
Abstract
Objective
In many cancers, including head and neck squamous cell carcinoma (HNSCC), different regions within a tumor have different metabolic phenotypes. Transfer of metabolites between compartments promotes tumor growth and aggressive behavior. Metabolic compartmentalization in HNSCC nodal metastases has not been studied, nor has its impact on extracapsular extension or clinical outcomes been determined.
Study Design
Retrospective analysis based on immunohistochemistry staining.
Setting
Tertiary care center.
Subjects and Methods
Primary tumors and nodal metastases from 34 surgically treated oral cavity HNSCC patients with extracapsular extension (ECE) were stained for monocarboyxlate transporter (MCT) 4, MCT1, translocase of outer mitochondrial membrane 20, and Ki-67. Strength of staining was assessed using a computer-assisted pathology algorithm. Immunohistochemistry (IHC) scores along with clinical factors were used to predict disease-free survival (DFS).
Results
Patterns of IHC staining showed metabolic compartmentalization both at the primary tumor sites and in nodal metastases. MCT4 staining in the perinodal stroma was significantly higher in specimens with ECE greater than 1 mm (macro-ECE, P = .01). Patients with high perinodal MCT4 staining were compared with those with low perinodal MCT4 staining. On multivariate analysis, only high perinodal MCT4 staining had a significant impact on DFS (P = .02); patients with high perinodal MCT4 had worse survival. DFS was not significantly worsened by advancing T stage, N stage, ECE extent, or perineural invasion.
Conclusion
Oral HNSCC displays compartmentalized tumor metabolism at both primary and metastases. Greater cancer-associated stromal conversion around ECE, denoted by high stromal MCT4, may be a biomarker for aggressive disease and worsened DFS.
Head and neck squamous cell carcinoma (HNSCC) is the sixth most common human cancer, with approximately 50,000 new cases diagnosed in the United States in 2013. 1 Even with advances in treatment, HNSCC recurrence rates remain as high as 50% to 60% over a 5-year period when all comers are taken into account. 2 Nodal metastasis in HNSCC is a strong driver of poor prognosis, 3 and survival is further worsened if lymph node metastases are found to have extracapsular extension (ECE).3,4 ECE is an indicator of poor prognosis for not only HNSCC but also squamous cell carcinoma of other sites such as skin, cervix, and lung.5-11 ECE predicts poor overall survival, recurrence at the primary site, and distant metastases. 12
Extracapsular Extension
Traditionally, ECE has been evaluated as a dichotomous variable, being present or absent; more recent evidence, however, suggests that prognosis may depend on the degree of ECE. On pathologic evaluation, ECE may be focal or extensive, or it may replace the entire node. Extensive ECE has been shown to worsen prognosis compared with focal ECE in laryngeal and hypopharyngeal tumors. 13 In studies of oropharyngeal tumors, regional metastases that completely replaced lymph nodes were predictive of more aggressive tumor behavior compared with metastases only focally extending outside the lymph node.14,15 These observations have raised the question of whether ECE should be graded. Prabhu et al 16 published a study evaluating graded ECE as a prognostic factor on a graded scale. They found that survival in node-positive cancers without ECE was not statistically significantly different from those with less significant ECE; however, in the presence of extensive ECE, survival was significantly worse despite adjuvant therapy.
The pathophysiologic mechanism of ECE is not fully understood. It was long thought that ECE occurred as the tumor grew within the node and was related only to the size of the metastasis with the node. Typically, 60% to 90% of nodes over 3 cm have been shown to have extracapsular spread compared with 23% of nodes under 1 cm. 17 However, the fact that even smaller nodes without complete tumor replacement may show ECE suggests that ECE is not related to size alone.18,19 Several theories have been proposed to explain this, such as trapped tumor emboli in the nodal capsule, yet such theories have not been explored. Clearly, the process of nodal metastasis and ECE involves a series of complex interactions within the microenvironment of the tumor and lymph node.
Metabolism in the Tumor Microenvironment
The tumor microenvironment plays a critical role in many of the processes involved in tumorigenesis, including metabolic mechanisms within the tumor. Metabolic coupling between distinct tumor compartments contributes to tumorigenesis, tumor invasion, and metastasis. 20 Pavlides et al 21 first published a “reverse Warburg” model of metabolism in breast cancer; in this model, cancer cells induce aerobic glycolysis in surrounding stromal cells, while they themselves maintain oxidative phosphorylation, fueling tumorigenesis.21-24 The glycolytic stromal cells that support cancer cells in this model are known as cancer-associated fibroblasts. Breast cancers with metabolic coupling have aggressive disease behavior and worse survival. 25 Our previous work shows that metabolic coupling exists in vitro in a squamous cell carcinoma co-culture model and in a subset of HNSCC tumors; when markers of metabolic coupling are present, tumors behave more aggressively. 26
Markers of Metabolic Coupling
The transfer of metabolites between metabolically coupled tumor compartments is thought to be mediated by monocarboxylate transporters (MCTs) 1 and 4 ( Figure 1 ). MCT1 generally functions as a transporter of pyruvate and lactate into cells. On immunohistochemistry (IHC) staining, cells with abundant MCT1 also have increased markers for cell growth and mitochondrial activity, as evidenced by increased staining for Ki-67 and translocase of outer mitochondrial membrane 20 (TOMM20), respectively ( Figure 1 ). MCT4 is a transporter of pyruvate and lactate out of cells, and its expression is upregulated by hypoxia and inflammation. MCT4 is commonly seen in cancer-associated fibroblasts (CAFs), and increased MCT4 staining in CAFs worsens disease-free survival in HNSCC. 26

Diagram of multicompartment tumor metabolism. Pyruvate and lactate are exported by monocarboxylate transporter (MCT) 4 from cancer-associated fibroblasts and imported by MCT1 into carcinoma cells to generate energy by oxidative phosphorylation. Carcinoma stains for MCT1, Ki-67, and translocase of outer mitochondrial membrane 20 (TOMM20).
Metabolism and Nodal Metastasis
The importance of nodal metastasis and ECE is well established, and our previous work suggests that metabolic coupling at the primary tumor indicates aggressive behavior in HNSCC. However, it is not known whether metabolic coupling between carcinoma cells and cancer-associated fibroblasts occurs at sites of nodal metastasis or if the metabolic phenotype at nodal metastases indicates disease behavior. This preliminary study aims to characterize the metabolic microenvironment of metastatic HNSCC and examine its potential role in ECE in lymph node metastases.
Materials and Methods
Subjects
Following institutional review board (IRB) approval, a clinical database of patients with oral cavity squamous cell carcinoma treated since 2009 was searched to identify patients treated at our institution with primary surgery for oral cavity HNSCC with nodal metastasis and ECE. From this database, 34 consecutive patients having undergone initial surgical resection and identified to have extracapsular lymph node extension (ECE) were identified having initial treatment between May 2009 and May 2015. All patients’ charts were reviewed for clinical and radiologic data, including age, sex, smoking history, primary tumor location, recurrence, and survival. Pathologic data reviewed were human papillomavirus (HPV) status, TNM stage, tumor grade, perineural invasion (PNI), lymphovascular invasion (LVI), and ECE. Patients were treated in accord with National Comprehensive Cancer Network (NCCN) guidelines and presented at a multidisciplinary tumor board, which made recommendations for adjuvant treatment, including radiation and chemotherapy.
Specimens
Initial pathology reports reported ECE as a binary variable (present or absent). All cervical metastases for identified patients were reexamined with hematoxylin and eosin (H&E) stains, and the extent of ECE was determined by computer-assisted measurement of the slides. ECE was quantified by distance from the edge of the capsule, either less than 1 mm (micro-ECE) or greater than 1 mm (macro-ECE) ( Figure 2 ). This was done in accord with previous grading strategies.14,27 Nodal specimens were then immunohistochemically stained for MCT1, MCT4, Ki-67, and TOMM20. All primary tumors also underwent immunohistochemistry (IHC) staining for MCT1, MCT4, Ki-67, and TOMM20, as previously described. 26
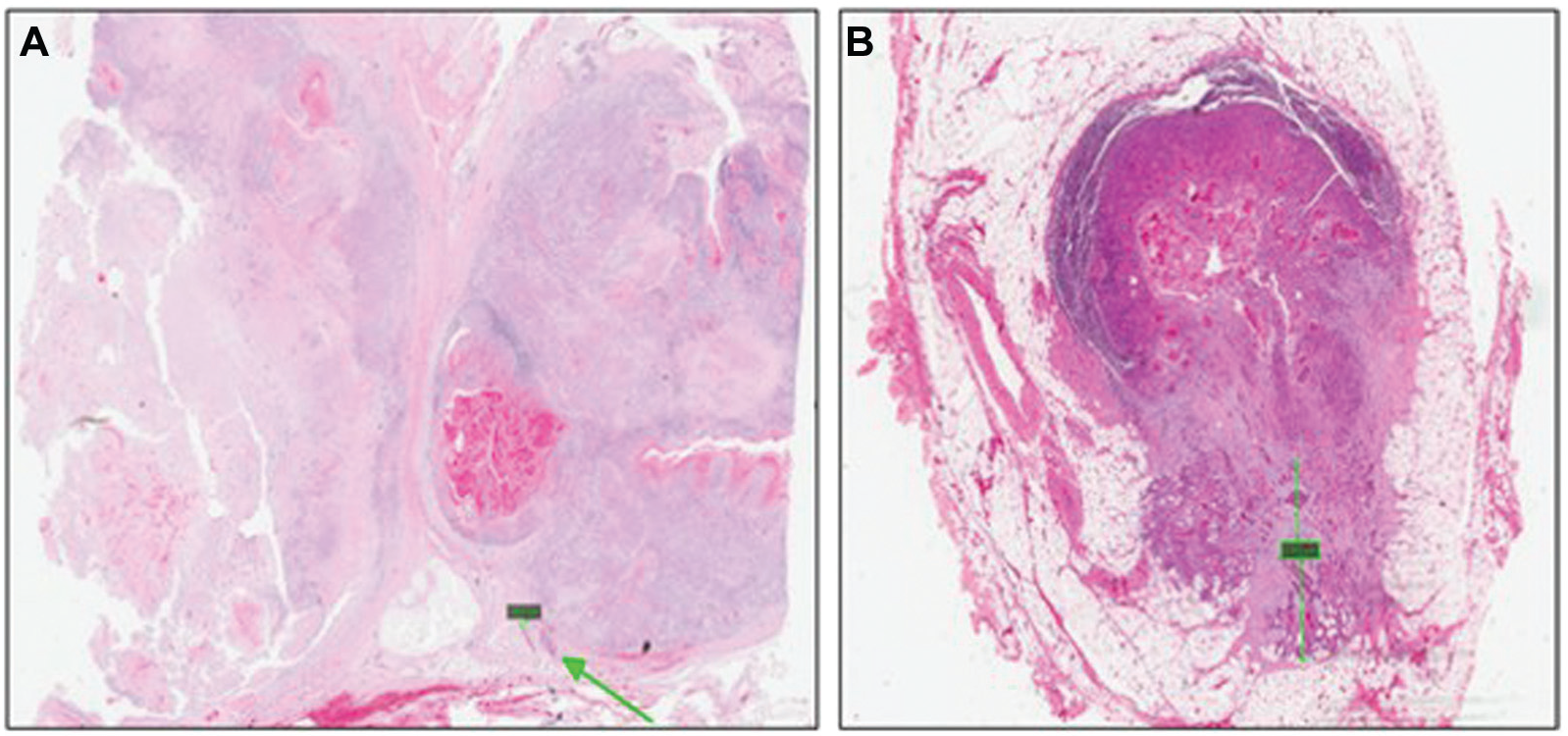
Hematoxylin and eosin staining of metastatic lymph nodes with computer-assisted measurement of extent of extracapsular extension (ECE). (A) Micro-ECE (less than 1 mm). (B) Macro-ECE (greater than 1 mm).
Briefly, paraffin-embedded primary tumors and nodal specimens were sectioned (4 microns) and stained for MCT1, MCT4, Ki-67, and TOMM20 using the Ventana Discovery Ultra IHC/ISH automated slide staining system (Ventana Medical Systems, Tucson, Arizona). Antigen retrieval was performed using Discovery CCI (cat. 950-500; Ventana Medical Systems) for a total application time of 64 minutes. Primary antibody immunostaining was performed for 45 minutes followed by secondary immunostaining using a horseradish peroxidase (HRP) multimer cocktail (cat. 760-500; Ventana Medical Systems), and immune complexes were visualized using the ultraView Universal DAB (diaminobenzidine tetrahydrochloride) Detection Kit (cat. 760-500; Ventana Medical Systems). Slides were then washed with a Tris-based reaction buffer (cat. 950-300; Ventana Medical Systems) and stained with Hematoxylin II (cat. 790-2208; Ventana Medical Systems) for 8 minutes. Primary antibodies were rabbit polyclonal affinity purified MCT1 (19-mer peptide sequence CSPDQKDTE GGPKEEESPV) and MCT4 (19-mer peptide sequence CKAEPEKNGEVVHTPETSV)(YenZym Antibodies, South San Francisco, California), Confirm Ki-67 (30-9) rabbit monoclonal antibody (cat. 790-4286; Ventana Medical Systems), and Tom20 (F-10) mouse monoclonal antibody (sc-17764; Santa Cruz Biotechnology, Santa Cruz, California).
Digital Image Analysis
Quantitative analysis of MCT1, MCT4, TOMM20, and Ki-67 immunohistochemistry was performed using Aperio software (Aperio, Nussloch, Germany) as described previously. 28 Briefly, digital images were captured with Leica and Aperio slide scanners under ×20 magnification with an average scan time of 120 seconds (compression quality 70). The “Membrane” algorithm was used for MCT1 staining analysis. Based on the manufacturers’ description, this algorithm detects the membrane staining for individual tumor cells in selected regions and quantifies the intensity and completeness of the membrane staining. The Aperio “Nuclear” algorithm was used for Ki-67 analysis to count the number of cancer cells in total and measure the intensity of positive staining in each cell. The percentage of positively stained cells was calculated respectively. Quantitative analysis of TOMM20 and MCT4 was also performed employing the “Colocalization” algorithm, which uses color deconvolution. Areas of staining were color separated from hematoxylin counterstained sections, and the intensity of the staining was measured on a continuous 0 (bright white) to 255 (black) scale. TOMM20 was considered high when at least 70% of cells demonstrated strong, diffuse cytoplasmic staining, and MCT4 was scored high where 70% of the cancer-associated fibroblasts expressed positivity within the stromal cells separating nests of proliferating carcinoma cells. The mean intensity was calculated for each specimen, and a value was assigned to each; these values, though arbitrary, can be used to compare across specimens that are analyzed in the same way.
Statistical Analysis
IHC staining scores for MCT 1, MCT4, Ki-67, and TOMM20 were compared between groups using the Student t test. Cutoff values for MCT4 strength of staining were determined using receiver operator characteristics curves. 29 Disease-free survival (DFS) was analyzed using Kaplan-Meier survival curves and was compared using the log-rank test. Multivariate analysis was conducted using a Cox proportional hazards model. Statistical significance was defined as P < .05. All statistical analyses were conducted using R statistics package version 3.3.1 (R Foundation, Vienna, Austria).
Results
Patients
Thirty-four consecutive patients with oral cavity cancer with lymph node metastases and ECE were studied ( Table 1 ). Tumors were distributed across T stage, and most patients had N2b or N2c disease. All patients were American Joint Committee on Cancer (AJCC) stage IVa, except 2 patients who were stage III (T1N1 and T2N1). No patients had positive surgical resection margins, and the remaining pathologic features are described in Table 1 . Follow-up for the entire cohort ranged from 3.5 to 76.5 months, with a mean follow-up of 24 months. Mean follow-up for surviving patients was 34.7 months (range, 3.6-76.5 months). Nineteen patients developed recurrence over the study period, with an average of 9 months to diagnosis of recurrence (range, 3.7-21 months); 12 patients had locoregional recurrence, and 7 had distant metastatic disease.
Demographics and Pathologic Features.
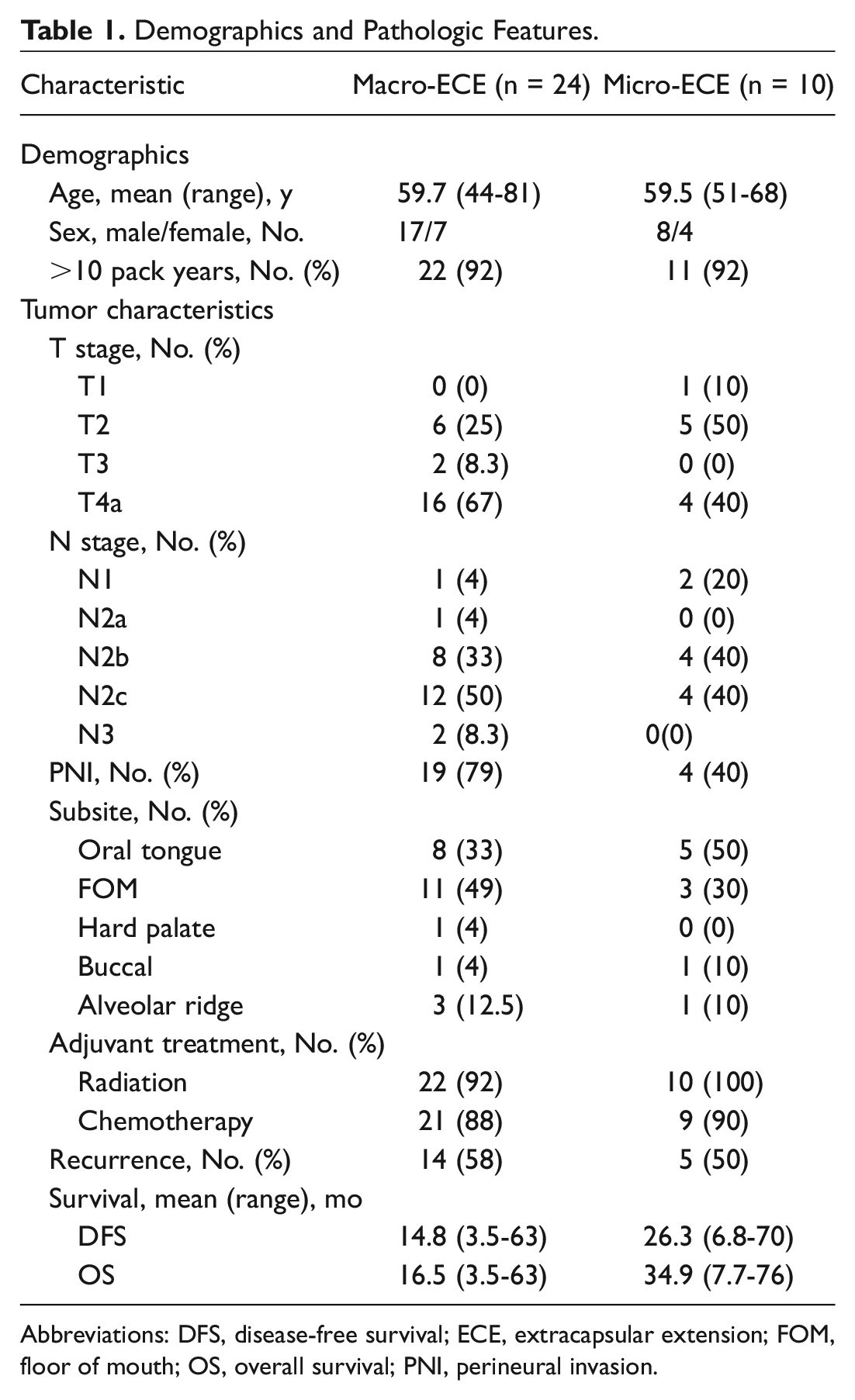
Abbreviations: DFS, disease-free survival; ECE, extracapsular extension; FOM, floor of mouth; OS, overall survival; PNI, perineural invasion.
Ten patients (29%) had micro-ECE, or ECE less than 1 mm from the edge of the capsule, and 24 patients (71%) had macro-ECE, or ECE greater than 1 mm from the capsule. Five patients with micro-ECE had recurrence: 3 with locoregional recurrence and 2 with distant metastasis. Among the patients with macro-ECE, 14 had recurrence ( Table 1 ). Extent of ECE was not associated with worsened DFS (P = .23; Table 2 ).
Univariate and Multivariate Survival Analysis by Log-Rank Test.
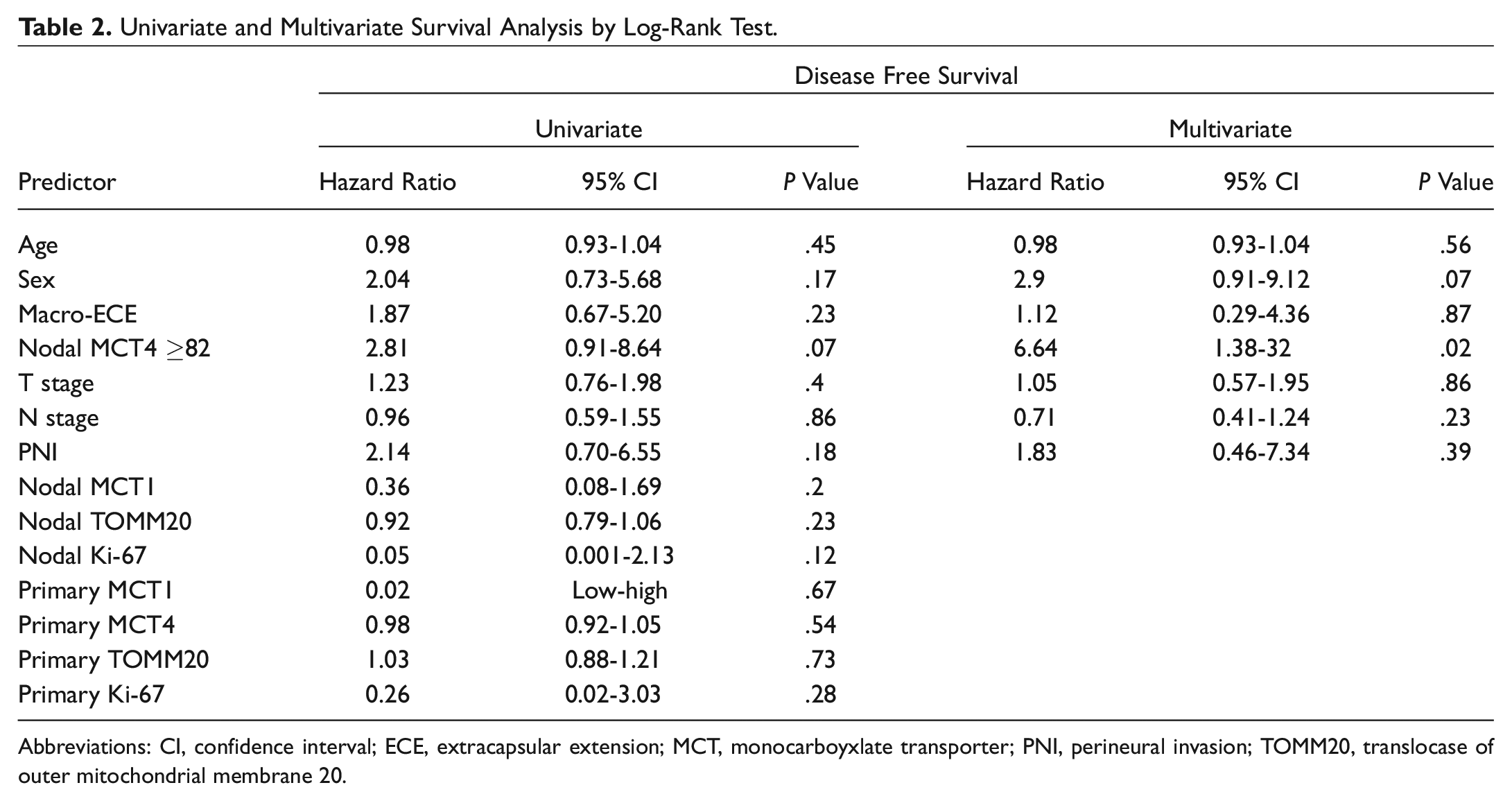
Abbreviations: CI, confidence interval; ECE, extracapsular extension; MCT, monocarboyxlate transporter; PNI, perineural invasion; TOMM20, translocase of outer mitochondrial membrane 20.
Immunohistochemistry
Primary tumors vs nodal metastasis
Staining patterns of carcinoma and stromal cells were assessed in both the primary tumors and at sites of lymph node metastasis. Patterns of MCT1, MCT4, TOMM20, and Ki-67 were consistent with metabolic compartmentalization at primary and nodal sites: MCT1, TOMM20, and Ki-67 stained strongly at the leading edge of the tumor, while MCT4 stained strongly in the stromal compartment ( Figure 3A-D , Figure 4A-D ). IHC strength of staining scores generated for each specimen were compared between primary and lymph node sites, with no difference seen between groups ( Table 3 ).
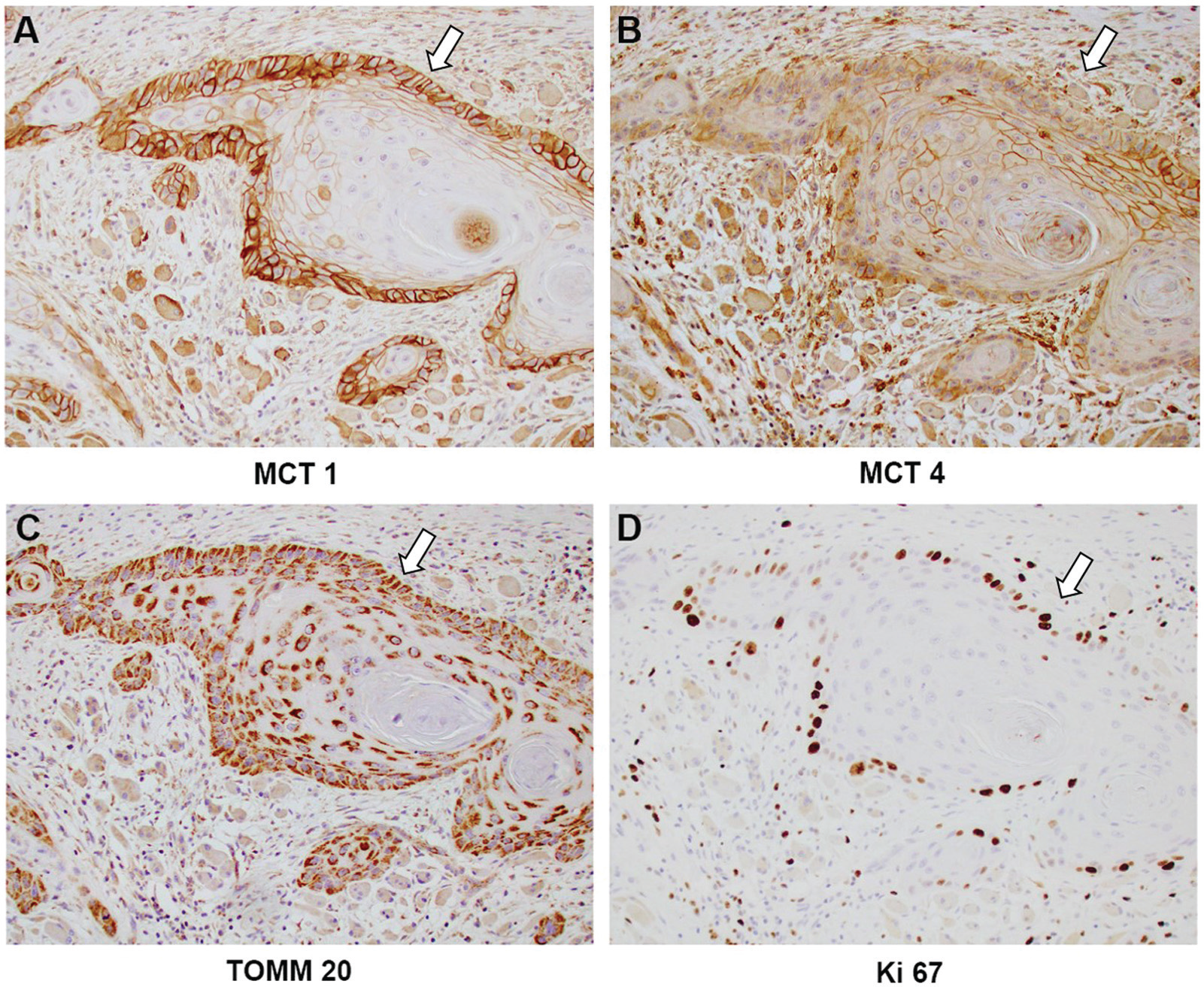
Immunohistochemistry staining (×20 light microscopy) of primary oral cavity tumor at tumor-stromal interface (white arrows). Note strong monocarboyxlate transporter (MCT) 1 (A), translocase of outer mitochondrial membrane 20 (TOMM20) (C), and Ki-67 (D) at leading edge of carcinoma, with stromal staining for MCT4 (B).
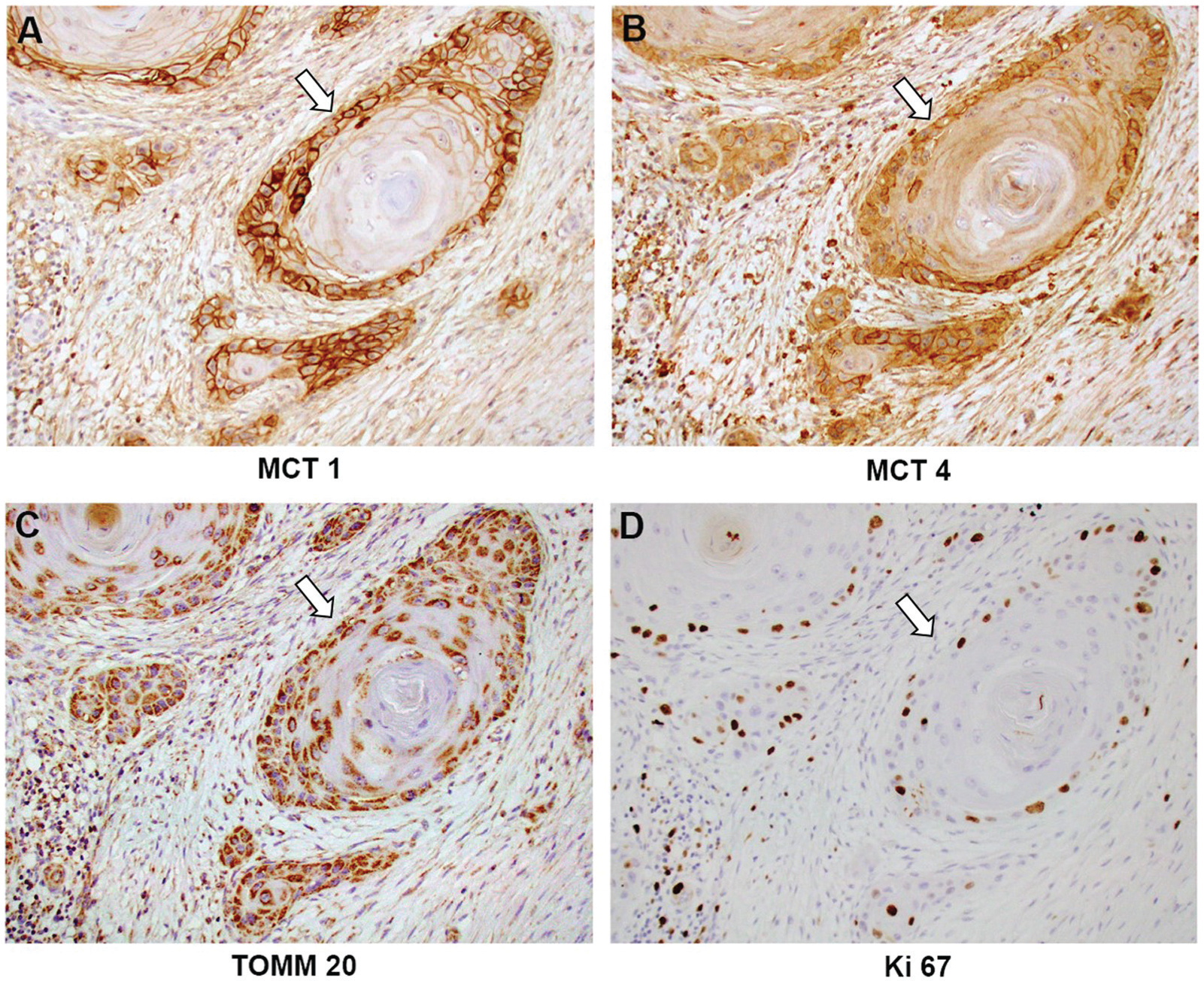
Immunohistochemistry staining (×20 light microscopy) of extracapsular extension of nodal metastasis tumor-stromal interface (white arrows). Note strong monocarboyxlate transporter (MCT) 1 (A), translocase of outer mitochondrial membrane 20 (TOMM20) (C), and Ki-67 (D) at leading edge of carcinoma, with stromal staining for MCT4 (B).
Average Strength of Immunohistochemistry Staining as Determined by Aperio Image Analysis. a
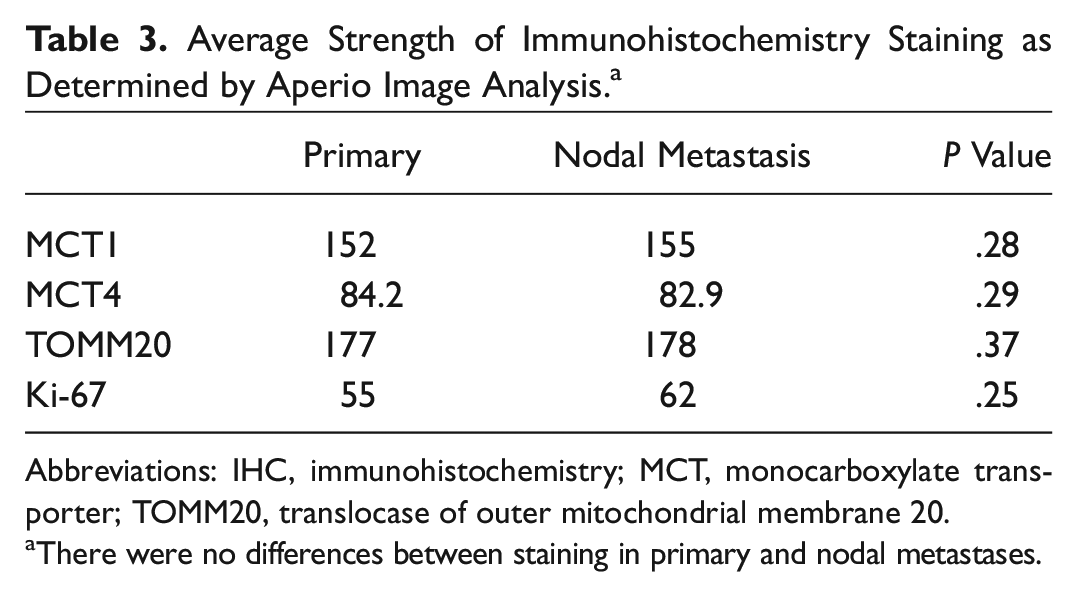
Abbreviations: IHC, immunohistochemistry; MCT, monocarboxylate transporter; TOMM20, translocase of outer mitochondrial membrane 20.
There were no differences between staining in primary and nodal metastases.
Micro- vs macro-ECE
Because one potential mechanism of ECE is that tumor deposits may simply grow larger than the lymph node capsule, size of the largest positive lymph node was evaluated for each patient. Among the macro-ECE group, average lymph node size was 2.93 cm (range, 1-6.5 cm), and among the micro-ECE group, average size was 1.99 cm (range, 1-3.3 cm). Interestingly, this difference in size of the largest lymph node between these groups was significant on t test (P = .03).
Stromal MCT4 was assessed in the lymph nodes at 2 sites: first, the perinodal stroma surrounding areas of ECE and, second, at the perinodal stroma away from sites of ECE. MCT4 staining was significantly stronger in areas of perinodal stroma around ECE than at extranodal sites where the nodal capsule was intact (Aperio value 61.1 vs 82.9, P < .001; Figure 5A , B ). Moreover, MCT4 stromal staining was significantly higher around nodes with macro-ECE compared with micro-ECE (Aperio value 85.3 vs 77.3, P = .01; Figure 5B , C ), suggesting a stronger shift toward glycolytic metabolism in the areas with greater ECE. A receiver operator characteristic curve analysis of perinodal MCT4 values suggested that a value of 82 be used as a cutoff to predict recurrence ( Figure 6A ); patients were thus grouped into high MCT4 (Aperio MCT4 value ≥82) or low MCT4 staining (Aperio MCT4 value <82). Kaplan-Meier curves were generated to compare DFS in high-MCT4 patients and low-MCT4 patients ( Figure 6B ). On univariate log-rank test, high perinodal MCT4 trended toward worsened DFS but did not reach statistical significance (hazard ratio [HR], 2.81; 95% confidence interval [CI], 0.91-8.64; P = .07).
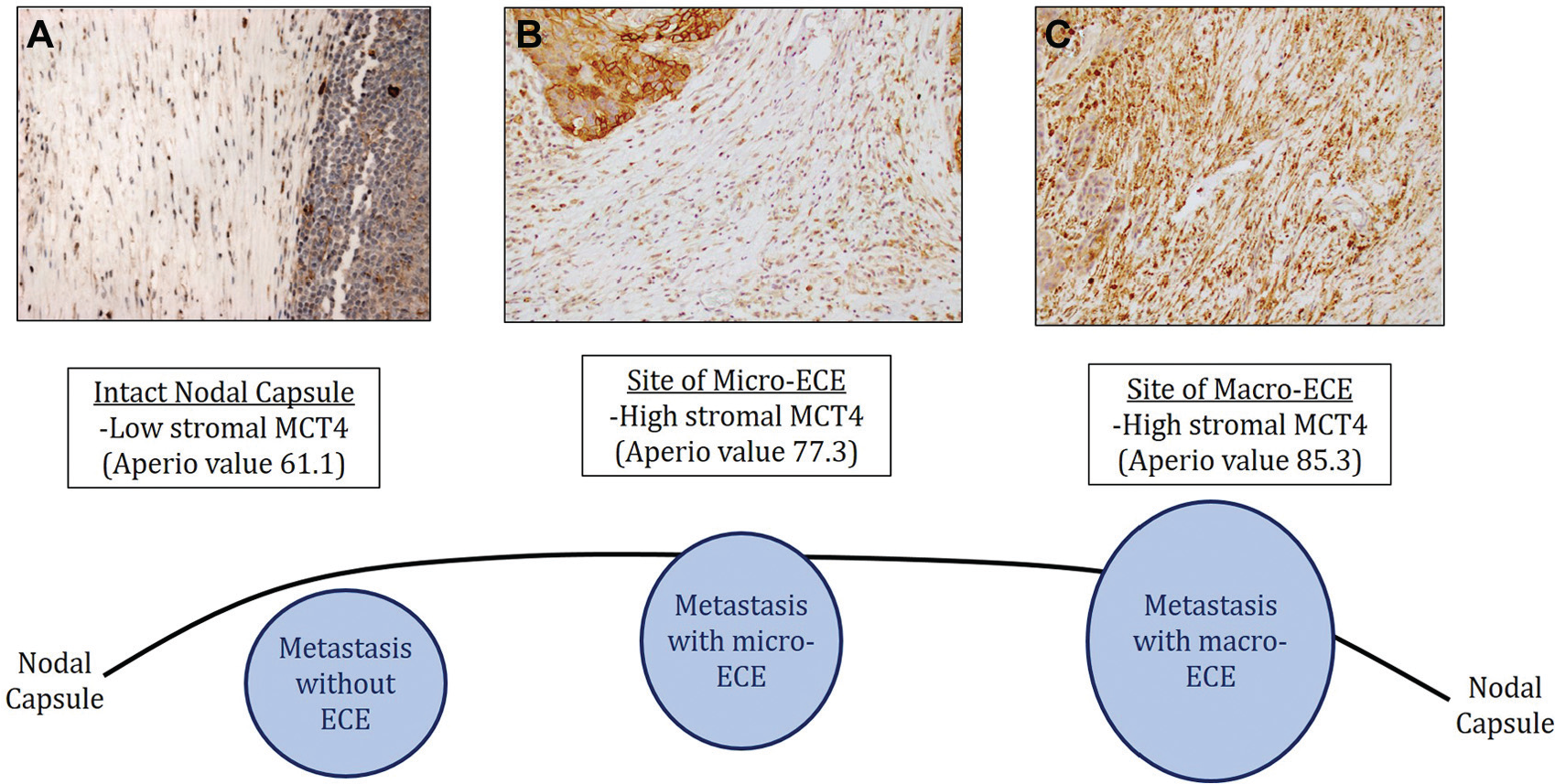
Immunohistochemistry (×20 light microscopy) of stromal monocarboxylate transporter 4 (MCT4) under different conditions, with diagram. At intact nodal capsule (A), fibroblasts stain MCT4 weakly. At micro–extracapsular extension (ECE) (B), fibroblasts stain MCT4 strongly. At macro-ECE, fibroblasts stain MCT4 stronger still.
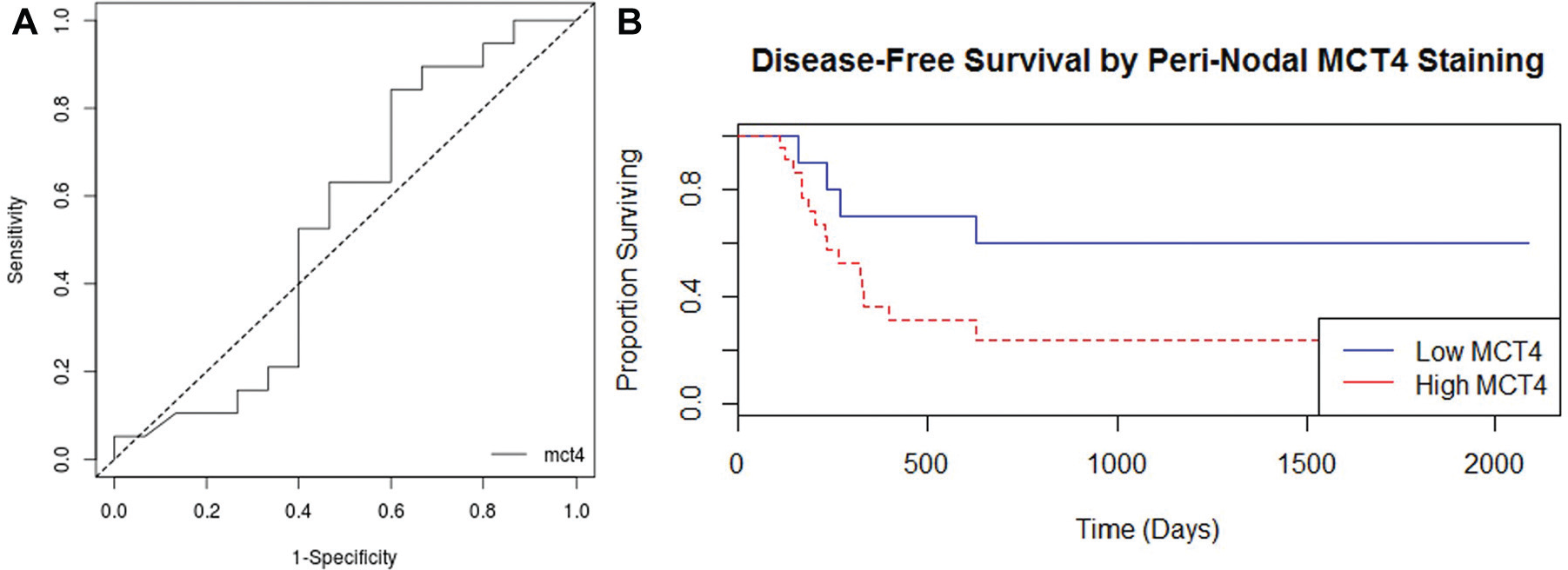
(A) Receiver operator characteristic curve for perinodal monocarboxylate transporter 4 (MCT4). Area under curve: 0.539. Sensitivity: 0.842. Specificity: 0.400. (B) Kaplan-Meier curve for low perinodal MCT4 (Aperio value <82, blue) vs high perinodal MCT4 (Aperio value >82, red).
Likewise, on univariate analysis, age, sex, extent of ECE, T stage, N stage, and presence of PNI did not significantly predict DFS in this population of advanced oral cavity squamous tumors ( Table 2 ). Other IHC markers, including MCT1, Ki-67, and TOMM20, did not have a significant impact on DFS ( Table 2 ).
However, on multivariate analysis, high perinodal MCT4 was a significant predictor of worsened DFS (HR, 6.64; 95% CI, 1.38-32; P = .02; Table 2 ). None of the other variables was significantly associated with worsened DFS, although male sex did approach significance (HR, 2.9; 95% CI, 0.91-9.12; P = .07).
Stromal MCT4 was also measured at primary sites and compared between macro-ECE and micro-ECE groups. While MCT4 staining was higher at the primary site of patients with macro-ECE (mean 85.6 vs 80.8 for micro-ECE), this difference trended toward but did not reach statistical significance (P = .055, not pictured).
Discussion
In this study, we sought to characterize patterns of metabolic coupling in lymph node metastases with ECE and to determine if the metabolic microenvironment predicts clinical behavior. Little work to date has focused on tumor metabolism in HNSCC primary lesions or nodal metastasis; however, there is evidence to suggest that markers of metabolic coupling predict outcomes in HNSCC and other cancers. Previous studies have shown that cancer-associated fibroblasts (CAFs) exist in HNSCC, support metabolic coupling, and play a significant role in tumorigenesis and prognosis.30,31 Our previous work has demonstrated increased expression of MCT4 in CAFs in HNSCC. 26 Increased MCT4 expression in CAFs correlated with a worsened prognosis in oral cavity squamous cell carcinoma.
In this study, increased MCT4 staining in perinodal stroma was identified in areas of ECE; using digital image analysis, a further increase in MCT4 was identified with increasing ECE. Patients with high perinodal MCT4 staining had a worse prognosis compared with those with low perinodal MCT4, establishing perinodal MCT4 as a significant prognosticator on multivariate analysis.
The increase in stromal MCT4 staining is a local effect seen in the region of the extension outside of the node, at regions of contact between the tumor cells and the stroma. This mimics the pattern seen at the primary tumor at the tumor-stromal interface where CAFs are found. In regions of tumor metastasis where the lymph node capsule is intact and interposed between the tumor and stroma, the adjacent stroma appears normal and does not stain strongly for MCT4. This implies that direct contact between the tumor cells and the stroma results in the development of a CAF phenotype as occurs in the primary tumor from fibroblasts already present at or recruited to the site.32,33 Further study would be warranted to investigate this.
The presence of CAFs in the perinodal stroma may be important to the pathogenesis of ECE. CAFs have shown to be critical to the tumor microenvironment in numerous ways, participating in processes such as invasion, angiogenesis, proliferation, metabolism, and metastasis. Insight into perinodal CAFs may provide insight into the mechanism by which ECE relates to worsened prognosis. The abundant recruitment or activation of CAFs may be a critical factor to create Paget’s “fertile soil” for tumorigenesis. Further investigation would be required to definitively determine causality in the relationship between CAFs and the nodal metastasis. However, the results of this study demonstrate that CAFs are present at sites of ECE and that increasing MCT4 staining correlates with increased ECE and worsened DFS.
Previous studies have linked greater extent of ECE with worsened prognosis in oropharyngeal, oral cavity, and laryngeal squamous cell carcinoma.14-16 While the present study failed to show a significant difference in DFS based on extent of ECE, tumors with greater perinodal MCT4 did have significantly worse DFS on multivariate analysis. This population of patients with ECE certainly represents a group of aggressive tumors, and an even more aggressive population was identified by high perinodal MCT4. Traditional predictors of poor outcomes, such as advanced T stage and perineural invasion, may have played less of a role in this population of patients, which has already been identified as a very aggressive subset simply by the presence of ECE. Increased perinodal MCT4 had a significant impact on survival even with this small population of patients, suggesting that it may be a powerful biomarker of aggressive disease.
To our knowledge, no previous study has investigated the metabolic profile of regional HNSCC metastases. In all cases here, the nodal metastases at sites of ECE demonstrated the same staining patterns as the primary tumor; that is, the tumor heterogeneity and metabolic compartmentalization seen on IHC staining in the primary tumor was also identified in the lymph node metastases. In breast cancer, tumor metabolism at primaries differs from sites of distant metastasis. 34 Whether this is also the case in HNSCC is unclear from this study, as only lymphatic metastases and not distant metastases were investigated. Future work could involve other metastatic sites to determine whether metabolic compartmentalization occurs there, as well.
If metabolic coupling is corroborated in future studies, it may be an attractive therapeutic target, especially in patients with aggressive disease. For example, metformin, a metabolically active drug normally used for diabetes mellitus, has been shown to simultaneously decrease the CAF phenotype and increase apoptosis of tumor cells in patients with HNSCC. 35 In population-based studies, metformin improves survival in patients with HNSCC. 36 While no MCT4 inhibitors are commercially available, the MCT1 inhibitor α-cyano-4-hydroxycinnamate (CHC) has been used in vitro to inhibit growth of gliomas and cervical squamous cell carcinoma.37,38 MCT1 inhibitors have not been used in human trials, but laboratory work at least suggests that targeting tumor metabolism has antitumor activity.
The small size of this study necessitates confirmation of the results here in a larger patient population. A greater sample size may allow for increased analysis and comparison between micro- and macro-ECE groups. Additional patient samples would also better define the distribution of MCT4 values seen in perinodal stroma and thereby strengthen a cutoff value to categorize tumor phenotypes.
Conclusion
Metabolic coupling occurs in HNSCC of the oral cavity and oropharynx, at both the primary tumor and at sites of regional lymph node metastasis. With an increasing degree of ECE, there is stronger staining for markers of metabolic coupling, especially MCT4. Greater perinodal MCT4 staining in the stroma around metastatic lymph nodes predicts worse DFS. Further study will be required to define the role of metabolic coupling in ECE and disease behavior, as well as develop therapies targeting tumor metabolism.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.