
Abstract
Objective
To assess health literacy in an adult tertiary care otolaryngology clinic population and to explore potential determinants of inadequate health literacy.
Study Design
Cross-sectional study.
Setting
Tertiary care otolaryngology clinic.
Subjects and Methods
The study population included all adult patients treated at 3 of Stanford University’s adult otolaryngology clinic sites between March 1 and 11, 2016. Data were collected via an anonymous questionnaire. Health literacy was assessed with the Brief Health Literacy Screen.
Results
Ten percent of patients had inadequate health literacy. White race (odds ratio [OR], 0.23) and having English as the primary language (OR, 0.12) were associated with adequate health literacy, while high school or lower level of education (OR, 3.2) was associated with inadequate health literacy. Age, sex, and Hispanic ethnicity were not associated with health literacy.
Conclusion
Our study highlights the need for health literacy screening in the otolaryngology clinic setting and identifies sociodemographic risk factors for inadequate health literacy. Further studies are needed to assess the impact of health literacy on patient outcomes and to test specific interventions to address health literacy and health outcomes.
Health literacy is the degree to which individuals have the capacity to obtain, process, and understand basic information and services needed to make appropriate decisions regarding their health. 1 Health literacy goes beyond the ability to read and write (fundamental literacy); it also includes skills (eg, speaking and listening), an adequate background medical knowledge, and the ability for self-advocacy. An estimated 90 million adults in the United States have inadequate health literacy. 2 Health literacy has been shown to affect outcomes in a number of medical conditions. Inadequate health literacy is associated with increased mortality in patients hospitalized for heart failure. 3 In asthma patients, inadequate health literacy has been shown to be associated with poor medication adherence, poor asthma control, decreased asthma-related quality of life, and increased asthma-related hospitalizations and emergency department visits.4-7 Inadequate health literacy is also associated with poor glycemic control and the development of retinopathy in diabetic patients. 8 Several studies suggest that the association between inadequate health literacy and poor outcomes may be partly mediated by poor understanding of medical information and erroneous illness and medication beliefs. Kale et al found that chronic obstructive pulmonary disease patients with inadequate health literacy were more likely to have beliefs about their illness and medication that were associated with poor adherence. 9 Similarly, a study on hypertensive and diabetic patients showed that patients with inadequate health literacy had poor knowledge of important information about their chronic disease. 10
Despite the complexity of care that is often required in otolaryngology patients, the literature on health literacy in this field is sparse. The few studies available have mostly focused on assessing the readability of patient education materials.11,12 The goal of our study was to assess health literacy in an adult tertiary care otolaryngology clinic population and to explore potential determinants of inadequate health literacy.
Methods
This was a cross-sectional study. The study population included all adult patients treated at 3 of Stanford Health Care’s adult otolaryngology clinic sites between March 1 and 11, 2016. Patients were excluded if they were <18 years old. Data was collected through an anonymous questionnaire, which was 1 page to limit the burden associated with completion. The questionnaire was included with the registration forms for every patient seen at the clinic sites during the study period. The questionnaire was administered in English. Patients with low English proficiency completed the questionnaire with the help of a medical interpreter. Data were collected on demographic and clinical factors, such as age, sex, race, Hispanic/Latino ethnicity, primary language, and highest level of education achieved. Race was recorded as white, black/African American, Asian, American Indian/Alaska Native, Native Hawaiian/Pacific Islander, or other. Highest level of education achieved was recorded as follows: less than high school diploma, high school diploma or GED, bachelor’s degree, or graduate or professional degree.
Health literacy was assessed via the Brief Health Literacy Screen (BHLS), a 3-item self-reported measure of health literacy. 13 The BHLS was developed to rapidly detect patients with inadequate health literacy. It has been formally validated against the Short Test of Functional Health Literacy in Adults 14 and Rapid Estimate of Adult Literacy in Medicine, 15 2 previously validated and widely used measures of health literacy. It has also been found to be reliable in detecting patients with inadequate health literacy, with an area under the receiver operating characteristic curve ranging from 0.73 to 0.86.13,16,17 The BHLS was chosen as a screening measure of health literacy because it is short and easy to administer, making it feasible to apply in clinical practice. The BHLS questions are as follows:
“How confident are you filling out medical forms by yourself?”
“How often do you have someone help you read hospital materials?”
“How often do you have problems learning about your medical condition because of difficulty understanding written information?”
For the first question, the response options were extremely, quite a bit, somewhat, a little bit, or not at all. For the other 2 questions, the response options were all of the time, most of the time, some of the time, a little of the time, or none of the time. Patient BHLS responses were recorded on a 5-point Likert scale. The first question was reverse coded. The score for the 3 questions was summed to equal 3 to 15 points, with higher scores indicating higher health literacy. 18 A response ≤3 (ie, somewhat or some of the time) on the Likert scale was considered indicative of inadequate health literacy for each question.16,17 A response >3 was considered indicative of adequate health literacy for each question. A summative BHLS score ≤9 was considered to indicate overall inadequate health literacy, while a summative score >9 was considered to indicate adequate health literacy.
SPSS 23 was used for statistical analysis (IBM Corp, Armonk, New York). Sociodemographic factors were compared between patients with adequate and inadequate health literacy. For univariable analysis, age was compared through Student’s t test. The impact of sex, race, Hispanic ethnicity, and level of education on health literacy was evaluated via Pearson’s chi square test (or Fisher’s exact test, as appropriate). Multivariable analysis was performed with binary logistic regression. Age, sex, race, Hispanic ethnicity, English as a primary language, and level of education (high school or less) on health literacy were entered a priori into the model. P value <.05 was considered statistically significant. This study was exempt from review by the Stanford University Institutional Review Board due to its status as a quality improvement project.
Results
Univariable Analysis
Of 618 patients who were seen in the clinics during the study period, 316 completed the questionnaire. The survey response rate was 51.1%. The patient characteristics are displayed in Table 1 . The median BHLS score was 14 (range, 3-15). Eighty-three patients (26%; 95% confidence interval [95% CI], 21%-31%) had difficulty with at least 1 of the 3 measured domains. Forty-four patients (13.9%; 95% CI, 10%-18%) had difficulty filling out medical forms; 59 (18.7%; 95% CI, 14%-23%) had difficulty reading medical material; and 50 (15.8%; 95% CI, 12%-20%) had difficulty understanding written information about their medical condition. Overall, 32 patients (10.1%; 95% CI, 7%-14%) had inadequate health literacy. Patients with inadequate health literacy were older than patients with adequate health literacy (mean difference, 10 years; 95% CI, 0.6-19.3 years; P = .002). The results of the univariable analysis are shown in Table 2 . White race (odds ratio [OR], 0.14) and having English as the primary language (OR, 0.08) were associated with adequate health literacy. High school or lower level of education (OR, 4.27) and Hispanic ethnicity (OR, 3.51) were associated with inadequate health literacy.
Patient Characteristics (N = 316). a
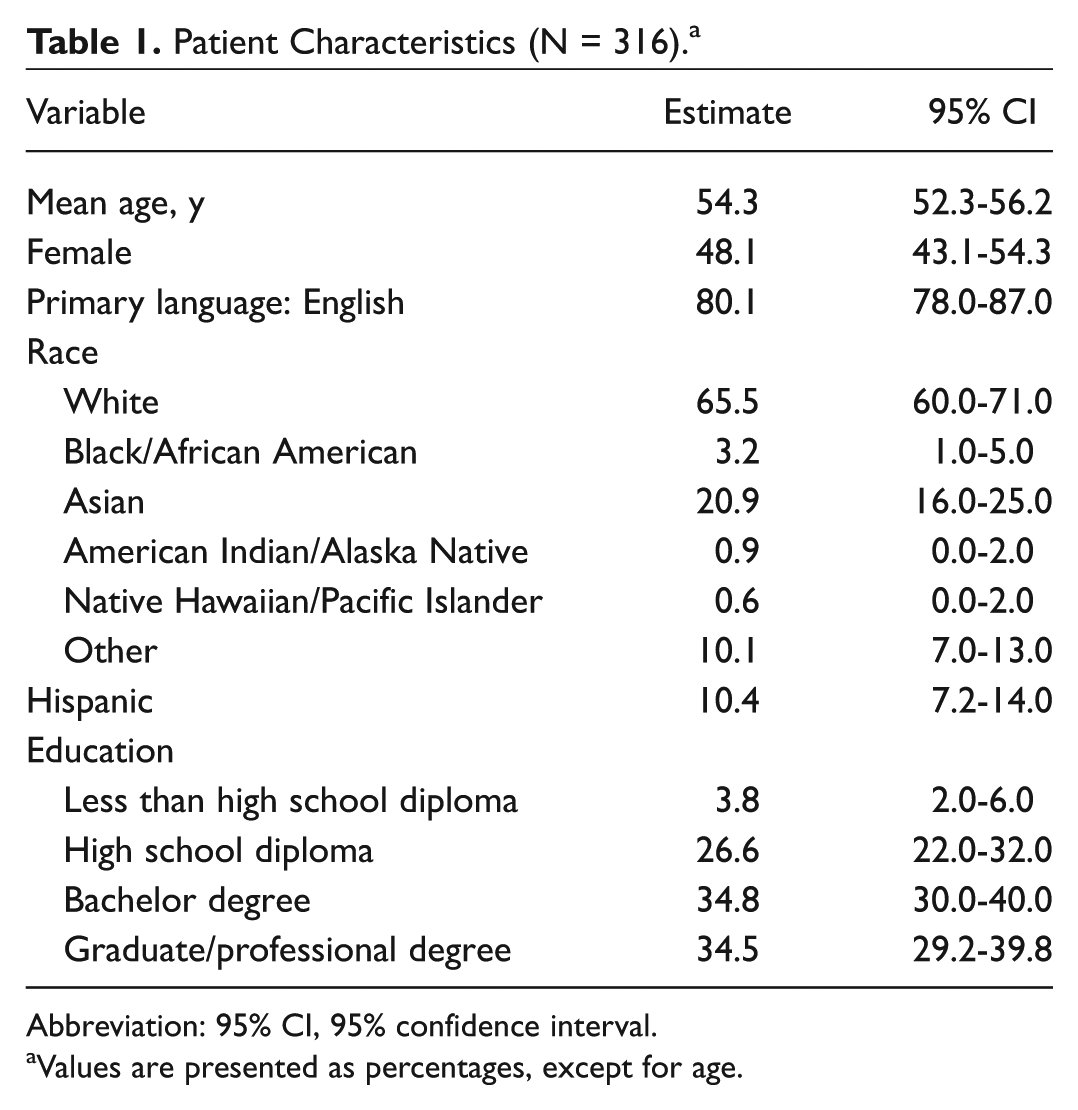
Abbreviation: 95% CI, 95% confidence interval.
Values are presented as percentages, except for age.
Factors Associated with Inadequate Health Literacy: Univariable Analysis.
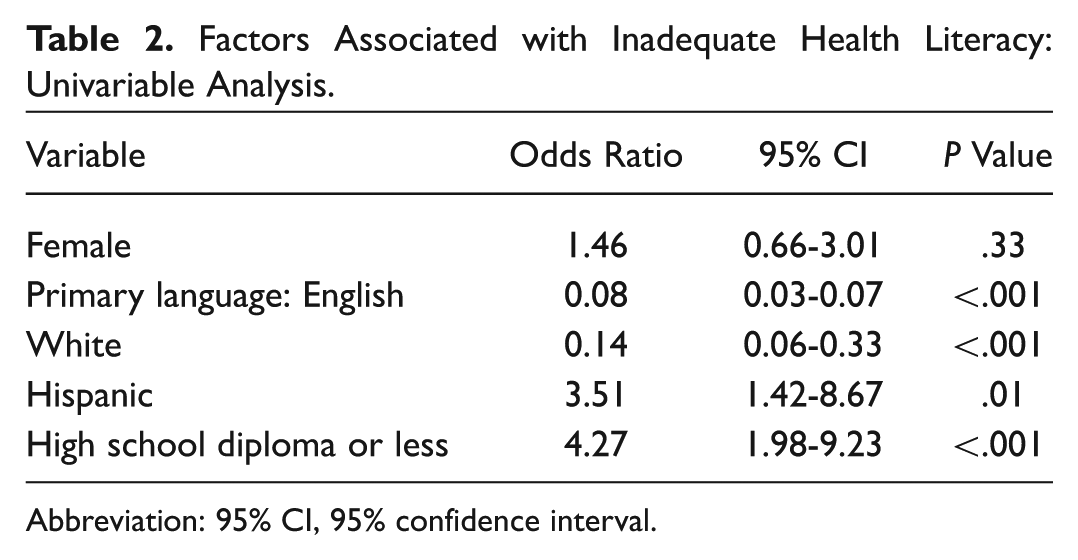
Abbreviation: 95% CI, 95% confidence interval.
Multivariable Analysis
The results of the multivariable analysis are shown in Table 3 . White race (OR, 0.23) and having English as the primary language (OR, 0.12) were associated with adequate health literacy, while high school or lower level of education (OR, 3.2) was associated with inadequate health literacy. Age, sex, and Hispanic ethnicity were not associated with health literacy.
Factors Associated with Inadequate Health Literacy: Multivariable Analysis.
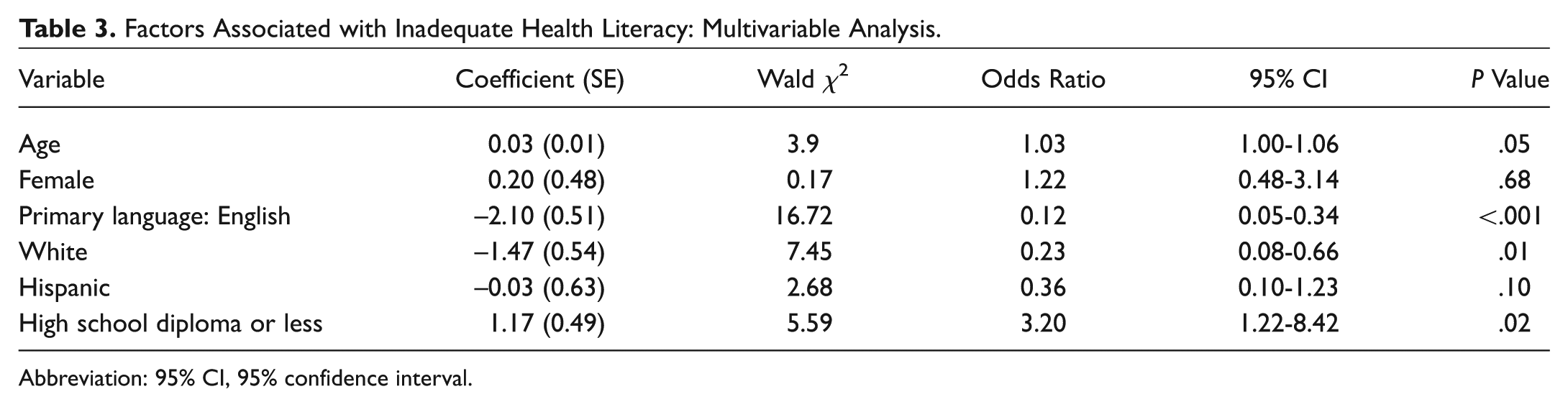
Abbreviation: 95% CI, 95% confidence interval.
Discussion
Our study showed that 10% of our patients had inadequate health literacy. Moreover, over a quarter of our patients had difficulty with at least 1 of the 3 health literacy domains measured. This is remarkable given that our institution is located in the Silicon Valley region, which has a reputation for having a high concentration of highly educated individuals. We found that patients with a high school education or less, racial minority patients, and patients who did not have English as their primary language were more likely to have inadequate health literacy. Although univariable analysis suggested that age and Hispanic ethnicity were associated with health literacy, these factors were not found to be associated with health literacy on multivariable analysis. Sex was also not associated with health literacy.
Identifying patients with inadequate health literacy is critical in today’s health care environment. Health care is shifting toward a shared decision-making model, giving patients more autonomy in directing their care. With the proliferation of medical knowledge, advances in medical science and technology, and increasing diagnostic and medical options, health care is becoming more complex. This increases the health literacy requirements for patients, who have to assimilate new information and make complex decisions, often at times of physical and emotional stress. Furthermore, recent policy changes have imposed increased administrative burden on patients. Patients now have to be able to compare insurance plans, verify which health care providers participate in their plans, and determine which services are covered.19,20 The introduction of electronic medical record systems with patient portals—in response to the 2014 requirements of the Centers for Medicare and Medicaid Services’ Electronic Health Record Incentive Programs—has increased the amount and complexity of medical information that patients have to process.21,22 Health literacy screening may help identify patients who require additional help in navigating the health care system.
The US Department of Health and Human Services has made improving health literacy a national priority. 23 The 2003 National Assessment of Adult Literacy (NAAL) included approximately 19,000 adults. 2 The assessments were performed in English and Spanish. Unlike previous versions, the 2003 NAAL included a health literacy component. Similar to our findings, the study found that higher level of education was associated with higher level of health literacy. Adults who spoke only English before starting school had higher average health literacy than did adults who spoke other languages alone or other languages and English. This is similar to our study, which showed that patients who did not have English as their primary language were more likely to have inadequate health literacy. In the 2003 NAAL, white and Asian/Pacific Islander adults had higher average health literacy than did black and American Indian/Alaska Native adults. This is also similar to our study, which showed that racial minorities were more likely to have inadequate health literacy. Contrary to our study, the 2003 NAAL found that Hispanic ethnicity was associated with low health literacy. The study also found that women had average higher health literacy than men and that younger age was associated with higher levels of health literacy. It is unclear from the report of the 2003 NAAL whether multivariable analysis was performed. The lack of multivariable analysis may account for the differences in findings observed.
To our knowledge, our study is the first to assess health literacy in a large diverse otolaryngology clinic population. Two studies have examined health literacy in head and neck cancer patients. Beitler et al examined health literacy in 8 patients who had undergone total laryngectomy for laryngeal cancer. 24 Three of the patients were found to have limited health literacy. The study did not analyze potential determinants of health literacy. Koay et al examined health literacy in 60 patients with head and neck cancer and 33 with lung cancer. 25 They found that 12% had limited health literacy. As in our study, lower education level was associated with low health literacy. Contrary to our findings, however, older age was also associated with low health literacy. The authors did not perform multivariable analysis, which may explain the difference in findings. In our study, age was found to be associated with health literacy on univariable analysis but not on multivariable analysis.
Several studies have established the feasibility of routine health literacy assessment in clinical practice. Cawthon et al reported their experience with routine health literacy screening at their institution. 26 Routine health screening with the BHLS was implemented across all adult hospital units, the emergency department, and 3 primary care practices. They found a 91.8% completion rate for the hospital and a 66.6% completion rate for the outpatient clinics. In the surgical literature, Komenaka et al examined the feasibility of routinely assessing health literacy in a breast surgery clinic. 27 A total of 2026 patients were included in the study, 96.6% of all patients seen in their clinic during the 2-year study period. Health literacy was examined with the Newest Vital Sign, a measure that involves the interpretation of the contents of a nutrition label. 28 In that patient population, 80% had inadequate health literacy. The authors found that patient satisfaction was higher during the health literacy assessment period as compared with the year prior. Their institution served a mainly indigent population, which may explain their unusually high rate of inadequate health literacy.
The main strength of our study lies in our relatively large sample size and the systematic collection and analysis of data. However, our study does have limitations. The cross-sectional nature of the study makes it susceptible to nonresponse bias. Since there is no universally accepted threshold for what constitutes an adequate survey response rate, it is unclear what impact our response rate of 51.1% has on the risk of response bias. In fact, several studies have shown that low response rates are not necessarily associated with nonresponse bias.29,30 Unfortunately, since the survey was administered anonymously, the characteristics of patients who did not respond to the survey could not be analyzed. It is possible that a higher proportion of low health literacy patients did not respond to the survey, leading to an underestimation of the proportion of patients with inadequate health literacy. Several factors associated with inadequate health literacy in our study, such as racial minority status and lower level of education, are also associated with increased risk of survey nonresponse. 31 Utilizing a nonanonymous survey format will enable comparative analysis of responders and nonresponders. However, this may lead to increased reporting bias due to potential stigma associated with inadequate literacy. The use of a self-reported measure of health literacy may have led to reporting bias. However, the BHLS has been shown to be a valid and reliable measure of health literacy.13,16,17,32 In addition, the questionnaire was administered anonymously, which reduces the risk of reporting bias. Since we utilized interpreters for patients with low English proficiency, incorrect interpretation of the contents of the questionnaire may have introduced some bias in our results. We utilized the BHLS because it is short and easy to administer, making it feasible to apply in clinical practice. Although the BHLS has been shown to reliably identify patients with inadequate health literacy, its main limitation is its inability to discriminate between adequate and marginal health literacy status. 13 Consequently, it is probable that some subjects in our “adequate” health literacy group may have had marginal health literacy. This is supported by the finding that a significantly higher proportion of subjects had difficulty with at least 1 of the measured domains when compared with the proportion deemed to have overall inadequate health literacy. Last, our institution is a tertiary academic medical center located in an area with a highly educated population. Thus, our results may not be generalizable to other otolaryngology practices.
In conclusion, our study showed that a significant number of our patients had inadequate health literacy. Patients who completed high school or less, racial minority patients, and patients who did not have English as their primary language were more likely to have inadequate health literacy. Age, Hispanic ethnicity, and sex were not associated with health literacy. Our study highlights the need for health literacy screening in the otolaryngology clinic setting, and it identifies sociodemographic risk factors for inadequate health literacy. Health literacy screening may identify patients who require additional help navigating the health care system; it might also facilitate allocation of the appropriate time and resources to assist these patients. We plan to conduct literacy load analyses of written patient education materials in our clinics, in an effort to improve readability and ease of understanding. In addition, we are exploring ways to incorporate documentation of health literacy assessment into our electronic health record system. Further studies are needed to assess the impact of health literacy on patient outcomes. This will enable us to design and test specific interventions to address health literacy and health outcomes in our patient population.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.