
Abstract
Objective
Tonsillectomy is still one of the most common surgical procedures, but there exists no standard guideline for pain management after tonsillectomy. Our aim is to determine whether oral spray of flurbiprofen reduces pain and has an influence on other morbid outcomes following tonsillectomy.
Study Design
Prospective, double-blind, randomized, placebo controlled.
Setting
Patients at Ataturk Training and Research Hospital, Ankara, Turkey.
Subjects and Methods
This study was performed on 84 patients (45 in flurbiprofen group, 39 in placebo group) who underwent tonsillectomy. The patients were randomly chosen, and each used oral spray of flurbiprofen 3 times daily or placebo solution at the same regimen. Efficacy was assessed by changes in Numeric Pain Rating Scale. Data were collected at postoperative days 1, 3, 5, and 7 for pain, bleeding, and healing. Data for Mallampati scores were also collected.
Results
There were no significant difference between groups with respect to the demographic data. The flurbiprofen group had statistically significant lower pain scores at days 1, 3, 5, and 7 (P = .000, P = .002, P = .001, P = .000, respectively). On days 3 and 7, pain scores were significantly different between different Mallampati groups (P = .049, P = .015, respectively). The flurbiprofen group required less analgesic than the placebo group during the study period on days 1, 3, 5, and 7 (P = .001, P = .001, P = .03, P = .001, respectively). Healing and side effects were not significantly different between the groups.
Conclusion
In this study, topical use of flurbiprofen may reduce posttonsillectomy pain without any evidence of additional complications.
Tonsillectomy is a common procedure that may cause considerable postoperative pain, especially in adults. In spite of the advances in surgical and anesthetic techniques, the cause of morbidity is still oropharyngeal pain after tonsillectomy, which may result in decreased oral intake, dysphagia, dehydration, and weight loss.
In general, there are 3 commonly used treatments for management of pain after tonsillectomy: opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), and acetaminophen. Opioid analgesics may cause respiratory depression, especially in individuals with obstructive sleep apnea. Acetaminophen may not be strong enough for posttonsillectomy pain. Although the Cochrane Collaboration concluded that NSAIDs can be safely used for the postoperative treatment of pain following tonsillectomy, their use after tonsillectomy has been controversial because of adverse effects on platelet function that may prolong bleeding time. 1 To avoid potential side effects of NSAIDs, topical use of local anesthetics has been proposed, which also have controversial results.2-4 However, no studies were found in the literature evaluating the efficacy of an oral spray form of a NSAID after tonsillectomy.
Oral spray of flurbiprofen has been approved for adults and children >12 years old for treatment of tonsillitis pain in Turkey; however, it was not previously used for the purpose of posttonsillectomy pain.
The goal in posttonsillectomy pain management is to mobilize the person, to initiate appropriate oral intake as soon as possible, and to reduce the risk of postoperative bleeding. In this prospective randomized double-blind study, we assessed the clinical efficacy of oral spray of flurbiprofen, which is a member of NSAIDs, in reducing posttonsillectomy pain and morbidity.
Materials and Methods
Clinical Trial
Eighty-four patients between the ages of 12 and 45 years who underwent tonsillectomy in Ataturk Training and Research Hospital between August 2014 and May 2015 were included in the study. These patients were separated into 2 groups to receive either flurbiprofen or distilled water as a placebo postoperatively in a randomized, double-blinded fashion. Different oral sprays were given in each group by nursing personnel who otherwise had no contact with the patients or the study. Both sprays were given to patients in similar bottles, and physicians who followed the patients were not informed about the ingredient of the bottles.
Tonsillectomy criteria were 3 attacks per year of chronic and recurrent tonsillitis or 5 attacks in 2 years with symptoms such as fever, snoring, sore throat, and inability to take normal diet. 5 Other inclusion criteria included diagnosis of obstructive sleep apnea with such symptoms as nocturnal snoring with partial upper airway obstruction, complete cessation of airflow with gas exchange abnormalities, and severe disturbance of sleep. Subject eligibility was based on the following exclusion criteria (eligible subjects must not satisfy any of these):
Known hypersensitivity to flurbiprofen
History of allergy to NSAIDs
Known bleeding disorder
Experiencing acute attacks of tonsillitis or peritonsillar abscess
Patients operated for suspicion of benign or malignant tonsillar tumors
Preoperative Evaluation
This study was approved by the ethics committee of the Ataturk Research and Training Hospital (approval 26379996/06). Written informed consents were obtained from all adults and parental consent for participants who were <18 years old. Children also gave verbal and written assent for the research. Use of anticoagulants was discontinued 10 days preoperatively. Preoperatively, as a routine procedure, complete blood counts, international normalized ratio, prothrombin time, and activated thromboplastin time were tested. On each operation day, 2 patients were prepared for tonsillectomy: one as selected randomly for the study and the other for the control group by simple randomization. Clinical parameters of height, weight, body mass index, and sex were also recorded.
The Mallampati score was assessed by asking the patient (in a sitting posture) to open his or her mouth and protrude the tongue as much as possible. The anatomy of the oral cavity was visualized—specifically, whether the base of the uvula, faucial pillars, and soft palate were visible. 6 Modified Mallampati scoring was used: class 1—soft palate, uvula, fauces, pillars visible; class 2—soft palate, uvula, fauces visible; class 3—soft palate, base of uvula visible; class 4—only hard palate visible.
Formulation and Packaging
Double blinding was done. The patient who received the drugs and the researcher who administered the drugs were both blinded to the intervention. The flurbiprofen and placebo sprays were prepared in the hospital by an experienced nurse. The drugs were packed by the nurse and named A and B following the codes. Each oral spray, either flurbiprofen or placebo, was filled into similar 30-mL bottles, and first applications were done by the nurse to tonsillectomy area with the help of tongue depressor. The commercial preparation of liquid flurbiprofen (30-mL bottle contains 0.075 g of flurbiprofen; each spray is 0.13 mL, 0.325 mg), and placebo solutions that were prepared from distilled water were transferred into these bottles. Distilled water and 5% dextrose were mixed with a ratio of 3:1 for replicating the taste of flurbiprofen. The subjects were assigned to either flurbiprofen or placebo treatment according to a computer-generated randomization code. Block randomization was done. A copy of the codes was archived at the Department of Biostatistics and another copy sent to the nurse. The participants were enrolled and assigned to intervention by F.G. The nurse gave the prescriptions and the bottles to the patients according to the randomization scheme. Codes were opened in the Department of Biostatistics after the analysis was over. The patients in each group were given 2 sprays to each tonsillar fossa 3 times a day (totally, 0.78 mL and 1.95 mg for 1 tonsillar fossa) after the operation and for 7 days. The dosage of spray was approved for use in this study by the Institutional Review Board, since this was the dose approved for tonsillitis by Ministry of Health in Turkey.
Surgical Technique
The same 2 surgeons (T.M. and F.G.) performed each surgical procedure using the same tonsillectomy method. Tonsillectomy was performed under general anesthesia by blunt dissection, and hemostasis was accomplished by bipolar cautery forceps at 20 W of power.
Postoperative Follow-up
Each patient was followed in the hospital for 2 days and discharged after the proper use of the spray was taught. Patients were told to visit the clinic on third, fifth, and seventh days for follow-up. Postoperative instructions included cold and soft diet for the first 3 days, then warm and soft diet for the next 7 days. Oral antibiotic suspension (sulbactam-ampicillin, 40 mg/kg; or clarithromycin, 10 mg/kg, in case of a history of penicillin allergy) twice a day for a week was administered postoperatively to both groups.
Pain Assessment
A pain rating scale was used to describe how much pain the patients were feeling and to measure how well the treatment was relieving their pain. On the day before surgery, patients were instructed to use the Numeric Pain Rating Scale (NRS) to express pain at swallowing 100 mL of water (0 = no pain, 5 = moderate pain, 10 = worst pain imaginable). 7 Previous studies provided support for the validity of the NRS as a tool to measure both intensity and unpleasantness of acute postoperative pain.8-10 For rescue analgesia, patients could receive diclofenac sodium (100 mg, intramuscular) on request. The maximum daily dose of diclofenac was 200 mg with an interval of 12 hours. No other analgesic was permitted during the first week after surgery. After discharge from the hospital, all injections were performed by primary care physicians on an outpatient basis to the patients who were suffering from pain. We also monitored the fentanyl consumption during anesthesia, surgical blood loss, and postoperative complications.
Analgesic techniques that produce NRS values in the 0-4 range have been reported to represent adequate analgesia. For this reason, the 0-4 range was identified as a “zone of analgesic success.” 11
Epithelialization Scores
Patients were clinically examined at postoperative days 1, 3, 5, and 7 for tonsillary bed healing. The healing was scored per Zodpe et al 12 : 0, complete healing; 1, 1%-25% bare mucosa; 2, 26%-50% bare mucosa; 3, 51%-75% bare mucosa; 4, 76%-100% bare mucosa.
Statistical Analysis
Analysis of categorical data and proportions was performed with the chi-square test. The Kolmogorov-Smirnov test was used to evaluate the distribution of variables. Analysis of continuous data was performed with the Mann-Whitney U test. Differences in NRS scores between the Mallampati groups were tested by 1-way analysis of variance and then by post hoc Tukey tests. In comparison of the different treatments, 95% confidence intervals (95% CIs) were calculated for difference between the mean responses of the 2 groups of patients. P value <.05 was considered significant. Data are expressed as mean ± SD. Data were analyzed using SPSS 22 for Mac.
Results
Patients’ Demographic Data
Of the 97 participants, 84 completed all trial treatments and assessments. Temporary postoperative uvula edema, which prevented the spray to reach the tonsillary bed effectively, developed in 3 patients, and these patients were excluded from the study ( Figure 1 ). The flurbiprofen group consisted of 45 patients (23 male and 22 female) with a mean ± SD age of 25.13 ± 8.18 years (range, 12-45 years); the placebo group consisted of 39 patients (18 male, 21 female) with a mean age of 26.02 ± 7.56 years (range, 12-38 years). Groups were similar in terms of demographics; age, sex, and body mass index (P > .05). The ratios of duration of anesthesia (P = .812), intraoperative fentanyl consumption (P = .912), and surgical-blood loss (P = .776) between the study and control groups were not statistically significant. There were no intraoperative or postoperative complications, bleeding, or adverse effects related to given medications ( Table 1 ).
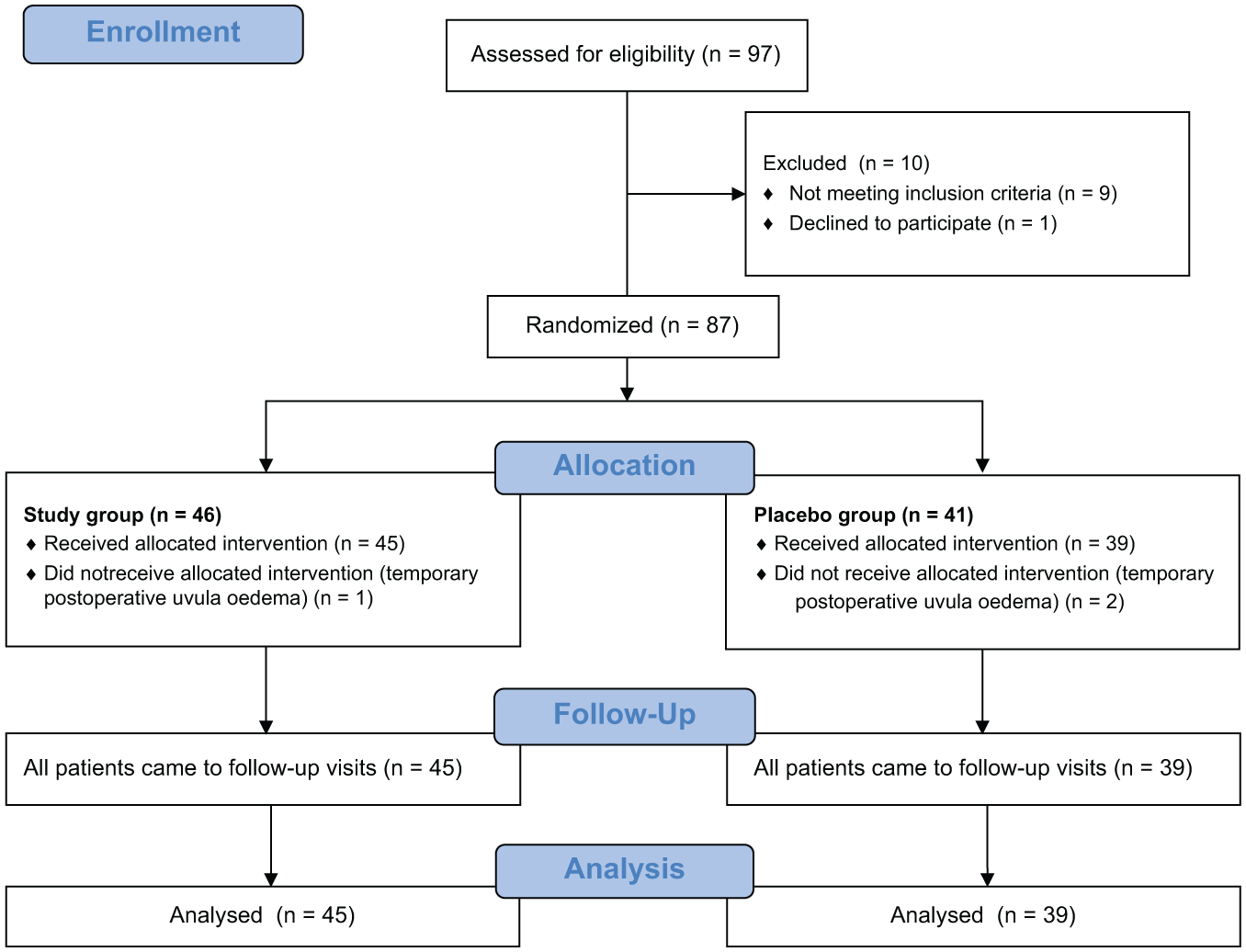
Flow diagram of the study.
Patient Characteristics and Surgical Data of the 2 Groups. a
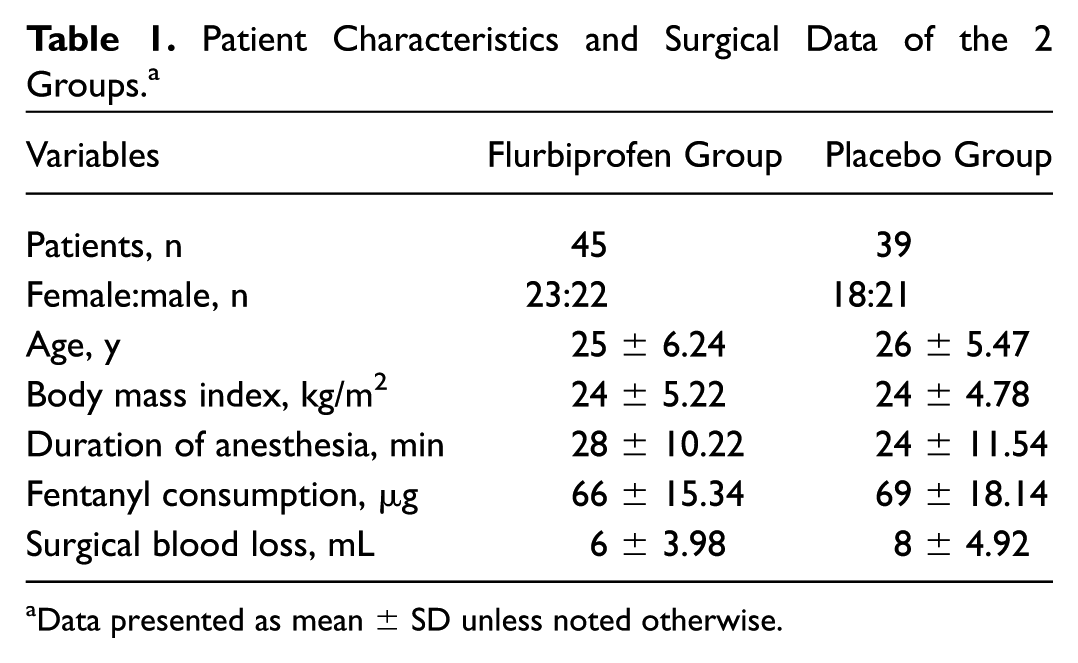
Data presented as mean ± SD unless noted otherwise.
Comparison of Pain Level between the Groups
The severity of throat pain marked on the NRS for pain was lower in the flurbiprofen group when compared with the placebo group, and this difference was statistically significant for all days ( Table 2 ). As illustrated in Figure 2 , the difference in average pain level was significant during the follow-up period (days 1, 3, 5, and 7: P = .000, P = .002, P = .001, P = .000, respectively).
Mean Numeric Pain Rating Scale Values of Posttonsillectomy Pain between the Flurbiprofen and Control Groups. a
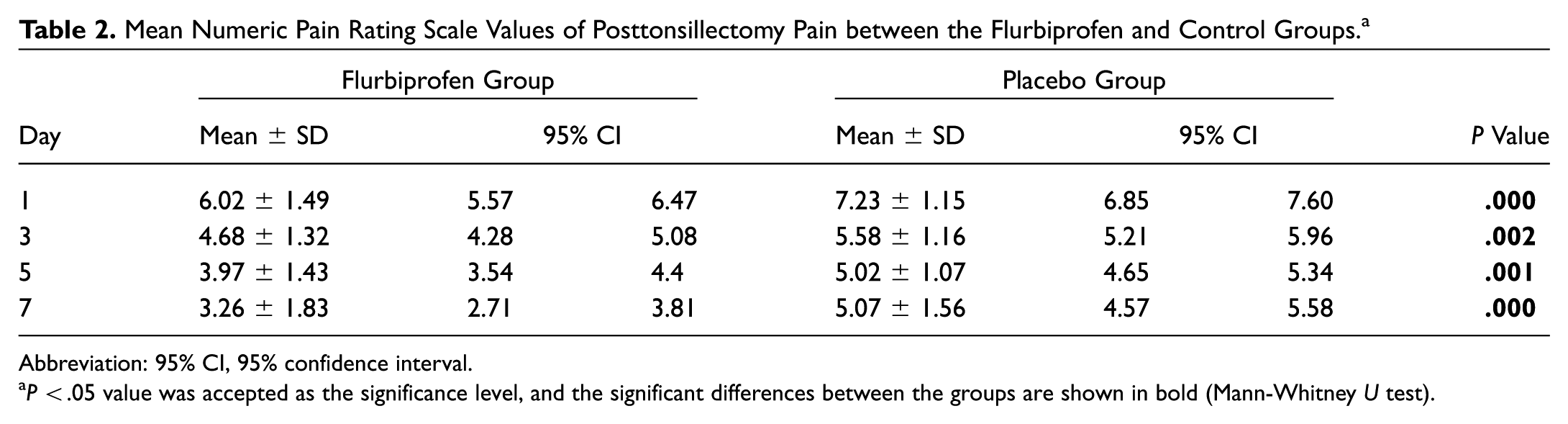
Abbreviation: 95% CI, 95% confidence interval.
P < .05 value was accepted as the significance level, and the significant differences between the groups are shown in bold (Mann-Whitney U test).

Mean Numeric Pain Rating Scale (NRS) scores for pain in flurbiprofen and control groups.
The flurbiprofen group required less analgesic than the placebo group during the study period, and the difference was statistically significant on days 1, 3, 5, and 7 (P = .001, P = .001, P = .03, P = .001, respectively; Table 3 ) Analgesic requirements were also shown as mean values in Figure 3 . During the first week, the participants in placebo group did not receive any pain killers except for the rescue intramuscular injection of diclofenac.
Postoperative Analgesic Requirements.
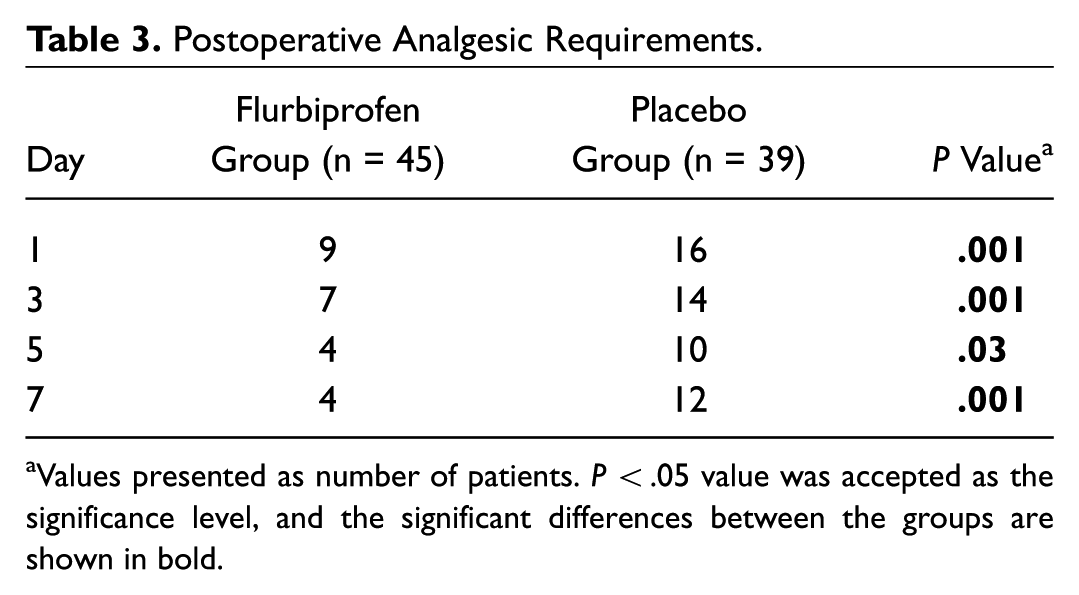
Values presented as number of patients. P < .05 value was accepted as the significance level, and the significant differences between the groups are shown in bold.
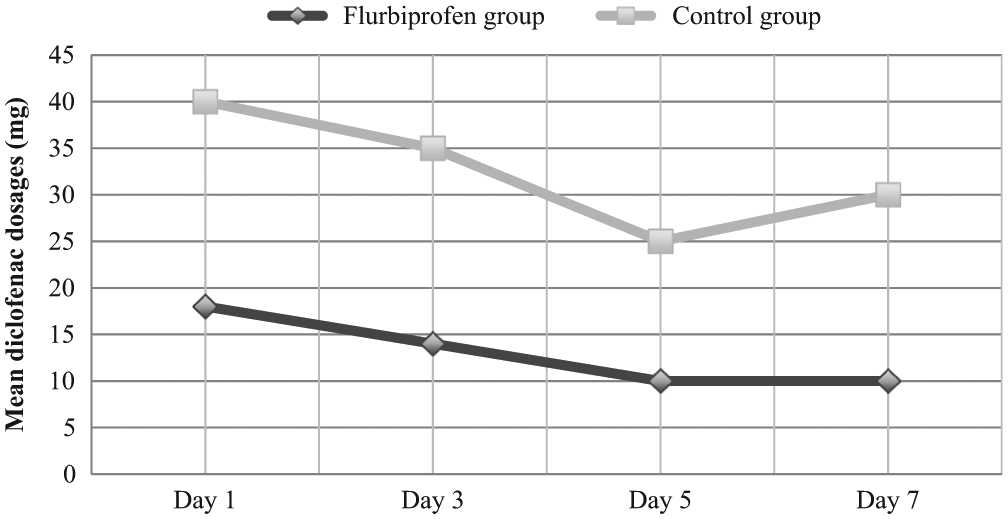
Analgesic dosages required.
For clinical significance, the 95% CIs for the mean NRS scores were shown in Table 2 . The 95% CIs for the difference in pain scores at days 1, 3, 5, and 7 between the 2 groups are shown in Figure 4 .
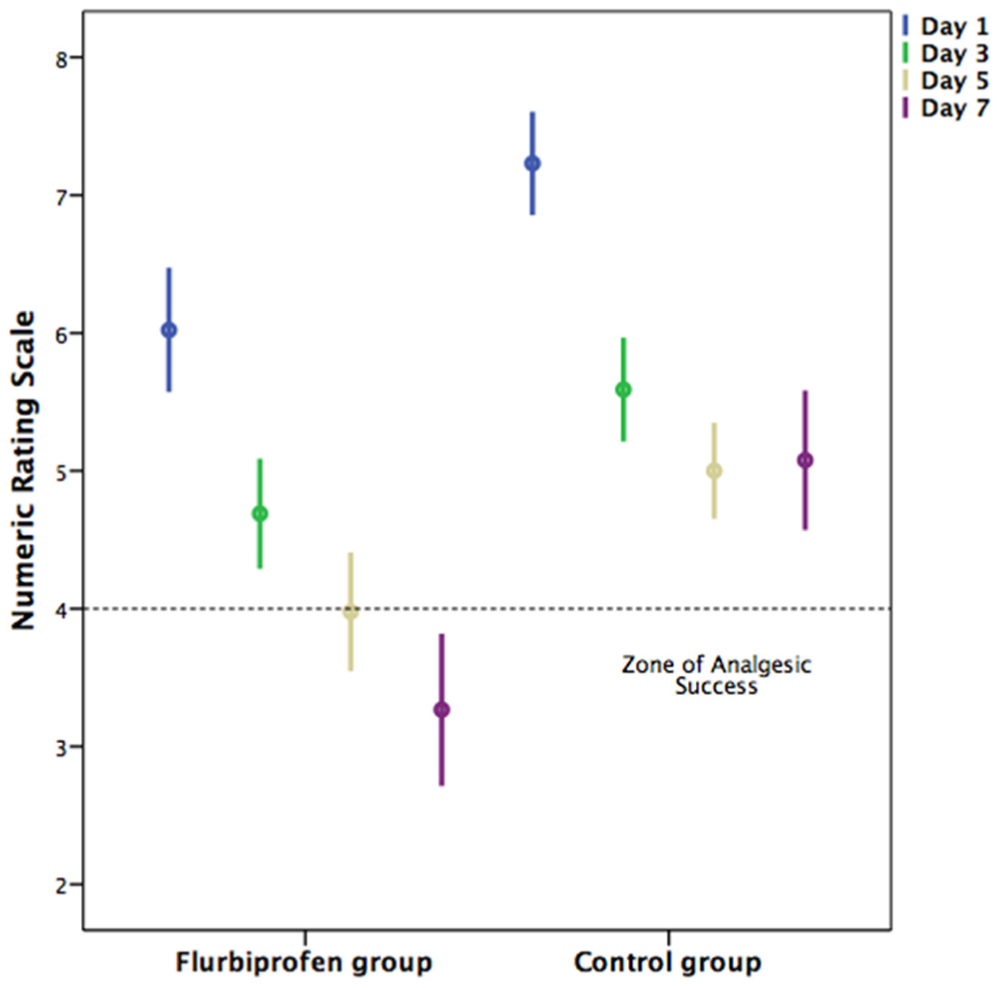
Assessment of the clinical significance of an analgesic technique based on 95% confidence intervals for the mean.
Epithelialization Comparison
The patients were examined for epithelization on days 1, 3, 5, 7 postoperatively, and most of them—77% (35 patients) in flurbiprofen group and 64% (25 patients) in placebo group—showed grade 1 epithelization on day 3. Moreover, 80% (36 in flurbiprofen group, 31 in placebo group) showed grade 3 epithelization in both groups on day 7. Healing of the tonsillary bed was not significantly different between groups (P = .725).
None of the patients reported significant bleeding that may need surgical intervention or hospital readmission in both groups.
Impact of Mallampati Class on the Effectiveness of the Spray
In the flurbiprofen group, 7 patients had a Mallampati class 4; 11 patients, class 3; 13 patients, class 2; and 14 patients, class 1. Mallampati class 4 had higher mean pain scores than other groups in terms of NRS scores on day 5 and day 7 ( Figure 5 ), and patients with Mallampati class 3 had higher NRS scores on days 3, 5, and 7 than patients with Mallampati classes 1 and 2, as shown by 1-way analysis of variance ( Table 4 ). Moreover, in post hoc Tukey multiple comparison tests between NRS and Mallampati classification, there were no statistically significant difference between or within the groups on days 1 and 5. On day 3, the difference between classes 2 and 3 was statistically significant (P = .047). On day 7, the differences between classes 4 and 1 and between classes 4 and 2 were statistically significant (P = .044, P = .01, respectively,).
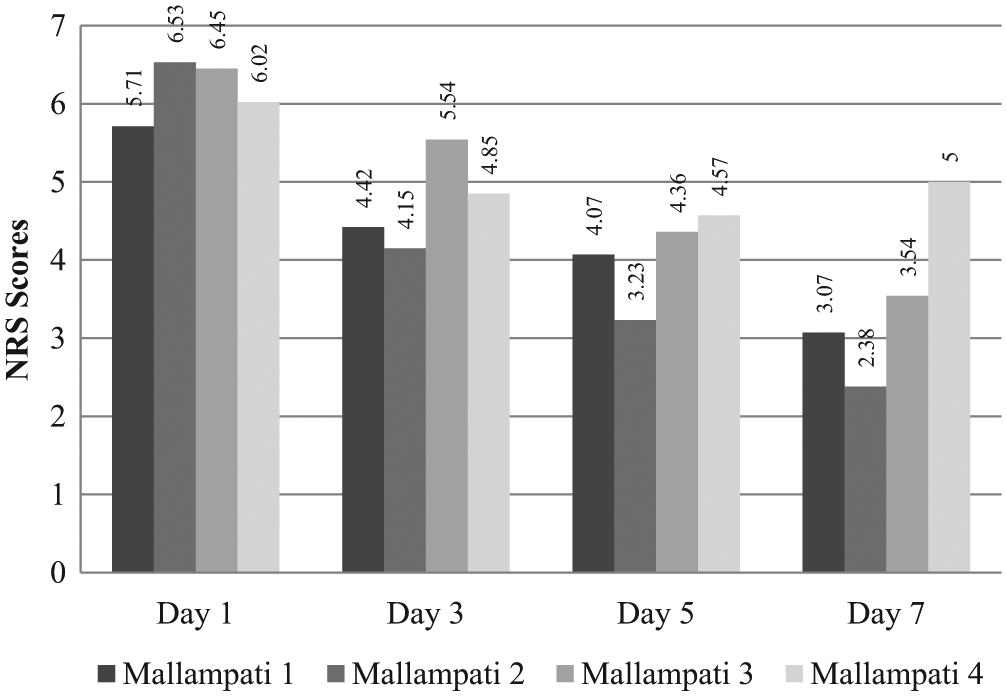
The relationship between mean Numeric Pain Rating Scale (NRS) scores and Mallampati scores in the flurbiprofen group.
Differences between Mallampati Scores and Numeric Pain Rating Scale Scores in the Flurbiprofen Group. a
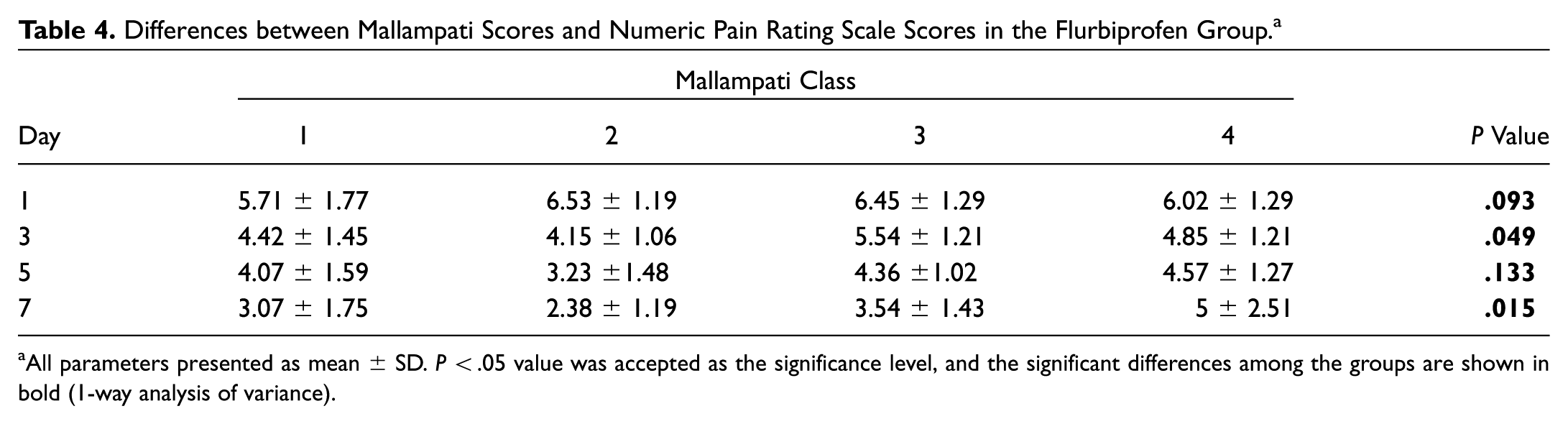
All parameters presented as mean ± SD. P < .05 value was accepted as the significance level, and the significant differences among the groups are shown in bold (1-way analysis of variance).
Discussion
The patient’s quality of life and most of the complications that occur during posttonsillectomy period are directly associated with pain, so it is very important, yet difficult, to control posttonsillectomy pain. In this study, we conducted a double-blind, randomized, placebo-controlled study evaluating the effects of oral flurbiprofen spray in patients who underwent tonsillectomy.
In the ophthalmology literature, topical ophthalmic NSAIDs are widely used for surgical pain. In the otolaryngology literature, topical lidocaine, bupivacaine, and topical application of opioid analgesics are used for posttonsillectomy pain relief. In addition, topical spray of diclofenac sodium is widely used for transdermal application, especially for treatment of signs and symptoms of rheumatic diseases. The mechanism of action of topical NSAIDs is similar to that of other nonsteroidal anti-inflammatory NSAIDs. They inhibit the enzyme cyclooxygenase—an early component of the arachidonic acid cascade—resulting in the reduced formation of prostaglandins, thromboxanes, and prostacyclin. But it is not completely understood how reduced synthesis of these compounds results in therapeutic efficacy.
The pain after tonsillectomy may be caused by inflammation, nerve irritation, and spasm of the exposed pharyngeal muscles, and it does not completely subside until the muscle becomes covered with mucosa 14 to 20 days after surgery. 13 In our study, epithelization scores of tonsillar fossa showed 80% healing on day 7, which is in concordance with previous literature. Patients in the oral flurbiprofen spray group did not show a significant difference in healing scores when compared with the placebo group (P > .05).
After tonsillectomy, pain may impair swallowing, leading to an increased risk of secondary infection, bleeding, and dehydration, resulting in prolonged hospitalization or occasional rehospitalization in the following days. 14 Many studies have been conducted to investigate the role of analgesic drugs in preventing posttonsillectomy pain; however, these agents are also strong inhibitors of prostaglandins and platelets and can be related to an increased incidence of postoperative bleeding and stomach and intestinal adverse reactions, such as bleeding, ulcers, and perforation of the stomach or intestines. There are few data available on the role of oral sprays in pain relief. A prospective study by Valijan demonstrated that benzydamine hydrochloride spray does not relieve the symptoms on posttonsillectomy patients when compared with placebo. 15 However, Kaygusuz et al demonstrated that 10% lidocaine hydrochloride sprayed on tonsillectomy fossa 4 times a day decreased the pain significantly when compared with placebo. 16 From the first postoperative day to the end of the seventh day, the patients who used flurbiprofen spray had significantly lower pain scores than the control group (days 1, 3, 5, and 7: P = .000, P = .002, P = .001, P = .000, respectively).
However, to determine clinical significance, confidence intervals (95%) of the groups were compared, as shown in Figure 4 , which illustrates the zones of “analgesic success” (0-4) and “analgesic failure” (4-10). Although days 1 and 3 were in the analgesic failure zone in both groups, pain scores of the flurbiprofen and control groups at days 1, 3, 5, and 7 were significantly different (P < .05), because the 95% CI did not overlap in each day. This situation may be explained by the fact that the patients with high Mallampati scores reduced the applicability of the spray. However, pain relief seems to be better at days 5 and 7 in the flurbiprofen group.
The patients with high Mallampati scores may have an elongated uvula, redundant soft palate tissue, and macroglossia. All these structures reduce the size of the oral cavity and obscure the posttonsillectomy fossa, especially among patients with Mallampati classes 3 and 4. These structures also tend to prevent the spray from reaching the pharynx, throat, or posterior part of the mouth where the posttonsillectomy fossa is located, as well as the dorsal portion of the tongue. Our study showed that the patients with Mallampati classes 3 and 4 had a higher pain scores on days 3, 5, and 7 when compared with the patients with Mallampati classes 1 and 2. Moreover, on days 3 and 7, pain scores were significantly different between the groups (P = .049, P = .015, respectively). In a post hoc Tukey test, Mallampati class 3 had statistically higher pain scores on day 3 and class 4 on day 7 (P = .042, P = .025, respectively). These results suggested that oral flurbiprofen spray may not be adequately effective to control posttonsillectomy pain in higher Mallampati scores, especially in classes 3 and 4.
It is known that throat pain may come in 2 peaks after tonsillectomy: the first within the first days and the second at about 7 to 10 days. The second pain attack peaks around days 7 to 10, when the scabs from the wound begin to fall off. In this study, analgesic requirement was higher in the placebo group on days 1, 3, 5, and 7 (P = .001, P = .001, P = .03, P = .001, respectively). Moreover, analgesic requirement was correlated with Mallampati classes: patients with higher Mallampati classes required a higher dosage of rescue analgesic.
In the literature, the only adverse effect (reported as a case) was fatal hypersensitivity reaction to flurbiprofen spray prescribed for acute pharyngotonsillitis. The cause of death was heart failure with acute asphyxia from edema of the glottis. 17 Although allergy to flurbiprofen has rarely been documented, the allergic reaction may be associated with propionic acid derivatives, which have a relatively high frequency of allergic reactions. To minimize the risks of side effects, we used flurbiprofen, which does not contain propionic acid derivatives, and no adverse effects were observed in our patients. Our results showed better pain-controlling results for the flurbiprofen group for posttonsillectomy pain. Fortunately, no adverse reactions were noted, such as bleeding, readmission to hospital, and allergic reactions.
The weakness of this study was the small and heterogeneous sample size. However, the study reached statistical significance. When we evaluated the clinical significance, the same significance could not be reached. If the patients with higher Mallampati scores were recruited from the study, it could have probably resulted in a higher clinical significance. Another weakness could be the fact that mouth opening was limited due to pain when the drugs were sprayed into the tonsillary bed, especially in children. As a result, further studies are needed to elucidate the role of flurbiprofen spray for wide use in posttonsillectomy pain management strategies.
Conclusions
This study showed that the use of oral flurbiprofen spray, compared with placebo, has acceptable advantages in managing pain after tonsillectomy. It is a novel and safe alternative in managing postoperative pain after tonsillectomy, with preliminary results.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.