
Abstract
Objective
Although thyroglossal duct cysts (TGDCs) are relatively common, malignancies within these lesions are infrequent. As a result, there are no large-scale series describing clinical characteristics. Our objectives were to perform a systematic review of the literature evaluating patient demographics, pathology, management, and prognosis of these patients.
Data Sources
PubMed, Embase, Cochrane reviews, and Google Scholar were searched for relevant articles. Articles meeting inclusion criteria were reviewed for data detailing epidemiology, treatment, and outcomes.
Review Methods
Inclusion criteria included English-language articles with original reports on human subjects. Two investigators independently reviewed all articles for the data collected, including epidemiology, treatment, and outcomes.
Results
Ninety-eight articles comprising 164 patients were included in the final analysis. The mean age at presentation was 39.5 years (9-83 years); 68.3% of patients were female. In total, 73.3% of cases were found on final pathologic analysis. The most common pathology was papillary cancer (92.1%). Of the patients, 98.9% underwent a Sistrunk procedure and 61.0% underwent total thyroidectomy. There was a 4.3% recurrence rate with a mean time to recurrence of 42.1 months from initial treatment. One patient died of TGDC carcinoma, while all other patients were disease free at the time of last follow-up (mean follow-up was 46.1 months).
Conclusion
TGDC carcinoma is typically diagnosed on final pathology. While management encompasses a Sistrunk procedure, further consideration should be given to thyroidectomy among patients ≥45 years of age and individuals with aggressive disease. TGDC carcinoma harbors an exceedingly low rate of mortality.
Representing an abnormal remnant of thyroid development, thyroglossal duct cysts (TGDCs) can form anywhere along the thyroid’s route of migration but are most commonly found inferior to the body of the hyoid bone. Developed nearly 100 years ago, the Sistrunk procedure is the most common surgery performed to address TGDCs. 1 Approximately 1% develop a carcinoma of some form, with the most common type being papillary carcinoma.2,3
The literature describing TGDC carcinoma comprises largely case reports and small series, with the largest cohort reporting findings from fewer than 25 patients. Consequently, providing patients with adequate prognostic information and detailing treatment guidelines represents a difficult endeavor. 4 Although TGDC carcinoma is thought to harbor excellent survival, there are minimal data on long-term outcomes of patients with TGDC carcinoma. 5 The aim of this systematic review was to analyze the epidemiology, treatment options, and outcomes of patients with TGDC carcinoma. To our knowledge, this is the only systematic review of TGDC carcinoma.
Methods
A systematic review was conducted based on principles set forth in the Preferred Reporting Systems for Systematic Reviews and Meta-Analysis (PRISMA) ( Figure 1 ). A PICOS (population, intervention, comparison, outcome, and study design) approach was used for this study. The target population was all patients with TGDC malignancies, and the surgical interventions performed were analyzed. The main outcomes analyzed were overall survival and recurrence rates.
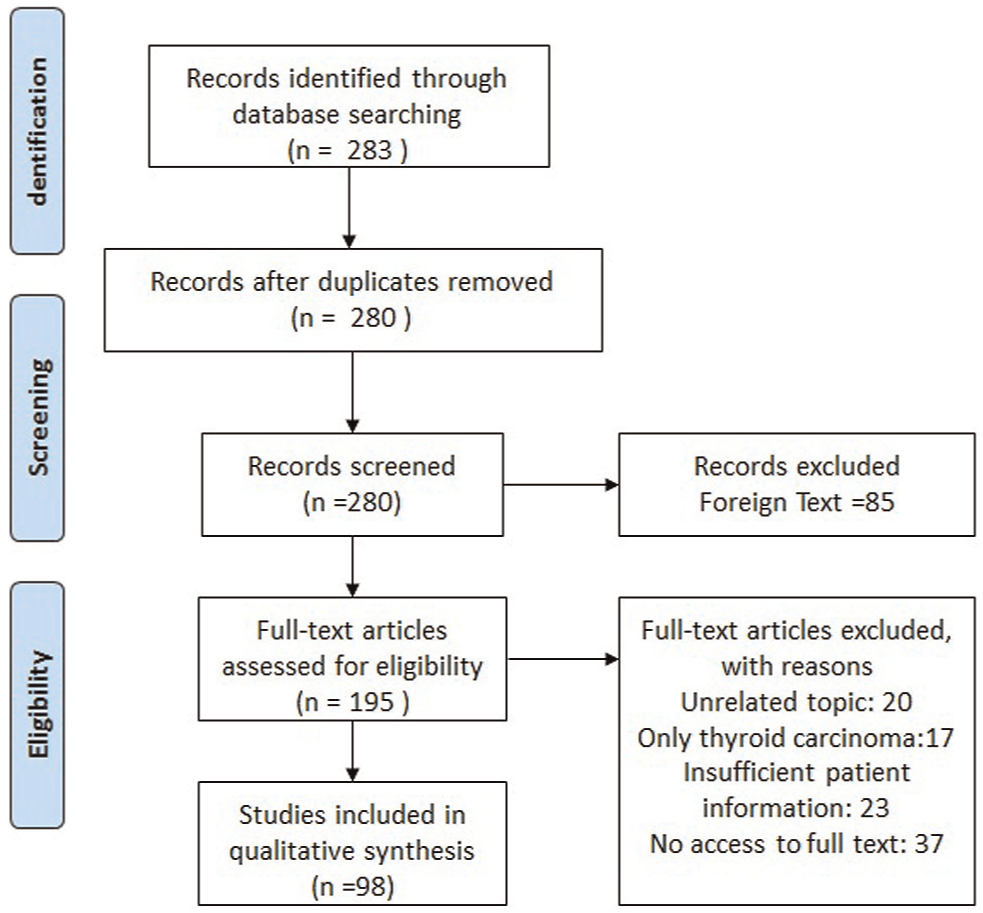
Article selection process based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
The PubMed, Medline, Google Scholar, Embase, and the Cochrane Database for Systematic Reviews were reviewed for articles related to TGDC carcinoma. To maximize retrieval of relevant articles, specific combinations of key words were used to query Medline. The terms were entered as follows: thyroglossal duct cyst carcinoma, papillary carcinoma and thyroglossal duct, thyroglossal duct cyst malignancy, thyroglossal duct cyst and cancer, and thyroid cancer and thyroglossal duct cyst. The title was initially reviewed for all studies retrieved, then the abstract. Studies that were pertinent were downloaded, and the entire paper was reviewed along with the references to ensure all relevant studies were included.
Only studies with primary data for patients who had TGDC carcinomas were included. Studies were excluded if they were not in the English language, if they were about nonhuman subjects, or if they had insufficient individual patient information. Two independent reviewers extracted the data, and any discrepancies were reviewed and discussed. Demographic information was collected, including age at diagnosis and sex. Clinical data collected included presenting symptoms, method of diagnosis, final pathologic diagnosis, and treatment performed (Sistrunk, total thyroidectomy, central neck dissection [CND], lateral neck dissection [LND], radioactive iodine [RAI], or external beam radiation). Outcomes collected included time to last follow-up, recurrence, and final pathology of the different treatment methods.
Results
Our literature review yielded 283 abstracts. No prior systematic reviews or meta-analyses were identified. Ninety-eight articles met the inclusion criteria and were included in the final analysis with a total population of 164 patients. Eighty-one case reports and 17 case series were included.4-101 The largest case series included 18 patients, and the studies that we evaluated spanned from 1986 to 2016. The mean age of presentation for the patients analyzed was 39.5 years (range, 9-83 years). In total, 31.7% of the patients were male and 68.3% were female ( Table 1 ).
Summary of the Collective Patients.
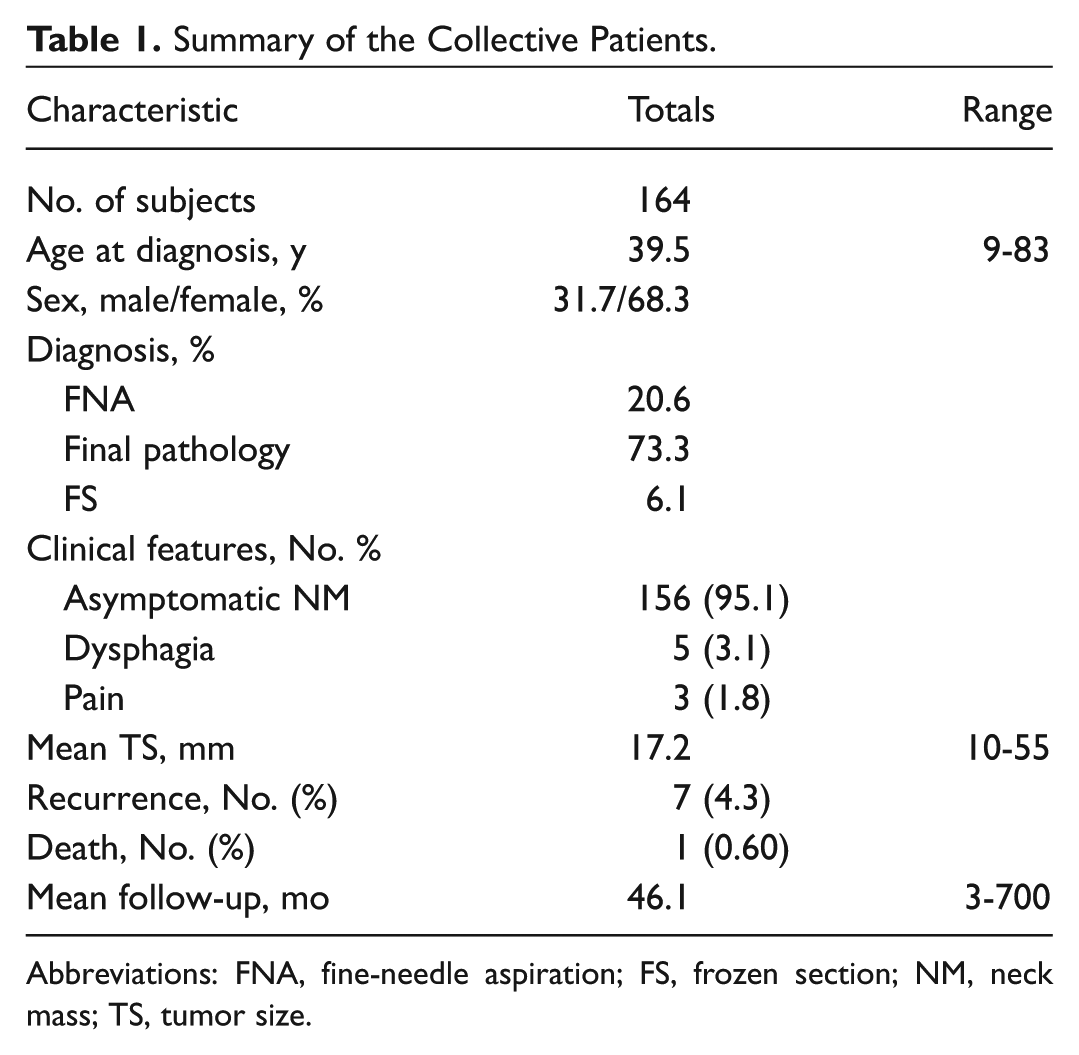
Abbreviations: FNA, fine-needle aspiration; FS, frozen section; NM, neck mass; TS, tumor size.
Clinically, 95.1% of patients presented with an asymptomatic neck mass, 1.8% endorsed pain, and 3.1% reported dysphagia. The imaging techniques commonly used to evaluate the neck mass included either computed tomography (CT) or ultrasound. The diagnosis of TGDC carcinoma was most commonly made on final pathologic analysis (73.3% of cases). In 20.6% of cases, the diagnoses were made based on fine-needle aspiration (FNA) findings. A total of 129 (78.6%) patients had an FNA during their preoperative workup, and it was positive for malignant cells in 23.6% of those patients. Of the cases, 6.1% were diagnosed based on frozen section. The mean tumor size was 17.2 mm. In total, 151 (92.1%) patients had papillary adenocarcinoma; Table 2 lists the other pathologic diagnoses.
Pathology of Thyroglossal Duct Cyst Carcinomas.
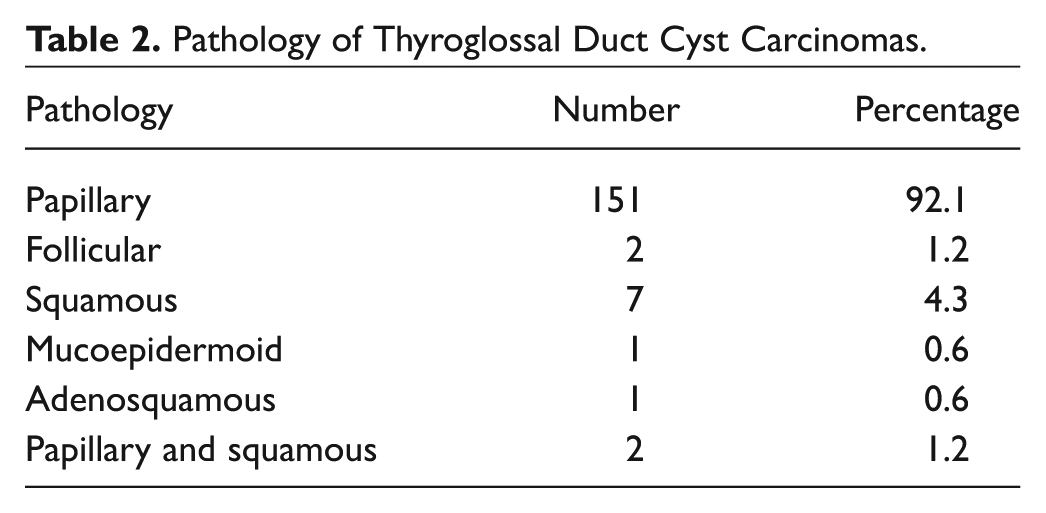
Figure 2 illustrates the various interventions that were performed. Of the patients, 98.9% had a Sistrunk procedure. Surgeries that involved resection of the central hyoid and tongue tissue were considered Sistrunk procedures. The second most common procedure performed was a total thyroidectomy at 61.0%; 34.5% had a lateral neck dissection and 26.4% had a central neck dissection. Table 3 illustrates the frequency of the most common treatment combinations and their outcomes. The most common treatment combinations were Sistrunk cyst excision followed by a Sistrunk and total thyroidectomy at 36.7% and 27.2%, respectively. Seven patients received external beam radiation as part of their treatment regimen. All but 1 patient treated with this modality had squamous cell carcinoma or mucoepidermoid carcinoma ( Table 4 ). That patient had papillary thyroid cancer with squamous metaplasia. None of the patients treated with radiation developed a recurrence.
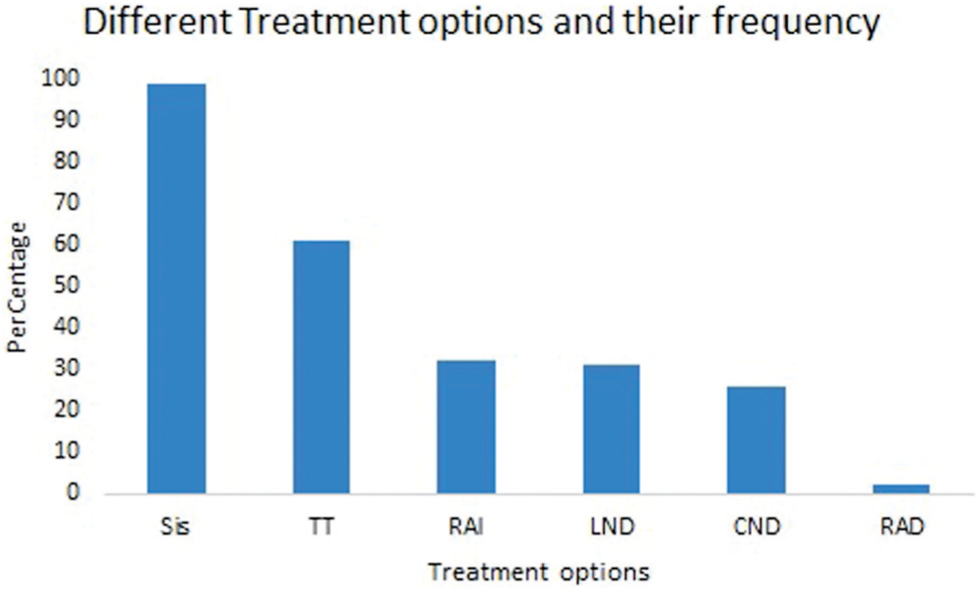
Prevalence of the different treatment modalities. CND, central neck dissection; LND, lateral neck dissection; RAD, external beam radiation therapy; RAI, radioactive iodine ablation; Sis, Sistrunk; TT, total thyroidectomy.
Summary of the Clinical and Pathologic Outcomes by Treatment Performed. a
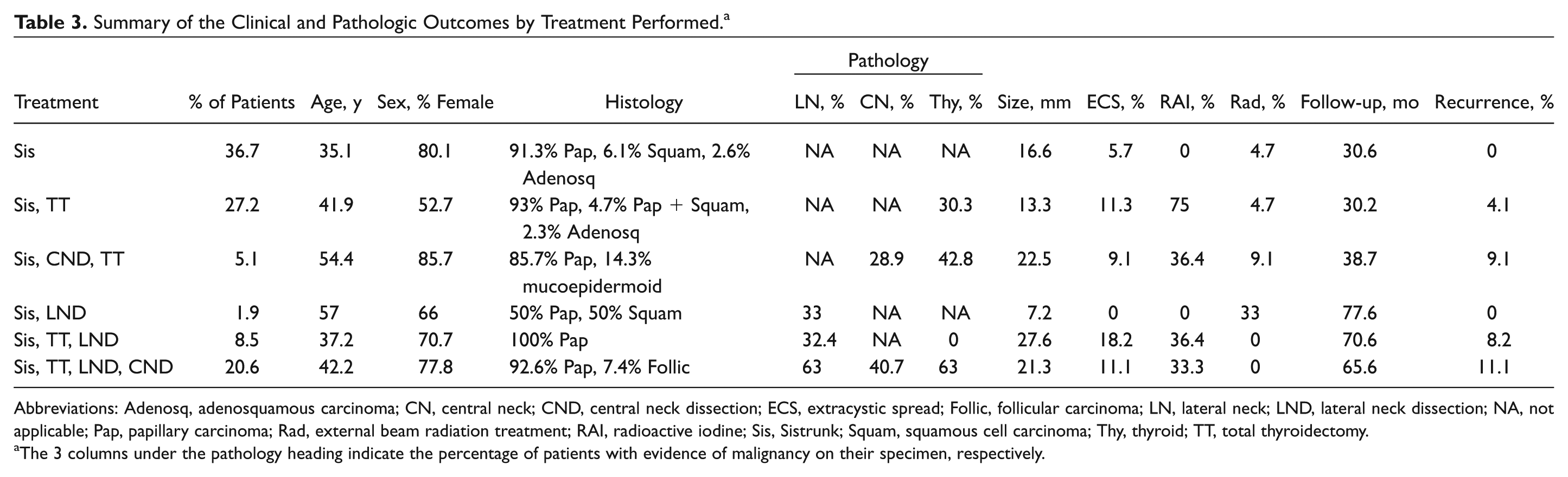
Abbreviations: Adenosq, adenosquamous carcinoma; CN, central neck; CND, central neck dissection; ECS, extracystic spread; Follic, follicular carcinoma; LN, lateral neck; LND, lateral neck dissection; NA, not applicable; Pap, papillary carcinoma; Rad, external beam radiation treatment; RAI, radioactive iodine; Sis, Sistrunk; Squam, squamous cell carcinoma; Thy, thyroid; TT, total thyroidectomy.
The 3 columns under the pathology heading indicate the percentage of patients with evidence of malignancy on their specimen, respectively.
Detailed Information on the 7 Patients Who Received External Beam Radiation as Part of Their Treatment.
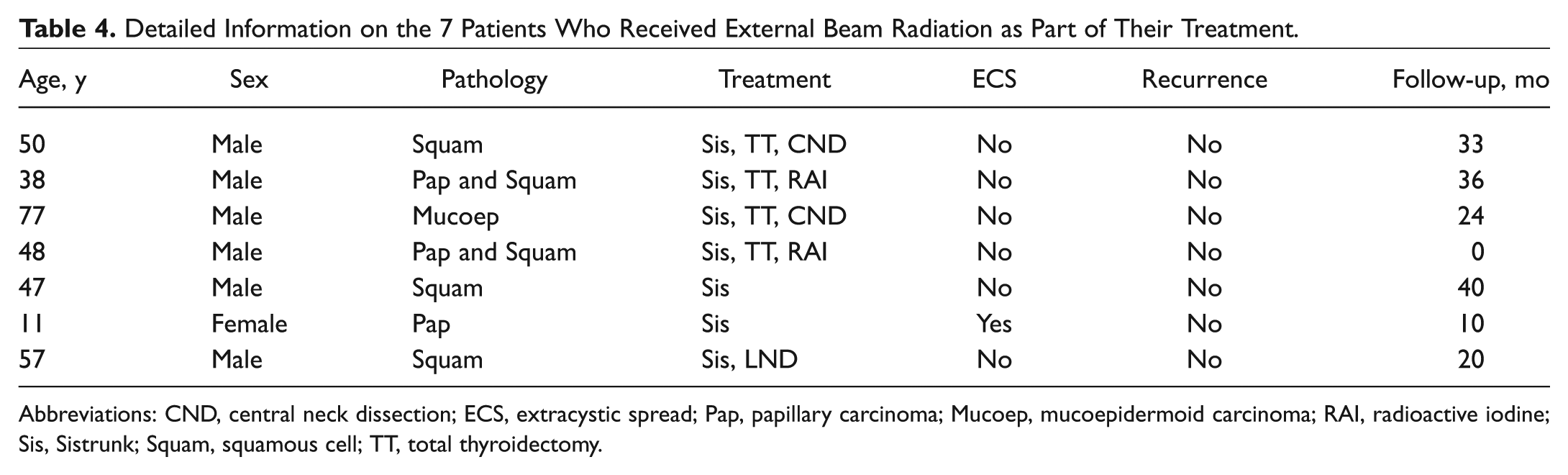
Abbreviations: CND, central neck dissection; ECS, extracystic spread; Pap, papillary carcinoma; Mucoep, mucoepidermoid carcinoma; RAI, radioactive iodine; Sis, Sistrunk; Squam, squamous cell; TT, total thyroidectomy.
Seven (4.3%) patients developed a recurrence following their initial treatment ( Table 5 ). The mean time to developing a recurrence was 42.1 months following initial treatment. Four (57.1%) patients were female, and the mean age at diagnosis was 41.4 years. All of these patients had papillary cancer. There was no significant difference in age between patients who had a recurrence compared with the rest of the subjects (P = .45). The most common site of recurrence was the lateral neck at 3 (42.9%). One patient died as a result of his disease.
Detailed Information on Patients Who Developed Recurrences.
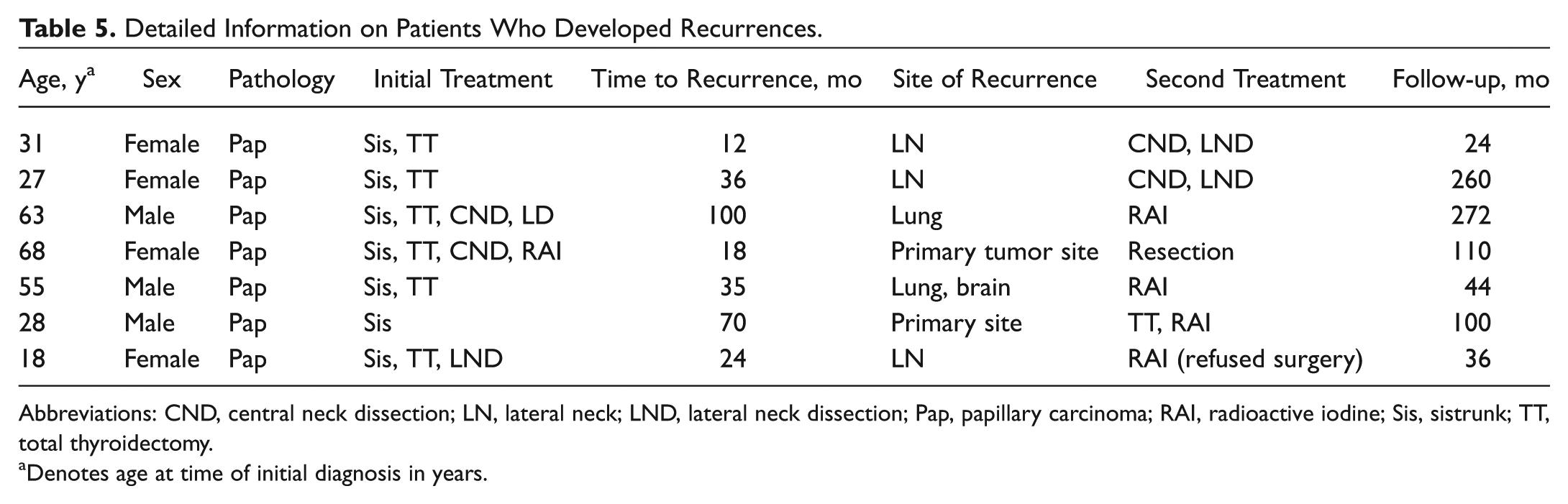
Abbreviations: CND, central neck dissection; LN, lateral neck; LND, lateral neck dissection; Pap, papillary carcinoma; RAI, radioactive iodine; Sis, sistrunk; TT, total thyroidectomy.
Denotes age at time of initial diagnosis in years.
Discussion
Malignant changes in TGDCs are rare and involve less than 1% of TGDCs.102,103 TGDC typically presents in a pediatric population, and most cases present before age 30 years; contrastingly, our results demonstrated that TGDC carcinoma tends to present later in life, with a mean age of 39.5 years.104,105 Furthermore, thyroid cancers are 2.9 times more common in females than males, and the findings of this study show that this predilection also extends to TGDC carcinoma. Patients with TGDC carcinoma were more likely to be female (68.3%). No molecular factors have been established to explain this difference. 106
In our series, 95.1% of patients with TGDC carcinoma presented with an asymptomatic neck mass. The incidence of associated symptoms was low, with 1.8% of patients endorsing a history of pain and 3.1% stating that they had dysphagia. TGDC commonly presents as well as a midline asymptomatic neck mass. Some authors have suggested that the presence of rapid expansion, a fixed cyst, and presence of pain are indicative of a TGDC carcinoma. 107 In contrast, our results indicate that differentiating a benign TGDC from one that has a malignancy is very difficult based on clinical findings.
Diagnosis of TGDC Carcinoma
Overall, 73.3% of TGDC carcinomas were diagnosed as incidental findings on final pathologic analysis, and another 20.6% were diagnosed preoperatively based on FNA analysis. The workup and evaluation of a TGDC often involve clinical findings in conjunction with imaging, either a CT scan or ultrasound. Some findings on ultrasound, such as a mural mass with associated microcalcifications, are suggestive of TGDC carcinoma. 108 CT scans can also demonstrate a mural mass with calcifications or a mass with enhancement. 109 Imaging is critical preoperatively to ensure the presence of a thyroid gland in the neck. There is debate over the utility of FNA biopsy preoperatively. It is a simple procedure and can be valuable for preoperative counseling and detecting malignant processes. 110 The sensitivity of FNA biopsy for TGDC carcinoma has been reported at 56% to 62% with a positive predictive value of 69%.18,111 The decreased sensitivity could be secondary to dilution of the aspirate with cystic fluid contents. As FNA has a controversial role preoperatively, it does not appear to be cost-effective or clinically appropriate to perform an FNA on every patient with a TGDC, including children. In addition, an FNA does not rule out the presence of a malignancy, especially if the clinical suspicion is high. On the other hand, preoperative knowledge of a carcinoma could save the patient another trip to the operating room, since often patients are taken back for a total thyroidectomy following a diagnosis of TGDC carcinoma. In our series, most diagnoses were made as incidental findings on final pathology. Hence, the possibility of finding a carcinoma needs to be discussed with patients preoperatively.
Pathologic Diagnoses
The most common pathologic diagnoses were papillary cancer at 92.1%, followed by squamous cell carcinoma at 4.3%. Other studies have reported that papillary thyroid cancer is the most common diagnosis at 75% to 85%, with mixed papillary and follicular second. Our results show a very high percentage of papillary cancer followed by squamous cell carcinoma. 112 Squamous cell carcinoma is hypothesized to originate from cyst lining and tends to have a worse prognosis. 113
Recurrence Rates/Outcomes
The mean follow-up time following surgical management of TGDC carcinoma was 46.1 months. Seven patients (4.3%) had a recurrence. There was no significant difference in age between patients who had a recurrence compared with the rest of the subjects (P = .45). The most common site of recurrence was the lymph node bed, with 42.9% of patients developing a recurrence in that location. Notably, none of these patients had prior lymph node dissections. The mean time to recurrence was 42.1 months. Interestingly, all patients with recurrences had papillary cancer. It was difficult to compare outcomes by pathologic diagnosis given the small sample size for nonpapillary cancer. One patient died as a result of his disease; this patient was a 55-year-old man with a diagnosis of papillary cancer treated with a Sistrunk and total thyroidectomy who had multiple distant metastases in the lung and brain 35 months following initial diagnosis that did not respond to radioactive iodine therapy. He was the only patient in the study with distant metastasis.
Management
The extent of surgical management of TGDC carcinoma remains controversial. In all instances, a Sistrunk procedure should be performed to excise the lesion. Findings from Patel et al 114 demonstrated that the extent of the original surgical procedure was the only significant predictor of outcomes, and the addition of a total thyroidectomy did not significantly affect outcomes. The next step in management pertains to the thyroid. The prevailing theory currently is that papillary carcinomas arise from the TGDC de novo and are not metastatic from the thyroid gland. Evidence that supports this theory includes the fact that there are no reports of TGDC medullary carcinoma. In our analysis, 61.0% of patients had a total thyroidectomy, and of these patients, 23.4% had a tumor in their thyroid gland. Recent series have estimated that the incidence of thyroid gland involvement ranges from 33% to 45%, in concordance with our data ( Table 3 ). This is not necessarily notable as it lies within the 30% to 35% rate of incidental thyroid carcinoma diagnosed on autopsy.115,116 The other reason for performing a total thyroidectomy is to facilitate radioactive iodine ablation. In our study, 32.2% of patients received radioactive iodine ablation. Several authors recommend a total thyroidectomy as a routine follow-up procedure for patients with TGDC carcinoma.103,117,118 The benefits of this are questionable given the associated risks with total thyroidectomy, including a 1% to 2% incidence of recurrent laryngeal nerve injury. In general, patients younger than 45 years without metastatic spread to the lymph nodes, no exposure to radiation, no concerning radiologic features, and with negative margins should not undergo a routine total thyroidectomy following TGDC carcinoma excision. 119 The low incidence of malignancy noted in the thyroid specimen (23.4%) does not justify the added risk of surgery. In patients with advanced disease, including spread to lymph nodes or extracapsular invasion, a thyroidectomy may be indicated to permit radioactive iodine ablation. Patients with TGDC carcinoma should undergo a thyroid ultrasound if they did not have one preoperatively to evaluate the thyroid for any nodules, and these can be managed according to established guidelines.
In our study, 31.0% of patients had a lateral neck dissection, and 52.6% of these patients had positive nodes. Overall, 16.4% of patients had positive lateral neck nodes; other studies have reported a similar incidence ranging from 10% to 15% ( Table 3 ). Unlike the thyroid gland, the lymphatics that drain the TGDC tend to drain to the lateral neck initially. In cases where patients have a clinically positive lateral or central neck node, a neck dissection would be indicated without question. For patients with an N0 neck clinically, the indications for neck dissection can be extrapolated from those that the American Thyroid Association has recommended for the N0 central neck in thyroid cancer, which are T3 and T4 tumors principally. 120 This extension would be applicable especially given the fact that TGDC carcinoma has been widely shown to be less aggressive and has better prognostic outcomes than thyroid cancer. The next step in management is the issue of radioactive iodine. In total, 32.2% of patients received radioactive iodine, and of the patients who only had a Sistrunk followed by a total thyroidectomy, 70% received radioactive iodine. Physicians who advocate for a total thyroidectomy following a diagnosis of TGDC carcinoma often cite the possibility of adjuvant RAI as an advantage of this approach. There are no clear guidelines for when RAI should be implemented. In patients with cancer spread to the lymph nodes or those with concurrent thyroid and TGDC carcinomas or large tumors, it would be appropriate to consider RAI treatment. 119 Other reports in the literature support these findings. Mondin et al 105 discussed the management of TGDC carcinoma based on an extensive literature review. Their findings suggested that all patients should receive a Sistrunk procedure and that a total thyroidectomy and cervical lymphadenectomy should be considered in the presence of a concerning clinical or radiological lesion.
Nonpapillary Malignancies
Squamous cell carcinoma of the TGDC is a rare entity, with only a 4.3% incidence rate in our study. It is associated with a worse prognosis and is thought to arise from the cyst walls. 121 The treatment consists of a wide local excision of tissue along with a neck dissection if there are positive nodes. For squamous cell carcinoma, the option of adjuvant radiation therapy exists. Of the 9 patients in our study who had either squamous cell carcinoma or papillary and squamous cell carcinoma, 5 received adjuvant radiation therapy ( Table 4 ). One of 2 patients with mucoepidermoid carcinoma also received adjuvant radiation therapy. In our analysis, a young patient who had an unusual pathology of papillary carcinoma with squamous features received adjuvant radiation. Extracapsular tumor extension was also present in this case. None of the patients who received adjuvant radiation had recurrent disease, and no patients died. The indications for adjuvant radiation in patients with TGDC carcinomas are controversial given the rarity of squamous cell carcinoma. The criteria generally include extension beyond cyst wall margins, involvement of lymph nodes, positive margins, and recurrent disease. 122
Limitations
As a systematic review, a limitation of this study is selection bias as only published articles that met inclusion criteria were included in the final analysis. In addition, the analysis was limited by the quality of the articles available on this topic. Since TGDC carcinomas are relatively uncommon, the data analyzed came primarily from case reports and case series. There were no randomized controlled trials or multi-institutional analyses conducted on this topic. Hence, the overall quality of the data was poor, and this may introduce temporal and selection biases. Improvements to this study could be an analysis of the impact of tumor size on outcomes, but this was not possible due to the lack of data from multiple sources. Moreover, some studies had limited follow-up time; this limits the data on long-term outcomes and recurrence rates. Despite these shortcomings, TGDC carcinomas are rare, and conducting randomized controlled trials to determine treatment algorithms will be difficult; hence, this review is a useful addition to the literature.
Conclusion
Thyroglossal duct cyst carcinomas are rare findings in TGDCs. They are usually diagnosed incidentally following histopathologic analysis of an excised TGDC. Papillary thyroid carcinoma accounts for most TGDC carcinomas. All patients should undergo a Sistrunk procedure for removal of the TGDC. Performing a total thyroidectomy is controversial and generally should be reserved for patients older than 45 years who may benefit from RAI treatment. Lateral neck dissection should be performed in patients with positive nodes and may be considered in patients with more aggressive features, such as large tumors and invasion of local structures. Overall prognosis is excellent, with a survival rate of 99.4% and a recurrence rate of 4.3% among cases reported in the literature.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.