
Abstract
Objective
To evaluate the impact of bilateral middle turbinate resection (BMTR) on patient-reported quality of life following primary and revision endoscopic sinus surgery (ESS) for chronic rhinosinusitis (CRS).
Study Design
Prospective cohort study.
Setting
Tertiary care center.
Subjects and Methods
Patients with CRS who were recruited from 11 otolaryngologic practices completed the Sino-Nasal Outcome Test–22, Chronic Sinusitis Survey, and EuroQol 5-Dimension questionnaires at baseline, as well as 3 and 12 months after ESS. In the primary ESS cohort (n = 406), patients who underwent BMTR (n = 78) at the time of surgery were compared with patients (n = 328) whose middle turbinates were preserved. In the revision ESS cohort (n = 363), a similar comparison was made between patients who did (n = 64) and did not (n = 299) undergo BMTR.
Results
Sino-Nasal Outcome Test–22, Chronic Sinusitis Survey, and EuroQol 5-Dimension scores showed similar improvements for both the turbinate resection and preservation cohorts at 3 months (P < .001) and 12 months (P < .001) after surgery. For patients who underwent revision surgery, the performance of BMTR resulted in greater improvement in Chronic Sinusitis Survey scores at 1 year as compared with the turbinate preservation group (change from baseline: 28.1 vs 20.7, respectively; P = .026). History of tobacco use and the presence of nasal polyps did not affect clinical outcomes at any time point.
Conclusion
Patients who underwent BMTR during primary and revision sinus surgery reported similar benefits in quality-of-life outcomes 1 year after surgery. In select patients undergoing revision sinus surgery, the performance of BMTR results in improved disease-specific quality of life.
Chronic rhinosinusitis (CRS) can affect the mucosa of the middle turbinate resulting in inflammatory changes and nasal obstruction in patients with severe disease. When patients with CRS fail maximum medical therapy and require surgical intervention, the decision whether to perform bilateral middle turbinate resection (BMTR) can present the surgeon with a dilemma. Debate about resection of the middle turbinates has been ongoing since Kennedy first summarized the risks and benefits in 1998. 1 While many surgeons agree that middle turbinates with marked polypoid or inflammatory changes should be partially, if not fully resected, the decision to resect a middle turbinate with less severe disease as part of primary or revision sinus surgery remains controversial. Some surgeons cite improved intraoperative access and decreased postoperative synechiae formation as reasons to perform middle turbinate resection,2,3 while others favor routine preservation out of concern for postoperative atrophic rhinitis, iatrogenic frontal sinusitis, or anosmia.1,4
Recent advances in outcomes research related to CRS has afforded clinicians the opportunity to assess the patient’s perspective on surgical effectiveness. 5 Routine assessment of patient-reported health utility and quality of life (QoL) has been performed to evaluate treatment options for CRS, including turbinate resection as an adjunct to sinus surgery.6-8 A 2008 prospective study evaluated the effect of BMTR on Lund-Kennedy endoscopy scores, olfactory function, and QoL. 9 Both cohorts were found to have similar improvements across the 3 measures during the 18-month follow-up period. The authors concluded that the decision to preserve or resect the middle turbinate could be left to the individual surgeon’s discretion with little or no detriment in outcomes. 9
The impact of BMTR on patient-reported QoL as it relates to primary versus revision sinus surgery has not been previously evaluated. Several studies have demonstrated a decrement in patient-reported surgical outcomes among patients who have undergone prior sinus procedures.10,11 Furthermore, diseased middle turbinates have been implicated as a common source of failure for many patients requiring revision sinus surgery.12-14 Inflamed turbinate mucosa may be the source of recurrent polyps or adhesions leading to sinus outflow obstruction. Thus, the goal of this study was to evaluate the impact of BMTR on patient-reported QoL after both primary and revision sinus surgery.
Materials and Methods
The study population consisted of 769 patients with CRS refractory to medical therapy who underwent endoscopic sinus surgery (ESS) at a tertiary care hospital between February 2011 and November 2014. Study patients were recruited from 11 otolaryngologic practices (4 academic and 7 private). Demographic data, medical comorbidities, and smoking history were extracted from the medical records. The inclusion criteria were age >18 years, a clinical diagnosis of CRS, and failure of medical therapy with plans for ESS. Additionally, all patients undergoing revision ESS were required to have both middle turbinates still present prior to surgery. Surgical outcomes from this prospective cohort of patients have been described.15,16 The exclusion criteria included a diagnosis of neoplasm, trauma, or cerebrospinal fluid (CSF) leak. 16 Patients who underwent only unilateral middle turbinate resection were also excluded from the study.
In the primary ESS cohort (n = 406), 78 patients who underwent ESS with BMTR were compared with 328 patients who underwent ESS without BMTR. In the revision ESS cohort (n = 363), 64 patients who underwent ESS with BMTR were compared with 299 patients who underwent ESS without BMTR. The decision to perform BMTR was based on the surgeon’s intraoperative evaluation. Indications included limited access to the frontal recess from marked lateralization or hypertrophy of the middle turbinate, extensive middle turbinate mucosal disease from polyposis, and iatrogenic destabilization during surgery. For all surgeons in the study, middle turbinate resection was performed with a cold technique that utilized turbinate scissors to remove the anterior two-thirds of the turbinate. Major complications—defined as epistaxis requiring return to the operating room for control, CSF leak, and orbital injury—were also compared between cohorts. All participating surgeons placed patients on nasal saline rinses beginning on postoperative day 1.
Patients completed the EuroQol 5-Dimension (EQ-5D) questionnaire, Sino-Nasal Outcome Test–22 (SNOT-22), and Chronic Sinusitis Survey (CSS) questionnaires on the day of surgery (baseline) and at 3 and 12 months postoperatively. Surveys were administered in person on the day of surgery and online thereafter. The patients completed all questionnaires independently. Data collection was performed in a manner compliant with the Health Insurance Portability and Accountability Act, as previously described. 17 Institutional review board approval was obtained from the Human Studies Committee of the Massachusetts Eye and Ear Infirmary.
Statistical Analyses
Baseline comorbidities, demographic and clinical characteristics, and QoL scores were compared between patients who had BMTR and those who did not ( Table 1 ). Two-sided t tests (2 independent samples) compared variables with continuous characteristics. Two-sided z tests (2 independent samples) compared proportions. The significance threshold (P < .004) for characteristics in Table 1 was calculated per the standard Bonferroni correction equation. 18
Baseline Comorbidities and Demographic and Clinical Characteristics. a
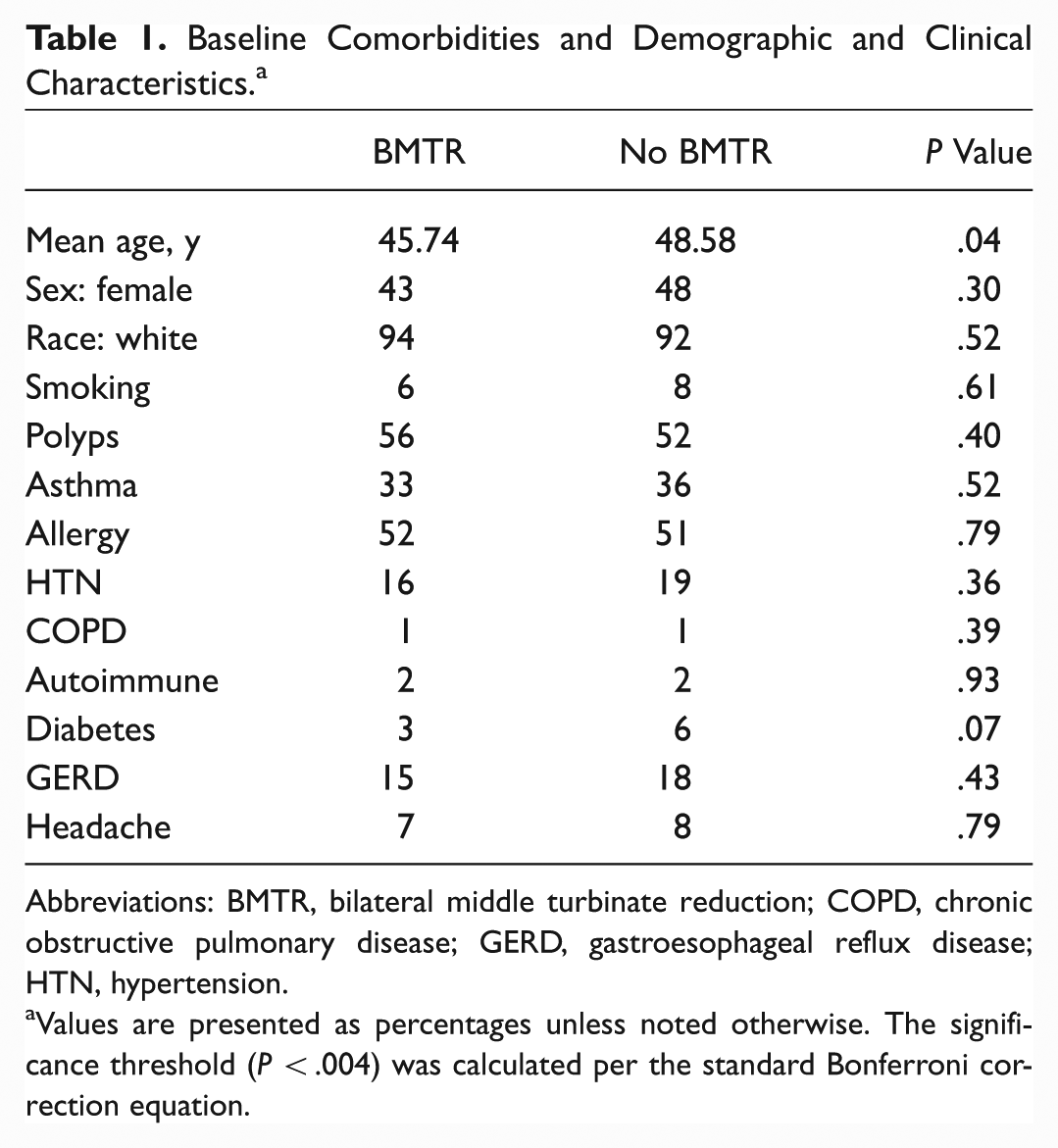
Abbreviations: BMTR, bilateral middle turbinate reduction; COPD, chronic obstructive pulmonary disease; GERD, gastroesophageal reflux disease; HTN, hypertension.
Values are presented as percentages unless noted otherwise. The significance threshold (P < .004) was calculated per the standard Bonferroni correction equation.
Univariate regressions were conducted to test the primary hypothesis of examining the association between patient-reported QoL and the timing of BMTR. Two-sided t tests (2 independent samples) compared SNOT-22, CSS, and health utility value (HUV) scores between the BMTR and non-BMTR cohorts at baseline and each of the follow-up time points through 1 year following surgery. Multivariate regression analysis was performed on all statistically significant univariate results. Finally, the accepted minimal clinically important differences (MCIDs) on all outcomes surveys were utilized, which is calculated as half the standard deviation of the mean baseline score of each survey.
Results
Patient Characteristics
A total of 769 patients with CRS who met inclusion criteria were enrolled over a 3-year period. The patient response rate was 77.7% at 3 months and 69.8% at 12 months. Patient demographics and comorbidities are provided in Table 1 . None of the demographic categories or comorbidities met the adjusted Bonferroni significance threshold (P < .004); thus, multivariate regression analysis was deemed to provide no additional information regarding the insignificant association between any of the items listed in Table 1 and BMTR. The baseline HUV (mean ± SD) for the primary ESS cohort was 0.837 ± 0.102 for the BMTR cohort and 0.836 ± 0.136 for the non-BMTR cohort. The baseline HUV for the revision ESS cohort was 0.819 ± 0.130 for the BMTR cohort and 0.826 ± 0.117 for the non-BMTR cohort.
Outcomes after Sinus Surgery
Based on a linear mixed model, changes from baseline and associated significance thresholds were calculated for all outcomes surveys at all time points ( Table 2 ). SNOT-22 and EQ-5D scores significantly improved and exceeded the MCID for both primary and revision cohorts at all time points ( Figures 1 and 2 ). Additionally, multivariate regression did not reveal any significant association between age, sex, smoking status, prior surgery, nasal polyps, allergy, or headache and the observed improvement in SNOT-22 or EQ-5D scores at 12 months. The timing of BMTR was not found to significantly change the average SNOT-22 or EQ-5D improvement at either 3 or 12 months.
Changes in Outcomes Measures over Time. a
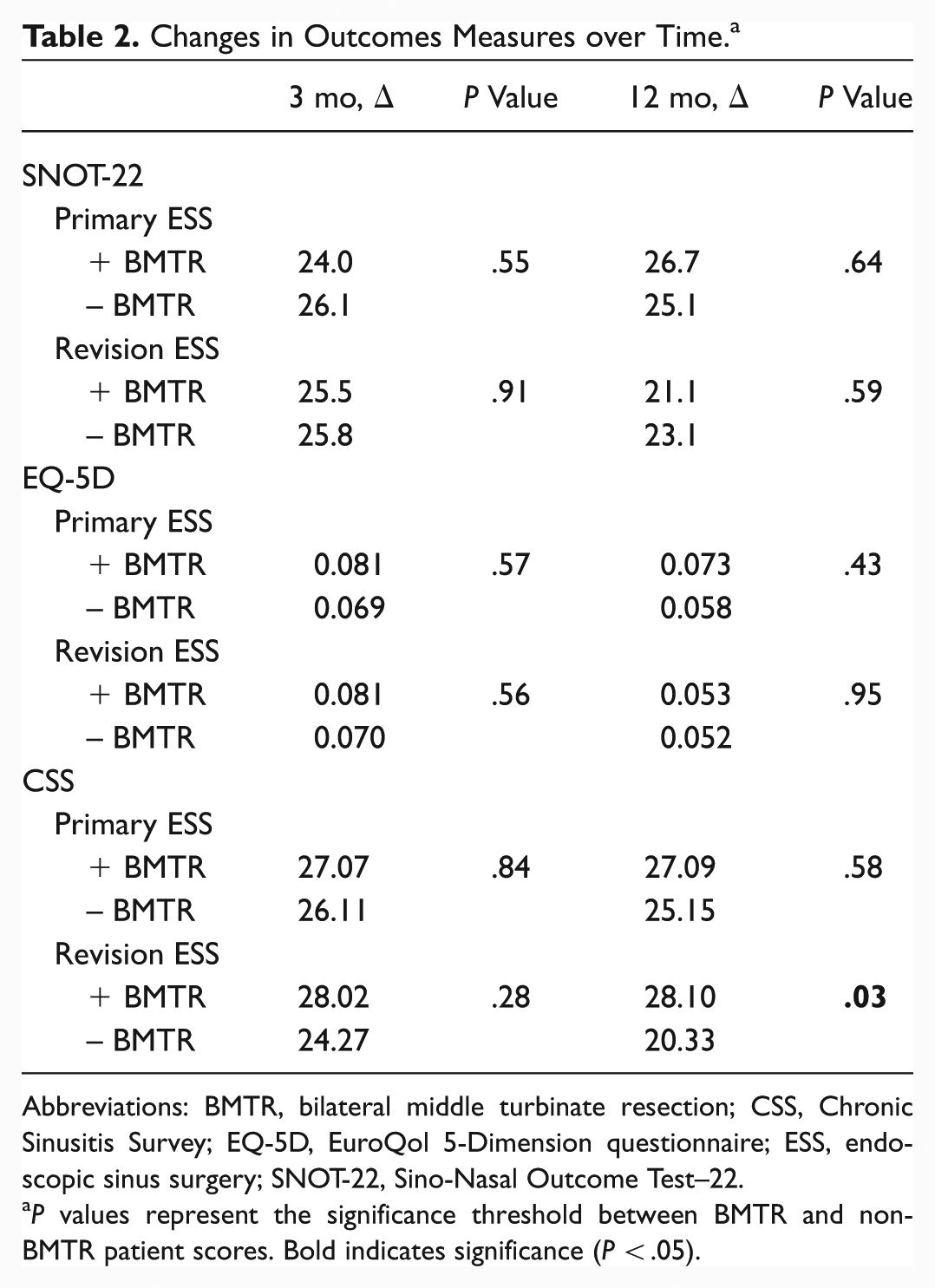
Abbreviations: BMTR, bilateral middle turbinate resection; CSS, Chronic Sinusitis Survey; EQ-5D, EuroQol 5-Dimension questionnaire; ESS, endoscopic sinus surgery; SNOT-22, Sino-Nasal Outcome Test–22.
P values represent the significance threshold between BMTR and non-BMTR patient scores. Bold indicates significance (P < .05).
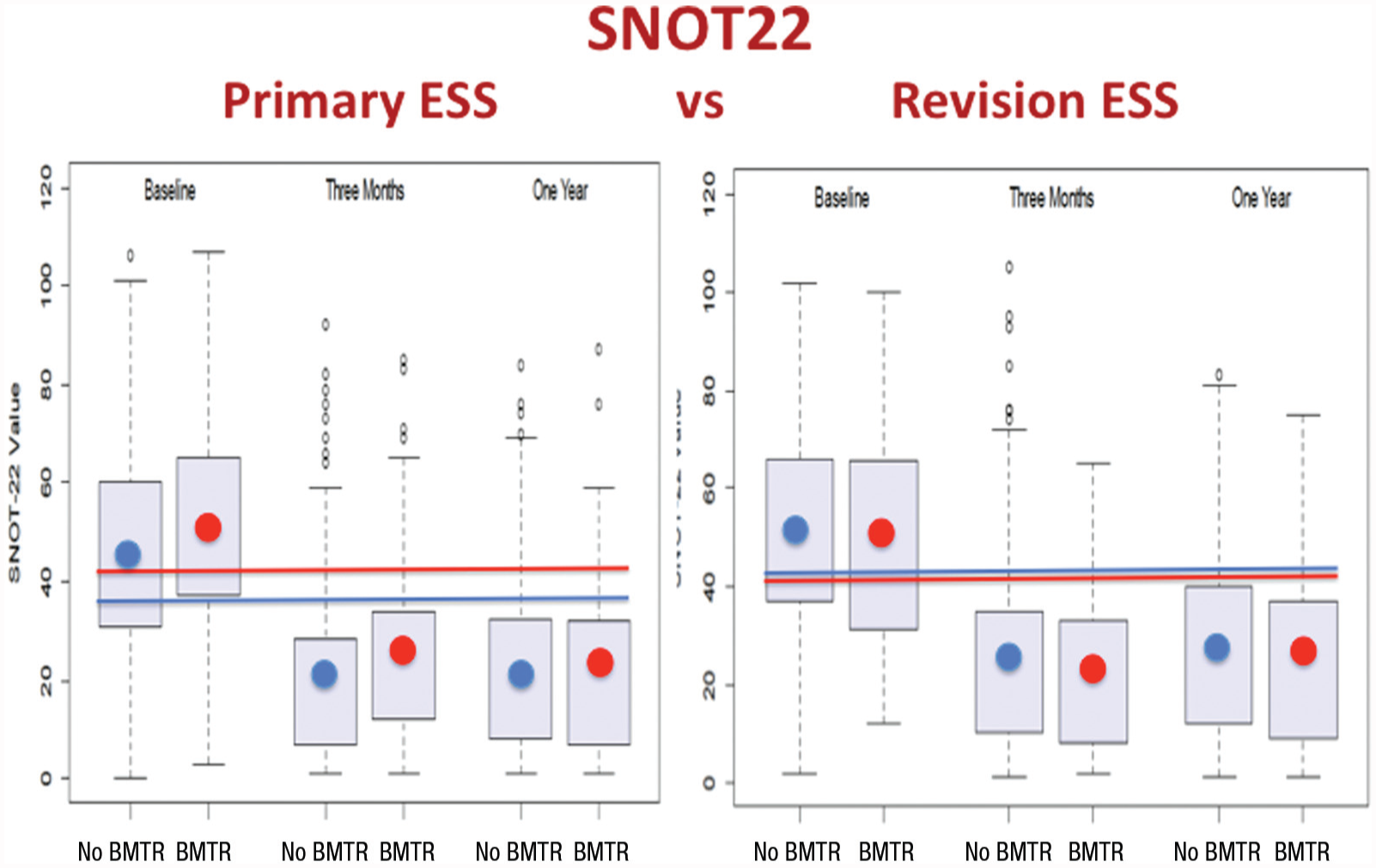
Patients with chronic rhinosinusitis undergoing ESS ± BMTR experience improved SNOT-22 scores durable at 1 year (P < .05). Circles, average scores; lines, minimal clinically important differences (≥8.90). Boxes, interquartile range; whiskers, 95% CI; small circles, outliers. BMTR did not effect the significant improvement in scores. BMTR, bilateral middle turbinate resection; ESS, endoscopic sinus surgery; SNOT-22, Sino-Nasal Outcome Test–22.
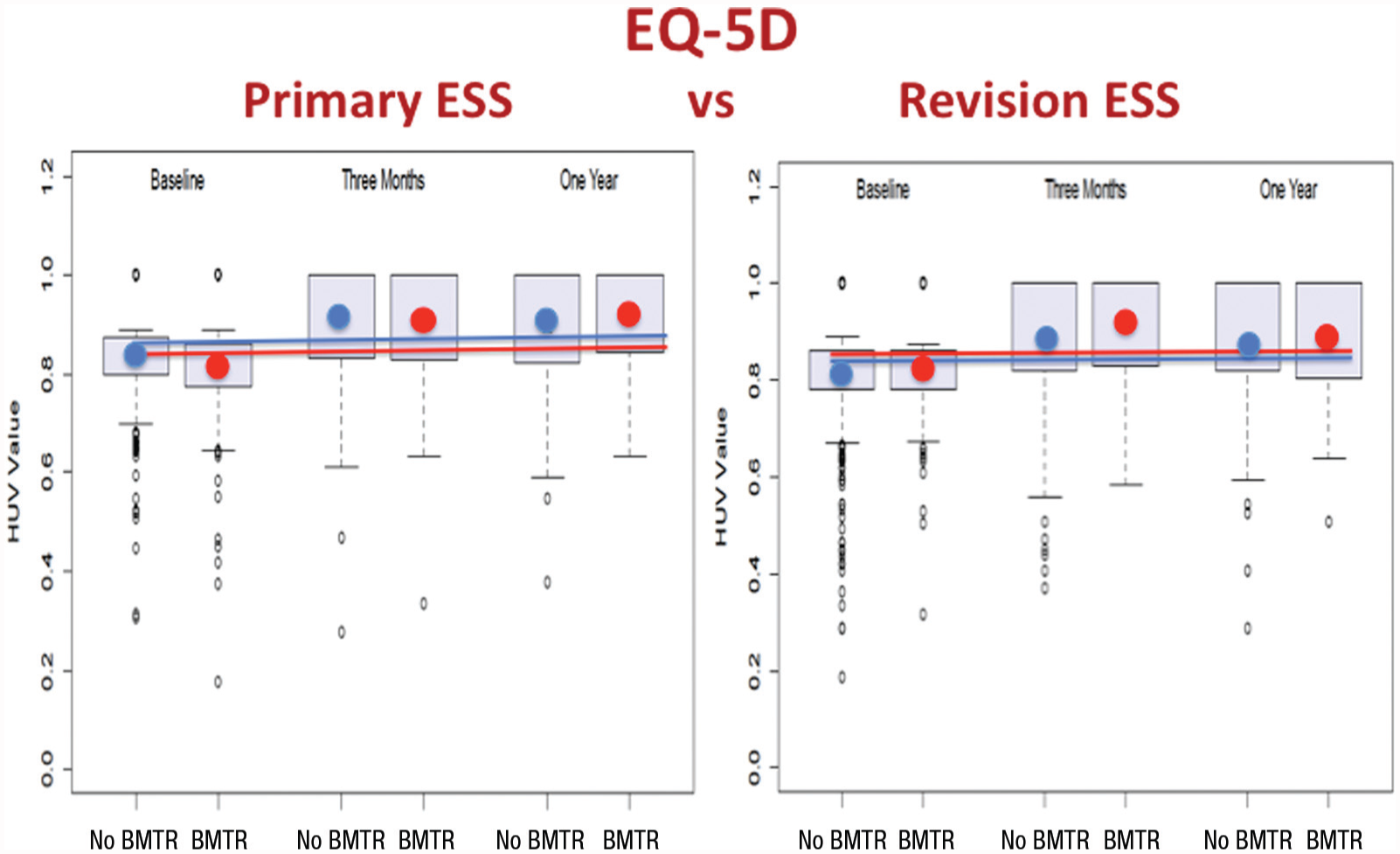
Patients with chronic rhinosinusitis undergoing ESS ± BMTR experience improved HUV scores durable at 1 year (P < .05). Circles, average scores; lines, minimal clinically important differences (≥0.03). Boxes, interquartile range; whiskers, 95% CI; small circles, outliers. BMTR did not effect the significant improvement in scores. BMTR, bilateral middle turbinate resection; EQ-5D, EuroQol 5-Dimension; ESS, endoscopic sinus surgery; HUV, health utility value.
CSS scores were also found to significantly improve and exceed the MCID at all time points for both cohorts ( Figure 3 ). Interestingly, for patients undergoing revision ESS, BMTR resulted in a significantly improved average CSS score on multivariate regression (P = .026) at 12 months. An examination of the effect of covariates on the change of CSS scores did not reveal any significant association between age, sex, smoking status, prior surgery, nasal polyps, allergy, or headache and the observed change in CSS scores at 12 months.
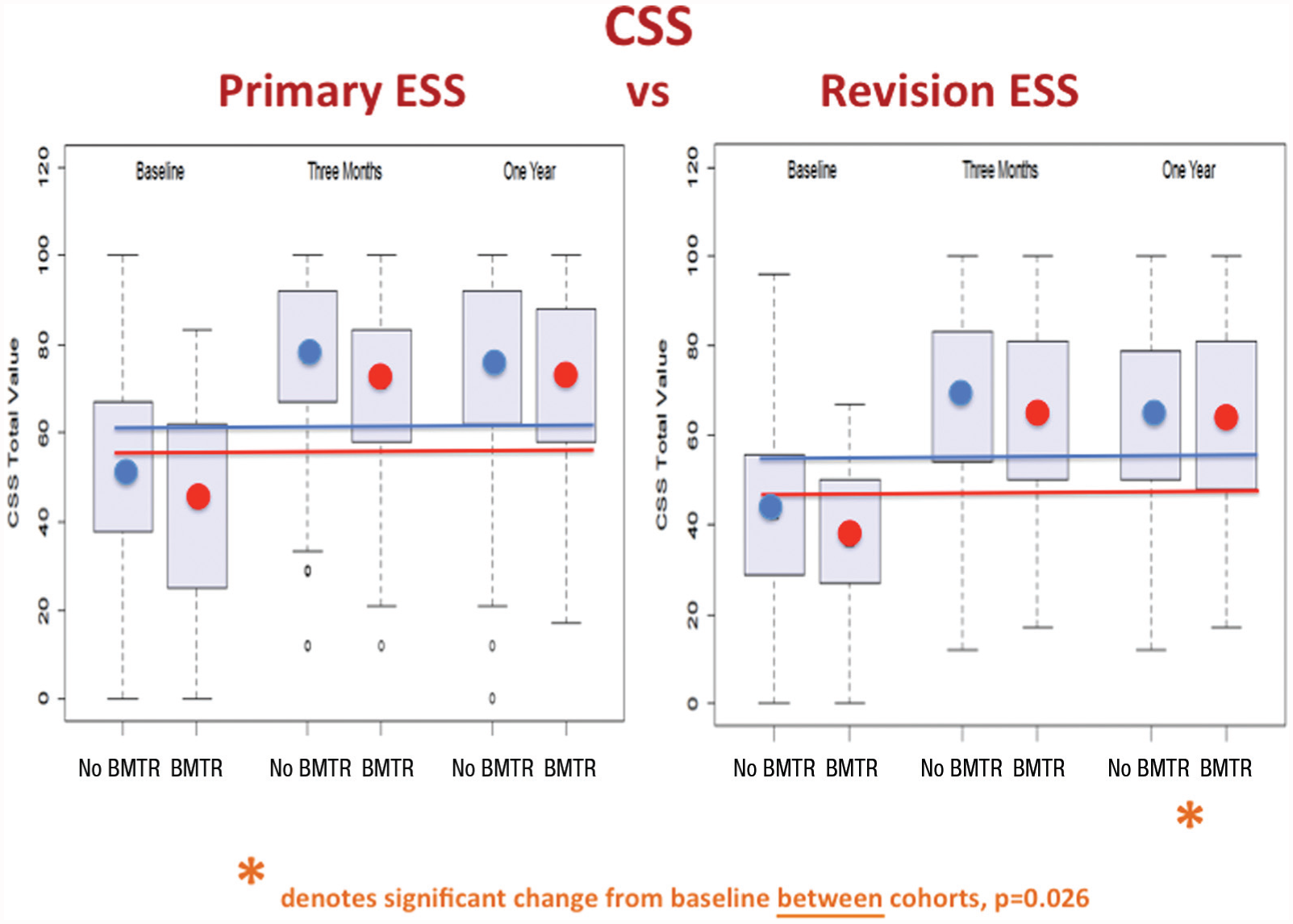
Patients with chronic rhinosinusitis undergoing ESS ± BMTR experience improved CSS scores durable at 1 year (P < .05). Circles, average scores; lines, minimal clinically important differences (≥9.75). Boxes, interquartile range; whiskers, 95% CI; small circles, outliers. In revision ESS, BMTR improved scores at 1 year (P = .026). BMTR, bilateral middle turbinate resection; CSS, Chronic Sinusitis Survey; ESS, endoscopic sinus surgery.
There were no major complications of CSF leak or orbital injury in either cohort. There were 7 cases of epistaxis requiring return to the operating room for control (2 of 7 patients underwent BMTR). The incidence of major epistaxis was not significantly associated with the performance of BMTR. Finally, there were no cases of atrophic rhinitis, iatrogenic frontal sinusitis, or required revision ESS reported in this patient cohort within the follow-up period of 1 year. Data are not available regarding the frequency of perioperative and postoperative antibiotic and nasal steroid prescriptions for this patient cohort.
Discussion
Given the ongoing debate regarding preservation versus resection of the middle turbinates during surgery for CRS, understanding the impact of BMTR on patient-reported QoL should serve to inform a surgeon’s intraoperative decision. Furthermore, evaluating the impact of BMTR at the time of initial versus revision sinus surgery will help validate such decisions across a range of patients undergoing ESS.
In the current study, patients with refractory CRS reported significant improvement in general and disease-specific QoL after primary, as well as revision, sinus surgery. Observed improvements in all tested health outcomes instruments were found to be durable, lasting at least 1 year after ESS. Patients undergoing BMTR showed improvement in QoL after ESS that was equivalent to that for patients who had their middle turbinates preserved. These findings suggest that the performance of a middle turbinectomy during ESS does not lead to a significant decrement in a patient’s QoL. Indeed, patients should be expected to have QoL improvements no different from patients who do not undergo BMTR. These results are similar to those reported by Soler et al who found that CRS patients undergoing ESS with and without BMTR had similar endoscopy scores, olfactory function, and disease-specific and general QoL scores at a mean follow-up time of 17.4 months. 9
An important focus of this study was to identify any association between the timing of BMTR and long-term patient-reported outcomes. For patients who underwent revision ESS, the performance of BMTR resulted in an equivalent improvement in SNOT-22 and EQ-5D scores but a significantly greater improvement in CSS scores at 1 year post-ESS. This finding may reflect improved long-term patency of the sinonasal passages when a middle turbinate has been resected. One could hypothesize that the increased anatomic size of these passages after BMTR makes them less susceptible to reobstructive symptoms, such as nasal congestion, should future mucosal swelling develop. An examination of the effect of covariates did not reveal any significant association between nasal polyps, age, sex, smoking status, allergy, or headache and these observed changes in CSS scores at 12 months.
Traditionally, surgeons who have advocated middle turbinate preservation have cited the increased risk of complications associated with this procedure.1,19 In the current study, there was no significant difference in the incidences of major epistaxis requiring a return trip to the operating room between cohorts. Additionally, there were no cases of CSF leak or orbital injury in either cohort. Choby et al similarly reported no difference in the rate of immediate complications in patients undergoing ESS with or without BMTR. 20 Additionally, Havas et al reported on a series of 1106 patients, half of whom underwent partial middle turbinate resection, and reported zero incidence of CSF leak and no significant difference between immediate complication rates for epistaxis and orbital hematoma. 21 Overall, our data support the position that BMTR remains a safe procedure in the hands of community-based and academic otolaryngologists.
The decision to resect the middle turbinates in this study was based on the surgeon’s intraoperative evaluation and aforementioned indications. Review of the data showed that BMTR was performed in 17.4% of revision cases and 19.8% of primary cases. Additionally, there was no significant difference between BMTR and non-BMTR cohorts in terms of baseline disease-specific or general health scores. Indications for BMTR may vary by surgeon. In this observational study, the majority of BMTR procedures (88.1%) were performed by 3 of the 11 surgeons. However, these same 3 surgeons also performed 88.5% of the non-BMTR procedures, which suggests a minimal effect of selection bias on patient selection for BMTR. Overall, the inclusion of patients from 11 otolaryngology practices, academic and private, help make the findings more generalizable.
In this study, several intrinsic assumptions and limitations merit attention. Response rates were 77.7% at 3 months and 69.8% at 12 months, which could represent a response bias with patients with poorer outcomes less likely to respond to subsequent questionnaires. However, a separate analysis was performed that included patients who did not respond at all time points, and it revealed no difference in terms of baseline demographics or any of the outcome measures. Finally, patients completed initial evaluations on the actual day of surgery, which could lead to reporting bias.
Conclusion
Patients undergoing primary and revision sinus surgery with BMTR reported significant benefits in disease-specific and general QoL outcome measures out to 1 year. BMTR for surgical access or disease is safe and perhaps favorable in select cases.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2016 AAO-HNSF Annual Meeting & OTO EXPO; September 18-21, 2016; San Diego, California.