
Abstract
Objective
A smartphone-enabled otoscope (SEO) can capture tympanic membrane (TM) images. We sought to compare a SEO to microscopic otoscopy in the detection and evaluation of TM pathology in an otology/neurotology practice.
Study Design
Prospective single-site study in adults presenting over a 3-month period.
Setting
Neurotology clinic within a tertiary care academic medical center.
Subjects and Methods
Following consent, 57 patients underwent a medical and microscopic ear examination. Afterward, clinicians photographed bilateral TMs using a SEO. A second “blinded” neurotologist received a SEO-acquired image of each TM and a brief patient history. Our primary end point was identification of TM pathology (or lack thereof) and the blinded neurotologists’ corresponding diagnosis. Secondary end points included patient-reported SEO comfort levels.
Results
A single SEO-acquired TM image and brief patient history resulted in correct diagnosis of 96% (23/24) of normal TMs and identification of 100% (33/33) of microscope-confirmed abnormal TMs. When pathology was identified by the “blinded” physician, the diagnosis was identical to that made by the primary treating physician 82% (27/33) of the time. On patient surveys, 93% (53/57) of patients felt “very comfortable” with SEO utilization, and 88% (50/57) reported viewing acquired images was “very useful” in understanding their condition.
Conclusion
A SEO is 96% specific in identifying normal TMs and 100% sensitive in identifying pathology. Its 97% positive predictive value and small false-positive rate makes it a useful screening tool. Furthermore, patients are receptive to this technology and felt comfortable with its utilization in a health care or possible telemedicine setting.
In 1841, Friedrich Hofmann described a device that could examine the tympanic membrane (TM) by focusing light into the external auditory canal. 1 Joseph Toynbee later coined the term otoscope as a reference to an instrument that can be used to diagnose disorders of the ear. 2 Since that time, the traditional handheld otoscope has proven itself as an indispensable tool in the field of otolaryngology and has not undergone any radical changes. Proper use of an otoscope requires appropriate experience and training, yielding a moderate learning curve for new users. 3
Smartphone-enabled otoscopes (SEO) can enhance visualization of the TM, feature high fidelity image and video capture features, and secure data in an encrypted Health Insurance Portability and Accountability Act (HIPAA)–compliant manner. A study that used a SEO to assess acute otitis media in children demonstrated that captured images are comparable to a conventional otoscope. 4 Furthermore, SEOs have been shown to be easier to use than standard otoscopes and can serve as efficacious learning tools for medical students and residents. 5
One potential application of SEOs is in the field of telemedicine. 6 Telemedicine extends the accessibility to general and specialized health care providers to rural areas and can improve patient satisfaction and health care–related expenses.7,8 The advantages of capturing and sending an image of a patient’s TM securely to a neurotologist for remote evaluation and consultation offers many benefits for patients and physicians. However, the accuracy of identifying TM pathology based on a single image of the TM captured by a SEO has not yet been investigated. We sought to assess the utility of a single SEO-obtained TM image in the clinical evaluation of patients with otologic symptoms compared to standard microscopic otoscopy.
Methods
This was a prospective single-site study in adults presenting to a neurotology clinic at a tertiary care academic medical center with institutional review board approval from the University of California, Irvine. Fifty-seven patients presenting to the otolaryngology clinic over a 3-month period between January and March 2016 with various otologic symptoms consented to participation in this study ( Table 1 and Table 2 ). After microscopic ear examination, subjects underwent SEO examination and photography of their right and left TMs by a trained member of the research team.
Patients Presenting with TM Pathology and Results of SEO Evaluation.
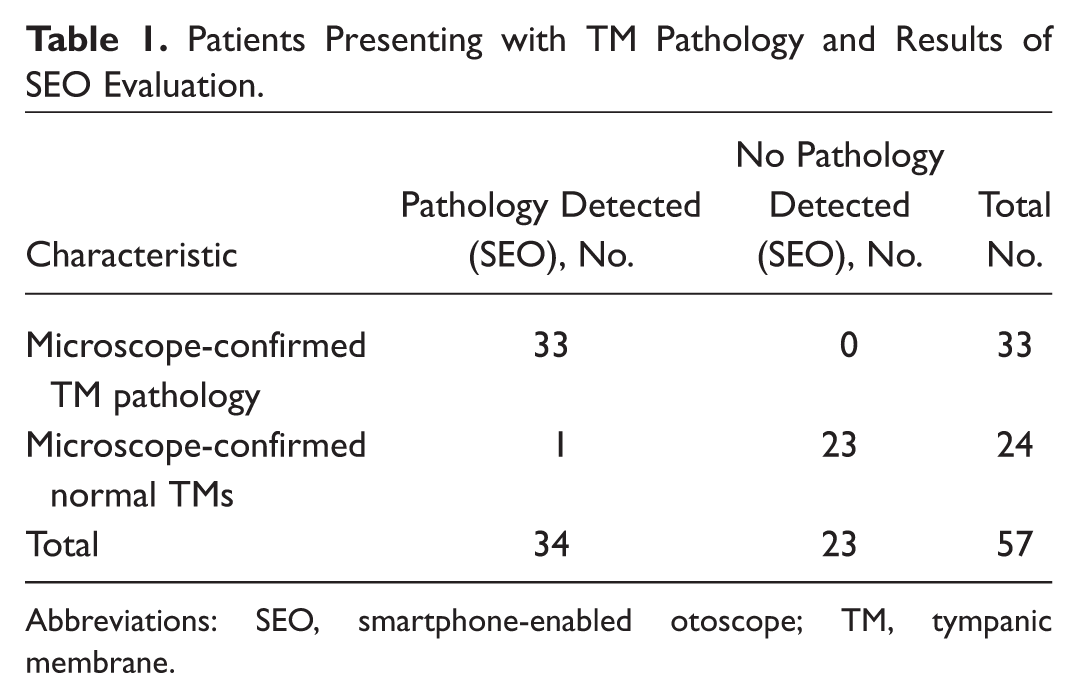
Abbreviations: SEO, smartphone-enabled otoscope; TM, tympanic membrane.
Sensitivity, Specificity, Positive/Negative Predictive Values, False Positives/Negatives.
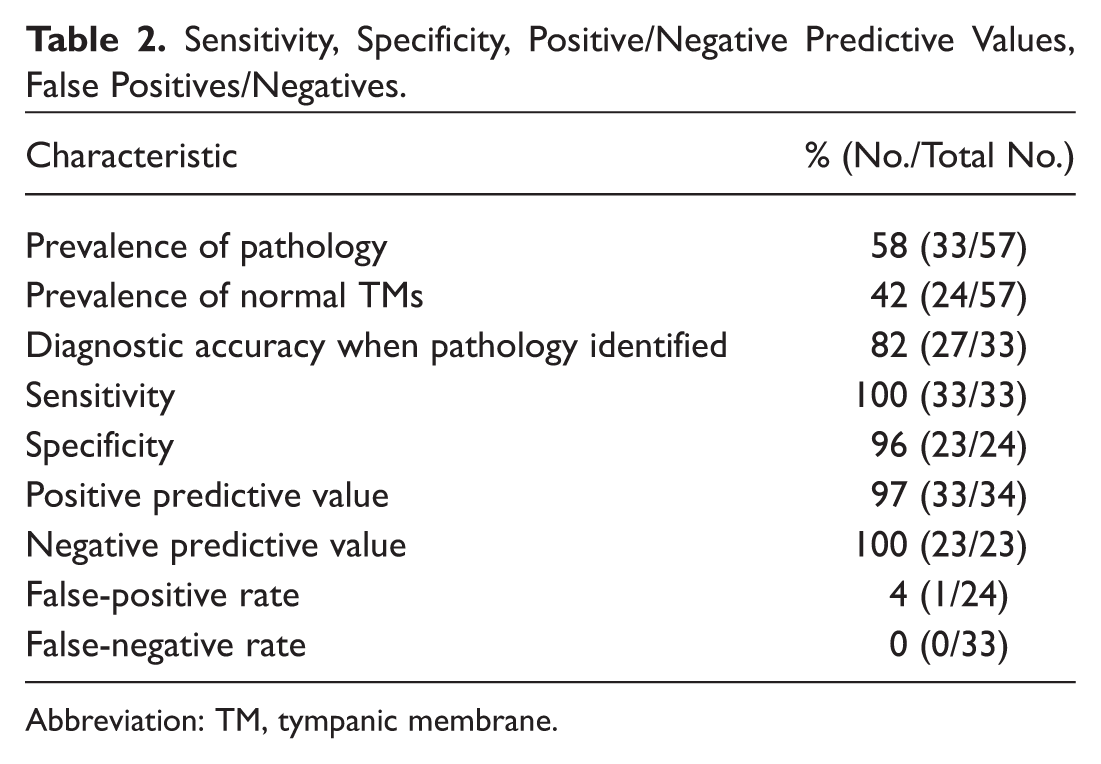
Abbreviation: TM, tympanic membrane.
Each patient subsequently received a 5-point Likert scale paper-based survey that assessed his or her comfort with SEO operation by physicians, residents, medical students, research assistants, and nurses. In addition, self-reported comfort levels with images captured on a mobile device and transmitted to other physicians assessed patient perception of digital data security. Last, self-reported comfort level with SEO as a personal health care tool in a telemedicine setting was assessed. All images were captured and stored on a 16-GB iPhone 5s (Apple, Cupertino, California) equipped with Cellscope-Oto for Clinicians software and hardware (CellScope, San Francisco, California). This device has been cleared by the Food and Drug Administration as an over-the-counter device.
The treating physician completed a physical examination using a microscope and documented the diagnosis and treatment. A second “blinded” neurotologist was given single images of bilateral TMs obtained from the SEO in addition to a brief patient summary (3-12 words), which included age, sex, significant medical history, and chief complaint ( Figure 1 ). Our primary end point was the classification of the TM as normal or abnormal by the “blinded” neurotologist, in addition to a diagnosis if pathology was detected. Secondary end points included patient-reported SEO comfort levels.
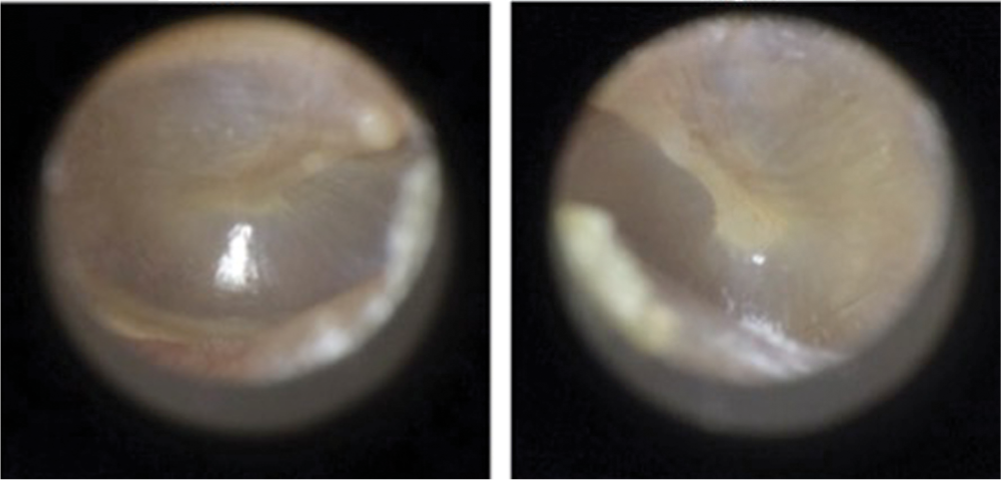
A screenshot of what was provided to the “blinded” physician providing smartphone-enabled otoscope (SEO) images of the left and right tympanic membrane and a short patient summary (upper left). These SEO images show a normal ear with no pathology.
Results
The prevalence of microscope-confirmed TM pathology in our study was 58% (33/57). The remaining 42% (24/57) of subjects did not exhibit detectable pathology upon microscopic examination by the treating neurotologist. The second “blinded” neurotologist correctly identified 100% (33/33) of pathology cases upon only seeing the SEO-acquired TM image supplemented by a brief patient summary ( Figure 2 and Figure 3 ). Of the 33 microscope-confirmed pathology cases, the diagnosis made by the blinded physician was identical to that made by the primary treating physician in 82% (27/33) of cases. These incorrectly diagnosed cases included chronic otitis media (n = 2), myringitis (n = 1), tympanosclerosis (n = 1), mild retraction (n = 1), and a pinpoint perforation (n =1). Correctly diagnosed pathology included chronic otitis media (n = 6), TM perforation or retraction (n = 12), cholesteatoma or glomus tympanicum (n = 3), exostoses (n = 2), eustachian tube dysfunction (n = 2), and postoperative changes (n = 2). The blinded clinician was able to correctly classify 96% (23/24) of normal cases as “no detectable pathology” ( Figure 1 ). In a single case, the blinded neurotologist incorrectly classified a microscope-confirmed “normal” TM as abnormal and diagnosed it as serous otitis media due to a line in the anterior superior quadrant that appeared similar to an air fluid level.

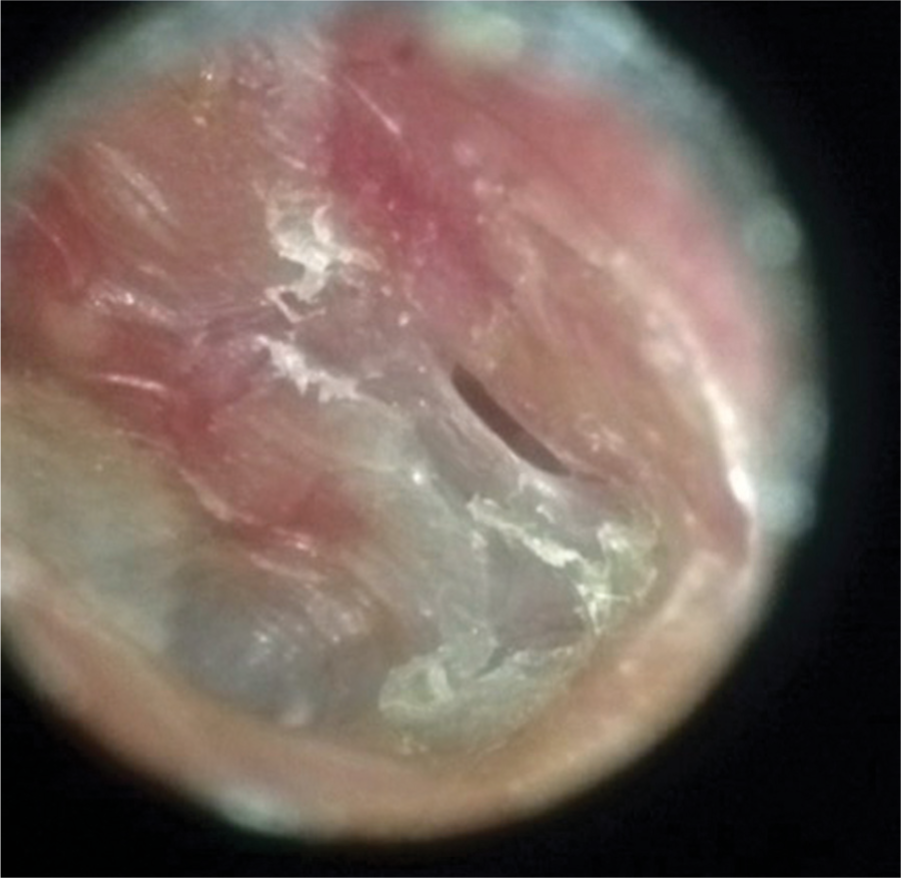
A smartphone-enabled otoscope image depicting cholesteatoma with chronic otitis media.
A smartphone-enabled otoscope image depicting a small slit tympanic membrane perforation.
Overall, the sensitivity of the blinded physician in correctly identifying pathology when pathology was present was 100% (33/33), while the specificity of identifying a normal TM was 96% (23/24). This yielded a positive predictive value of 97% (33/34) for abnormal TM identification and a negative predictive value of 100% (23/23) for normal TM classification ( Table 1 ). The false-positive rate was 4% (1/24), while the false-negative rate was 0% (0/33).
In assessing the patient experience, 93% (53/57) of patients selected the highest comfort level on the 5-point Likert scale subsequent to SEO operation by our research team members, usually consisting of a research assistant or medical student. It was determined that 88% (50/57) of patients felt that seeing the images was “very useful” in learning about their condition, which was the highest score on the Likert scale. In assessing patient comfort of remote or home-based SEO operation, 77% (44/57) felt “very comfortable” in capturing and sending secure images to their physician remotely, while 11% (6/58) did not feel comfortable.
Discussion
A single SEO image acquired by medical personnel of the TM provided to a remote new otologist was sensitive and specific in identification of abnormal and normal TMs, respectively. In addition to 100% sensitivity in abnormal TM detection using a SEO-acquired image, its specificity in recognizing pathology was 96% and false-positive rate was 4%, suggesting its efficacy as a screening tool. Furthermore, the 0% false-negative rate for patients with TM pathology highlights the diagnostic potential of the SEO. However, with a diagnostic accuracy of 82% when pathology was identified, the SEO appears to be more efficacious as a screening tool rather than a diagnostic one. This suggests that remote evaluation of a SEO-acquired TM image supplemented by brief history provided to a neurotologist can help determine if an in-office appointment is warranted.
In a screening capacity, one could foresee SEOs being loaned to parents to document and send images of their child’s TM to their physician for evaluation or SEO use in the primary care setting for digital evaluation with a remote otolaryngologist for consultation and referral. SEOs allow for multiple images of the right or left TM to be captured and stored in a cloud-database environment for virtual accessibility on a computer or mobile device. It also provides built-in video capture capabilities that may be used in assessing TM mobility by using the insufflator port attached to the device allowing for pneumatic otoscopy. This can provide further diagnostic details for the otolaryngologist looking at the pictures remotely.
Although video-based otoscopy has already been employed in a telemedicine capacity, the infrastructural hardware costs coupled with the necessity for professional equipment operation limit its utility. 9 SEOs overcome these limitations by their relative affordability and minimal training for proper device operation. Our data suggest that patients are receptive to SEO technology being presented to them on a familiar device such as an iPhone. Most patients felt comfortable in allowing a lower level provider such as a nurse, medical student, or undergraduate researcher to operate the SEO. The review of still images with the patient allowed for better education and counseling previously unattainable with traditional otoscopes or microscope. This was reflected in that the majority (93%) of patients felt very comfortable with SEO utilization by the provider, and 88% of patients felt that subsequently seeing the acquired image was helpful in their conceptualization of their medical condition.
Although SEOs have been previously demonstrated to be accurate and cost-effective mobile otoscopes in the diagnosis of otitis media, we think they could be particularly useful in telemedicine.10-12 In the field of dermatology, clinicians have used digital imaging to offer their expert opinion remotely. Within dermatology, a referring physician provides a digital image and patient history to a remote dermatologist for consultation. 13 This has helped decrease health care costs, 14 even allowing for reimbursements from major payers. 15 The adoption of this model is foreseeable within the field of otolaryngology to ultimately improve health care access by remote screening and patient triage, as well as possibly circumvent unnecessary outpatient appointments. Reimbursement for this service will occur once efficacy data have been demonstrated.
However, SEO operation by patients and family members for remote evaluation, or health care providers for digital consultation, bears certain limitations. First, although relatively simple, users must learn how to properly use the SEO to capture an adequate TM image. In our experience, the neurotologist experienced no challenges in capturing images. However, in 12 (21%) of cases, the practitioner removed cerumen when necessary prior to obtaining the image; this may prove to be challenging for patients who do not have the capability to do this at home or for primary care physicians who may not have the necessary equipment to perform cerumen debridement prior to obtaining an SEO image. Second, patients and family members may not recognize the TM and instead image the ear canal, reducing the efficacy of the device. In addition, users must have the proper equipment: a smartphone able to connect to the SEO, the SEO unit and mounting case, and disposable otoscope speculums. In particular, patients would be unable to take an image of their own TM. Thus, SEO deployment in a telemedicine setting requires properly training and equipping someone other than the patient on SEO operation. Despite these challenges, the simplicity of use and opportunities for digital image acquisition by a remote health care provider warrant further evaluation of SEO incorporating in the otology toolbox. This technology can eventually replace bulky video-otoscopy currently used in a telemedicine capacity due to SEO simplicity and ease of use. Future studies into the diagnostic potential of SEOs should evaluate a larger patient population with a wide range of pathologies.
Conclusion
SEO utilization was sensitive and specific in identifying both abnormal and normal ear exams, respectively, when a neurotologist was given a single image of the TM and a short patient history. These images can be easily acquired with minimal training by health care professionals and medical students given proper training on SEO operation. SEO-acquired high-resolution pictures of the TM can be useful in screening patients with otologic pathologies.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Paper presented at the American Neurotology Society; May 18-22, 2016; Chicago, Illinois.