
Abstract
Objective
To determine the variables that are predictive of failed decannulation (FD), delayed decannulation (DD), and days to decannulation in patients who underwent head and neck cancer resection with free tissue transfer reconstruction for head and neck squamous cell carcinoma.
Design
Case series with chart review.
Setting
Tertiary care otolaryngology–head and neck surgery referral center.
Subject and Methods
Patients (N = 108) were included who underwent head and neck cancer resection with free tissue transfer reconstruction and tracheostomy between 2011 and June 2014. Patients with laryngectomy, previous tracheostomy, and other airway pathology necessitating tracheotomy were excluded. Preoperative patient variables and cancer site/staging variables were analyzed, as well as extent of structures resected and type of reconstruction. Univariate and multivariate binary logistic and Cox regression analyses were used to determine predictors of FD and DD. Cox regression analysis was used to determine predictors of days to decannulation.
Results
Of the 108 included patients, 16 had FD, and 26 had DD. Univariate analysis demonstrated that advanced stage (r = 0.233, P = .021), total glossectomy (r = 0.924, P < .001), anterolateral thigh flap reconstruction (r = 0.906, P < .001), smoking at time of surgery (r = 0.319, P = .002), and pack years (r = 0.322, P = .001) were associated with FD. Cox regression analysis showed that total glossectomy, exp(B) = 15.837 (95% confidence interval [95% CI]: 1.949-128.679); anterolateral thigh flap reconstruction, exp(B) = 8.439 (95% CI: 2.435-29.620); and smoking status, exp(B) = 2.970 (95% CI: 1.617-5.456) were independent predictors of days to decannulation and FD.
Conclusions
Patients with total glossectomy defects and those who continue to smoke are at increased risk for FD and DD. Aggressive smoking cessation programs may decrease the risk of FD and DD. Patients should be counseled about their risk profiles.
Patients with head and neck cancer (HNC) are frequently treated with combination therapy that includes surgical resection with or without surgical defect reconstruction. Tracheotomy is a procedure commonly performed at the time of HNC resection and free tissue transfer reconstruction (HNC-RR) as a temporary airway. 1 This definitive surgical airway is used to bypass the extensive postoperative upper airway edema that occurs as a result of HNC-RR. Patients are normally decannulated within 10 days following surgery such that speech and swallowing rehabilitation can begin. 2
A subset of HNC-RR patients will fail to decannulate within 10 days, resulting in a prolonged or permanent tracheostomy. Delayed decannulation (DD) can result in significant morbidity: it can increase the length of hospital stay and delay speech and swallowing rehabilitation, and it is more likely to be associated with other postoperative complications.3-6 Failed decannulation (FD) is a significant potential complication, as a permanent tracheostomy significantly affects a patient’s quality of life, increases cost related to long-term tracheostomy care, and predisposes to months and years of potential complications relating to tracheostomy.5,7 Indeed, there is a growing emphasis on functional outcomes and quality of life in the treatment of head and neck squamous cell carcinoma (HNSCC).8,9 As such, knowledge of the variables that can predict DD or FD is potentially very useful: modification of these risk factors can decrease the rate of FD/DD, and the knowledge of nonmodifiable risk factors would allow for appropriate counseling of patients regarding their risk profiles.
Several studies have examined variables that are predictive of FD/DD following tracheotomy for various indications other than HNC-RR,10-16 such as increased patient age,10,14 peak flow rate during induced cough, 11 male sex, 14 and several others. Of note, Hernández et al found that the indication for tracheotomy significantly affects the variables that are predictive of FD, 14 indicating that the predictors may be unique in HNC-RR patients.
One study examined tracheostomy-related complications in HNC-RR patients. 2 This study identified that free tissue transfer reconstruction, primary site (anterior tongue and floor of mouth), age, and preoperative radiation were predictive of DD. However, this study was not specific to patients undergoing HNC-RR, as only a small subset of patients had free tissue transfer reconstruction. It also examined all tracheostomy-related complications and did not examine predictors of FD. Thus, the predictors of FD and DD in HNC-RR patients are not well understood.
The primary objectives of this study were to determine the variables that are predictive of FD, DD, and days to decannulation following HNC-RR.
Methods
Institutional ethics review board approval was obtained from the University of Alberta Health Research Ethics Board (Panel B) prior to commencement of this study (Pro00053638). We conducted a retrospective review of all patients who underwent HNC-RR between January 2011 and January 2014 at the University of Alberta Hospital. All patients with HNC-RR are managed postoperatively with a standardized province-wide head and neck reconstruction clinical pathway.17,18 This includes downsizing tracheostomy tubes between postoperative days 3 and 5, with the goal of decannulation between postoperative days 4 and 7. According to the pathway, the clinical decision of decannulation is made only after a patient has had the tracheostomy tube plugged for at least 24 hours continuously with no desaturations, oxygen requirements, need for suctioning, or respiratory distress.
Inclusion criteria were all adults with a biopsy-proven diagnosis of HNSCC and preoperative staging imaging (computed tomography scan or equivalent). Patients must have had a tracheotomy at the time of HNC-RR. Patients were excluded from the study if they underwent surgery for a nonmalignant indication or a primary pathology other than HNSCC or if the pathology report or imaging was unavailable, as final pathologic staging is known to have a less-than-excellent correlation with preoperative clinical staging. 19 Patients with a history of HNC-RR, prior radiation to the head and neck, or a laryngectomy; patients who died before 60 days after surgery; and those who had a tracheostomy prior to HNC-RR were also excluded. If a patient was found to have airway pathology necessitating tracheotomy other than HNC-RR, such as subglottic stenosis or vocal fold paralysis, he or she was also excluded.
One of 2 reviewers (A.I., S.V.) collected patient charts to determine eligibility criteria and extract the variables under review. The main outcome variable was the number of days between tracheotomy and decannulation. FD was defined as persistent tracheostomy at the time of discharge from hospital after HNC-RR and/or persistent tracheostomy >60 days after HNC-RR. DD was defined as persistent tracheostomy >10 days after HNC-RR and not fulfilling criteria for FD. There are no established criteria for defining DD in the literature; however, the cutoff of 10 days was chosen because it is after 10 days that the presence of the tracheostomy becomes the primary barrier to discharge and speech and swallowing rehabilitation.
The variables under study included patient factors, cancer TNM stage and subsite, mode of treatment (surgery, radiation, chemotherapy, or combination), postoperative surgical defect, and details of reconstruction, including type of free flap. Patient factors included age, sex, Charlson Comorbidity Index, Eastern Cooperative Oncology Group performance score, obesity (body mass index ≥30), and smoking status. A “current smoker” was defined as a patient who was smoking at least 5 cigarettes per day within 4 weeks of surgery. A “previous smoker” was defined as a patient who had quit smoking prior to 4 weeks before surgery. Postoperative defect was classified as <50% or ≥50% resection of each specific oral cavity or oropharyngeal subsite or structure.
Descriptive and inferential statistics were performed with SPSS 22. Univariate Pearson correlation coefficients were between each predictor variable and both FD and DD. Multivariate binary logistic regressions were used to determine independent predictors of DD (including patients with DD and FD) as well as independent predictors of FD only. Multivariate Cox hazard regression analysis was used to determine independent predictors of days to decannulation. The significance level was set at P = .05. Any predictor variable that met a statistical significance of P = .10 in univariate analysis, as well as any variables deemed clinically significant, were included in the multivariate analysis.
Results
In total, 386 patients were identified as eligible for inclusion into the study. Of these, 106 were excluded because they underwent a laryngectomy; 39 did not have a tracheotomy at the time of HNC-RR; 45 had a primary pathology other than HNSCC; and 24 had a tracheostomy prior to HNC-RR or had a separate indication for tracheostomy. Sixty-two patients either did not have a staging computed tomography scan, or the computed tomography and/or final pathology report was unavailable. Two patients died before postoperative day 60. This resulted in 108 patients being included in the study. The mean age was 63 years, with 56% men. The majority of patients (81%) had advanced HNSCC (stage III or IV); 57% had oral cavity HNSCC; and the remaining had oropharyngeal HNSCC ( Table 1 ).
Demographics and Selected Descriptive Statistics of Patient Cohort (N = 108). a
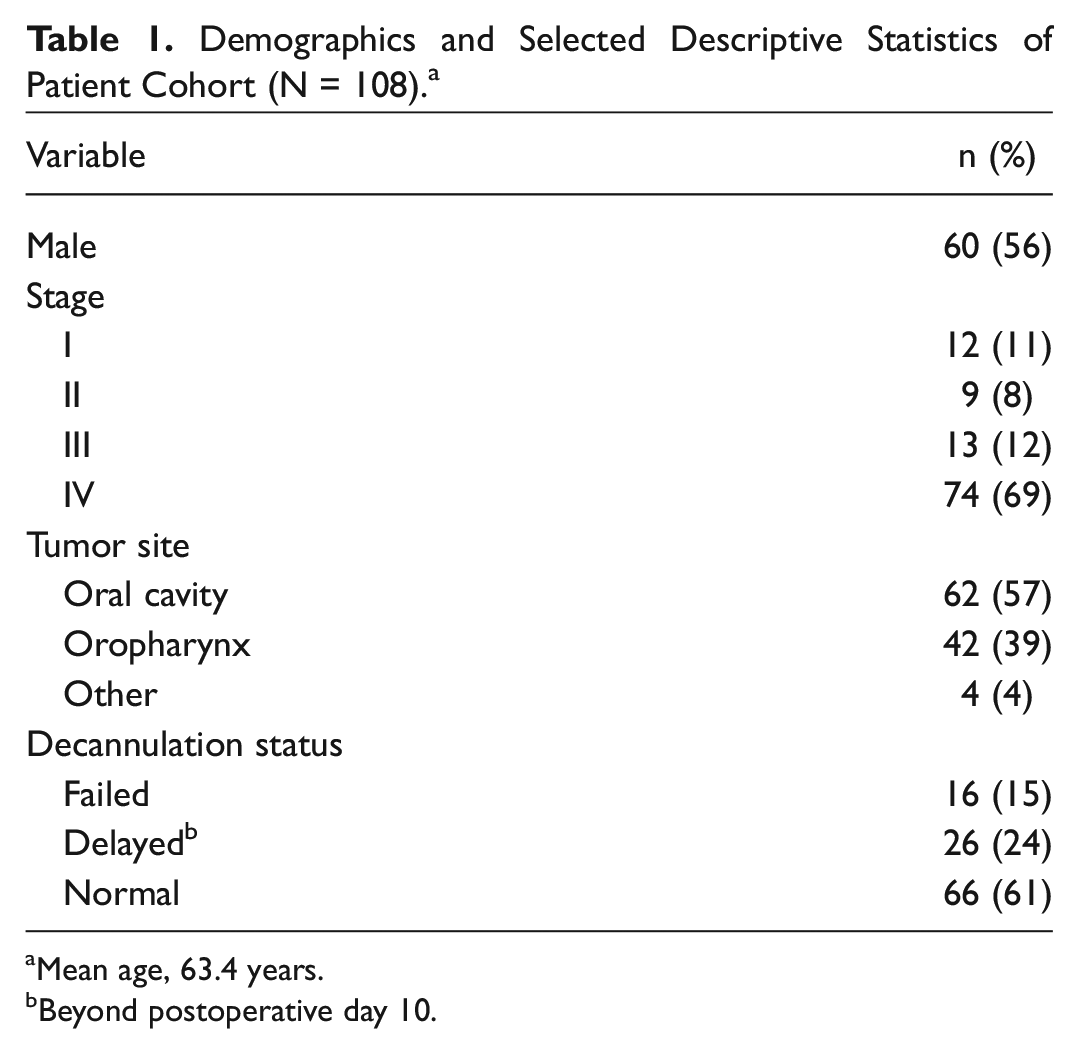
Mean age, 63.4 years.
Beyond postoperative day 10.
Of the 108 included patients, 16 (15%) had FD, and 26 (24%) had DD. On univariate analysis (see Table 2 ), variables that were associated with FD included advanced stage (r = 0.23, P = .02), pathologic tumor stage (r = 0.32, P < .01), Eastern Cooperative Oncology Group score (r = 0.25, P = .02), total glossectomy defect (r = 0.92, P < .01), total base-of-tongue resection (r = 0.67, P < .01), anterolateral thigh flap (ALTF) reconstruction (r = 0.91, P < .01), and smoking status (r = 0.32, P < .01). Radial forearm free flap reconstruction was negatively associated with FD (r = −0.25, P = .02). Additional variables that were associated with DD included Charlson Comorbidity Index score (r = 0.28, P = .01) and Eastern Cooperative Oncology Group score (r = 0.21, P = .04).
Univariate Analysis of Variables Associated with Failed and Delayed Decannulation. a
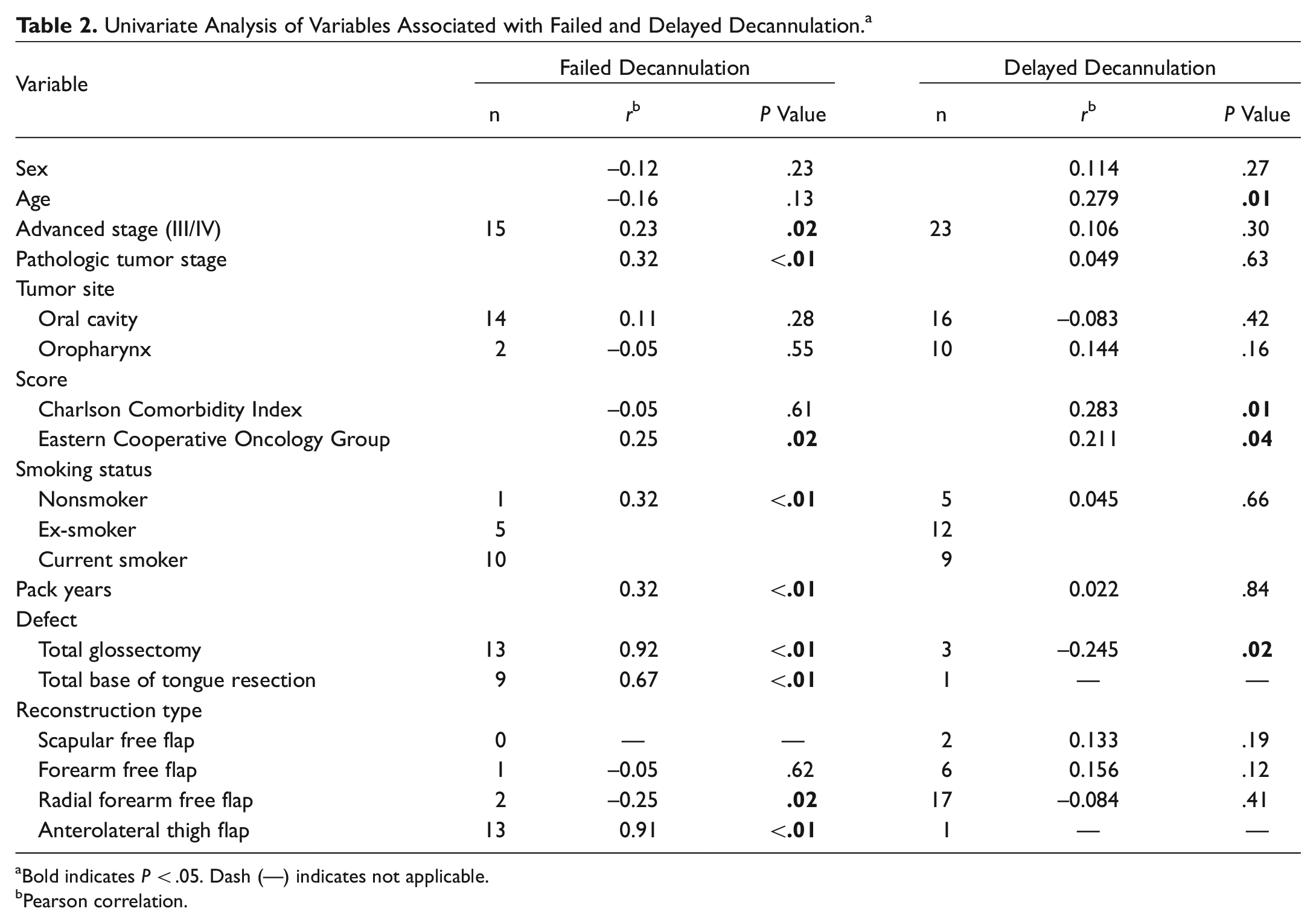
Bold indicates P < .05. Dash (—) indicates not applicable.
Pearson correlation.
In multivariate binary logistic regression, total glossectomy defect, exp(B) = 5.14 (95% confidence interval [95% CI]: 1.80-14.50); current smoking, exp(B) = 35.38 (95% CI: 1.86-173.47); and ALTF, exp(B) = 7.65 (95% CI: 3.71-15.80) were strong independent predictors of FD ( Table 3 ). None of the variables were significant independent predictors of DD in multivariate binary logistic regression. Cox hazard regression demonstrated that total glossectomy defect, exp(B) = 15.84 (95% CI: 1.95-128.68); ALTF reconstruction, exp(B) = 8.44 (95% CI: 2.44-29.62); and current smoking, exp(B) = 2.97 (95% CI: 1.62-5.46) were all independent predictors of increased days to decannulation ( Figures 1 and 2 ). Notably, patients who continued to smoke had a higher rate of FD and were decannulated on average 4 days later than nonsmokers. Of the 16 patients with FD, 4 achieved decannulation at last follow-up (range, 6 months to 3 years).
Multivariate Binary Logistic Regression of Predictors of Failed Decannulation.
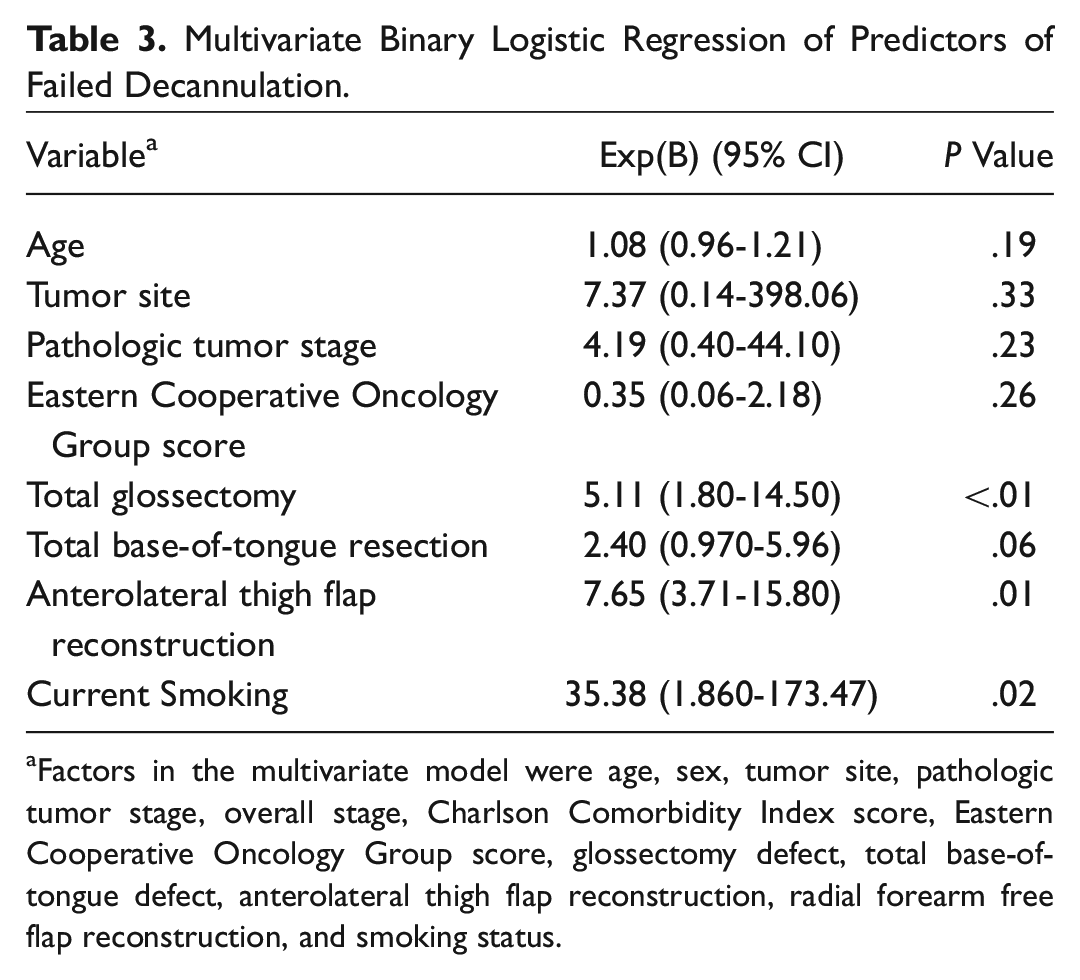
Factors in the multivariate model were age, sex, tumor site, pathologic tumor stage, overall stage, Charlson Comorbidity Index score, Eastern Cooperative Oncology Group score, glossectomy defect, total base-of-tongue defect, anterolateral thigh flap reconstruction, radial forearm free flap reconstruction, and smoking status.
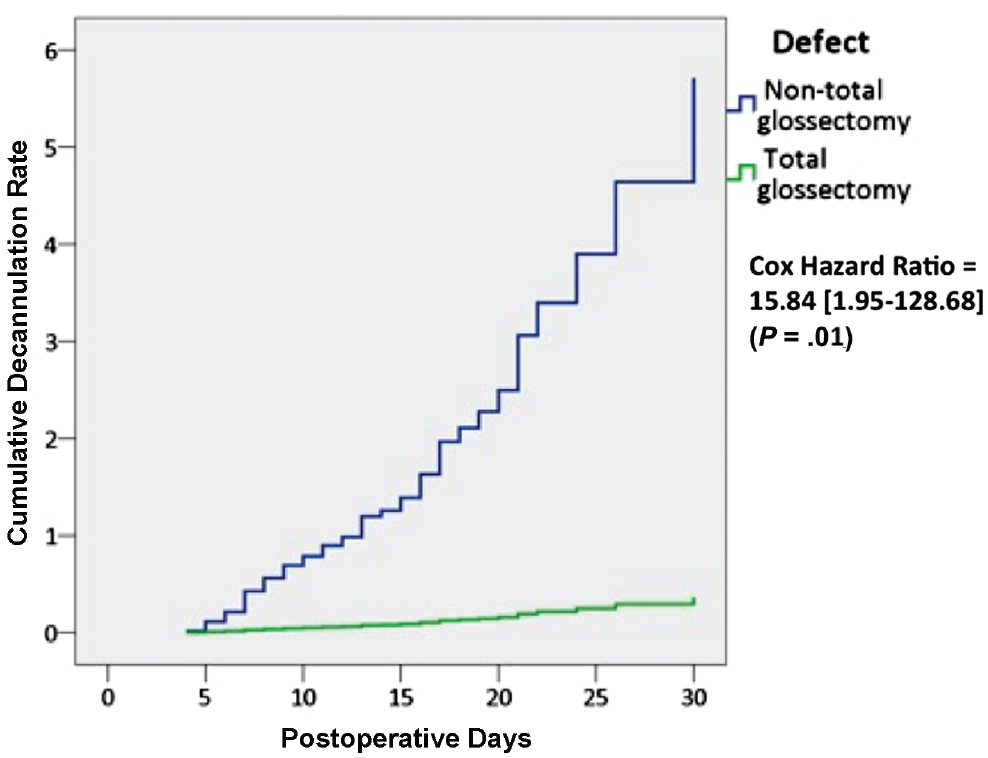
Cox hazard regression of decannulation in patients with total glossectomy defects vs patients with total glossectomy defects.

Cox hazard regression of decannulation in current smokers, ex-smokers, and lifetime nonsmokers.
Discussion
Patients with HNSCC often require multimodality treatment, with surgery being one of the mainstays.20,21 Patients who undergo HNC-RR for HNSCC often require significant postoperative care, in the immediate postoperative period as well as with speech and swallowing rehabilitation. The postoperative course requires significant patient education regarding what will be involved in postoperative rehabilitation; however, the significance of the tracheostomy can sometimes be overlooked because it is viewed as a temporary airway procedure in cases of HNC-RR. There is an extreme paucity of literature on tracheostomy-related complications in HNC-RR patients, particularly in relation to the risk of FD and DD. This can make patient counseling difficult, especially in those who suffer the complication of FD, because they often feel unprepared to manage a tracheostomy at home and are not routinely counseled on this preoperatively.
This study demonstrated that FD and DD may not be as uncommon as previously thought (15%). What makes this finding more significant is that FD can be predicted preoperatively in the majority of cases. As demonstrated in the multivariate analysis, patients who require a total glossectomy for a large oral cavity tumor should be counseled that they are 5 times more likely to have FD over those that do not require a total glossectomy. This is likely multifactorial, but a large part is thought to be due to the inability to properly handle and swallow oral secretions, which may preclude the ability to decannulate. In this study, however, it was not possible to determine the reason for FD (eg, pulmonary toilet, failure to handle secretions, lack of upper airway patency). This complication was also highly related to ALTF reconstructions in this study, and this was likely due to the fact that total glossectomy defects are often reconstructed with the ALTF at our center, as it provides the necessary soft tissue bulk to adequately reconstruct very large oral and oropharyngeal defects. ALTF reconstruction in general is often used for more extensive surgical defects and was likely a surrogate marker for a larger defect in our patient cohort. In the Cox hazard regression, total glossectomy defects and ALTF were independently predictive of a longer time to decannulation, although the effect of the total glossectomy defect was almost twice as much as that of the ALTF. In univariate analysis, radial forearm free flap was negatively associated with FD, likely because it was more commonly used for smaller defects in this patient population.
The predictive value of smoking status is critical for preoperative patient counseling. Patients who continued to smoke beyond the 4-week preoperative time were 35 times more likely to suffer FD and were also more likely to have a longer time to decannulation. This is in keeping with other literature demonstrating that smokers are more likely to suffer postoperative complications for HNSCC, 3 although this was not specific to tracheostomy complications. Other studies have also shown that smokers have increased intra- and postoperative sputum production, which may make decannulation more difficult. 22 Smoking cessation, however, has been shown to significantly decrease the number of postoperative complications if it occurs as little as 4 weeks preoperatively. 23 Smoking cessation has also been shown in the pulmonary literature to result in a measurable improvement in pulmonary function, including forced expiratory flow. 24 This may in part help to explain the difference in decannulation rate found between current smokers and ex-smokers/nonsmokers, especially in light of the fact that peak flow rate during induced cough may be predictive of successful decannulation. 11 This is important in counseling patients who are continuing to smoke at the time of diagnosis and/or at the time of decision to proceed with surgery for HNSCC. This population is composed of patients who continue to smoke despite being diagnosed with a highly smoking-related malignancy, thus clearly finding it difficult to quit. The knowledge that continuing to smoke significantly increases the risk of having a permanent or prolonged tracheostomy can provide extra motivation and a highly tangible goal for cessation. Evidence has shown that high-intensity smoking cessation programs can be very successful if begun even weeks before surgery and the cessation rate is maintained at least 12 months after surgery. 23
Limitations of this study included that it was retrospective, which precluded the measurement of some variables, such as alcohol use as well as the reason for failure to decannulate, which may have given further insight into the risk factors. For example, the decision to leave a tracheostomy tube in place may in some cases be influenced by the need for postoperative radiation and supine positioning. Nevertheless, postoperative radiation was not significantly associated with FD or DD in this patient cohort. This was also a small cohort, which is problematic when determining predictors associated with a relatively rare complication such as FD, and such some predictors may have been missed. Finally, all patients were treated at a single center with a single treatment paradigm, which may limit the applicability of this study to other centers that perform head and neck surgery.
In the future, we plan to perform a larger prospective study examining predictors of FD and DD that would account for other variables not examined here. This would include a preoperative evaluation of each patient’s need for tracheostomy, as other studies have identified that some oral cavity free flaps can be safely performed without a tracheostomy. 25
Conclusion
FD and DD are infrequent but important complications of HNC-RR with tracheotomy. Patients with total glossectomy defects and those who continue to smoke at the time of surgery are at increased risk. Early smoking cessation and education programs may have the potential to decrease the incidence of these complications. Patients should be appropriately counseled about their personal risk profile for before undergoing HNC-RR.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the 2015 AAO-HNSF Annual Meeting & OTO EXPO; September 27-30, 2015; Dallas, Texas.