and outpatients in terms of demographics, procedure type, surgeon volume, year of surgery, overall disease burden, specific comorbidities, and prior utilization ( Table 1 ).
Characteristics of Patients Receiving Thyroid and Parathyroid Surgery as Outpatients and Inpatients before and after Propensity Score Matching.
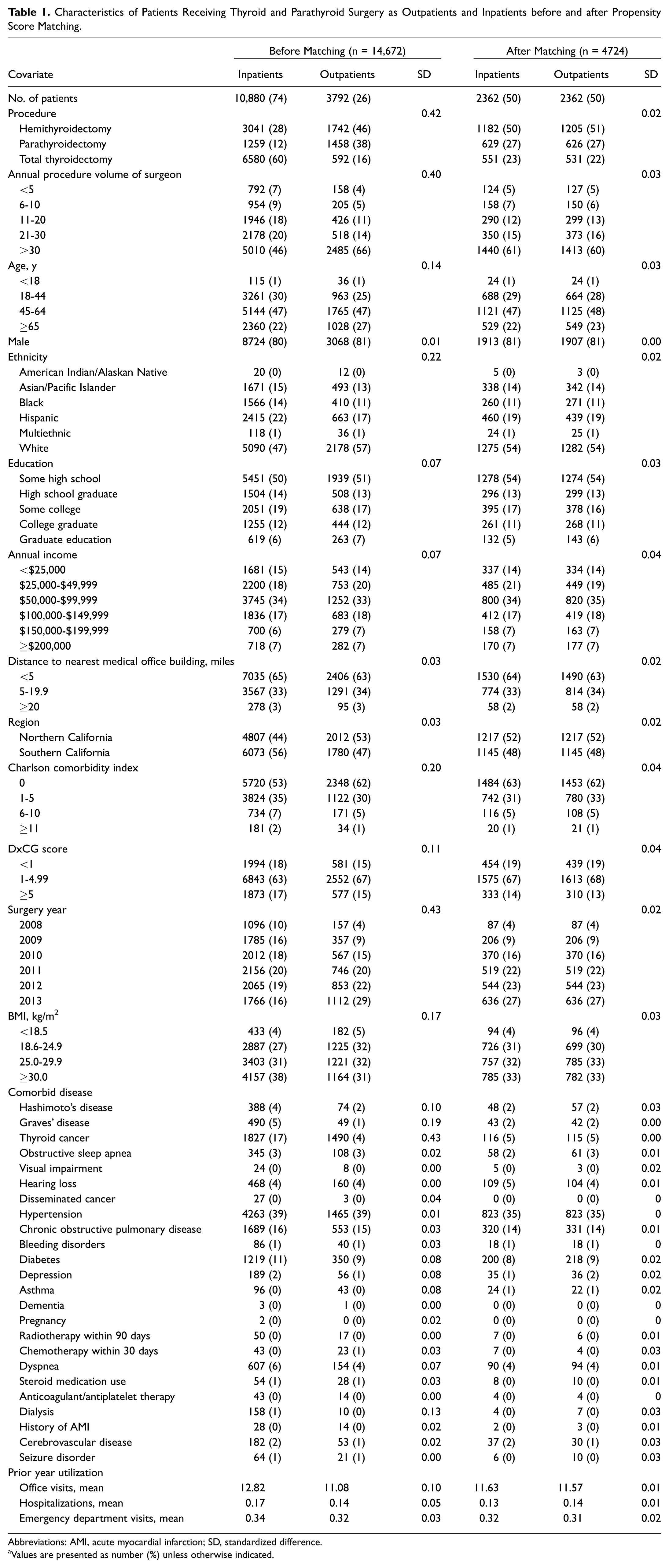
Abbreviations: AMI, acute myocardial infarction; SD, standardized difference.
Values are presented as number (%) unless otherwise indicated.
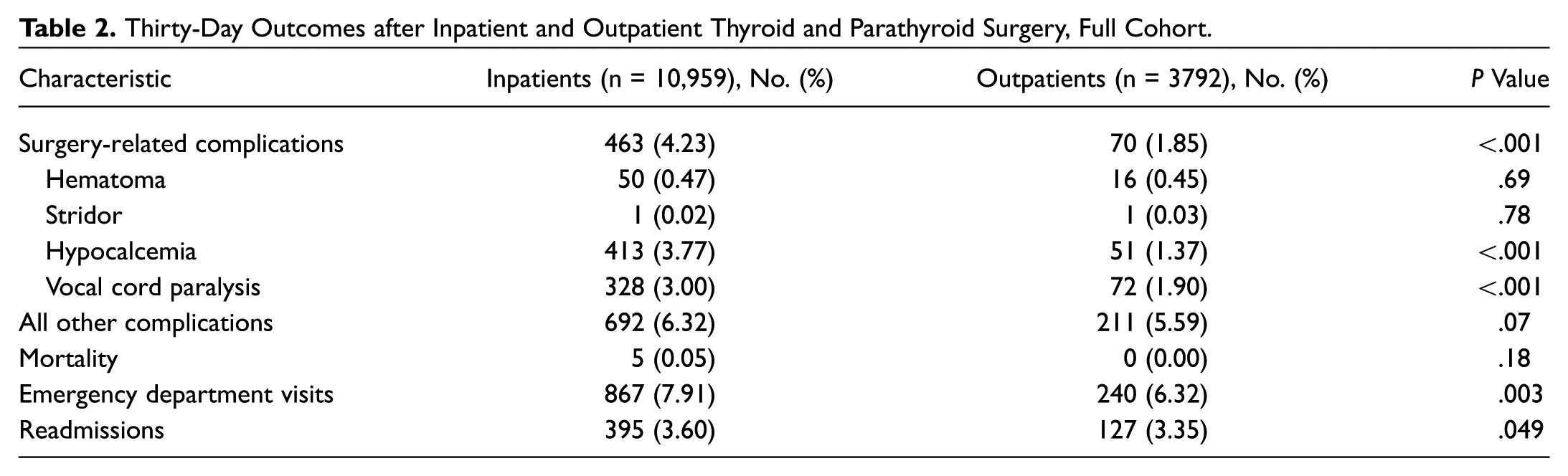
Before matching, rates of hypocalcemia, vocal cord paralysis, and the overall measure of surgery-related complications were lower among patients undergoing surgery as outpatients than among those with inpatient procedures, which may have been a function of the higher proportion of total thyroidectomies performed on an inpatient basis ( Table 2 ). After matching, no statistically significant differences between inpatient and outpatient procedures were found for complication rates or postdischarge utilization ( Table 3 ).
Thirty-Day Outcomes after Inpatient and Outpatient Thyroid and Parathyroid Surgery, Full Cohort.
Thirty-Day Outcomes after Inpatient and Outpatient Thyroid and Parathyroid Surgery and 95% Confidence Intervals, Matched Cohort.
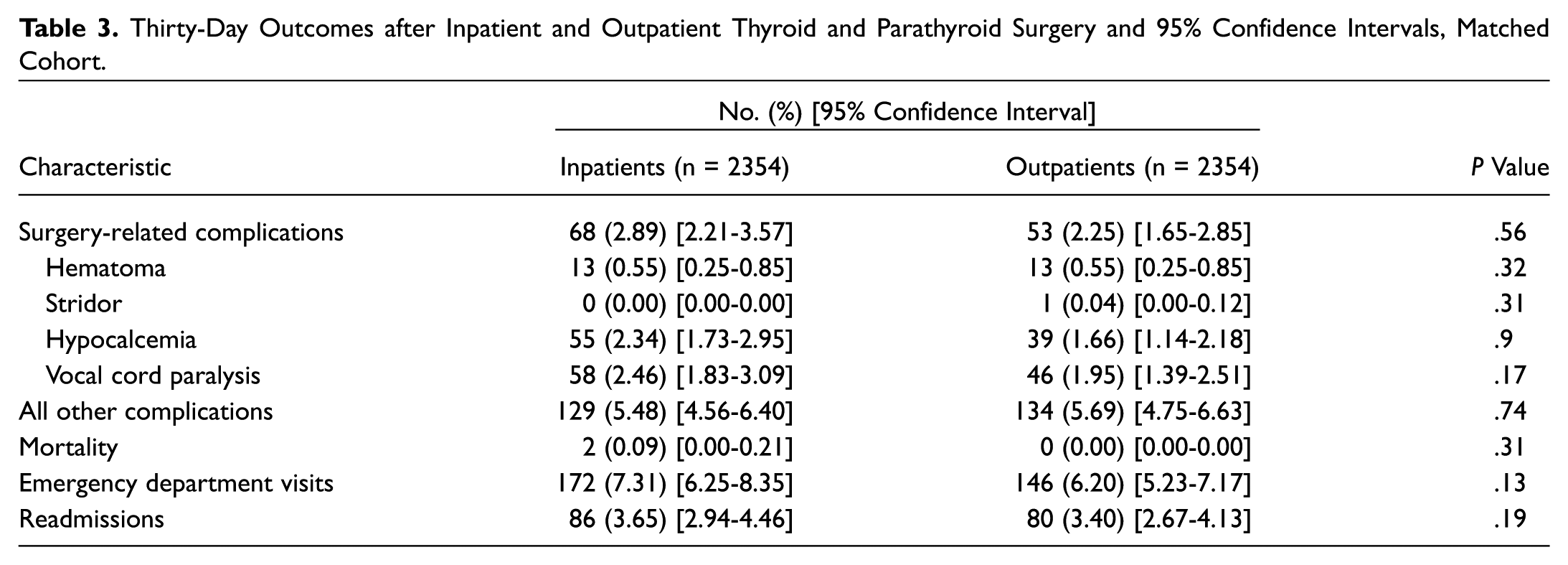
Before matching, rates of hematoma and mortality were lower in patients undergoing outpatient surgery. After matching, there was no statistically significant difference between inpatients and outpatients in hematoma rates, which were 0.55% in both groups. In the matched-pair groups, 2 deaths occurred among inpatients (0.09%) and none among outpatients (0.00%), a difference that was not statistically significant. Hematoma was not a cause of either inpatient death.
Discussion
Our use of propensity score methods resulted in well-matched cohorts of patients undergoing thyroid and parathyroid procedures that we used to compare the outcomes of outpatient and inpatient surgery. We found no differences in measured outcomes between outpatient and inpatient surgery for patients undergoing thyroid and parathyroid procedures.
Our findings differed from those of Khavanin et al, 6 who found that outpatient surgery was associated with decreased odds of complications, readmissions, and reoperations. Possible explanations include the fact that we assessed thyroid surgery–specific complications of hypocalcemia and hematoma, and the previous study using NSQIP data captured hypocalcemia only when it was recorded as the reason for readmission during a single year that data were available. In addition, our matching variables included those used by Khavanin et al, 6 as well as all ATA eligibility criteria and relative contraindications for which EHR data were available. We also defined outpatient procedures as discharge within 8 hours of surgery completion, whereas NSQIP data specify outpatients as discharged within 23 hours. Consequently, variations in assessed complications, studied populations, and lengths of stay may account for the differences between our findings and those of the previous study. With respect to readmissions, Khavanin et al 36 found decreased odds of 30-day readmissions for individuals undergoing surgery as outpatients; they also found readmission rates of 2.5% for outpatients and 3.3% for inpatients, which are consistent with other reports.16,30,36,37 We found no statistically significant differences between outpatients and inpatients in 30-day readmission rates that were also comparable to previous reports.
Strengths of our study include the assessment of specialty-specific complications and a robust set of matching variables that included the ATA relative contraindications to outpatient thyroid procedures and surgeon volume. In addition, we excluded patients with intraoperative complications necessitating hospitalization. Our goal was to demonstrate the safety of planned outpatient surgery for the included procedures among patients for whom we had data for the ATA selection criteria. Patients with intraoperative complications would likely be admitted on an unplanned basis. Using a specific definition of outpatient surgery is also a strength because existing reports of outpatient thyroidectomy include lengths of stay from approximately 1.5 hours after surgery to 23 hours.6,15-31 Another strength of our study was the inclusion of more than 200 surgeons at 43 medical centers with inherent variations in surgical practice, such as postoperative calcium supplementation, which increases the generalizability of our findings to other settings.
Several limitations also deserve mention. Over the course of the study period, the matching rate for parathyroidectomies and hemithyroidectomies decreased due to a continuing shift from inpatient to outpatient procedures. Consequently, approximately 50% of surgeries in the matched cohorts were hemithyroidectomies and approximately 20% were total thyroidectomies; we could not evaluate results by procedure type. The relatively low proportion (22% and 23%) of total thyroidectomies in the matched cohorts may have resulted in lower overall complication rates, 10 decreasing our ability to detect differences in rates between inpatient and outpatient procedures. In addition, approximately 75% of outpatient and inpatient procedures in the matched cohorts were performed by surgeons with an annual procedure volume of 21 or more, which may also have resulted in lower overall complication rates.12-14 Our study took place in an integrated health care system; although we do not expect that the delivery system affected our findings, their generalizability to other settings is unknown. We did not match for intraoperative factors such as estimated blood loss, surgery duration, or the use of thermal energy devices. Complications were identified by ICD-9 codes that may have been used inconsistently; we did not perform chart reviews to ascertain the degree to which this might have occurred. Matching variables included the consensus-based ATA guidelines for patient selection for outpatient surgery. 3 Evidence-based criteria for patient selection may have resulted in a different study population and different findings, but such criteria do not yet exist.
It is important to note that we did not assess the impact of using the ATA eligibility criteria and relative contraindications for outpatient surgery on complications. We can make no assertions about their potential to improve the safety of outpatient surgery through patient selection. However, our results suggest that outpatient thyroid and parathyroid procedures are equally safe among patients who are matched on a robust array of variables, which may encourage surgeons to perform more outpatient procedures. At this point in time, the ATA guidelines are the best available tool for identifying candidates for outpatient surgery and can be used with more confidence. However, we also note that patient education addressing early recognition of complications and appropriate action steps is an essential part of a safe outpatient surgery program. 3
Future research should use decision analysis methods to increase the rigor with which the best candidates for outpatient thyroid and parathyroid surgery are identified. In addition, future research should identify cost savings related to performing an increasing proportion of thyroid and parathyroid surgery on an outpatient basis, as suggested by Terris et al. 3 Al-Qurayshi et al 38 recently documented that thyroid procedures performed by high-volume surgeons were associated with lower costs of care, yielding an estimated savings of $2 billion over 14 years. Future research should apply a similar analysis to outpatient procedures.
Conclusion
This study, using propensity score matching techniques, suggests that thyroid and parathyroid procedures performed on an inpatient and outpatient basis offer comparable quality outcomes. Thyroid and parathyroid surgery are never free of risk, but outpatient surgery can be considered as safe as inpatient surgery. There remain multiple factors to consider when choosing the appropriate venue for surgery, and further assessment of risk stratification should assist surgeons in making the best decisions about surgical setting.
Author Contributions
Disclosures
Sponsorships: None.
Funding source: None.
Footnotes
Acknowledgements
The authors thank Violeta Rabrenovich and Heather Qian for their essential support of this study. Jennifer Green provided editorial assistance. Matt Lando, MD, provided valuable review of the draft manuscript.
No sponsorships or competing interests have been disclosed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.