
Abstract
Objective
Bell’s palsy is a cranial nerve VII dysfunction that renders the patient unable to control facial muscles from the affected side. Nevertheless, some patients have reported cutaneous changes in the paretic area. Therefore, cutaneous sensibility changes might be possible additional symptoms within the clinical presentation of this disorder. Accordingly, the aim of this research was to investigate the relationship between cutaneous sensibility and facial paralysis severity in these patients.
Study Design
Prospective longitudinal cohort study.
Settings
Tertiary care medical center.
Subjects and Methods
Twelve acute-onset Bell’s palsy patients were enrolled from March to September 2009. In addition, 12 sex- and age-matched healthy volunteers were tested. Cutaneous sensibility was evaluated with pressure threshold and 2-point discrimination at 6 areas of the face. Facial paralysis severity was evaluated with the House-Brackmann scale.
Results
Statistically significant correlations based on the Spearman’s test were found between facial paralysis severity and cutaneous sensitivity on forehead, eyelid, cheek, nose, and lip (P < .05). Additionally, significant differences based on the Student’s t test were observed between both sides of the face in 2-point discrimination on eyelid, cheek, and lip (P < .05) in Bell’s palsy patients but not in healthy subjects.
Conclusion
Such results suggest a possible relationship between the loss of motor control of the face and changes in facial sensory information processing. Such findings are worth further research about the neurophysiologic changes associated with the cutaneous sensibility disturbances of these patients.
Bell’s palsy is an idiopathic peripheral nerve (cranial nerve VII) dysfunction causing acute ipsilateral facial muscle weakness. 1 This disorder does not have a specific etiology2,3 but can be diagnosed from the appearance of specific signs and symptoms, blood chemistry tests, nerve conduction tests, cerebrospinal fluid investigations, or neuroimaging methods. 4 Herpes simplex virus has been suggested as its main cause,5-7 although there could be other causes, such as ischemia,8,9 autoimmunity,10-12 and bacterial infection. 13
In most of the medical literature, the disease has an incidence oscillating between 11 and 40 cases per 100,000 people annually, 14 mostly affecting persons between 15 and 45 years old.14,15 There is no tendency of paralysis to occur more frequently in one side of the face than in the other.16,17 Bilateral paralysis is unlikely to occur, since it is evident in only 0.3% to 2.0% of facial palsy cases. 18
Corticosteroids 19 and antiviral agents, 20 alone or in combination,21,22 have been used in the treatment of Bell’s palsy. Additional treatments include electrical stimulation, 23 surgery,24,25 physical therapy, 26 and acupuncture. 27 Complete recovery occurs in >70% of cases. 28 Most patients recover within 3 weeks, even if untreated, 1 although some cases demonstrate moderate or severe sequelae following their recovery.4,28,29
Recently, some evidence emerged regarding sensory features related with Bell’s palsy. Within this framework, cutaneous changes have been reported in the paretic area, such as numbness, 30 mild pain,28,31 hypoesthesia in reaction to a pinprick,30,32 variations in temperature sensation, 30 and increases in both vibration threshold and cutaneous pressure threshold at the same time as a reduction in static 2-point discrimination. 33 Experimental evidence in rats suggests that the lack of active facial movements impairs facial somatosensory information processing in the primary motor cortex. 34 Therefore, cutaneous sensibility changes are possible additional symptoms within the clinical presentation of idiopathic facial paralysis.
Accordingly, the current study tested the hypothesis that specific cutaneous sensitivity variations occur in patients with Bell’s palsy. To do so, the researchers tested for a correlation between cutaneous sensitivity measures and clinical characteristics, such as the time since the onset of the palsy and the individual’s House-Brackmann score. In addition, pressure threshold and 2-point discrimination measures in both facial sides of Bell’s palsy patients were compared with the same evaluations in matched healthy volunteers.
Methods
From March to September 2009, 52 patients affected with facial paralysis who reached the Fundación Cardioinfantil Instituto de Cardiología, the Hospital San José, or the Clínica Universidad de La Sabana in Bogotá, Colombia, were evaluated. Forty patients were excluded because their facial paralysis was associated with tumors, traumatic brain injury, central nervous system lesions, or other cranial nerve lesions. So, the experimental group included 12 acute-onset Bell’s palsy patients (<2 weeks since diagnosis; 7 women and 5 men; mean age = 33.42 years, SD = 17.85). Twelve sex- and age-matched healthy volunteers (mean age = 31.75 years, SD = 19.04) formed the control group. In the experimental group, 5 participants were prescribed with physical therapy in association with an oral pharmacologic treatment (prednisone, 50 mg/d; valacyclovir, 2000 mg/d) within 10 days of symptom onset; the remaining 7 received only physical therapy treatment during the same period. Control group participants did not receive any treatment.
All procedures agreed with the Declaration of Helsinki’s ethical principles. The Ethics Committee of the School of Medicine, Universidad Nacional de Colombia, approved the study. The participants provided informed consent, in agreement with Colombian state law 008430.
Patients’ sensitivity was evaluated weekly for 5 consecutive weeks, beginning at each patient’s recruitment. Healthy volunteers’ sensitivity was evaluated once. Cutaneous sensitivity was measured in 6 facial areas: forehead, eyelid, cheek, nose, lips, and jaw ( Figure 1 ).
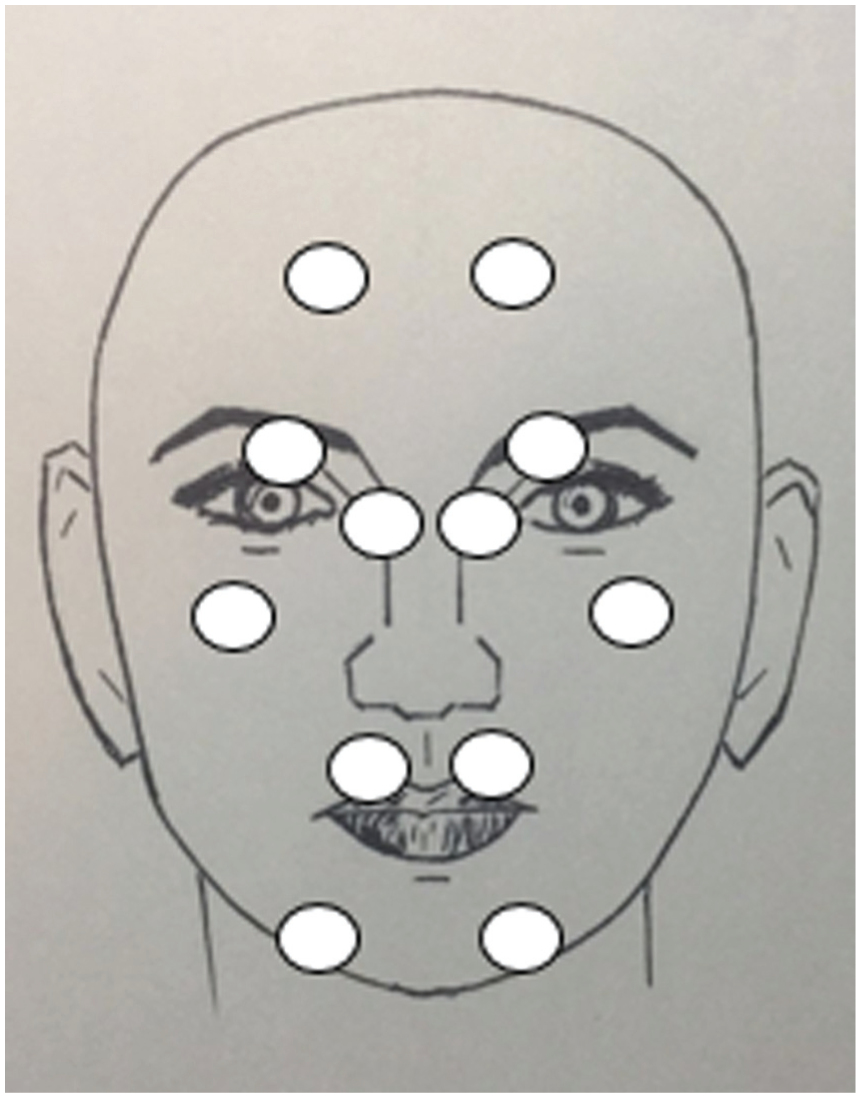
Facial areas where cutaneous sensitivity was evaluated. Open circles indicate the places used for evaluation: forehead, eyelid, cheek, nose, lip, and jaw. © Sara Suzunaga.
Facial paralysis severity was also assessed weekly with the House-Brackmann scale. This scale, recommended by the American Academy of Otolaryngology, 35 classifies the facial motor function into 6 grades, from normal symmetrical function in all areas (grade I) to total paralysis (grade VI). 36 In addition, this scale can monitor facial function status over time and assess the course of recovery and the effects of treatment. 37
Pressure threshold evaluation was conducted with a Von Frey esthesiometer (model 16013; Lafayette Instruments, Lafayette, Indiana). This esthesiometer includes 9 filaments that apply a nominal weight over the skin. The specific values for each filament can be seen in Table 1 .
Nominal Weight Value for Each Filament in the Von Frey Esthesiometer: Lafayette Instruments, Model 16013.
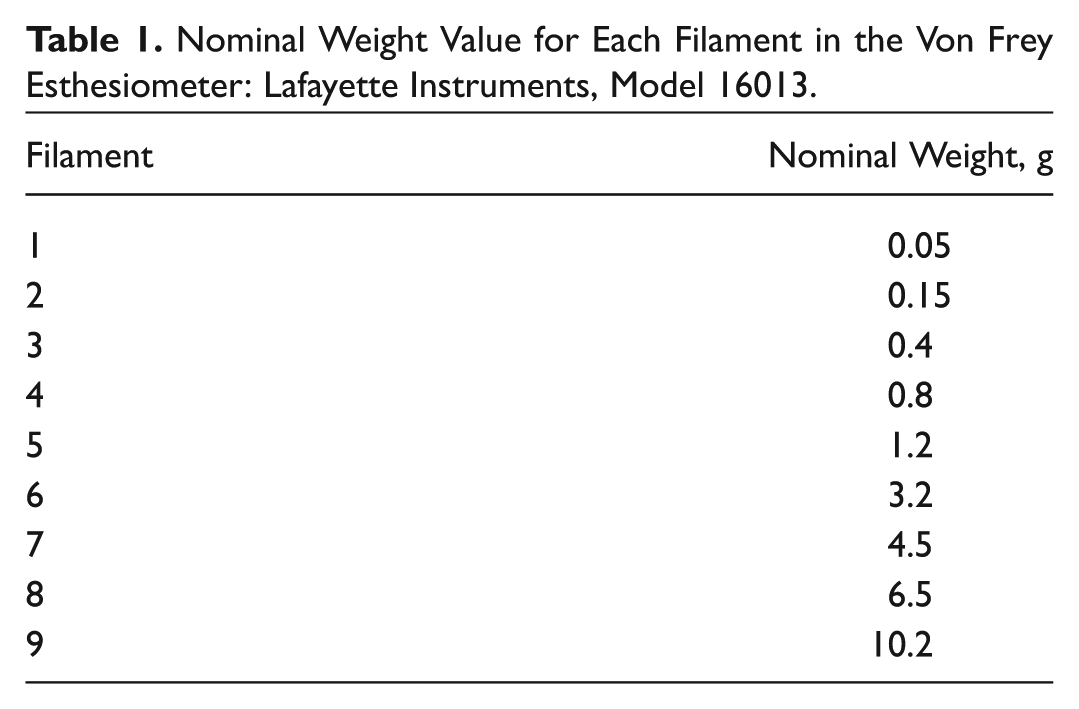
Pressure threshold was evaluated in 2 successive trials with filaments of either ascending or descending nominal weight. The score for each trial was the middle value between the nominal weights of the filaments used when pressure perception appeared (ascending) or disappeared (descending). An average of these 2 scores was used as the patient’s score for a facial area in a given week. This procedure was based on the method of limits for determining absolute thresholds proposed by Fechner (as cited in Goldstein 38 ).
A 2-point esthesiometer (model 16011; Lafayette Instruments) was used to assess 2-point discrimination. For this evaluation, a similar procedure was performed, also based on the above-mentioned method of limits. Ascending and descending trials were done with 3-mm increments or decrements in a range from 0 to 24 mm. A middle value between the 2-point distances was used as each trial score when point perception shifted from 1 to 2 (or vice versa). An average of the ascending and descending trial scores was used as a patient’s score for a facial area in a given week.
To assess the level of cutaneous sensitivity disturbance in Bell’s palsy patients, pressure threshold and 2-point discrimination in the affected side were each expressed as a percentage change with respect to the value obtained in the nonaffected side. Thus, with the cutaneous sensibility measure in each facial region of the nonaffected side as a reference (ie, 100%), the corresponding magnitude of the region in the affected side was expressed as a percentage of it. A value >100% should be interpreted as an increase in the sensory measure in the affected side and, consequently, as a lesser level of cutaneous sensitivity.
Spearman’s rank correlation coefficient between facial paralysis severity and the time elapsed since the onset of the illness or the level of cutaneous sensitivity disturbance was determined to assess relationships between such variables. Rank correlation took into account the ordinal scale of paralysis severity.
The differences in cutaneous sensitivity between both sides of the face in Bell’s palsy patients were analyzed with a Student’s t test; however, pressure threshold in both forehead and nose was compared with a Wilcoxon signed-rank test due to uneven variances, as evidenced by Levene’s test (P = .022 and .003, respectively). In healthy controls, such analysis was conducted with a Wilcoxon signed-rank test for pressure threshold in jaw (P = .004, Levene’s test) and for 2-point discrimination in lips (P = .018, Levene’s test); for the remainder of the cutaneous sensibility assessments in this group, Student’s t test was used.
The statistical analyses were performed with the corresponding modules of SPSS 21.0 (IBM Corp, Chicago, Illinois), with a significance level set at P ≤ .05.
Results
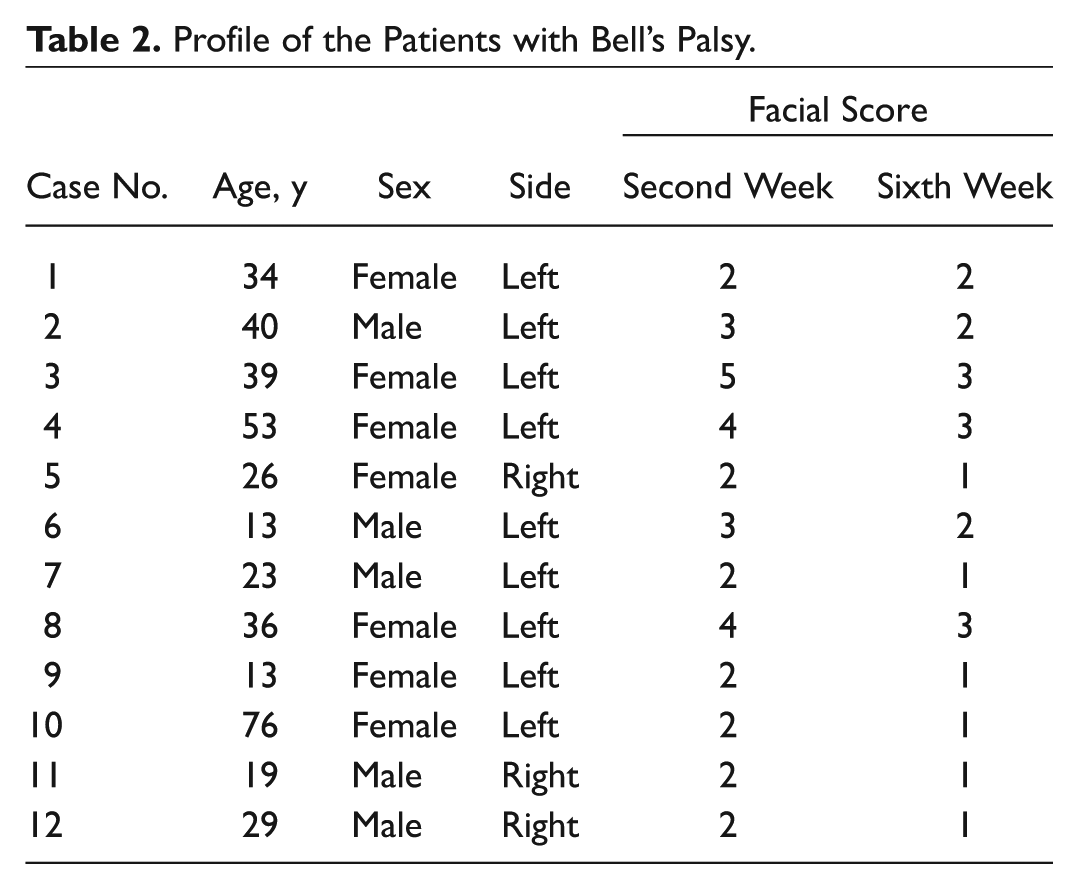
Demographic data are summarized in Table 2 . Nine patients had left-sided Bell’s palsy, and 3 presented a right-sided palsy. Seven patients were female, and 5 were male. At the beginning of the study, facial paralysis evaluation showed 7 patients scoring II (slight paralysis) on the House-Brackmann scale; 2 patients, III (moderate paralysis); 2 patients, IV (moderately severe paralysis); and 1 patient, V (severe paralysis). The healthy control group consisted of 12 sex- and age-matched participants.
Profile of the Patients with Bell’s Palsy.
Based on Spearman’s rank correlation coefficient, a significant decrease in the House-Brackmann score was observed along the 5 weeks following the onset of the paralysis (r = −0.361, P = .005; Figure 2 ).
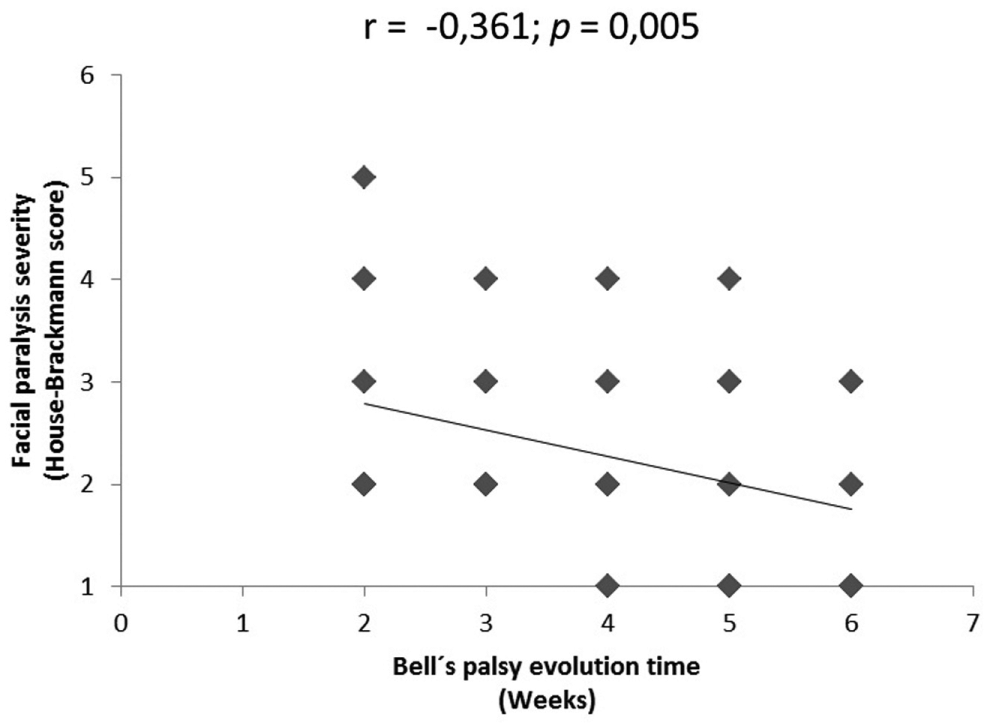
Facial paralysis severity as a function of Bell’s palsy evolution time, based on Spearman’s rank correlation test. Diamonds represent the data for each patient; the solid line represents the best linear regression fit for the whole data.
There were statistically significant correlations between House-Brackmann score and pressure threshold disturbance at the eyelid (r = 0.396, P = .002), cheek (r = 0.454, P < .001), and nose (r = 0.310, P = .016). There were also significant correlations between House-Brackmann score and 2-point discrimination impairment at the forehead (r = 0.368, P = .004), eyelid (r = 0.284, P = .028), cheek (r = 0.360, P = .005), and lip (r = 0.255, P = .049). The more severe the facial paralysis, the more intense the alteration in sensorial measurements ( Table 3 ).
Spearman’s Correlation Values between Cutaneous Sensitivity and Facial Paralysis Severity.
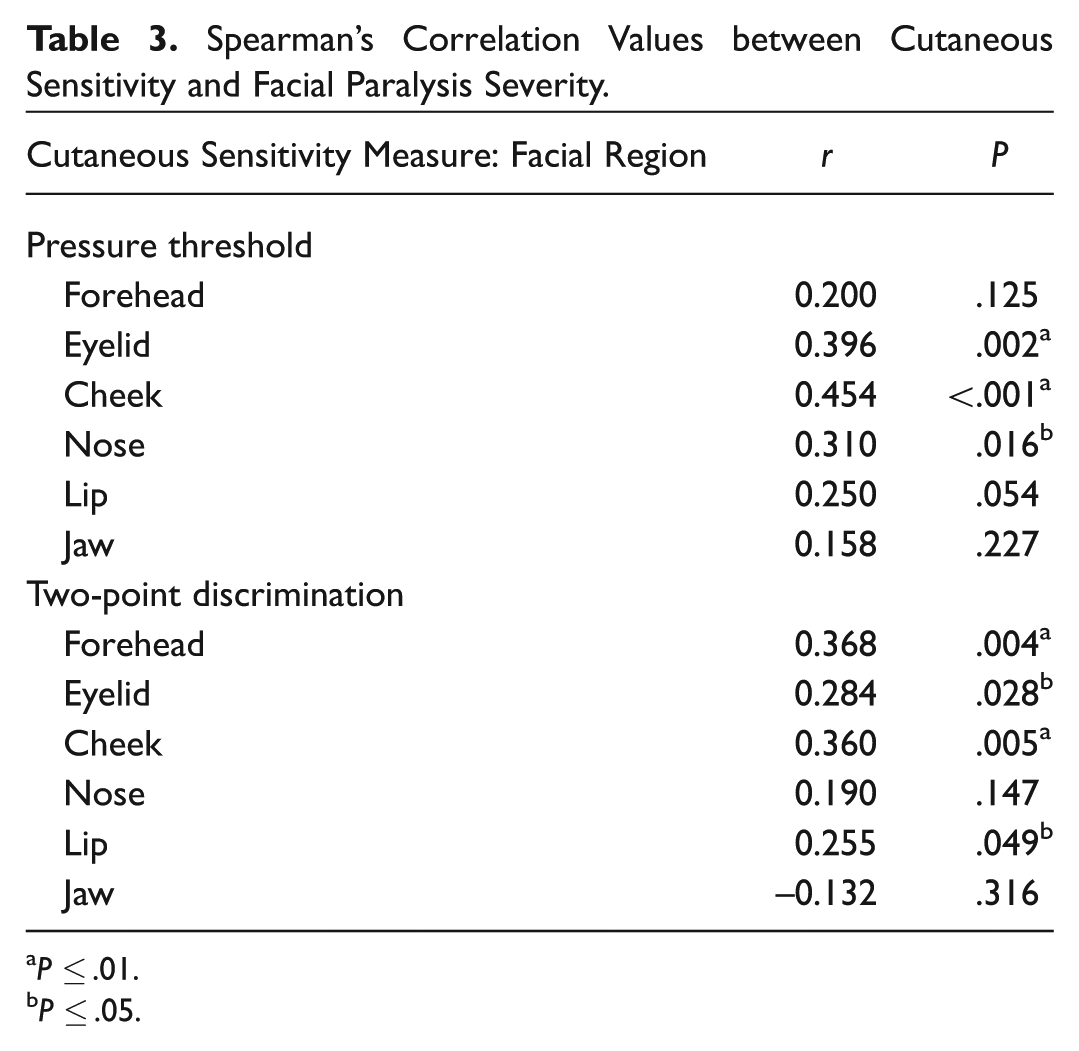
P ≤ .01.
P ≤ .05.
Globally, there were no significant side-to-side differences in pressure threshold for either Bell’s palsy patients (affected vs unaffected) or healthy controls (left vs right). However, with respect to 2-point discrimination, there was statistically significant impairment in the affected side of Bell’s patients at the eyelid (t = 2.543, P = .014), cheek (t = 2.060, P = .044), and lip (t = 2.696, P = .009); in contrast, there were no significant side-to-side differences in any of the evaluated facial areas in healthy volunteers ( Table 4 ).
Side-to-side Comparison in 2-Point Discrimination: Bell’s Palsy Patients and Healthy Volunteers.
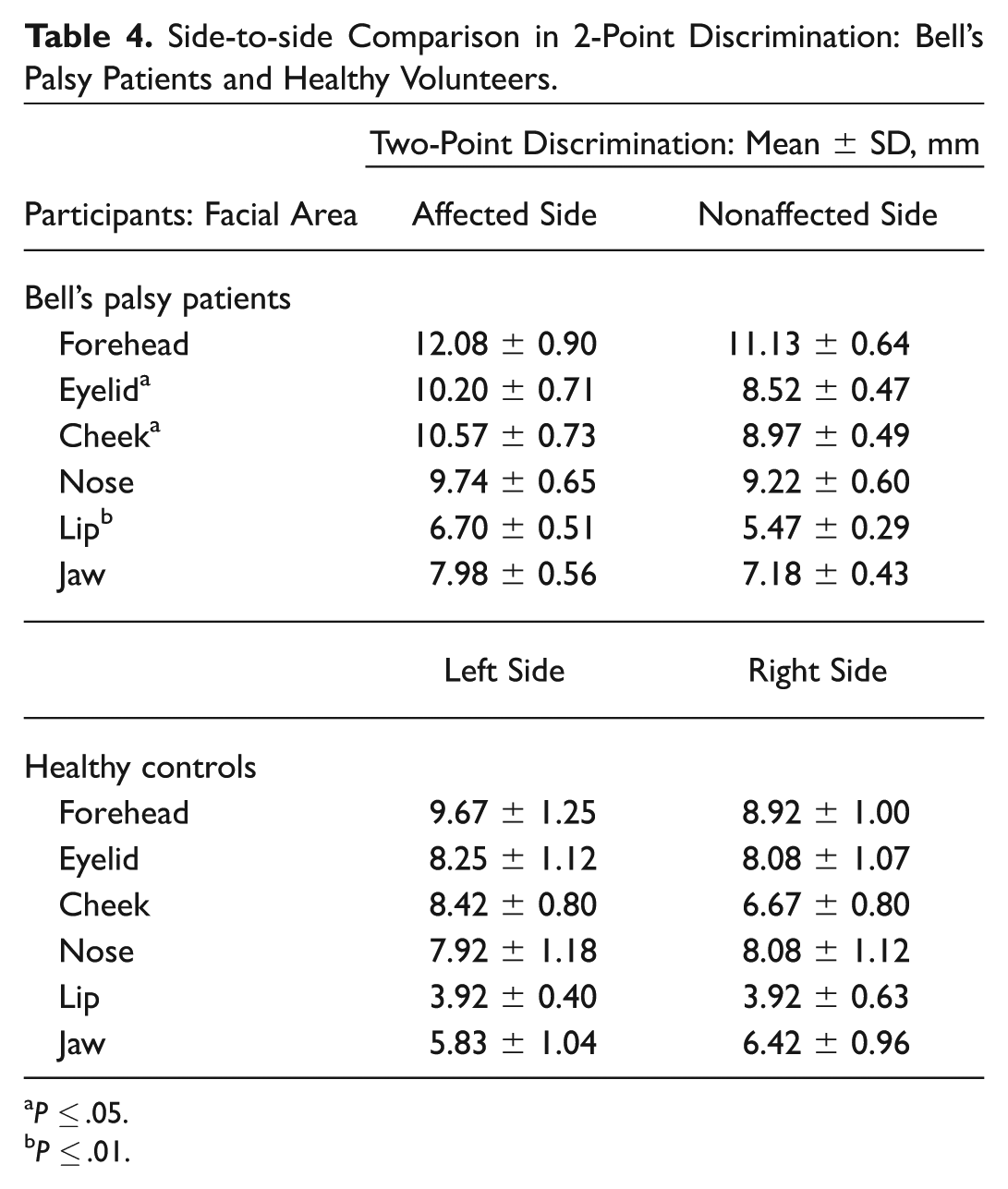
P ≤ .05.
P ≤ .01.
Discussion
The main aim of this study was to investigate the relationship between cutaneous sensibility and facial paralysis severity in Bell’s palsy patients. In this regard, pressure thresholds and 2-point discrimination measures were obtained in both facial sides of Bell’s palsy patients and later correlated with the House-Brackmann score. These sensorial data were also compared with the same values from matched healthy volunteers.
Nine patients had the left side of the face affected, while only 3 had the right side affected, which does not correspond with the equal distribution described in some studies. 4 Severity of facial paralysis with the House-Brackmann scale diminished significantly along the observation interval. As a result, a significant recovery occurred between the second and fifth weeks since the onset of symptoms. This result is consistent with descriptions of the duration of this illness, which estimate that time of recovery should be between 2 and 6 weeks in most cases. 39
A later analysis showed statistically significant correlations between pressure threshold disturbance and House-Brackmann assessment of the eyelid, cheek, and nose and between 2-point discrimination and House-Brackmann score on the forehead, eyelid, cheek, and lip. Thus, these sensory perturbations’ reduction paralleled the decrease in facial paralysis severity. This can be due to the close relationship between facial movement and somatosensory information processing mentioned above. However, since the above-mentioned correlations are not strong enough, it should be inferred that there are additional factors determining cutaneous sensibility disturbances other than the motor impairment. In addition, there were no significant differences in cutaneous pressure threshold identified across both sides of the face among Bell’s palsy patients and the healthy control group. Since this latter finding runs contrary to the changes described for this measure in patients with unilateral facial paresis, 33 this issue deserves further research.
Moreover, 2-point discrimination threshold impairment occurred on the affected side of Bell’s palsy patients in the eyelid, cheek, and lip. This finding is consistent with other observations in such patients, 33 which suggests an impairment in the processing of this threshold associated with a decrease in facial movement. Nevertheless, similar to the homologous pressure threshold analysis, there was no similar reduction in the remainder of the evaluated facial regions, which also justifies further research on the tactile changes occurring alongside diminished motor control of the face.
In this vein, changes in sensory information processing in the contralateral vibrissal primary motor cortex occurred after peripheral facial nerve lesions in animal models; such disturbance may be due to vibrissal paralysis–induced changes in somatosensory input. Thus, the variation in this sensory input would produce a reorganization of the dendritic trees in the vibrissal primary motor cortex and the other cortical areas; this sensory unbalance may also occur in patients with facial nerve paralysis irrespective of the underlying etiology. 34 Such paralysis-induced reorganization has to be studied in other sensorimotor cortical and subcortical regions to understand the underpinnings of the correlation between cutaneous sensibility changes and facial paralysis severity and its inhomogeneous distribution in the present sample. However, the observed changes would be a possible explanation for some functional sequelae in these patients. 40
Conclusion
Statistically significant correlations were found between facial paralysis severity and cutaneous sensitivity on forehead, eyelid, cheek, nose, and lip. Additionally, changes in 2-point discrimination among Bell’s palsy patients were observed on the eyelid, cheek, and lip. These findings may be due, at least partially, to a defective processing of facial somatosensory information associated with impaired facial movement. There was also no significant correlation between facial paralysis severity and cutaneous sensitivity on the jaw; in addition, statistically significant differences in pressure threshold between affected and nonaffected sides of Bell’s palsy patients were not observed.
Although some changes in sensory information processing were observed in the vibrissal primary motor cortex after contralateral peripheral facial nerve lesion in rats, the neurophysiologic changes underlying the cutaneous sensibility disturbances of Bell’s palsy patients are not yet completely understood. Therefore, further research is needed on this subject.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We thank the staff at the Fundación Cardioinfantil Instituto de Cardiología, Hospital San José, and the Clínica Universidad de La Sabana for their assistance with the recruitment of participants for the study. We also thank Dr Jorge Herrera Ariza, Dr José Carreño, Dr Mónica Rincón, Dr Yisel Estrada, Fabio Motta, Aura Hernández, Sandra Farías, Henry Ayala, and Katherine Andrade for their assistance with the recruitment and scheduling of participants. Additionally, we acknowledge the contribution of Sara Suzunaga, who designed 1 of the figures used in this study.
No sponsorships or competing interests have been disclosed for this article.