
Abstract
Objective
We aimed to develop and validate an ex vivo dissection station for endolaryngeal surgery suitable for different kinds of laryngeal specimen and any type of operating technique (CO2 laser, cold instruments by endoscopic or microscopic techniques).
Study Design
Experimental construction and validation of a highly specialized dissection station.
Setting
Laboratory and international dissection course.
Methods
We designed a lightweight dissection station made of polycarbonate resin approved for use with a CO2 laser. The cylindrical box hosts an articulated laryngeal support. The laryngoscope is positioned on an articulated arm, which is fixed on the construction’s footplate. Validation of the larynx box was performed during an international dissection course on laryngeal surgery held in January 2016.
Results
We assessed the suitability of our novel dissection station among specialized laryngologists with a mean experience of 14 years. Feedback from the participants was very positive, with a mean general impression of 9.5 (out of 10 points) and a recommendation score of 9.6 for further use. Its utility in transforming the taught surgical steps into daily practice has been highly recognized, with a score of 9.5.
Conclusion
The lightweight and transparent larynx box is suitable for any kind of laryngeal specimen, and any surgical intervention can be taught at reasonable cost. It is safe and suitable for use with CO2 lasers. Validation among experienced surgeons revealed its suitability in the teaching of endolaryngeal microsurgery and laser surgery.
Endolaryngeal surgery represents a group of common interventions in otorhinolaryngology, either as a diagnostic technique or as a minimally invasive approach to some laryngeal pathologies. However, the learning curve is steep in view of the limited workspace inside the laryngoscope and the length of the instruments. As is often the case in surgical training, the initial experiences are often gathered during cadaveric dissection courses. A dissection laboratory is a useful educational tool to frequently rehearse the required specialized surgical skills, particularly in endolaryngeal microsurgery and laser surgery. However, the availability of fresh human cadavers is limited and may be further restricted by financial or regulatory issues. There is therefore an urgent need for low-cost and easy-to-handle models or simulators. 1
To this end, the ex vivo animal model is worth considering, as fresh animal specimens are widely available at very low cost. Several animal models have been proposed for endolaryngeal surgery and implemented as models. The histologic comparison of animal larynges has for some time favored the canine model. 2 Recently, several groups have described and validated the porcine larynx as a suitable candidate,3,4 which was endorsed for its phonatory properties. 5 The ovine model was also used in recent studies 6 on whole heads, even in training for fibrolaryngoscopy. 7 The choice of a suitable animal model appears to be well investigated and therefore possible.
Hence, a crucial issue to address is the setting of the dissection station. Routinely used for temporal bone dissection, ex vivo laboratories exist in numerous institutions and could host an endolaryngeal dissection station. In endolaryngeal surgery, a lifelike model should include a realistic laryngeal exposure, and it should be comfortable to use, hygienic, and safe with regard to use with a CO2 laser. Different settings for laryngologic education have been proposed, ranging from wooden boxes3,8 to specially designed larynx holders9,10 and even a manikin. 11
The aim of this study is to develop and validate a dissection station for endolaryngeal surgery suitable for different kinds of larynx (eg, human, canine, porcine, ovine) and any type of operating technique (CO2 laser, cold instruments by endoscopic or microscopic techniques). Moreover, it must be safe, hygienic, portable, and easy to use.
Material and Methods
Larynx Box
We constructed a dissection station box ( Figure 1 ) from CO2 laser-resistant material called Makrolon (Bayer Material-Science, Leverkusen, Germany). It is composed of linear polycarbonate resins and low-viscosity, high-performance thermoplastics, which completely absorb the laser energy. The polycarbonate is bought as flat plates or cylindrical tubes and thereafter cut into the required forms. The cylindrical container of 25-cm diameter is fixed with liquid bicarbonate glue on a footplate of the same material, measuring 40 cm in length and 30 cm in width. The laryngeal support hosted by the dissection station consists of a plate of 130 mm in length and 64 mm in width, with 4 incisions on each side to fix the straps, which securely fix the specimen. It is articulated in all 3 dimensions for optimal positioning as a function of the laryngeal specimen used. Required material thickness is 8 mm for the straight parts and 4 mm for the tube. The specimen remains accessible during the whole procedure through the cap on top of the box. An external articulated arm mounted on the footplate serves as holder of the laryngoscope, measuring 75 × 65 mm and with a height of 112 mm. The position (height and inclination) of the laryngoscope may be adjusted by the 2 screws. A rubber diaphragm covers the opening for the laryngoscope (40 mm in diameter). There are 4 rubber feet on the base of the station to prevent it from slipping. Total height of the device is 26.7 cm. Details on the construction are shown in Figure 2 . For optimal exposure and an ergonomic setting, the position of the laryngoscope and the laryngeal support may be amended when required. The transparent material allows constant verification of the accurate placement of the specimen, laryngoscope, and instruments during training. Moreover, it guarantees a hygienic work environment, since it can easily be cleaned and disinfected after use (even by a machine). Moreover, the lightweight larynx box (approximately 1.5 kg) is portable and may therefore be used in different facilities.
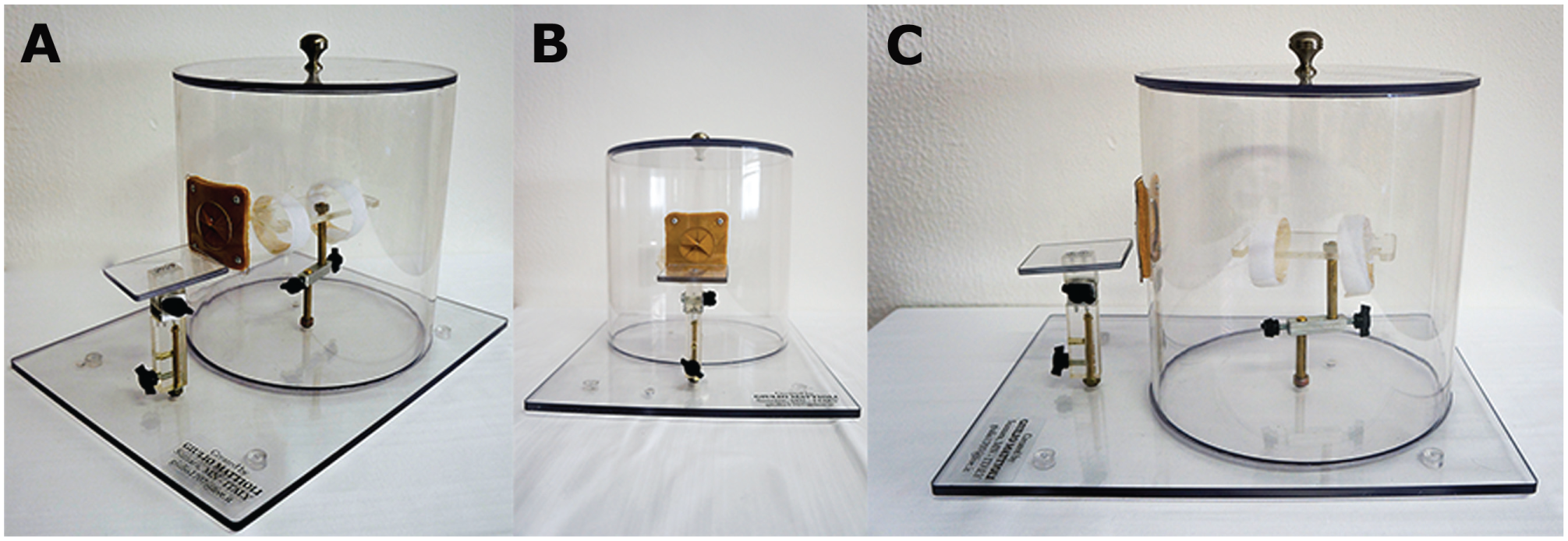
A-C, Multiple views of the ready-to-use dissection station constructed from polycarbonate resins. The laryngeal specimen and the laryngoscope are fixed on articulated arms permitting an ergonomic dissection.
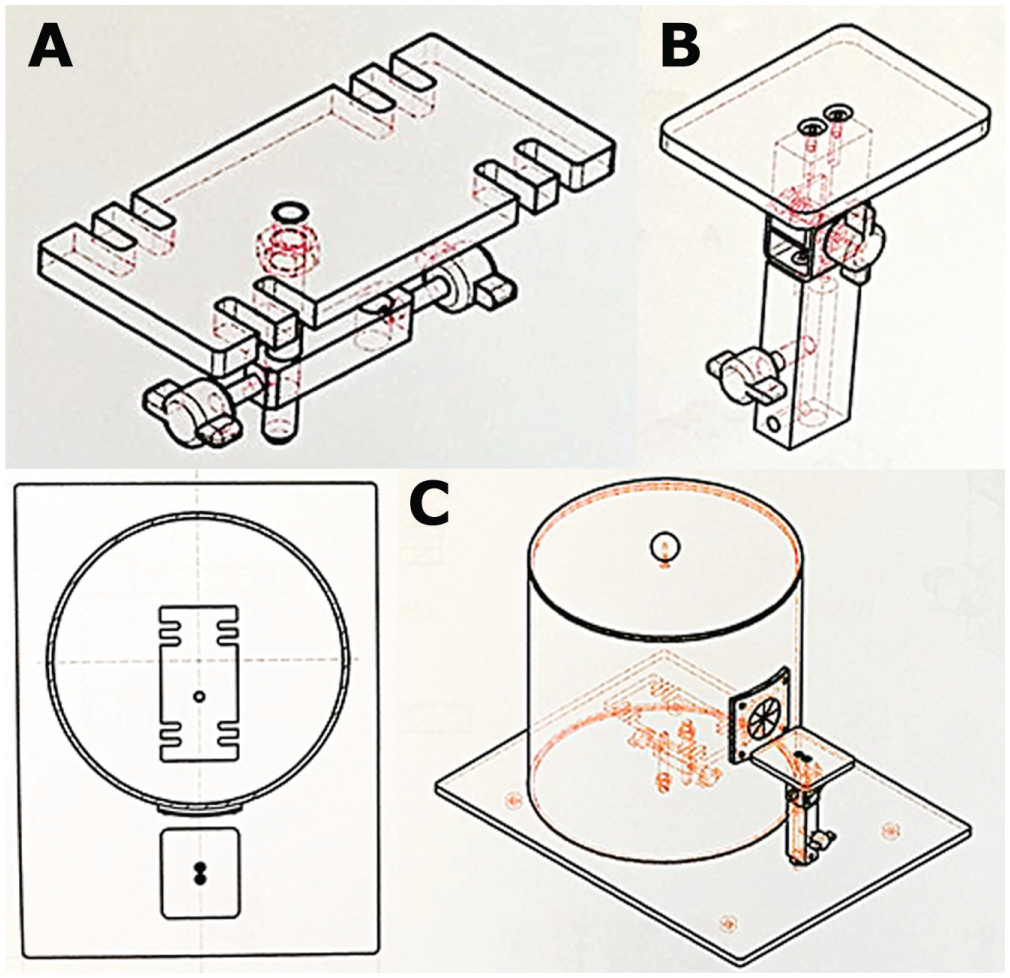
Construction details. A, Internal articulated holder of the laryngeal specimen. B, External articulated holder of the laryngoscope. C, Cylindrical box measuring 25 cm in diameter and fixed on a plate, 30 × 40 cm.
The production cost is <300 euros. The Patent Cooperation Treaty has patented the dissection station as a CO2 laser box for surgical simulation (patent 43828).
Dissection Course and Larynx Box Evaluation
In January 2016, we evaluated the dissection station during an international dissection course on the laryngotracheal framework, which was run in the Department of Otorhinolaryngology–Head and Neck Surgery at University Hospital of Modena, Italy with 24 participants.
For optimal teaching during dissection, we used our larynx box equipped with a laryngoscope with an integrated 0° endoscope (Karl Storz, Tuttlingen, Germany) connected to a portable screen with a light source (Karl Storz), which was placed in front of the dissector ( Figure 3A ). The panoramic view of the larynx offered by the endoscope allowed a thorough understanding of the anatomic structures and the teaching steps involved in the different interventions.
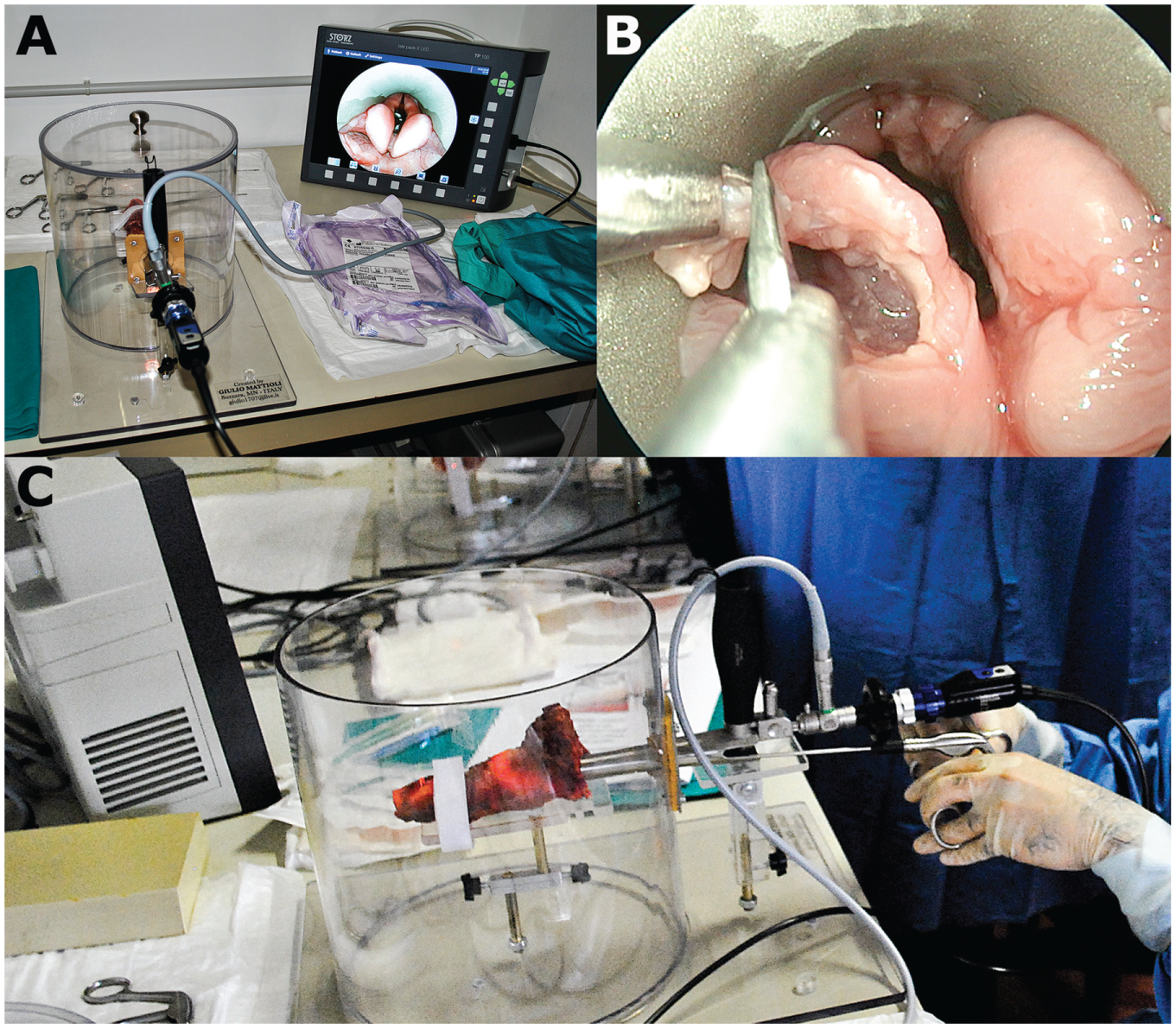
Endoscopic setup. A, Dissection course setup with a laryngoscope containing a 0° endoscope connected to a portable screen. B, Sample dissection. C, Overview of the dissection station in use.
Since the ovine model has been described to be suitable for laryngology training, 6 we used the larynges of 6-month-old lambs from the local butchery. Our Institutional Review Board approved the use of fresh ex vivo ovine laryngotracheal specimens in the larynx box. Animal welfare and slaughtering are subject to regular veterinary inspection and regulations for alimentary use. All participants were trained in cordectomy, arytenoidectomy, posterior cordotomy, and supraglottoplasty ( Figure 3 ).
After the course, each participant completed a questionnaire to subjectively evaluate the larynx box and its suitability for surgical training. We evaluated tissue properties, reliability of dissection, level of difficulty, as well as the general properties of our dissection station, such as specimen position, laryngeal exposure, suitability of the station, and whether the experience gained during the dissection would translate into clinical practice. For each question, the participants gave a rating from 1 (very poor) to 10 (excellent).
CO2 Laser Training
The use and safety of the larynx box with use of the CO2 laser were evaluated in our laboratories. Makrolon is also used in the production of laser protection glasses and is therefore considered to be laser safe. Moreover, polycarbonates are flame retardants and provide additional safety when used with a CO2 laser. As expected, we did not note any damage or alterations to the dissection station during its use with the CO2 laser.
After setting up the box as described, we performed the same exercises with cold instruments (cordectomy, arytenoidectomy, posterior cordotomy, and supraglottoplasty) using a Leica F40 microscope and a CO2 laser ( Figure 4 ). All participants wore standard eye protection glasses as routinely used during CO2 laser surgery.
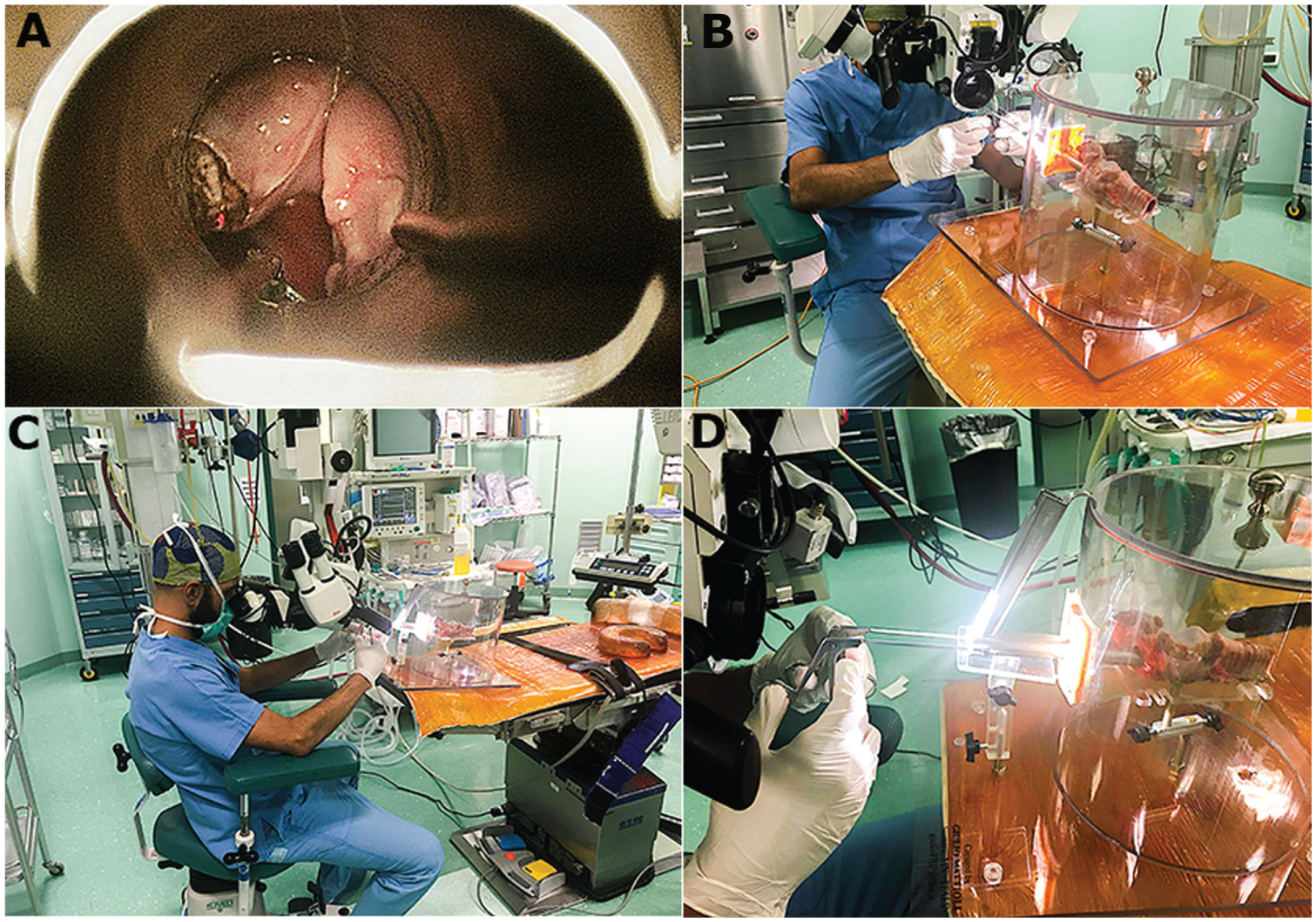
Microscopic setup. A, Example of CO2 laser dissection of an ovine larynx. B-D, Different angles and overview of the dissection station in use with a microscope.
Results
We assessed the suitability of our novel dissection station among 24 specialized laryngologists, with a mean experience of 14 years (range, 3-35 years). The participants came from 8 countries.
The feedback from the participants was very positive, with a mean general impression of 9.5 points (out of 10) and a mean recommendation score of 9.6 for further use. The larynx box was shown to be very convenient for surgical training, with a high rate of approval and a highly recognized utility in transforming the taught surgical steps into daily practice (9.5).
Figure 5 summarizes all results concerning the questions put to the participants during the dissection course.
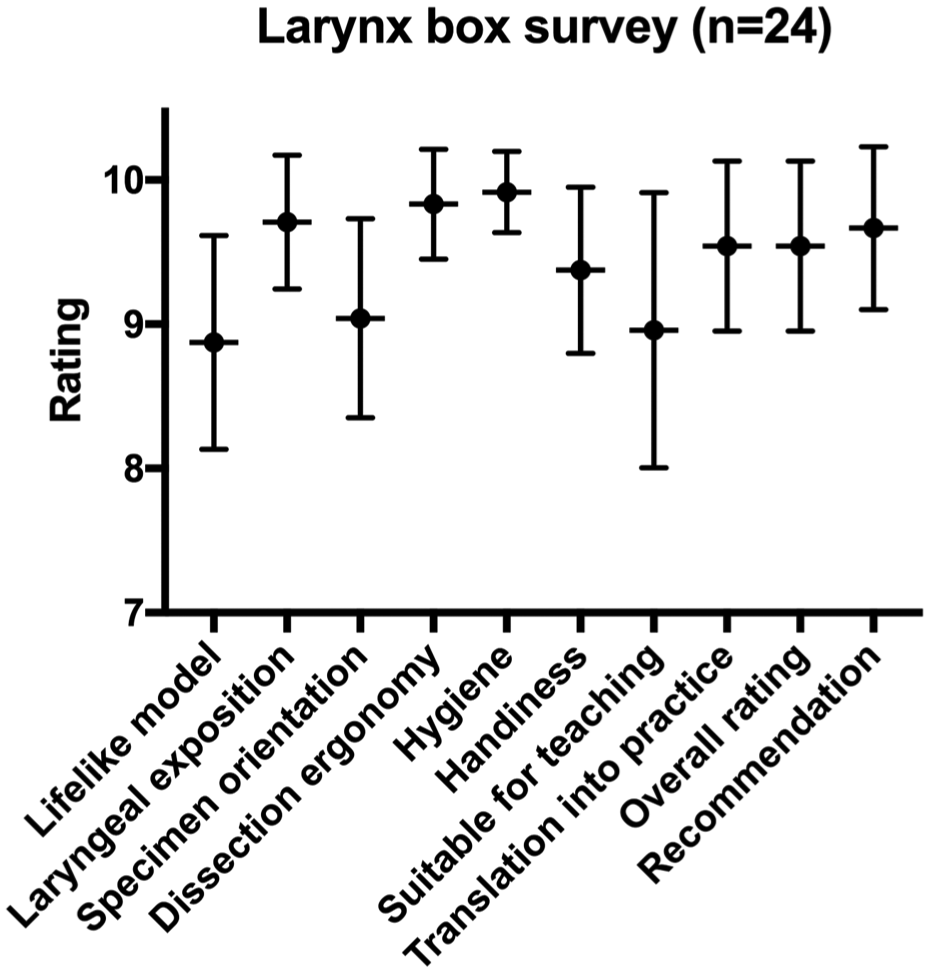
Dissection course survey. Subjective performance of the larynx box is shown as x-y plot. Scores range from 0 (very poor) to 10 (excellent). Values are represented as mean ± SD.
During CO2 laser dissection, the larynx box appeared to be safe, and no material alterations were observed. All surgeons easily performed the proposed endolaryngeal interventions.
Discussion
The system for endolaryngeal surgery presented in this study is a lightweight, safe Makrolon construction containing adjustable holders for a laryngeal specimen of any kind (human, animal) and with any laryngoscope. These precisely adjustable parts provide a realistic laryngeal exposure simulation. Moreover, the dissection station is relatively small, portable, and easy to clean and disinfect. It may be integrated without any drawbacks in an already-existing dissection and training laboratory (eg, temporal bone dissection laboratory containing a microscope) or brought to the operating room or any other facility suitable for surgical training.
Moreover, our dissection station permits use with CO2 lasers. The polycarbonate resins used for the box absorb the laser energy, representing no danger to the environment. Therefore, the Patent Cooperation Treaty approved it for use with a CO2 laser. The use of the CO2 laser in endolaryngeal surgery represents an important aspect of modern surgical approaches and has its own learning curve. 12 In our experience, training in the use of a CO2 laser can be easily performed on fresh tissue via the described dissection station. The trainee may improve his or her understanding of tissue reactions to the application of CO2 laser and therefore gain useful experience and not just in the handling of the instruments. Since the larynx box may be brought to the operating room or a temporal bone dissection laboratory, we may take advantage of already-existing infrastructure for education, which limits additional costs.
In 1997, Paczona presented a larynx holder composed mainly of a wooden box. 8 In 2012, Nasser et al presented a wooden system for education in phonomicrosurgery. 3 In our opinion, the choice of a highly durable polycarbonate resin material has several advantages over wood—namely, its weight, the possibility to clean and disinfect it, and its safety with use of CO2 lasers. Moreover, in a wooden box, the position of the specimen, the instruments, and the laryngoscope may not be assessed during dissection without opening it. Specially designed dissection stations, including custom-made laryngoscopes9,10 or even a wall-mounted laryngoscope, 4 are suitable for permanent installation in a dissection laboratory, but they are heavy and therefore not easily portable, as required during dissection courses, for example. With the system described (larynx box, 0° endoscope fixed to the laryngoscope, and portable screen with integrated light source), a dissection course may be organized with reasonable material expense at any suitable venue.
The same advantage applies to the use of CO2 lasers, since they may not be available at every dissection laboratory. Moreover, in open designed dissection stations, the use of CO2 lasers cannot be considered safe, as when used in a closed box made of certified material. The airway manikin with an integrated porcine larynx developed in 2012 by Nixon et al 11 presents the advantage of simulating laryngeal exposure on a manikin rather than adjusting the different holders, as in all other stations (including that described here). Nevertheless, the cost-effectiveness of this model remains an issue, since these airway models are expensive, although the authors did not mention its price. Moreover, they cited the risk of fire with use of the CO2 laser. In our opinion, dissection in the laboratory should be safe and without any compromise.
As for the use of synthetic models, 13 the animal model appears to be superior in terms of tissue quality and tactile feedback to the operator during dissection. Furthermore, the range of possible interventions taught on a real larynx is higher than on a synthetic model, which in fact is not as cost-effective as an animal model. 14 The use of widely available and cheap animal larynges is, in our opinion, a valuable aspect in terms of providing a lifelike educational experience.
We designed the tool described here and used during the dissection course, but we did not evaluate it. This represents a limitation of the study as compared with, for example, Dedmon et al, 4 who validated their simulator. Further evaluation by setting up a standardized educational program using our novel dissection station will be the subject of further research.
Conclusion
We designed and validated a highly developed dissection station for endolaryngeal surgery. The lightweight and transparent larynx box is suitable for any kind of laryngeal specimen, and any surgical intervention can be taught at reasonable cost. Moreover, it is safe and suitable for use with CO2 lasers. Validation among experienced surgeons revealed its suitability as a teaching tool in endolaryngeal microlaser and laser surgery.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We wish to thank Giulio Mattioli, who handcrafted the larynx box.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.