
Abstract
Objective
The primary objective was to determine the prevalence of Helicobacter pylori among patients with laryngopharyngeal reflux. The secondary objective was determining if H pylori eradication leads to greater symptom improvement in patients with laryngopharyngeal reflux as compared with standard proton pump inhibitor therapy alone.
Data Sources
EMBASE, Cumulative Index to Nursing and Allied Health Literature, MEDLINE, World Health Organization International Clinical Trials Registry Platform, European Union Clinical Trials Register, Cochrane Library databases of clinical trials, and ClinicalTrials.gov.
Review Methods
A systematic review was performed of studies assessing the diagnosis or treatment of H pylori among patients with laryngopharyngeal reflux. Randomized controlled trials, cohort studies, case-control studies, and case series were included. A meta-analysis of prevalence data and assessment of heterogeneity was performed on relevant studies.
Results
Fourteen studies were analyzed in the review, with 13 eligible for the meta-analysis. We determined that the prevalence of H pylori among patients with laryngopharyngeal reflux was 43.9% (95% confidence interval, 32.1-56.5). The heterogeneity of studies was high, with an overall I 2 value of 92.3%. We were unable to quantitatively assess findings for our secondary outcome, since H pylori identification and treatment were not the primary focus of the majority of studies.
Conclusion
There is a high rate of H pylori infection among patients with laryngopharyngeal reflux. The infection rate in North America and Western Europe has not been adequately studied. There is insufficient evidence to make a recommendation regarding the testing and treatment of H pylori infection among patients with laryngopharyngeal reflux.
Laryngopharyngeal reflux (LPR) is an extraesophageal manifestation of gastroesophageal reflux disease (GERD) and is a common problem in the field of otolaryngology. 1 Indeed, LPR is diagnosed in up to 10% of patients presenting to an otolaryngologist 2 and approximately one half of all patients with laryngeal disorders. 3 The most common symptom of LPR is chronic dysphonia (92% of patients), 4 followed by chronic throat clearing (50%), chronic cough (44%), globus pharyngeus (33%), and dysphagia (27%).4,5 The proposed direct mechanism for LPR is the retrograde flow of gastric contents into the laryngopharynx. 2 There, the acid and pepsin of the refluxate cause inflammation and irritation of the sensitive tissues of the larynx and hypopharynx. Another indirect proposed mechanism is irritation of the esophagus, which triggers a vagal-mediated laryngeal reflex, resulting in LPR symptoms. 6 One important feature of LPR, as compared with GERD, is that fewer episodes of reflux are necessary to injure laryngeal mucosa as opposed to mucosa of the esophagus. 7 Only 3 episodes of reflux per week are required to initiate the symptoms of LPR, while GERD requires nearly 50 per week.8,9
Despite the frequency with which LPR is encountered, controversy still exists regarding the pathophysiology and the optimal investigations for diagnosis or the optimal treatment. 1 Although tests such as 24-hour double-probe pH monitoring and multichannel impedance are currently considered the gold standard in LPR diagnosis, the cost, time, and invasiveness of these investigations often render them impractical.1,10 Otolaryngologists therefore typically rely on clinical diagnosis alone.
The current mainstay of LPR treatment is largely based on the treatment of GERD, with acid suppression through H2 antagonists, proton pump inhibitors (PPIs), and lifestyle modifications. These interventions have been shown to be of benefit among patients with symptoms of GERD and laryngopharyngeal symptoms.1,10,11 However, a significant number of patients do not respond to PPI therapy and continue to be symptomatic.1,12 This demonstrates the need for a better understanding of the disease, as well as the need for more effective treatments for patients with LPR.
Helicobacter pylori is recognized as the major causative agent of chronic gastritis, peptic ulcer disease, gastric adenocarcinoma, and gastric MALT lymphoma. 13 The effects of H pylori on GERD are more complex and depend on the predominant anatomic pattern of infection. 13 When H pylori infection occurs in the gastric antrum, it causes an increase in the acidity of gastric secretions; eradication of H pylori in these patients is associated with improved reflux symptoms. 14 There have, however, been significantly fewer studies investigating the relationship between H pylori and LPR.
Our goal was to improve the understanding of the role of H pylori in LPR through a systematic review and meta-analysis. The primary objective of this study was to determine the incidence of H pylori infection among patients with clinically diagnosed LPR. As a secondary objective, we wished to determine if diagnosing and eradicating H pylori in LPR patients leads to greater improvement in LPR symptoms when compared with standard PPI therapy alone.
Materials and Methods
Search Strategy
With the assistance of an experienced librarian at the University of Ottawa, we searched databases including EMBASE, MEDLINE (via OVID), the Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature, World Health Organization International Clinical Trials Registry Platform, European Union Clinical Trials Register, Cochrane Library databases of clinical trials, and Clinicaltrials.gov. The search included studies between 1946 and October 27, 2015.
Exclusion of duplicate abstracts was performed by the 2 primary authors (R.C, J.P.B.). Eligibility of titles and abstracts were independently assessed by the primary authors. Articles that were deemed eligible and met inclusion criteria then underwent a qualitative and a quantitative analysis by the same 2 authors. Disagreements between authors were resolved through consensus.
Our review was performed in accordance with the guidelines and standards of the Cochrane Handbook for Systematic Reviews of Interventions. 15 We reported our findings in accordance the PRISMA standards (Preferred Reporting Items for Systematic Reviews and Meta-analyses). 16 Our review was registered prospectively with PROSPERO (2015:CRD42015024312). 17
Inclusion and Exclusion Criteria
All studies investigating the prevalence, treatment, or identification of H pylori among patients with LPR were included for the initial review. Studies were included that included an assessment and/or treatment of GERD in addition to LPR, but they were excluded if the focus was solely on GERD. Randomized controlled trials (RCTs), cohort studies, case-control studies, and case series were included. Studies were excluded that did not test for H pylori or did not report a prevalence of H pylori. Only studies published in English were included.
Data Extraction
Data forms were developed prospectively and tested on a small number of studies. Study-related data were recorded: the type of study, the author list, the country where the study took place, the year of publication, and the number of patients involved. Patient demographics were recorded, including age, sex, and ethnicity, as were the inclusion and exclusion criteria of the study. The method of LPR diagnosis was recorded, including whether 24-hour pH monitoring and validated symptom/finding severity scores (Reflux Symptom Index and/or Reflux Finding Score) were employed or whether the diagnosis was made by clinical grounds alone. 5 The diagnostic methods used to detect H pylori and the resulting prevalence of H pylori among patients with LPR were recorded. The prevalence of GERD in study populations, if reported, was recorded. Treatment regimen and response to treatment, if reported, were also recorded.
Risk-of-Bias Assessment
Two authors (R.C., J.P.B.) independently utilized the Cochrane Collaboration’s tool for assessing risk of bias to evaluate RCTs for selection, performance, detection, reporting, attrition, and other biases. 18 The Newcastle-Ottawa Scale was used to assess cohort studies. 19 Risk of bias was not assessed in case series and case-control studies. Discrepancies between researchers were settled through consensus.
Data Analysis
Results were reported descriptively first. DerSimonian and Laird’s random effects approach was used for meta-analysis. 20 When it was not possible to conduct a head-to-head comparison between treatments, a meta-analysis of prevalence data was performed.
Statistical heterogeneity among studies was quantified with the I 2 statistic and by assessing the significance of the Cochrane Q test. Regarding I 2 , 50% was used as a threshold to discriminate between low and high heterogeneity. 21 When a high level of heterogeneity was encountered, a subgroup analysis was conducted to further explore sources of variability among studies. 22 The following clinical and methodological covariates were used for subgroup analysis: method of H pylori detection, patients with or without presence of GERD, method of LPR diagnosis, study design, and geographic region where the study was conducted. PRISMA guidelines were utilized for reporting of data analysis.
Results
General Study Information
A total of 1082 studies were identified through our literature search and reviewed ( Figure 1 ). After discussion between reviewers, 26 papers were included for full-text review.23-48 Twelve papers were subsequently excluded, yielding 14 that were identified for data collection and qualitative analysis.23-34 Further details of the excluded papers may be found in Appendix A (available in the online version of the article). The details of the papers included in the analysis are located in Table 1 .35-48 One further paper 43 was excluded from the quantitative analysis because H pylori positivity was used as an inclusion criterion; thus, it could not be included in the analysis for prevalence of H pylori. This left a total of 13 papers in our quantitative analysis.
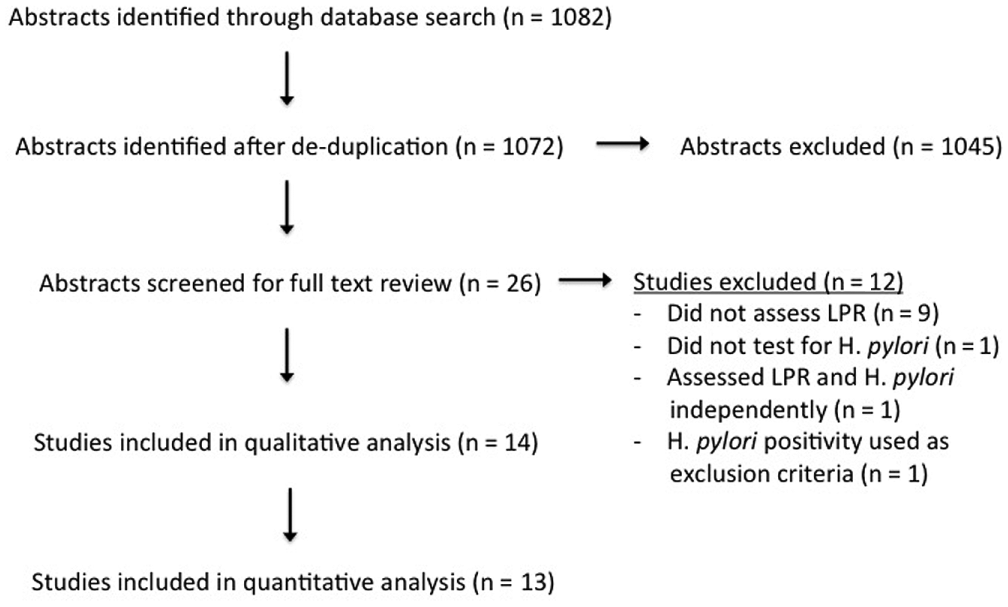
PRISMA flow diagram of study selection. H pylori, Helicobacter pylori; LPR, laryngopharyngeal reflux.
Study Characteristics and Risk of Bias.
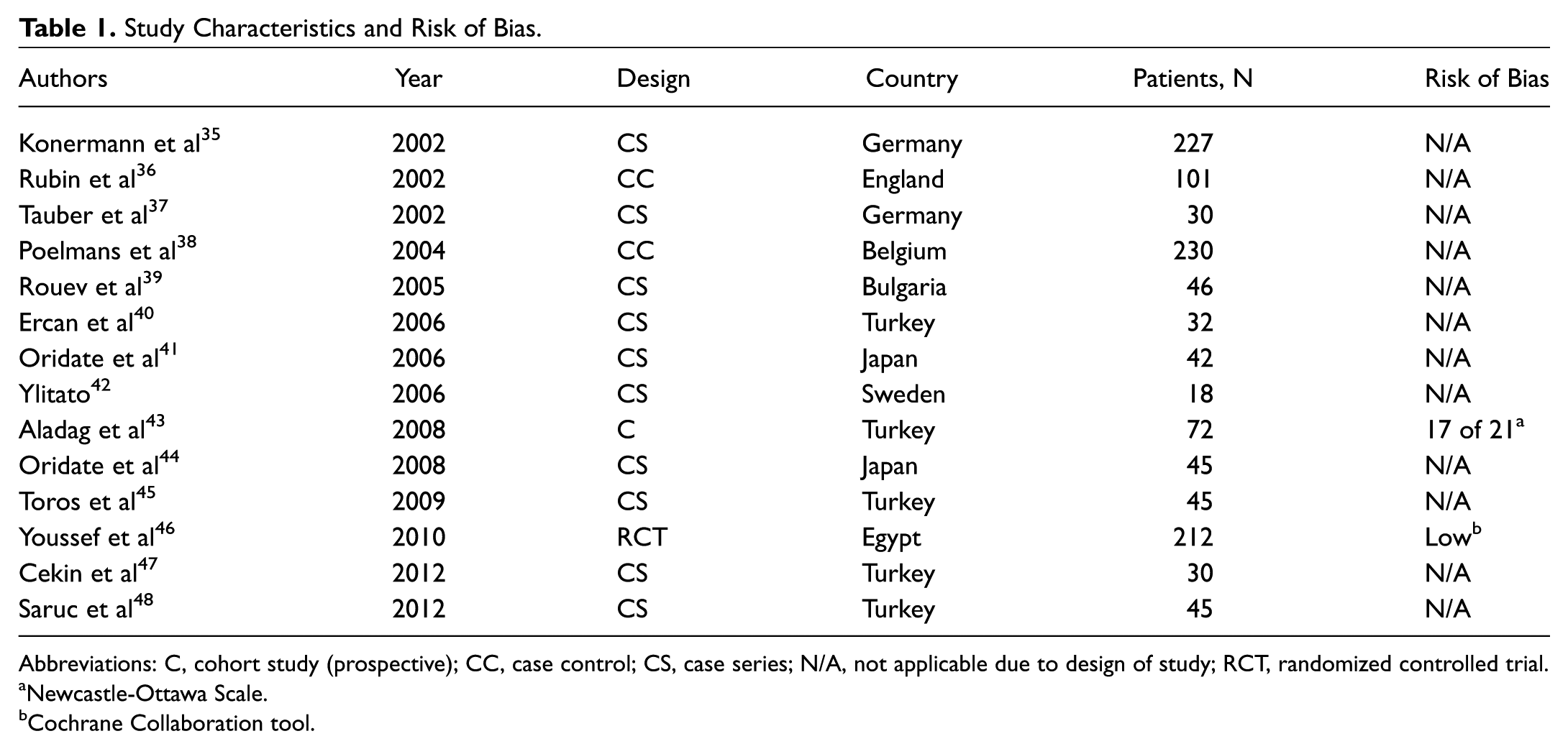
Abbreviations: C, cohort study (prospective); CC, case control; CS, case series; N/A, not applicable due to design of study; RCT, randomized controlled trial.
Newcastle-Ottawa Scale.
Cochrane Collaboration tool.
Risk-of-Bias Assessment
Only 1 RCT was included in our meta-analysis; the risk of bias of this study was low. 46 Only 1 other study met inclusion criteria for risk-of-bias assessment, with an overall Ottawa-Newcastle score of 17 our of 21, indicating low risk of bias. This study was included in the systematic review; however, it was excluded from the meta-analysis. 43 All other included studies were case-control or case series; therefore, risk-of-bias assessment was not performed.
Clinical Characteristics
Of the 13 studies included in the quantitative analysis, 10 were performed in Europe (including Turkey),35-40,42,45,47-49 2 in East Asia,41,44 and 1 study in Northern Africa ( Table 2 ). 46 H pylori prevalence within individual studies ranged from 7.1% to 68.8% ( Table 3 ). Testing for H pylori was most commonly performed by gastric antral biopsy (n = 6),37-40,45,48 followed by serology (n = 3).27,36,41 One study employed urea breath testing 42 ; another used H pylori stool antigen testing 46 ; and a final study utilized polymerase chain reaction (PCR) for H pylori of tissue obtained from a laryngeal biopsy. 47 One study did not indicate the method of H pylori detection. 35 In the diagnosis of LPR, 3 studies used 24-hour pH monitoring to confirm the diagnosis.35,40,46 Considering GERD as a distinct diagnosis from LPR, 2 studies reported a prevalence in the range 0% of 50%.35,37 Three studies reported a prevalence in the range of 50% to 75%.39,40,42 Five studies had a GERD prevalence of 100%.38,41,44,45,48 Three studies did not assess for GERD.36,46,47
Study Clinical Characteristics.
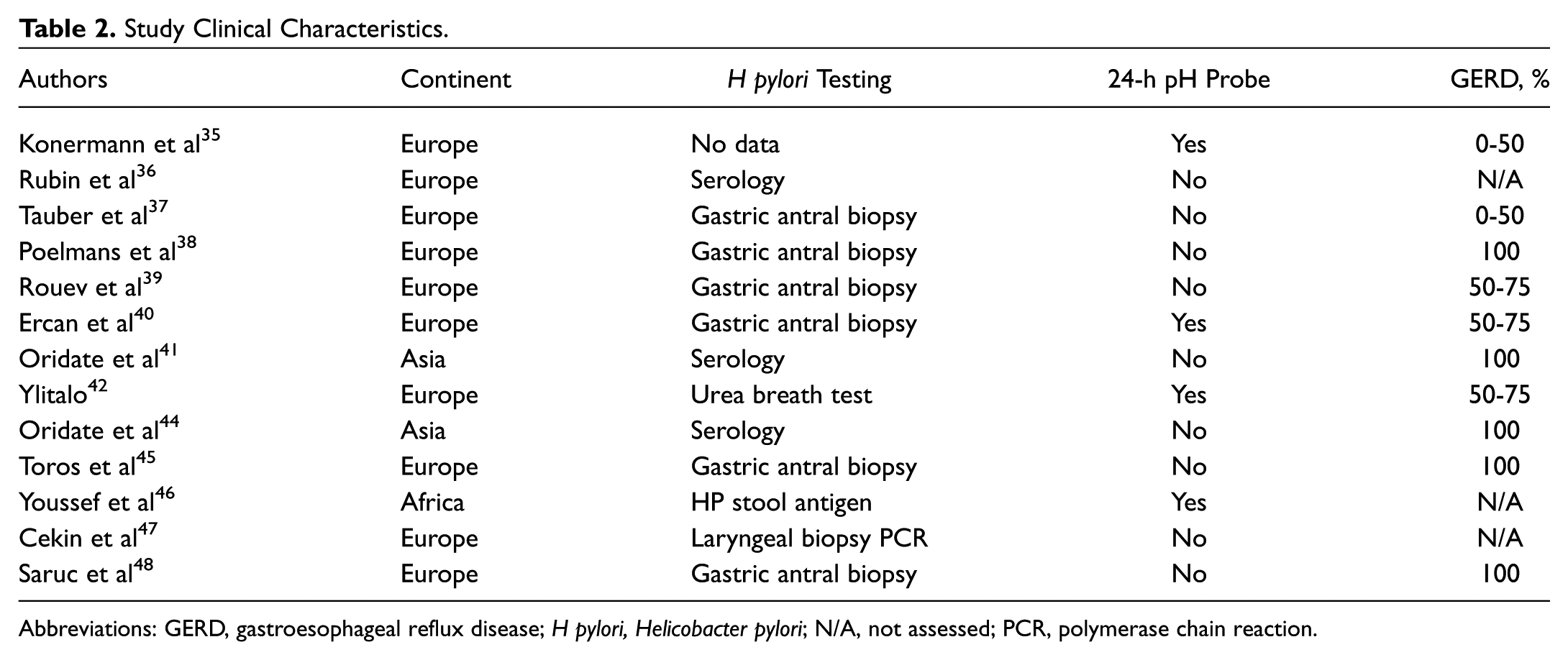
Abbreviations: GERD, gastroesophageal reflux disease; H pylori, Helicobacter pylori; N/A, not assessed; PCR, polymerase chain reaction.
Prevalence of Helicobacter pylori.
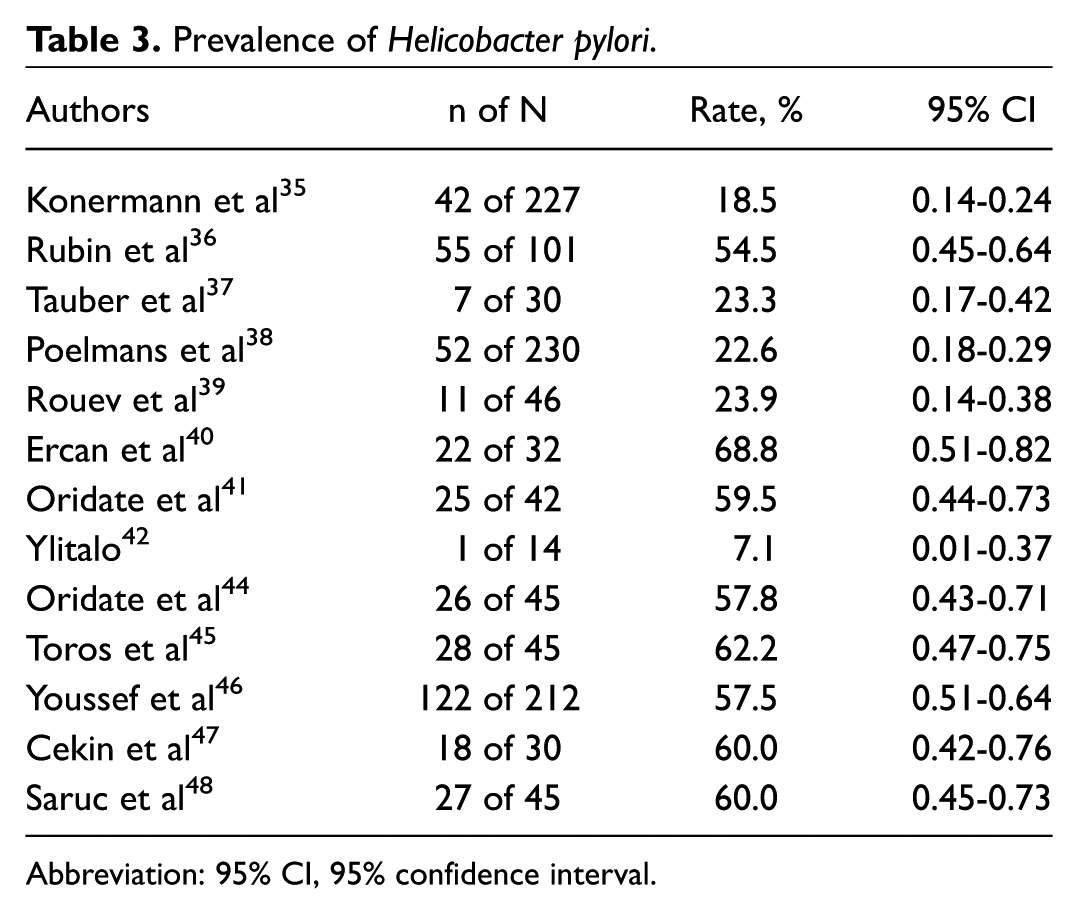
Abbreviation: 95% CI, 95% confidence interval.
Prevalence Rates and Assessment of Heterogeneity
From meta-analysis, the overall median prevalence of H pylori among patients with LPR across the 13 studies included in the quantitative analysis was 57.5%, with a range between 18.5% and 68.7%. Heterogeneity, an I 2 value of 92.3% (Q = 155.1, P < .001) was obtained, indicating high levels of heterogeneity. Due to the significant heterogeneity, we did not perform a standard meta-analysis on the prevalence data. There was a positive association between rate of concomitant GERD with LPR and H pylori positivity. Studies reporting a rate of GERD between 0% and 50% had a 20.5% prevalence of H pylori 35,37; the prevalence of H pylori was 35.2% in studies with a GERD rate between 50% and 75%39,40,42 and 51.1% in studies where the rate of GERD was 100% ( Table 4 ).38,41,44,45,48
Subgroup Analysis of H pylori Prevalence Based on Study Design Characteristics.
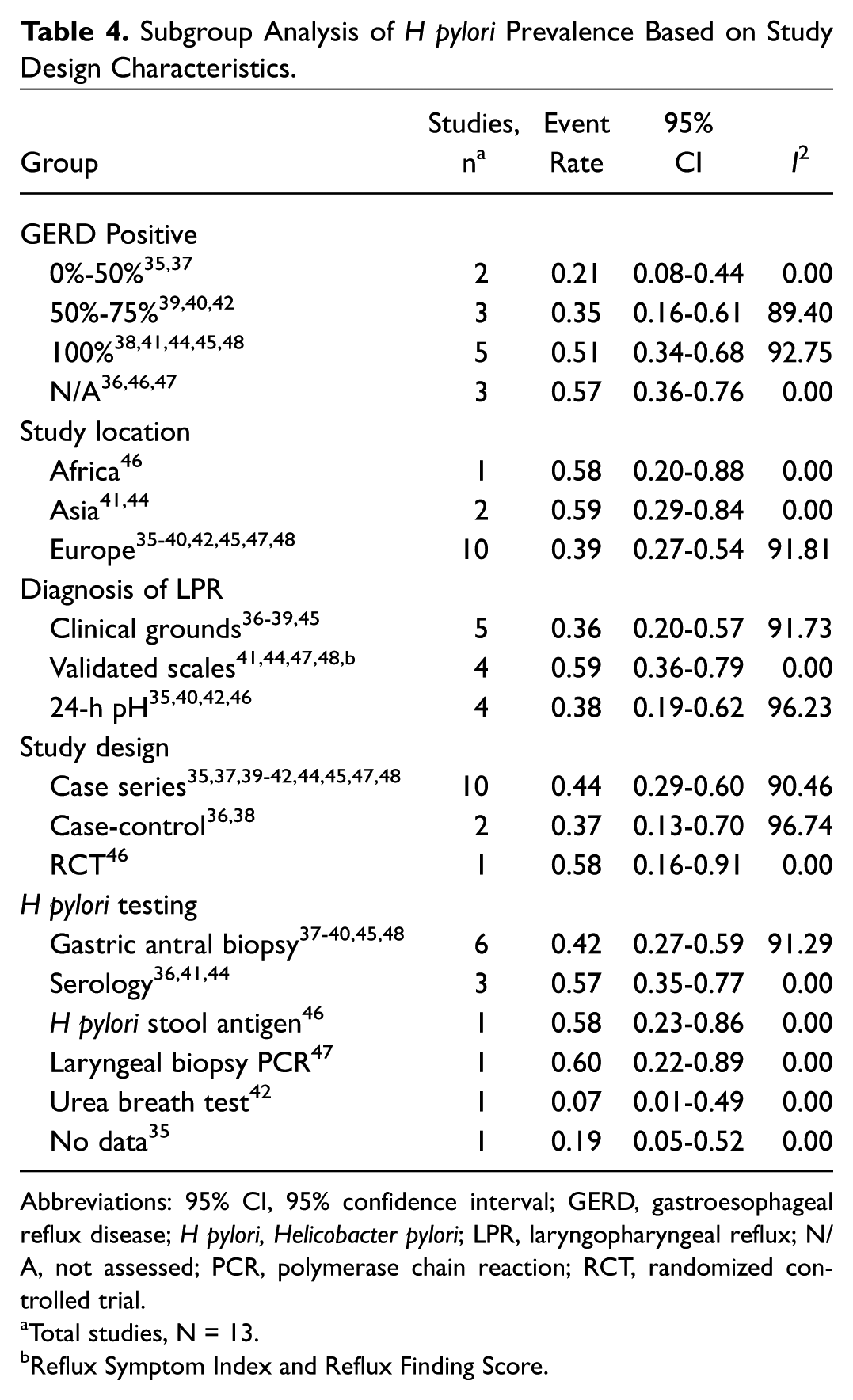
Abbreviations: 95% CI, 95% confidence interval; GERD, gastroesophageal reflux disease; H pylori, Helicobacter pylori; LPR, laryngopharyngeal reflux; N/A, not assessed; PCR, polymerase chain reaction; RCT, randomized controlled trial.
Total studies, N = 13.
Reflux Symptom Index and Reflux Finding Score.
Subgroup Heterogeneity Analysis
To explore the effects of sources of variability among studies, we performed additional analysis on subgroups based on presence of GERD, geographic location, method of LPR diagnosis, method of H pylori detection, and study design. In terms of the percentage of patients with GERD symptoms, high levels of heterogeneity were noted in studies that had 50% to 75% of patients with GERD (I 2 = 89.3%)39,40,42,47 and 100% (I 2 = 92.7%; Table 4 ).38,41,44,45,48,50 In studies with no patients with GERD or studies that did not assess for GERD, heterogeneity was low (I 2 = 0).35-37,46,47 The majority of studies were performed in Europe (10 of 13), and these studies had high levels of heterogeneity (I 2 = 91.8%).35-40,42,45,47,48 A comparison of subgroups by method used to diagnose LPR noted high levels of heterogeneity when the diagnosis was made on clinical grounds alone (I 2 = 91.7%).36-39,45 In studies that used validated scoring scales for diagnosis, heterogeneity was low (I 2 = 0%).41,44,47,48 Heterogeneity was also high (I 2 = 96.2%) when 24-hour pH monitoring was employed for diagnosis.35,40,42,46 In terms of the study design, case series35,37,39-42,44,45,47,48 and case-control35,36 designs demonstrated high levels of heterogeneity (I 2 = 90.5% and 96.7%, respectively). Only 1 RCT was performed; thus, no heterogeneity was calculated for this study design. 46 When the subgroups were evaluated by method used to assess and diagnose H pylori, the 6 studies utilizing gastric antral biopsy had high heterogeneity (I 2 = 91.3%),37-40,45,48 and the 3 studies using serology had low heterogeneity (I 2 = 0%).36,41,44 Of the rest of the studies, 1 used stool antigen testing 46 ; 1, laryngeal biopsy PCR 47 ; 1, urea breath test 42 ; and 1, no method of testing reported. 35 Thus, no heterogeneity analysis was conducted for these studies.
The Effect of H pylori Eradication on LPR Symptoms
In the majority of the studies identified, H pylori identification and treatment were not the primary focus. Given this, we were unable to assess for our secondary outcome; however, we descriptively report the findings of studies investigating this association in the discussion.
Discussion
LPR is one of the most commonly diagnosed problems in the field of otolaryngology. However, the current mainstay of treatment—acid suppression therapy with PPIs—is not uniformly effective. 12 Given its complex association with GERD, we hypothesized that H pylori may be implicated in the LPR, where undetected infection may be present in refractory cases. For patients with LPR, we determined an overall prevalence of H pylori of 43.9%, representing a substantial proportion of LPR patients who are infected with H pylori; however, at present, testing for H pylori is not routine in the workup of LPR.
Two studies compared standard treatment for LPR with that of H pylori eradication in terms of symptom resolution. In their cohort study, Aladag et al assessed 72 patients with LPR, all of whom were H pylori positive on serology. 43 Each was treated with 2 weeks of triple-eradication therapy with omeprazole, metronidazole, and amoxicillin. Three months following treatment, 44.4% (32 of 72) of patients were H pylori positive on serology after eradication therapy. A statistically significant reduction in the symptoms of throat irritation (P = .003) and sore throat (P < .001) was observed in the eradication group, based on patient self-reporting questionnaires. There was no significant reduction in chronic cough, intermittent hoarseness, globus sensation, or cervical dysphagia.
The only RCT investigating the effect of H pylori treatment on LPR was performed by Youssef et al, 46 which enrolled 212 patients with reflux symptoms and findings. The diagnosis of LPR was confirmed by 24-hour pH monitoring. These patients underwent stool antigen H pylori testing, with 57.5% (122 of 212) testing positive. The 90 patients who were H pylori negative were treated with esomeprazole (40 mg, once daily for 4 weeks). The 122 patients who were H pylori positive were randomized in 2 treatment groups: 61 underwent treatment with esomeprazole magnesium, 40mg, once daily for 4 weeks; the other received triple therapy with esomeprazole magnesium, 40mg, amoxicillin sodium, 1g, and clarithromycin, 500mg, for 4 weeks. Marked symptom improvement occurred in 87 of 90 H pylori–negative patients after PPI therapy, as graded by a single otolaryngologist. Thirty-eight percent (23 of 61) of H pylori–positive patients treated with PPI alone showed a marked improvement in symptoms after 4 weeks, as compared with 86.7% (53 of 61) in the triple-therapy group. Validated assessment scales were not used, however.
There appears to be an inverse correlation between H pylori prevalence and reflux disease on a population level; however, the effects of H pylori on GERD depend on the anatomic location of infection.51,52 Gastric antral-predominant infection has been shown to cause an increase in the acidity of gastric secretions and duodenal ulcers. This group constitutes the majority of H pylori–infected patients with coexisting GERD. 53 Eradication of H pylori in these patients is associated with improved symptoms of reflux disease. 14 By contrast, patients with corpus-predominant gastritis or pangastritis have reduced gastric acid production; H pylori infection among these patients has been found to be associated with a mild increase in GERD.53,54 Regardless, H pylori eradication is currently recommended when infection is identified in either pattern, due to its multiple negative health impacts. 55 We hypothesize that the antral-dominant group may represent certain patients with intractable symptoms of LPR; however, further studies would be necessary to explore this possible relationship.
One major limitation of our systematic review was the heterogeneity of the constituent studies. There was no standard definition or method for diagnosis of LPR across the various studies. Ideally, a high-quality study with validated symptom and finding assessment scales would provide more usable information for the practicing otolaryngologist. Furthermore, multiple diagnostic modalities for H pylori were employed, including methods both noninvasive and invasive. Gastric astral biopsy with histology was the most commonly employed method of testing, which has been shown to have a sensitivity and a specificity >95% and is considered by some to be the gold standard of H pylori diagnosis; however, cost and operator dependence of analysis are limiting factors in its use. 13 Serology was the most frequently used noninvasive testing modality employed, as used in 3 studies.36,41,44 A meta-analysis showed serology to have a sensitivity of 85% and a specificity of 79%.13,56 However, the positive predicative value is highly dependent on the prevalence in the study population. 57 Fecal antigen testing, another noninvasive method, had a very high pretreatment sensitivity, specificity, positive predictive value, and negative predictive value in a previous systematic review. 49 A single study included in our review employed PCR analysis of tissue obtained during laryngeal biopsy for H pylori. 47 In terms of LPR, it remains unknown which testing modality is optimal for confirming the presence of H pylori.
Another limitation of this systematic review is the fact that the constituent studies came from a narrow range of geographic locations. The prevalence of H pylori differs greatly by geographic location, with the prevalence in the developed world approaching 50% by age 60 years.50,58 In the developing world, the prevalence rises to 80% by age 50 years; infection is also found to occur at an earlier age in this population. Most of the studies from which our prevalence data were derived were performed in Southeast Europe and Japan, which have higher overall prevalences than North America or Western Europe. 44 Indeed, the prevalence rate among Canadian adults is 37.9%, 59 compared with a higher prevalence of 82.5% in the general population of Turkey. 60 Furthermore, although our review was performed in North America, no studies included in the review were performed in a North American population.
The accurate diagnosis and treatment of LPR remain a challenge for otolaryngologists. Given the overall prevalence of H pylori of 43.9% among patients with LPR, in the predominately Southeast European and Asian population identified herein, we believe that further study is warranted to estimate this rate in a North America population, with standardized methods of LPR diagnosis. Although we were unable to determine our secondary objective, some evidence of greater improvement of LPR symptoms with H pylori eradication exists.43,46 Despite its limitations, we believe that this study provides convincing evidence that a relationship between H pylori and LPR exists and should be further explored with a high-quality RCT. Determining if H pylori plays a role in LPR in the North American population has the potential to significantly affect patient care and treatment outcomes. Although the majority of studies are of low quality with only 1 RCT, there is evidence of a potential relationship; therefore, clinicians might consider testing for and/or treating H pylori among patients with refractory LPR.
Conclusion
In this study, we report an overall H pylori prevalence rate of 43.9% among patients with LPR. The prevalence rate was determined by meta-analysis of 13 publications; the majority of which were conducted in Western Asia and Southeast Europe. Due to the variability of H pylori prevalence among countries, it remains unclear whether a rate of 43.9% justifies recommending investigating and treating LPR patients for H pylori. However, because H pylori eradication therapy has been successful at significantly reducing some of the symptoms of LPR,43,46 this emerging relationship merits further study. We believe that a dedicated trial investigating the efficacy of H pylori eradication in a predominantly North American and Western European population is warranted and would help clarify this relationship.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Supplemental Material
Additional supporting information is available in the online version of the article.