
Abstract
Objective
Given that 30% to 40% of children have persistent obstructive sleep apnea (OSA) after adenotonsillectomy, we evaluated whether children with hypopnea-predominant OSA were more likely to have complete disease resolution after adenotonsillectomy than those with apnea-predominant disease. We also identified risk factors that might modify the relationship between disease resolution and polysomnographic event type (ie, hypopnea vs apnea).
Study Design
Case series with chart review.
Setting
Tertiary pediatric hospital.
Subjects/Methods
Consecutive 1- to 18-year-old typically developing children diagnosed with OSA from March 2011 to December 2012 underwent adenotonsillectomy and completed pre- and postoperative polysomnography within 1 year of surgery.
Results
Fifty-eight children were included (27 female; mean ± SD: age, 5.6 ± 3.1 years; body mass index z score, 1.1 ± 1.7). Overall, adenotonsillectomy resulted in significant improvement in obstructive apnea-hypopnea index (oAHI) from 23.3 ± 40.0 to 4.3 ± 8.2 events per hour (P < .001), obstructive apnea index (5.1 ± 7.4 to 0.4 ± 0.8, P < .001), and obstructive hypopnea index (oHI; 18.1 ± 37.5 to 3.7 ± 8.1, P < .001). There was complete response (oAHI <1.0 event/h) in 24 of 58 patients (41%) but no difference by event type (P = .11). On univariate analysis, only race, sex, oxygen saturation nadir, and oHI were predictive of response to adenotonsillectomy, while multivariate analysis found that prematurity, age, oxygen saturation nadir, oHI, obstructive apnea index, and oAHI were predictive. Event type was not significant, even in a model controlling for age, race, sex, prematurity, asthma, body mass index, and baseline polysomnographic variables.
Conclusion
This small study demonstrated no difference in disease resolution between children with hypopnea- and apnea-predominant OSA who underwent adenotonsillectomy. Additionally, adenotonsillectomy significantly improved OSA in most children, and high preoperative oAHI was associated with persistent postoperative OSA.
Obstructive sleep apnea (OSA) is a common and well-recognized disorder affecting 1% to 5.8% of children in the United States.1-4 Major risk factors for the development of OSA include adenotonsillar hypertrophy, male sex, obesity, and the presence of coexistent neurologic disorders.1,3,5,6 The short- and long-term consequences of untreated disease can be serious, with numerous studies documenting increased hyperactive behavior, neurocognitive deficits, and cardiovascular complications.6-10 In view of these significant sequelae, it is essential for clinicians to recognize OSA and ensure that affected children receive appropriate treatment.
Overnight polysomnography (PSG) is the gold standard for diagnosis. It provides quantitative data regarding the frequency and duration of 2 distinct OSA event types—hypopneas and apneas. As well, PSG is used postoperatively to determine whether surgery has yielded complete versus partial resolution of disease.
Surgical removal of the tonsils and adenoids (T&A) is the first-line treatment for pediatric OSA. This approach results in complete disease resolution in 60% to 70% of children, and an even greater number have an improved quality of life after surgery11-13; 30% to 40% are, however, left with persistent disease, as measured by postoperative PSG.14,15
Risk factors for persistent OSA include a wide spectrum of medical comorbidities as well as older age, obesity, craniofacial deformity, and Down syndrome.1,14-16 Studies also show that children with more severe OSA are more likely to have persistent disease after T&A.17-20 The identification of specific risk factors is critical, as it enables clinicians to individualize treatment and make certain that children are adequately followed postoperatively. Characteristics of preoperative PSG have been explored to predict outcomes of adenotonsillectomy. 21 However, what remains unanswered is whether general practitioners can use specific PSG results, such as the effect of hypopnea versus apnea predominance of obstructive events, to predict outcomes after surgery.
Although clinicians are generally taught that children with partial airway obstruction (hypopneas) are more likely to have resolution of OSA after T&A than are those with complete airway obstruction (apneas), this general tenet is not supported by evidence-based literature. The primary aim of the current study was therefore to evaluate whether children with hypopnea-predominant OSA were more likely to have complete resolution of OSA after T&A when compared with children with apnea-predominant disease. Our secondary aim was to identify risk factors that might modify the relationship between OSA resolution and PSG event type (ie, hypopnea vs apnea).
Methods
Patient Selection
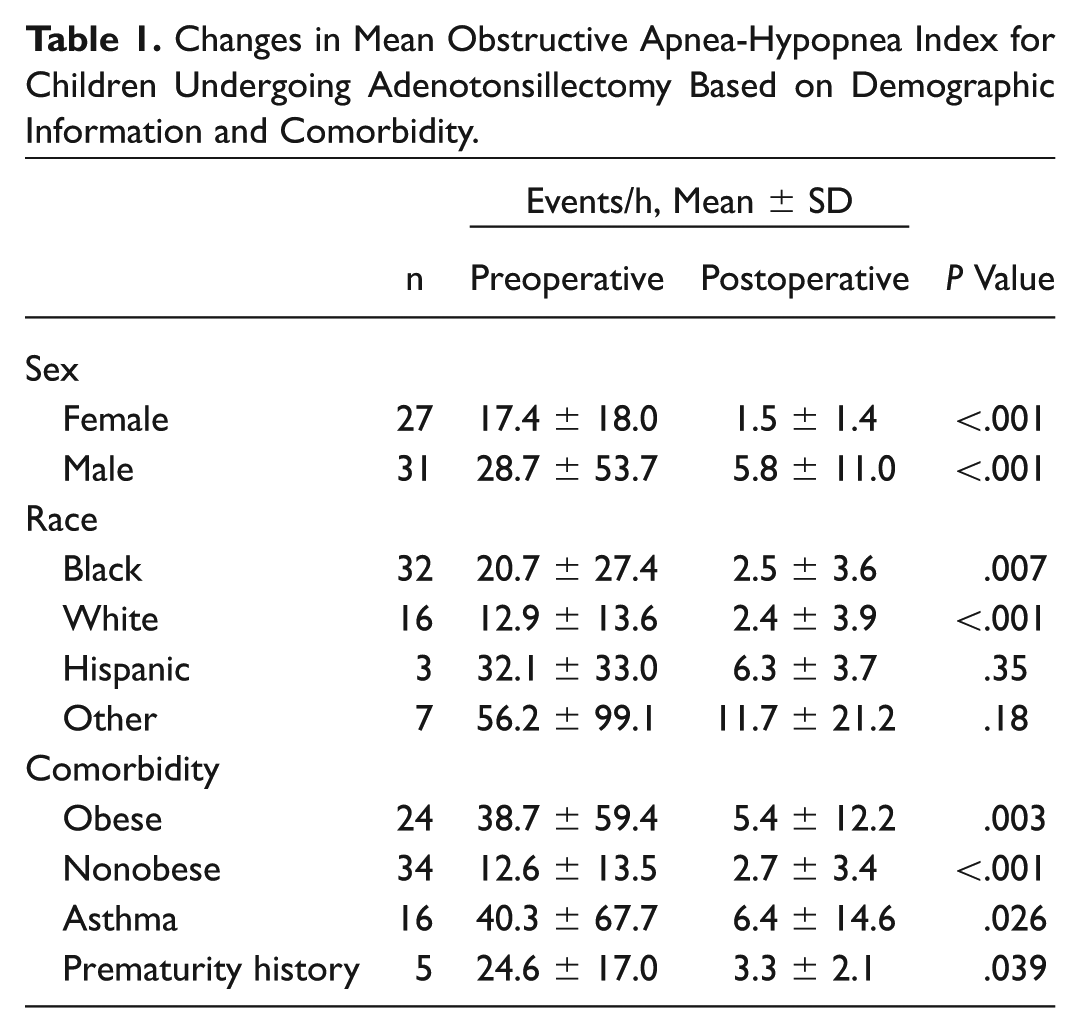
A retrospective case series with chart review was performed for consecutive children aged 1 to 18 years who were diagnosed with OSA from March 2011 to December 2012. Children who subsequently underwent T&A and completed pre- and postoperative overnight PSG within 1 year of the time of surgery were included in the study. PSG results and demographic data were documented for these patients ( Table 1 ). The body mass index (BMI) of all study participants was calculated and reported through BMI z scores as derived from the 2000 growth standards of the Centers for Disease Control and Prevention. 22 Health-related exclusion criteria included a known syndromic disorder or chromosomal abnormality, craniofacial deformity, and neurologic impairment. Patients with incomplete data and those who did not the meet the PSG inclusion criteria were also excluded. Approval for this study was obtained from the Institutional Review Board at Johns Hopkins School of Medicine.
Changes in Mean Obstructive Apnea-Hypopnea Index for Children Undergoing Adenotonsillectomy Based on Demographic Information and Comorbidity.
PSG Data
Overnight PSG was performed in the Johns Hopkins Pediatric Sleep Laboratory, with Somnologica or REMLogic (Embla, Broomfield, Colorado). Signals included electroencephalograms (leads C3-A2, C4-A1, and O1-A2), left and right electrooculograms, submental electromyogram, tibial electromyogram, electrocardiogram, and oxyhemoglobin saturation (Masimo, Irvine, California). End-tidal CO2 (Novametrix, Murrysville, Pennsylvania) was obtained in all participants. Airflow was acquired with a nasal cannula (Salter Labs, Arvin, California) connected to a differential pressure transducer (Pro-Tech, Mukilteo, Washington). Respiratory effort was assessed with thoracic and abdominal inductive plethysmography (Embla), and body position was monitored via infrared video camera. Several sleep studies from the same laboratory were carried out with the same equipment but different software, Alice 4.0 (Healthdyne, Marietta, Georgia), and a strain gauge with piezoelectric crystals instead of plethysmography to evaluate respiratory effort. Pediatric sleep medicine physicians at the Johns Hopkins Hospital interpreted all results.
PSG Analysis
PSG was scored according to the American Academy of Sleep Medicine (AASM) guidelines. 23 Apnea was defined as complete absence of airflow for at least 2 breath cycles. Apneas were identified as obstructive when associated with continued or increased inspiratory effort; they were identified as central when associated with no inspiratory effort. A mixed apnea was identified when absence of airflow was associated with periods with and without inspiratory effort. Hypopnea was defined as a decrease in airflow ≥50% for at least 2 breath cycles, followed by a ≥3% decrease in saturation or an electrocortical arousal from sleep. Respiratory event-related arousals (RERAs) were not scored by either sleep laboratory. The obstructive apnea hypopnea index (oAHI) was calculated as the number of obstructive and mixed apneas and hypopneas divided by the total sleep time; central apneas were excluded from this calculated value. The obstructive apnea index (oAI) was calculated as the number of obstructive and mixed apneas divided by the total sleep time; central apneas were also excluded from this calculated value. The obstructive hypopnea index (oHI) was calculated as the number of obstructive hypopneas divided by the total sleep time. OSA severity was stratified by the oAHI: mild OSA was defined as 1 to <5 events per hour; moderate OSA, 5 to <10 events per hour; and severe OSA, ≥10 events per hour.
Children were further categorized by preoperative event-type predominance. The postoperative oAHI was used to differentiate patients with complete resolution of OSA (oAHI <1.0) from those with partial resolution (oAHI >1.0) for each group.
Statistical Analysis
We used descriptive statistics to examine the distribution of demographic and clinical characteristics. PSG variables—including mean oAHI, oxygen saturation nadir, oAI, and oHI values—did not follow a normal (Gaussian) distribution. Therefore, the Wilcoxon signed-rank test (nonparametric) was used to compare these values in children with and without hypopnea-predominant disease. Univariable and multivariable linear regression modeling with backward and forward model selection was performed to show the relationship between change in PSG parameters and event type. The prediction model for change in oAHI included event type, baseline oAHI, baseline oxygen saturation nadir, syndromic status, neurologic impairment, prematurity, asthma, and attention-deficit/hyperactivity disorder, while controlling for age, race, sex, and BMI z score. Significance was considered as a P value <.05. Data were analyzed with Stata 12 (Stata Corporation, College Station, Texas).
Results
Baseline demographic variables are presented in Table 2 . Fifty-eight children (27 females, 47%) with a mean ± SD age of 5.6 ± 3.1 years were included in the study. Black children composed 55% of the patient population; smaller percentages of children were white (28%), Hispanic (5%), and other (12%). Sixteen (28%) children had asthma, and 5 (9%) had a history of prematurity. For 7 children, data were insufficient to calculate BMI. The mean BMI z score for the remaining 51 children was 1.1 ± 1.7 kg/m2 (range, 2.6-5.9 kg/m2), which correlates with a mean BMI percentile of 71.9% ± 33.8% (range, 0.5%-100%).
Demographics and Response to Adenotonsillectomy in Children with Apnea- and Hypopnea-Predominant Obstructive Sleep Apnea. a
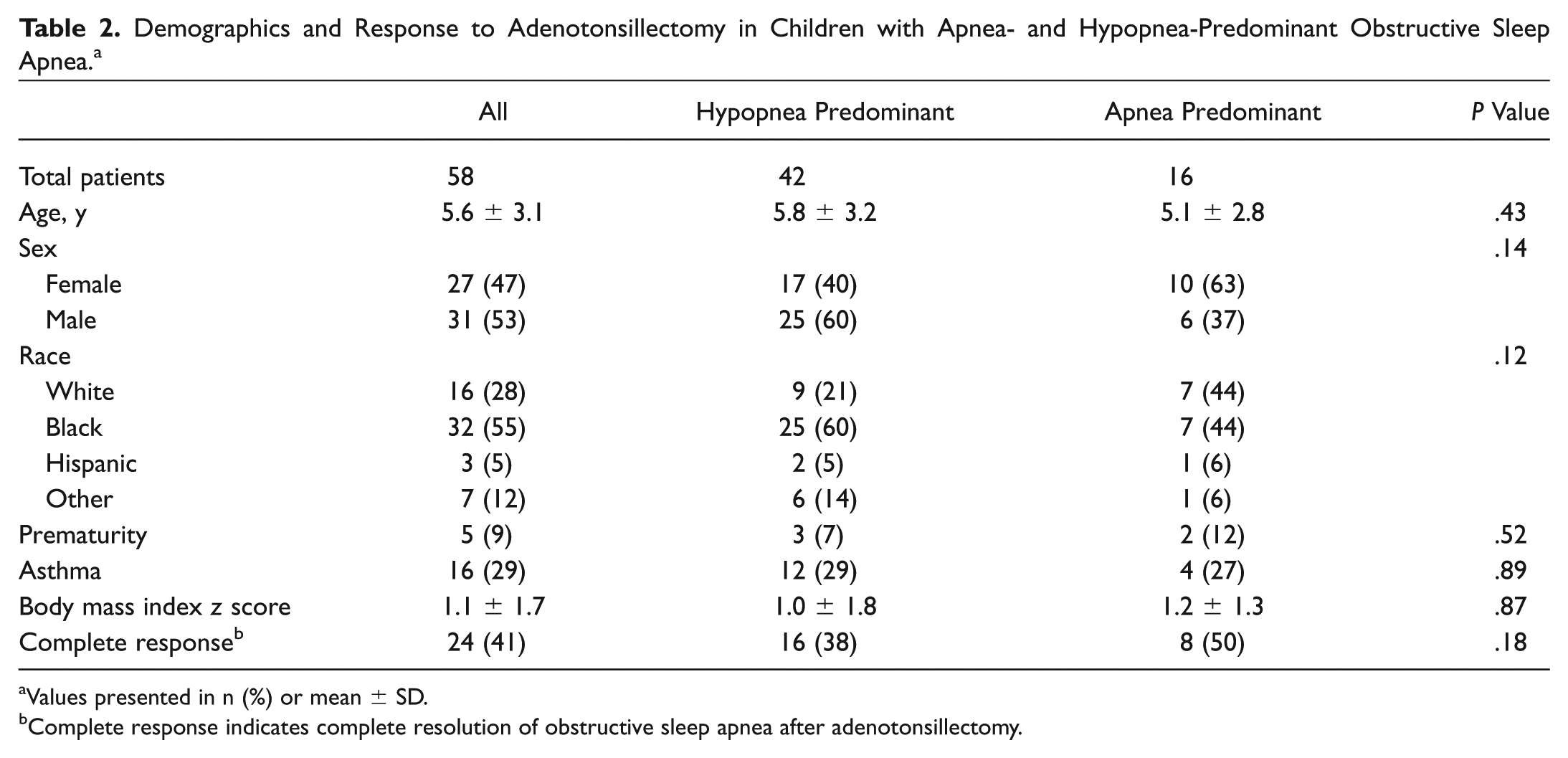
Values presented in n (%) or mean ± SD.
Complete response indicates complete resolution of obstructive sleep apnea after adenotonsillectomy.
The average intervals between preoperative PSG and surgery and postoperative PSG and surgery were 98 ± 68 days and 145 ± 62.3 days, respectively. Overall, T&A resulted in significant improvement in the oAHI (23.3 ± 40.0 to 4.3 ± 8.2 events/h, P < .001), oAI (5.1 ± 7.4 to 0.4 ± 0.8 events/h, P < .001), oHI (18.1 ± 37.5 to 3.7 ± 8.1 events/h, P < .001), and oxygen saturation nadir (83.8% ± 8.5% to 90.0% ± 4.4%, P < .001; Table 3 ). When children were stratified into a hypopnea-predominant group (n = 42) and an apnea-predominant group (n = 16), there continued to be significant improvement in all 4 reported PSG parameters (oAHI, oHI, oAI, and oxygen saturation nadir) for both groups (P = .001-.032; Table 4 ). Twenty-four (41%) children had complete resolution of OSA after surgery (oAHI < 1.0). Of these children, 16 (38%) were classified as hypopnea predominant, whereas 8 (50%) were apnea predominant ( Table 2 ).
Changes in Respiratory Sleep Study Parameters for Children Undergoing Adenotonsillectomy (n = 58). a
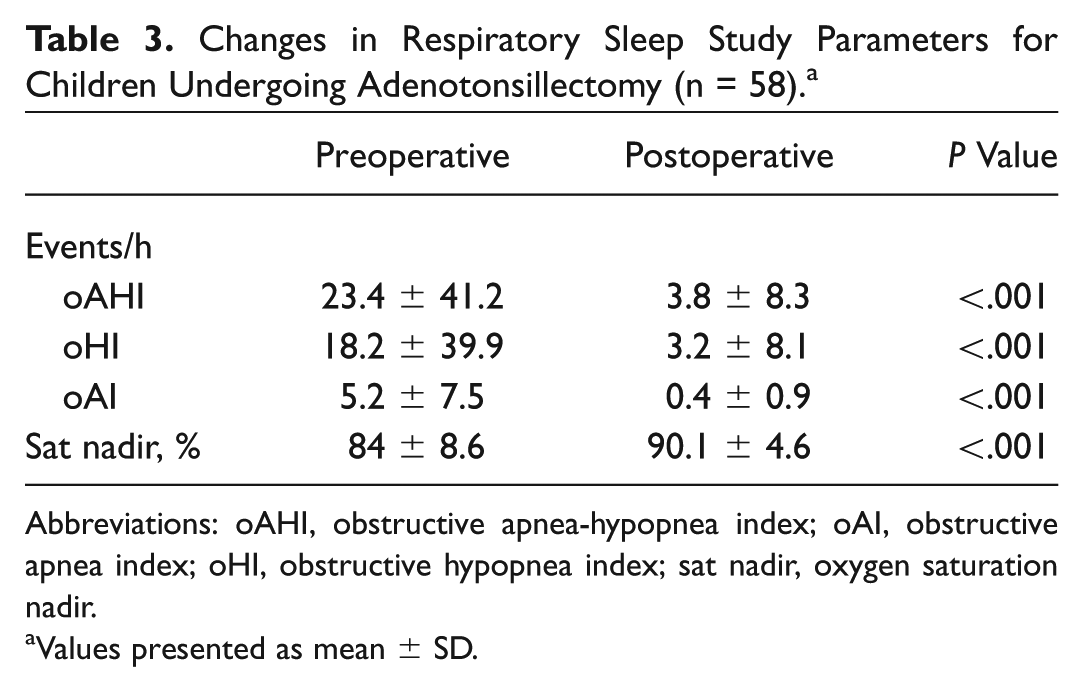
Abbreviations: oAHI, obstructive apnea-hypopnea index; oAI, obstructive apnea index; oHI, obstructive hypopnea index; sat nadir, oxygen saturation nadir.
Values presented as mean ± SD.
Changes in Respiratory Sleep Study Parameters for Children with Apnea- and Hypopnea-Predominant Obstructive Sleep Apnea. a
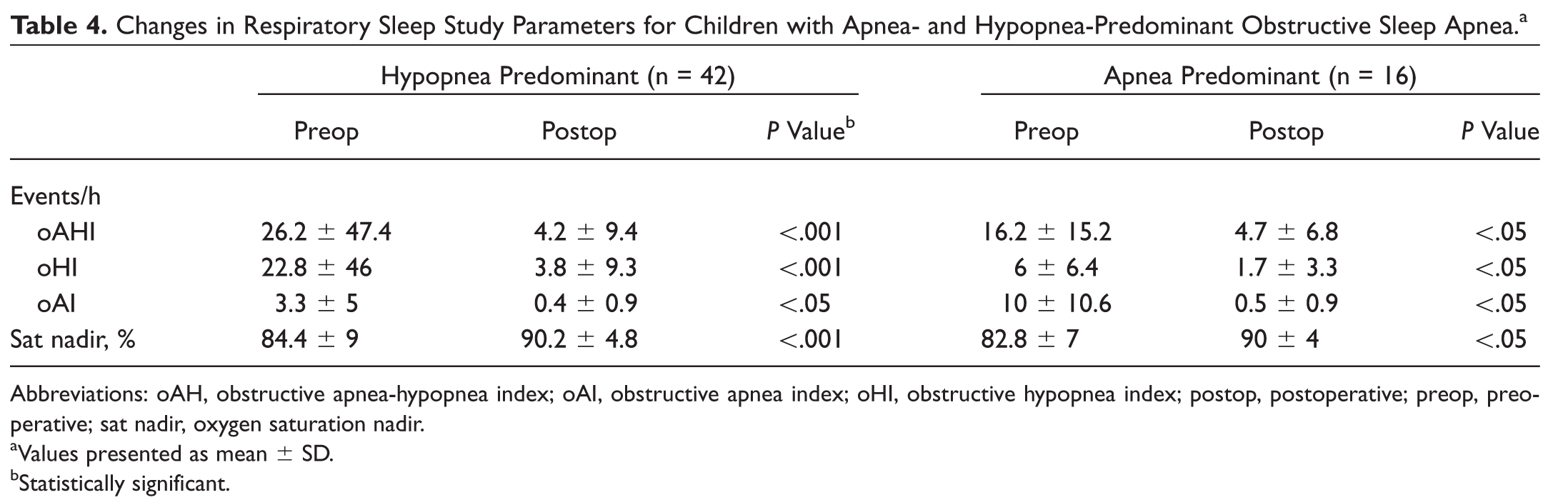
Abbreviations: oAH, obstructive apnea-hypopnea index; oAI, obstructive apnea index; oHI, obstructive hypopnea index; postop, postoperative; preop, preoperative; sat nadir, oxygen saturation nadir.
Values presented as mean ± SD.
Statistically significant.
As shown in Table 5 , when postoperative changes in sleep parameters were compared between the hypopnea- and apnea-predominant groups, there was significantly more improvement in oAI in apnea-predominant children (7.6 events/h) than in those who were hypopnea predominant (2.8 events/h, P = .008). In contrast, there were no significant differences between the these 2 groups in terms of oAI, oHI, and oxygen saturation nadir (P = .35, P = .10, and P = .83, respectively).
Differences in Respiratory Sleep Study Parameters before and after Adenotonsillectomy for Children with Apnea- vs Hypopnea-Predominant Obstructive Sleep Apnea. a
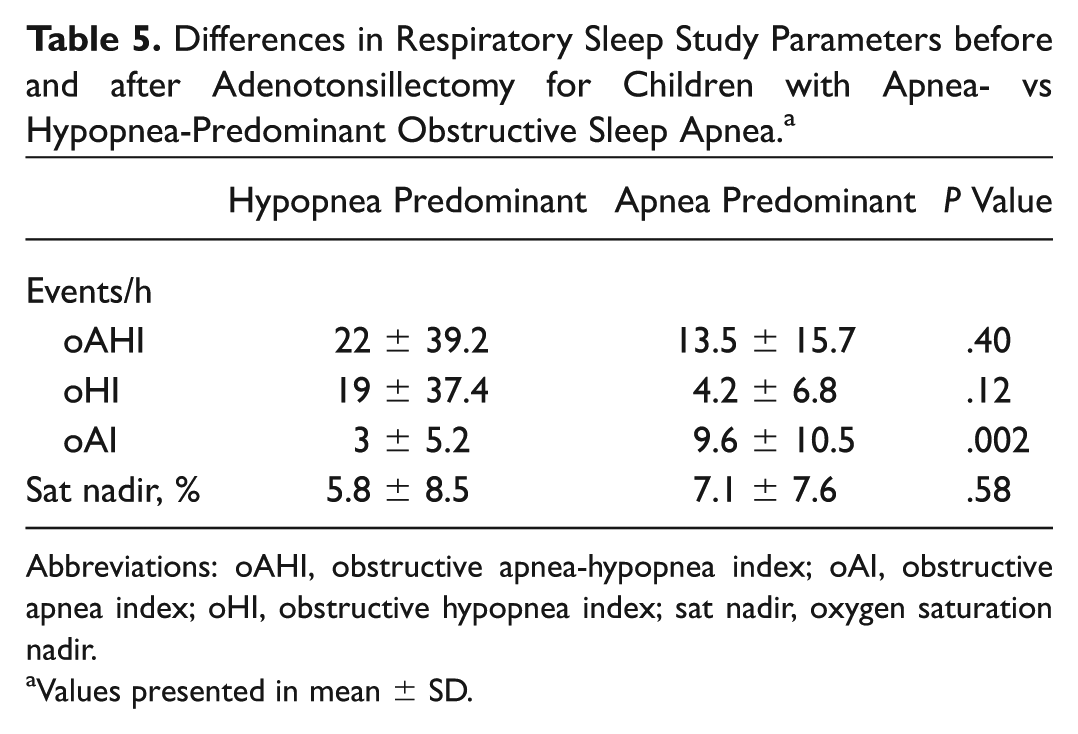
Abbreviations: oAHI, obstructive apnea-hypopnea index; oAI, obstructive apnea index; oHI, obstructive hypopnea index; sat nadir, oxygen saturation nadir.
Values presented in mean ± SD.
Regression results are presented in Table 6 . Backward model selection included age, prematurity, attention-deficit/hyperactivity disorder, oAHI, oAI, oHI, and saturation nadir but not race, sex, or BMI z score. That model had an r2 of 0.42. We added back race, sex, and BMI given their known association with persistent OSA, and the final model r2 was 0.47. The presence of hypopnea-predominant disease was not predictive of complete OSA resolution (P = .19), change in oAHI (P = .41), or change in oHI (P = .12) on univariable analysis. Complete response to T&A was associated with lower baseline oAHI (P < .001), older age (P = .015), higher oxygen saturation nadir (P = .006), lower oHI (P = .042), and lower oAI (P = .046) on multivariable analysis (r2 = 0.97). Change in the oAHI after T&A was also associated with a lower baseline oAHI (P < .001) on multivariable analysis (r2 = 0.97).
Regression Results Predictive of the Postoperative Obstructive Apnea-Hypopnea Index for Children Undergoing Adenotonsillectomy. a
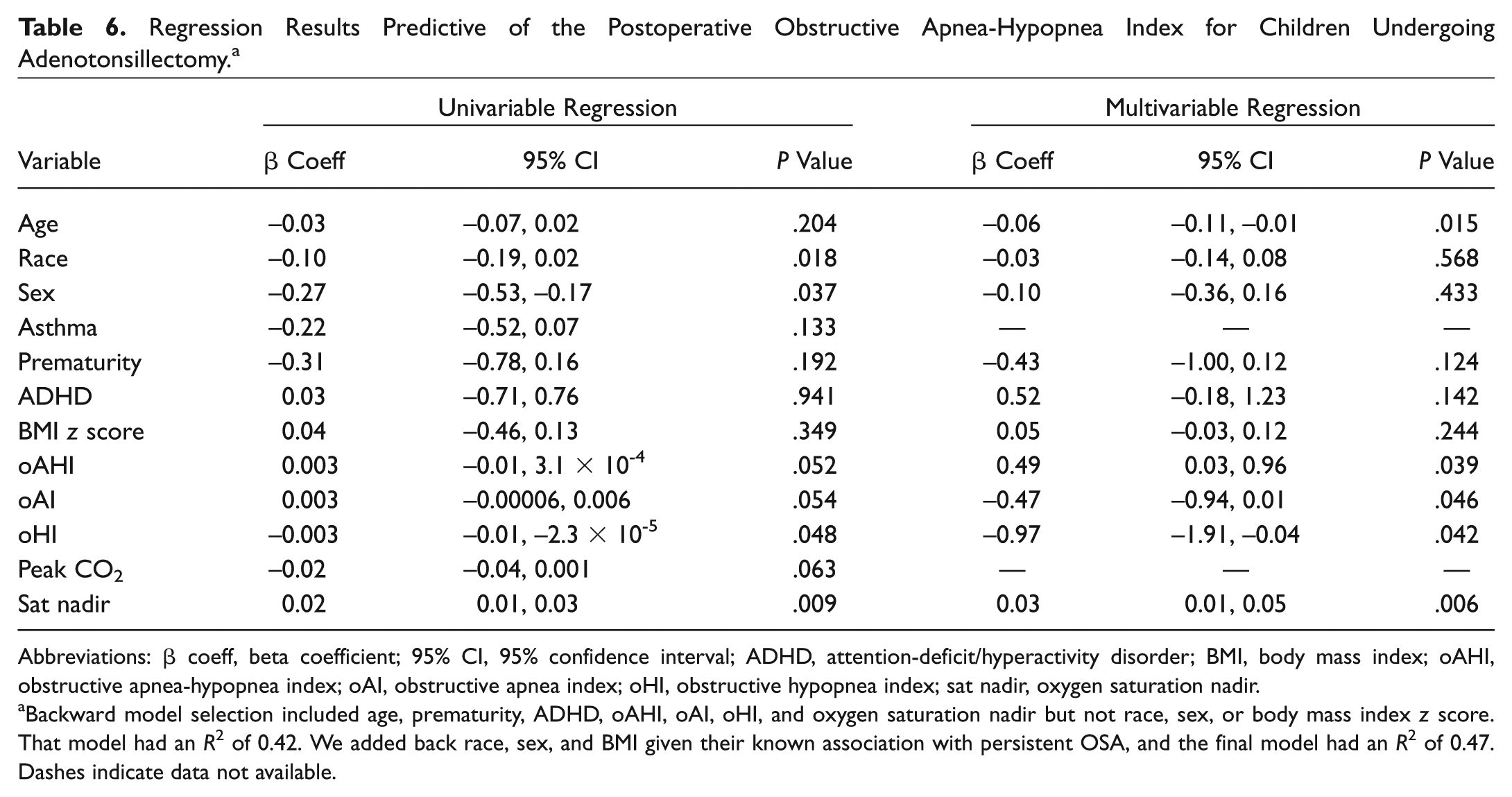
Abbreviations: β coeff, beta coefficient; 95% CI, 95% confidence interval; ADHD, attention-deficit/hyperactivity disorder; BMI, body mass index; oAHI, obstructive apnea-hypopnea index; oAI, obstructive apnea index; oHI, obstructive hypopnea index; sat nadir, oxygen saturation nadir.
Backward model selection included age, prematurity, ADHD, oAHI, oAI, oHI, and oxygen saturation nadir but not race, sex, or body mass index z score. That model had an R2 of 0.42. We added back race, sex, and BMI given their known association with persistent OSA, and the final model had an R2 of 0.47. Dashes indicate data not available.
Discussion
Overall, our findings corroborate those of previous studies showing that T&A improves the oAHI, oAI, oHI, and oxygen saturation nadir regardless of comorbidities or race/ethnicity.12,14,20,24-26 Although we anticipated that children with hypopnea-predominant disease would be more likely than those with apnea-predominant disease to have complete resolution of OSA after T&A, there was no significant difference in OSA resolution between these 2 groups. Our multivariable evaluation of the risk factors that could affect this relationship revealed that low baseline oAHI was the only significant predictor of improvement in the oAHI and that this model explained 97% of the variability of the change in the oAHI. Univariate analysis of the factors modeled for the change in oAHI revealed that race explained 7%, BMI z score 8%, saturation nadir 30%, and baseline oAHI 98% of the variability in our prediction model. We were surprised at the high r2 value given the complexity of this disease and the multiple factors that have previously been associated with persistent pediatric OSA.
Forty-one percent of children in our study had complete resolution of OSA after T&A. This rate is significantly lower than that reported in a meta-analysis carried out by Freidman et al, who found that 59.8% of children had an oAHI <1 event/h after surgery; a pooled subanalysis of children with morbid obesity and/or severe OSA demonstrated a 38.7% resolution rate after T&A. 25 Our low resolution rate may be explained by the inclusion of children with risk factors known to be associated with persistent OSA, including obesity, older age, and asthma.11,14,15,27,28 Another pertinent factor may be that black children have been shown to be at higher risk for persistent OSA independent of obesity29,30 and they were 55% of our study population.
Findings from our study also support the positive relationship between neurologic impairment and persistent OSA. Reports regarding the prevalence of OSA in children with neurodevelopmental delays suggest that OSA occurs in >50% of children with Down syndrome 31 or Prader-Willi syndrome 32 ; however, authors also imply that reported prevalences are likely underestimated due to failure to recognize OSA, as well as inconsistent evaluation by parents and physicians. Additionally, persistent OSA is commonly seen in children with cerebral palsy and comorbid obesity. 33
Clinicians face challenges in identifying children who may require closer follow-up and postoperative PSG, especially given that subjective improvement is often reported for patients with partial disease resolution. 26 Determining which PSG data can be helpful in alerting clinicians to children at risk for persistent OSA can facilitate accurate and early identification of susceptible children. A further workup (ie, cine magnetic resonance imaging, drug-induced sleep endoscopy) would be warranted for these children. 34
Given that our study is retrospective, its main limitation is that it is prone to selection bias; however, it was the practice of the senior author (S.L.I.) to order a sleep study on all children evaluated for sleep-disordered breathing. In addition, although our overall sample size was reasonable, the apnea-predominant group was small. We were thus underpowered to show a small difference in rates of OSA resolution between groups. Last, the racial composition of our population (55% black) may limit the generalizability of our findings to other cohorts.
Conclusion
In this retrospective case series, we found no significant difference in disease resolution between children with hypopnea- and apnea-predominant OSA who underwent T&A; however, the number of children with apnea-predominant disease was limited. Our data support previous findings that T&A significantly improved OSA in most children and that baseline PSG parameters, such as high preoperative oAHI, are associated with persistent OSA after T&A. Future trials including a larger population of apnea-predominant children would be helpful in determining if OSA event type would help clinicians predict whether complete disease resolution will occur.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.