
Abstract
Objective
Contralateral reactive lesions (RLs) represent a distinct entity among benign bilateral vocal fold (VF) lesions. Lack of uniform nomenclature and a myriad of surgical options have hampered attempts to develop treatment guidelines. The objective of this study is to better define RLs and their prognosis, through the development of a standard nomenclature, with an aim to guide treatment and delineate the role of phonosurgery.
Study Design
Case series with chart review.
Setting
Tertiary care center.
Subjects and Methods
Analysis was performed on patients with Current Procedural Terminology code 31545. Operative reports with a primary lesion and contralateral RL were included. Outcomes included the Voice Handicap Index–10 (VHI-10) and GRBAS (grade, roughness, breathiness, asthenia, and strain) scale, lesion persistence/recurrence, mucosal wave, and edge character based on blinded videostroboscopy review.
Results
A nomenclature was developed based on intraoperative RLs (n = 30), defined by lesion consistency (fibrous or polypoid) and relationship to normal VF edge (gradual or steep). Reactive lesion treatment included no intervention, excision, potassium titanyl phosphate laser, steroid injection, or a combination thereof. Observations included the following: inconsistent treatment modalities were employed, excision of RLs did not yield better outcomes, fibrous RLs were more likely to persist and polypoid lesions more likely to recur, gradual lesions were more likely to remain disease free, and most treatments showed improved mucosal wave, VHI-10, and GRBAS.
Conclusions
Reactive lesions have not been well classified, and treatments are based on subjective intraoperative decision making with unpredictable outcomes. The nomenclature proposed will allow for a better definition of the RL and provide a framework for future research to identify optimal treatment.
Benign lesions of the vocal fold (VF) are common. Standard clinical classification has included nodules, polyps, Reinke’s edema, and cysts. 1 More recently, fibrous masses and reactive lesions (RLs) have been added. 2 However, there is still no consensus on terminology, and this is especially true of benign traumatic bilateral vocal fold lesions (BVFLs).3-7 At times, definitive diagnosis can only be established intraoperatively, as Poels et al 8 showed that bilateral lesions were found in 53% of patients preoperatively and in 82% of these patients when explored intraoperatively. 3 It is essential to understand that accurate definition of benign BVFLs guides prognosis and therapeutic planning. 5
Reactive lesions represent a difficult entity within BVFLs. They are not well defined, their behavior is not well understood, and there is no consensus on the best treatment; therefore, we propose a standard nomenclature for the RL. Different groups have attempted to characterize the entity. Some authors describe a contralateral reactive callus with epithelial hyperplasia caused by shearing forces of a unilateral VF lesion.2,5,9-11 Poels et al 8 add that the contact swelling depends on laryngeal load, with shorter traumatic periods yielding less indurated lesions. They all warn that the unilateral lesion with contralateral RL can be a diagnostic pitfall often confused with bilateral nodules.8,12
In 2000, Rosen et al 7 performed a retrospective study (n = 85) evaluating patients with BVFL and found 64 patients to have a unilateral VF lesion with a contralateral RL (UVFL/RL). They did not identify specific RL criteria but described the entity as varying in size and morphology. They demonstrated significant differences in the UVFL/RL entity compared with bilateral nodules in the following parameters: increased asymmetry of VF vibration, increased shimmer and peak amplitude variation on aerodynamic analysis, decreased laryngeal efficiency as higher subglottic peak air pressure, and a higher perception of vocal disability on the Voice Handicap Index.
Few groups have studied optimal treatment of the RL. In their experience, Sataloff et al 13 believe that most RLs will resolve with removal of the primary offending lesion and voice therapy due to reduced VF edema and lesion contact. They recommend surgical excision of the RL only if conservative measures fail.
Many studies have discussed different types of lesions, yet the question remains as to what characteristics predict RL behavior and how to treat them. Are RLs similar to nodules, warranting conservative treatments such as sole resection of the primary lesion, voice therapy, or steroid injection, with phonosurgery reserved for recalcitrant cases?5,6,11,14-16 Are all reactive lesions fibrous or do some have polyp-like characteristics? The objective of this study was to create a nomenclature for RLs for prognosis and treatment and to further delineate the role of phonosurgery. From the nomenclature developed, we hypothesized that fibrous lesions would resolve with less invasive treatments in contrast to polypoid lesions, which would require surgical excision.5,6,11,14-16 Gradual lesions were expected to respond better to conservative treatment compared with steep lesions that caused greater tissue deformity.
Methods
This case series with chart review was approved as an exempt study by the New York Eye and Ear Infirmary Institutional Review Board Review Committee. A retrospective analysis of charts from 2007 to 2012 at a tertiary care center was performed on all patients who underwent surgery with Current Procedural Terminology code 31545 (suspension microlaryngoscopy with resection of nodule/submucosal mass with local flap reconstruction). Operative reports with a dictated primary lesion and contralateral reactive VF lesion were included. Minimum follow-up of 3 months was required.
Clinical parameters collected included basic demographics, BVFL intervention, follow-up time within 1 year, dysphonia assessed by the Voice Handicap Index–10 (VHI-10) and GRBAS (grade, roughness, breathiness, asthenia, and strain) scores (preoperative and postoperative—1 week, 6 weeks, 4 months, 9-12 months), preoperative VF lesion consistency (defined as fibrous or polypoid), preoperative VF lesion edge character described by transition height from the normal VF edge (defined as gradual or steep), lesion persistence (lesion presence on first postoperative visit), lesion recurrence (lesion presence any time after a first postoperative visit where a lesion was not visualized), postoperative mucosal wave (defined as none, present but decreased, or normal), postoperative edge character (defined as straight, fullness, or tissue insufficiency). The GRBAS scores were determined by the speech-language pathologist, with at least 6 years of experience with voice patients, who was present during the patient visit, without knowledge of previous scores. Difference in VHI-10 and GRBAS scores was calculated as change from the preoperative visit to the last recorded postoperative visit. Lesion persistence/recurrence, mucosal wave, and edge character were assessed by blinded review of videostroboscopy clips presented to the senior author. Lesion recurrence was assessed at the final stroboscopy study available. If recurrent disease was found, preliminary stroboscopy studies were reviewed to assess for persistence immediately after surgery. Mucosal wave was assessed at the anteromedial one-third of the true VF at modal frequency.
Objective statistical evaluation was completed in combined single-group analysis (n = 30), with analysis of subgroups deferred due to low power.
Results
Thirty patients met inclusion criteria (10 males, 20 females) with a mean age at intervention of 39.5 years. Follow-up was 3 to 12 months (mean, 8.4 months). Based on review of intraoperative RLs, a nomenclature for the contralateral reactive VF lesion was developed. Lesion consistency was defined as fibrous or polypoid, and relationship to the normal VF edge was defined as a gradual or steep transition. Lesions were characterized as fibrous if their consistency was opaque, with thickened epithelium; lesions were polypoid if their consistency was translucent and smooth in nature. Lesions were characterized as gradual if they were relatively flush with the normal VF edge so that palpation with a probe would not rock the lesion, whereas steep lesions demonstrated a palpable step off from the normal edge. The following RLs were identified: gradual fibrous (n = 18), steep fibrous (n = 6), gradual polyp (n = 4), and steep polyp (n = 2), with intraoperative examples demonstrated in Figure 1 . All patients underwent preoperative and postoperative voice therapy. All primary lesions (2 fibrous, 28 polyps) were excised using the microflap technique; RLs were treated with various interventions, including no intervention (n = 3), excision via microflap (n = 11), potassium titanyl phosphate (KTP) laser resulting in photocoagulation to ischemia without ablation (n = 3), injection of 40 mg/mL methylprednisolone acetate (n = 6), microflap excision with methylprednisolone acetate injection (n = 5), or KTP as described with methylprednisolone acetate injection (n = 2).
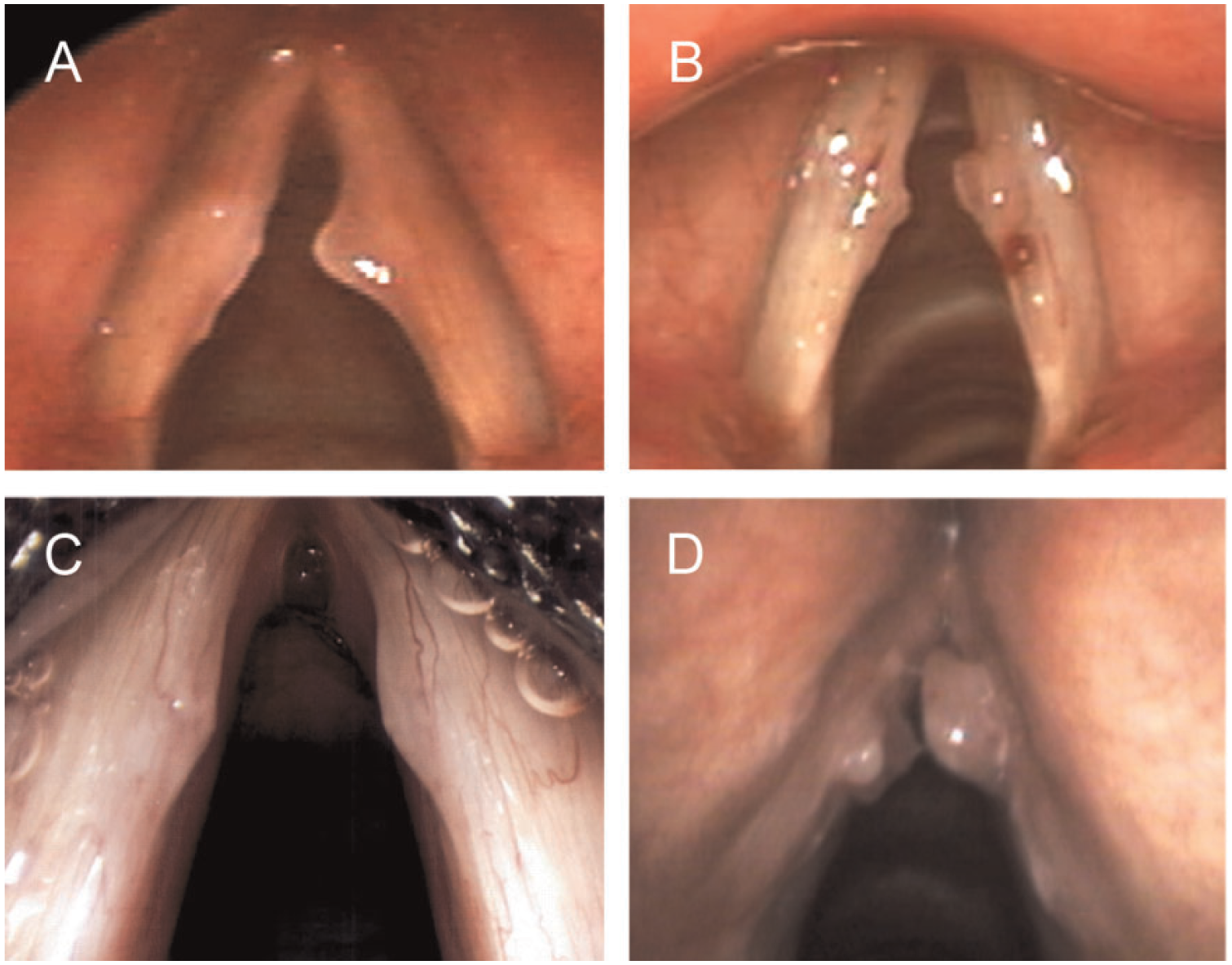
Reactive vocal fold lesion characteristics. (A) Left reactive gradual fibrous lesion. (B) Left reactive steep fibrous lesion. (C) Left reactive gradual polypoid lesion. (D) Left reactive steep polypoid lesion.
As a whole, for lesions with no intervention, 3 of 3 resolved; for those that had intervention, 17 of 27 resolved, 5 of 27 persisted, and 5 of 27 recurred as noted by fullness of the VF edge. All persistent lesions were noted on the first available postoperative stroboscopy examination (mean, 6.3 days postoperative, excluding 1 patient who only had a stroboscopic examination available 55 days postoperative). The mean time to recurrence was 2.6 months. Resolution, persistence, and recurrence patterns as a function of lesion consistency and intervention are demonstrated in Table 1 . For those lesions that persisted on the first postoperative follow-up, at their final visit (mean, 7.5 months), 3 of 5 lesions were unchanged, 1 lesion improved, and 1 completely resolved (a gradual fibrous lesion treated with steroid injection). In addition, at latest follow-up, persistent lesions showed a decrease in VHI by an average of 17.3 (mean, 8.3 months postoperative) and decrease in GRBAS score by an average of 0.5, 0.5, 1.25, 1.25, and 0.5 (mean, 8.9 months postoperative); mucosal wave remained unchanged in 3 of 5 persistent lesions, improved in 1 patient, and was worse in 1 patient.
Lesion Persistence/Recurrence as a Function of Consistency and Intervention.
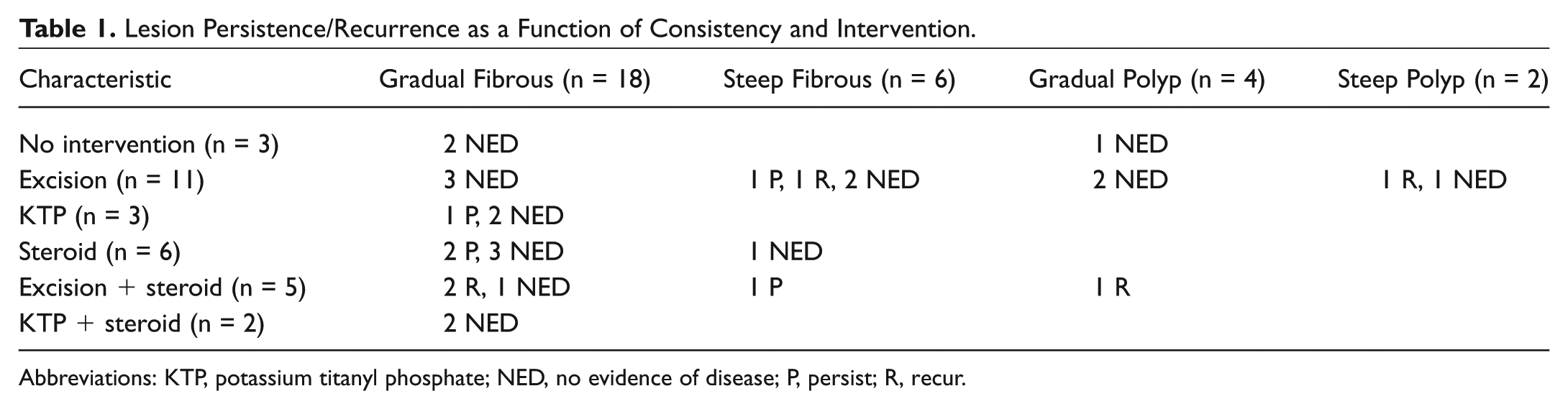
Abbreviations: KTP, potassium titanyl phosphate; NED, no evidence of disease; P, persist; R, recur.
With almost all treatments, mucosal wave of the reactive lesion vocal fold (RLVF) remained unchanged (n = 13) or improved (n = 12). Two patients showed a decrease in mucosal wave: 1 gradual fibrous lesion treated with steroid injection and 1 steep fibrous lesion treated with excision; mucosal wave could not be adequately assessed in 3 patients. Changes in mucosal wave based on intervention are displayed in Table 2 .
Mucosal Wave Based on Intervention.
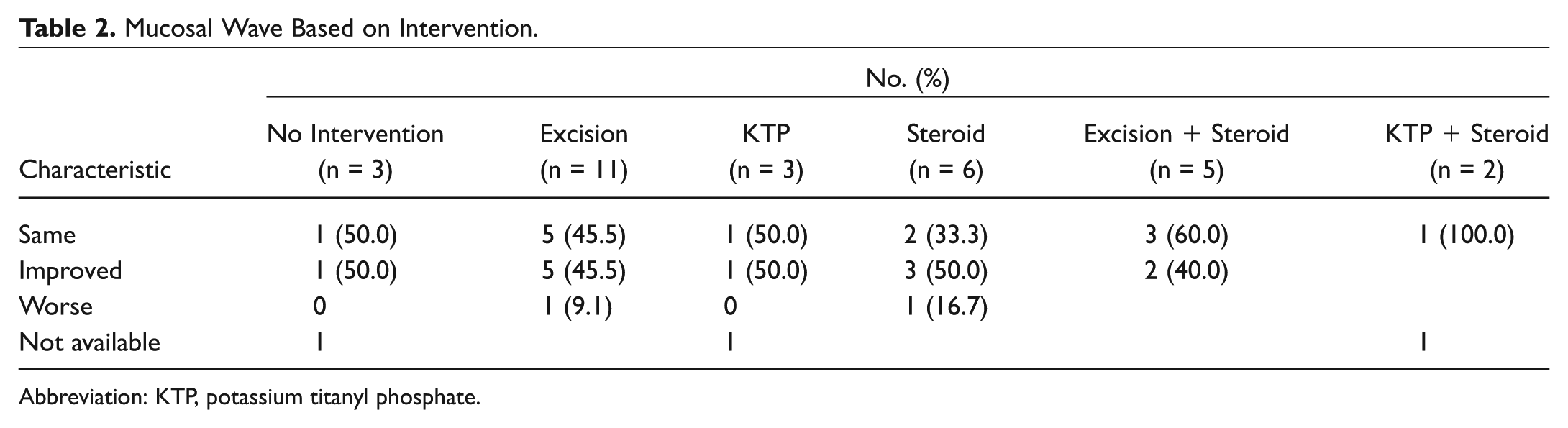
Abbreviation: KTP, potassium titanyl phosphate.
Using a combined single-group analysis, both VHI (P = .00006, using the Wilcoxon signed-rank test) and GRBAS score (P < .00001, using a paired t test) showed significant improvement at a mean of 8.6 months posttreatment. Mean VHI score decreased by 16.5, and mean GRBAS decrease was 1, 1, 1, 0.6, and 0.7. No statistical analysis was performed between subgroups given the limited sample size of each group. Changes in VHI-10 and GRBAS based on intervention are displayed in Table 3 .
Dysphonia Scales Based on Intervention.
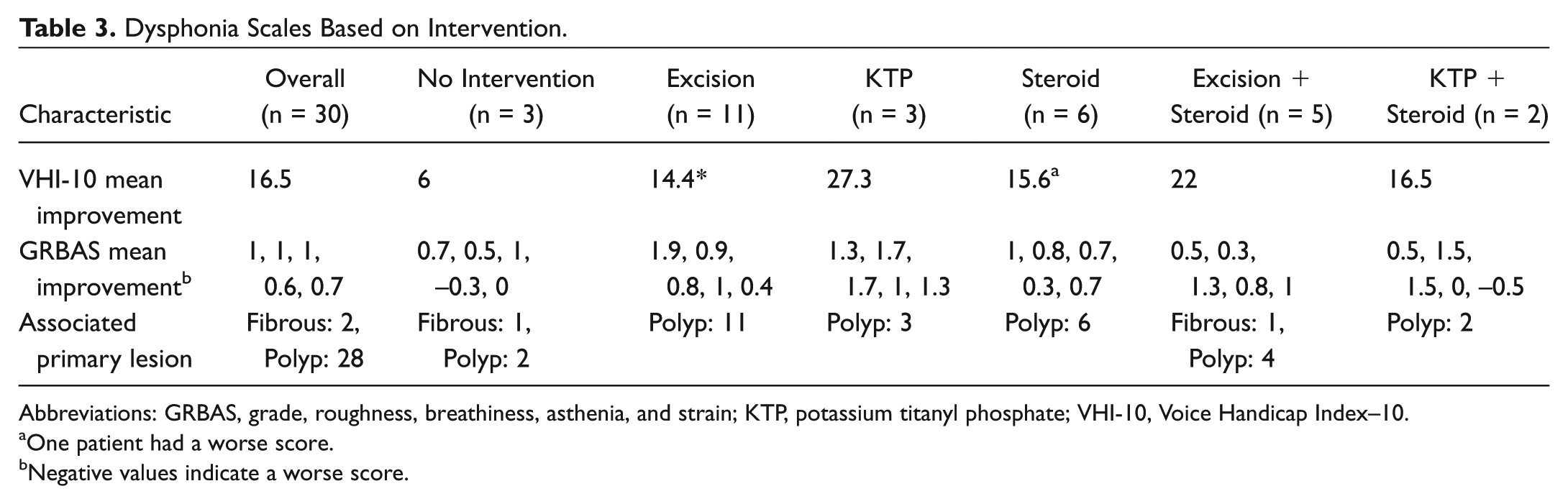
Abbreviations: GRBAS, grade, roughness, breathiness, asthenia, and strain; KTP, potassium titanyl phosphate; VHI-10, Voice Handicap Index–10.
One patient had a worse score.
Negative values indicate a worse score.
Study observations included the following: no consistent treatment modalities were employed based on lesion type, treatments that included RL excision did not yield better outcomes, fibrous RLs were more likely to persist and polypoid lesions more likely to recur, gradual compared with steep RLs were more likely to remain disease free, almost all treatments showed improvement or no change in mucosal wave, and all treatments demonstrated a decrease in VHI-10 and GRBAS scores.
Discussion
In the present study, a nomenclature for the RL was developed and outcomes of various interventions were presented. The nomenclature focuses on 2 aspects of the lesion that are thought to play a role in surgical decision making: lesion consistency and relationship to the normal VF edge. Consistency is defined as fibrous, similar to nodule texture, or polypoid. Relationship to the normal VF is defined as a gradual or steep transition. We hypothesized that fibrous lesions would resolve with less invasive treatments, such as removal of the primary lesion, voice therapy, and steroid injection, in contrast to polypoid lesions, which would require surgical excision.5,6,11,14-16 Gradual lesions were expected to respond better to conservative treatment compared with prominent steep lesions that appeared thicker and caused greater deformity.
All primary lesions were excised, but no consistent treatment modalities were employed based on lesion type under the proposed nomenclature. Reactive lesion treatments included no intervention, excision, KTP laser, steroid injection, excision with steroid injection, and KTP with steroid injection. All treatments demonstrated improvement or no change in mucosal wave and significant improvement in dysphonia as graded by VHI-10 and GRBAS scores. Importantly, much of the voice improvement likely occurred secondary to surgical excision of the primary lesion, and changes in voice scores cannot be attributed only to treatment of the RL. However, based on a combined single-group analysis, we are able to generally conclude for all patients with a dominant phonotraumatic lesion and an RL that voice is expected to improve regardless of treatment approach. Fibrous RLs were more likely to persist and polypoid RLs were more likely to recur regardless of edge character. This may indicate that fibrous RLs behave in a more recalcitrant fashion than presumed and as compared with typical nodules. Studies have reported a significant association between highly fibrotic nodules and a poorer response to steroid injection. This is thought to be due to increased epithelial thickening and fibroblast proliferation.15,17 In consideration of the higher recurrence of polypoid RLs, their formation may be due to more factors than just trauma from a contralateral lesion. Factors such as inherent vulnerabilities in the VF, voice use, glottal closure patterns, or comorbidities such as allergies or reflux may play a role.
Gradual, as compared with steep, RLs were more likely to remain disease free. This may reflect a greater difficulty for the chosen therapies to achieve resolution of steep lesions or a larger degree of physical stress in the system preoperatively that persists postoperatively. Furthermore, in terms of persistence and recurrence, treatments that included RL excision did not result in better outcomes regardless of lesion type, suggesting that observation or less invasive interventions, which carry lower risk, may be preferable.
There are a number of limitations to this study. Lesion types were assigned in a retrospective manner. Future studies should focus on assigning lesion types in the nomenclature to various treatment arms to be followed prospectively. Another limitation is the small sample size (n = 30) given that there were 6 treatment arms (patient range, 2-11). In addition, factors unrelated to lesion characteristics, such as daily vocal demands and compliance with voice therapy, could not be accurately evaluated in this retrospective investigation and could confound the study.
Despite its limitations, we believe this study illustrates the importance of a standard nomenclature in defining RLs and the randomness of choosing a therapeutic modality, which results in unpredictable outcomes. To improve patient care, RLs must be categorized so their treatment and its results can be studied in a prospective fashion. By providing a nomenclature and preliminary treatment data, this study sets a framework for future investigation in identifying the optimal treatment of RLs.
Conclusion
Reactive VF lesion is a distinct entity that has not been well classified with no current treatment guidelines. Thus far, treatments appear to be based on subjective intraoperative decision making of ill-defined parameters. This study proposes a nomenclature for RLs, defining lesion consistency as fibrous or polypoid and relationship to the normal VF edge as a gradual or steep transition. Distinct treatment protocols cannot be suggested, although it appears that fibrous lesions are more likely to persist, polypoid lesions are more likely to recur, and gradual compared with steep lesions are more likely to remain disease free. Importantly, excision of the RL does not appear to be better than alternatives and may carry higher risk. The nomenclature suggested in this study will allow for better definition of the RL and sets the stage for future research in identifying optimal treatments.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This work was presented as a poster to the Fall Voice Conference; October 15-17, 2015; Pittsburgh, Pennsylvania.