
Abstract
Objectives
Patient preferences are crucial for the delivery of patient-centered care. Discrete choice experiments (DCEs) are an emerging quantitative methodology used for understanding these preferences. In this study, we employed DCE techniques to understand the preferences of patients presenting for an ear, nose, and throat clinic visit.
Study Design
DCE.
Setting
Decision science laboratory.
Methods
A DCE survey of 5 attributes—wait time, physician experience, physician personality, utilization of visit time, and cost/copayment—was constructed with structured qualitative interviews with patients. The DCE was administered to participants from the general population, who chose among hypothetical scenarios that varied across these attributes. A conditional logit model was used to determine relative attribute importance, with a separate logit model for determining subject effects.
Results
A total of 161 participants were included. Cost/copayment had the greatest impact on decision making (importance, 32.2%), followed by wait time and physician experience (26.5% and 24.7%, respectively). Physician personality mattered least (4.7%), although all attributes were significantly correlated to decision making. Participants preferred doctors who spent more time performing physical examination than listening or explaining. Participants were willing to pay $52 extra to avoid a 4-week delay in appointment time; $87 extra for a physician with 10 years of experience (vs 0 years); and $9 extra for a caring, friendly, and compassionate doctor (vs formal, efficient, and business-like).
Conclusion
DCEs allow for powerful economic analyses that may help physicians understand patient preferences. Our model showed that cost is an important factor to patients and that patients are willing to pay extra for timely appointments, experience, and thorough physical examination.
Keywords
Patients routinely make choices about health care and, in so doing, place implicit value on the goods and services provided to them. Unfortunately, providers often have little insight into patient preferences and their underlying valuation, which can make delivery of patient-centered care more difficult. As defined by the Institute of Medicine, patient-centered care involves “providing care that is respectful of, and responsive to, individual patient preferences, needs and values, and ensuring that patient values guide all clinical decisions.” 1 Because otolaryngology is often focused on providing quality-of-life interventions to patients, otolaryngologists have much to gain from understanding what patients value in clinical and surgical interactions.
Over the past 25 years, stated preference methods have become a commonly accepted means of measuring value in health care. 2 These survey-based techniques are increasingly being used to elicit patient preferences for medical products and services. 3 Within otolaryngology, however, only a few such studies exist: access to acute ear, nose, and throat (ENT) care, 4 polysomnography for pediatric obstructive sleep apnea, 5 hearing aid attributes,6,7 and treatment for vestibular schwannoma 8 have been investigated with stated preference methodologies. Among stated preference methods, discrete choice experiments (DCEs) are particularly useful for eliciting patient preferences by presenting respondents with choices among hypothetical treatment options.
In this study, we examine one of the core health care delivery platforms in otolaryngology—the routine outpatient clinic visit—through the lens of patient preference. By utilizing a DCE, we attempt to quantify the value of several key components of the patient-doctor interaction.
Methods
This study received approval from the Massachusetts Eye and Ear Institutional Review Board. The design and execution were performed in reference to published guidelines within the field of stated preference research.3,9,10
Selection of Attributes and Levels
The selection of attributes began with a literature review of similar studies of patient preferences for clinic visits performed in other specialties.11-13 After compilation of an initial set of attributes, semistructured interviews were conducted among 15 consecutive patients seeking an appointment for ENT complaints. These were conducted before the patient’s appointment had started. Patients were first asked to discuss what attributes of a clinical ENT visit were important to them; then, they were prompted to select the most important factors from both the interview and the literature-determined list of attributes, and these results were tallied. Attribute-specific levels were determined, for continuous variables, by dividing the range between the minimum and maximum expected values (eg, copayment range of $ 0-$120 typically required at our institution) and, for categorical variables, by utilizing qualitative descriptions.
Experimental Design and Pilot Testing
Based on the final list of attributes and levels ( Table 1 ), a hypothetical clinical scenario was constructed in a computer-based format. Participants were asked to imagine that they had a mild sore throat of 6 weeks’ duration, for which over-the-counter medications and primary care consultation had provided no relief. Appropriate background about the purpose of the study was given.
Attributes and Levels of the Discrete Choice Experiment.
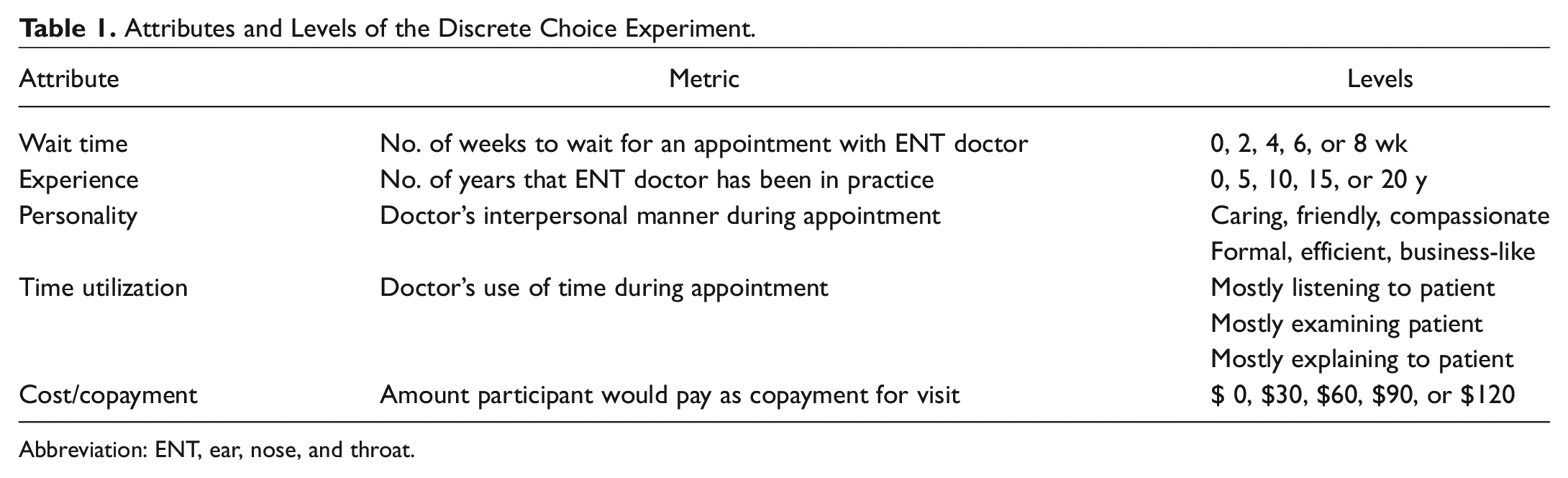
Abbreviation: ENT, ear, nose, and throat.
The survey then asked respondents, in an open-ended and unprompted fashion, to describe what was important in a specialist office visit. For the DCE portion of the survey, a partial-profile design was utilized, as a full-profile design would have included 750 possible combinations. The Discover platform (Sawtooth Software, Orem, Utah) was used to construct these choice sets to ensure balance and efficiency among levels. Fourteen discrete choice sets with 4 profiles were built into each survey ( Figure 1 ). Consequentiality, a measure of internal validity, 14 was assessed by asking participants whether they believed that their responses would be taken into consideration by doctors, hospital administrators, and other patients. Stated comprehension was assessed by asking whether patients understood the survey. Finally, the survey instrument assessed demographic information.
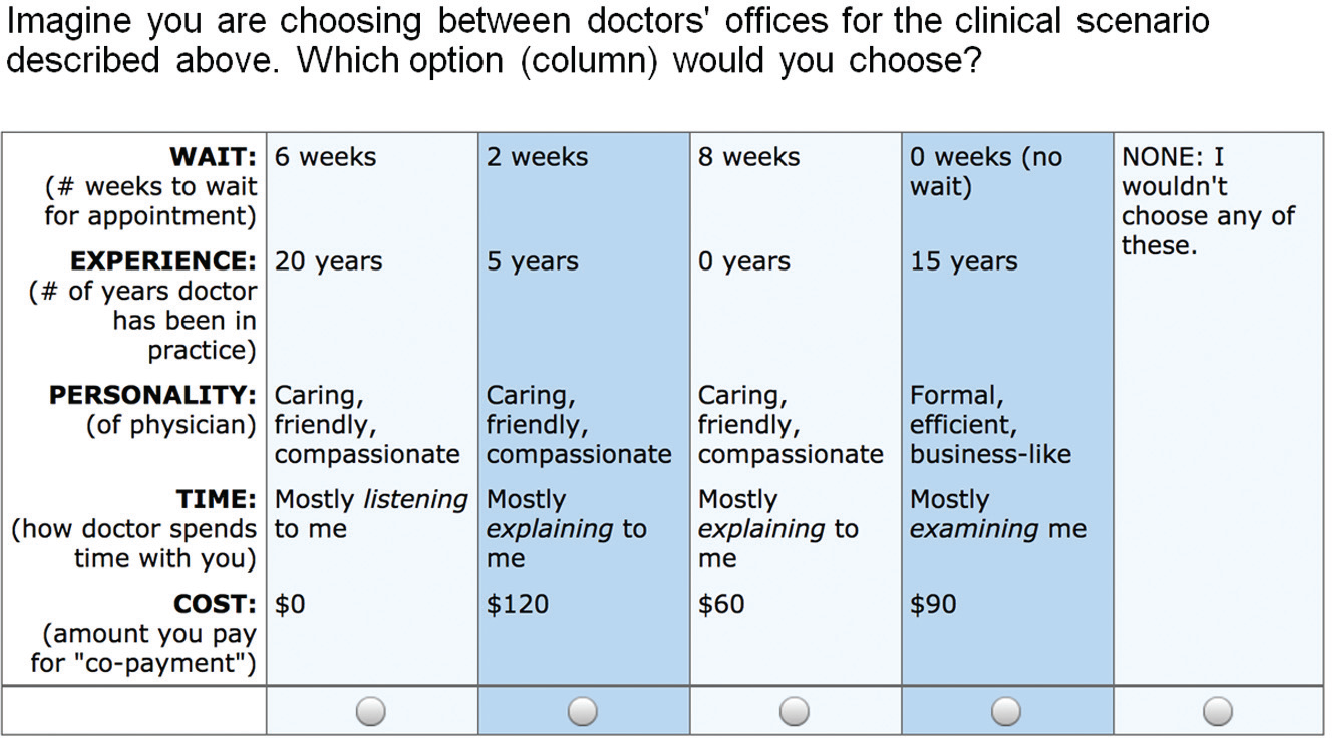
One of 14 discrete choice experiment sets with 4 profiles (columns).
The survey was administered as a pilot test to 15 patients presenting to an otolaryngology clinic at a tertiary referral hospital for throat-related complaints. This pilot was conducted to ensure that the questions were well understood and to elicit feedback on formatting and content. Based on this feedback, the number of cost and experience levels was increased.
Subjects and Data Collection
Subjects were recruited from the general population within eastern Massachusetts from a large established subject pool maintained by the Harvard Decision Science Laboratory. Exclusion criteria were age <18 years old, prisoners, and non-English speakers. Subjects were not permitted to take the survey multiple times.
Data collection was performed with computerized surveys taken in a monitored setting at the laboratory over a period of 5 consecutive days. The 15 patients in the pilot study were not included. Participants were compensated $12 for a completed survey. The goal sample size was 160 to 170 completed surveys, in keeping with other health-related DCEs. 10
Data Analysis
A conditional logistic regression model was used to analyze respondent data. Part-worth utilities were represented by the coefficients in the regression model, and the importance of each attribute—defined as how much difference each attribute made in the participant’s overall utility, expressed as a percentage—was calculated for each respondent and then averaged across the cohort. 15 Marginal willingness to pay (WTP)—a monetary value of change in utility based on incremental alterations in attribute levels—was calculated according to this model for each attribute. Demographic factors were analyzed per logistic regression for association with the utility of the 5 attributes. Tests of validity included consistency of responses in rank order preferences of the attributes, reported consequentiality, and stated comprehension. Statistical significance was set at a type I error threshold of 0.05.
Results
Patient Characteristics
A total of 164 participants took the survey, and 161 of these completed all DCE questions (98.1%). Baseline demographics of the participants are shown in Table 2 . Notably, the population was majority female (55.9%), with an average age of 37 years, with most having attending at least some college. The majority of patients did not have dependent children living within their household (80.7%); 19.4% lived with a chronic medical condition.
Demographic Characteristics of Participants.
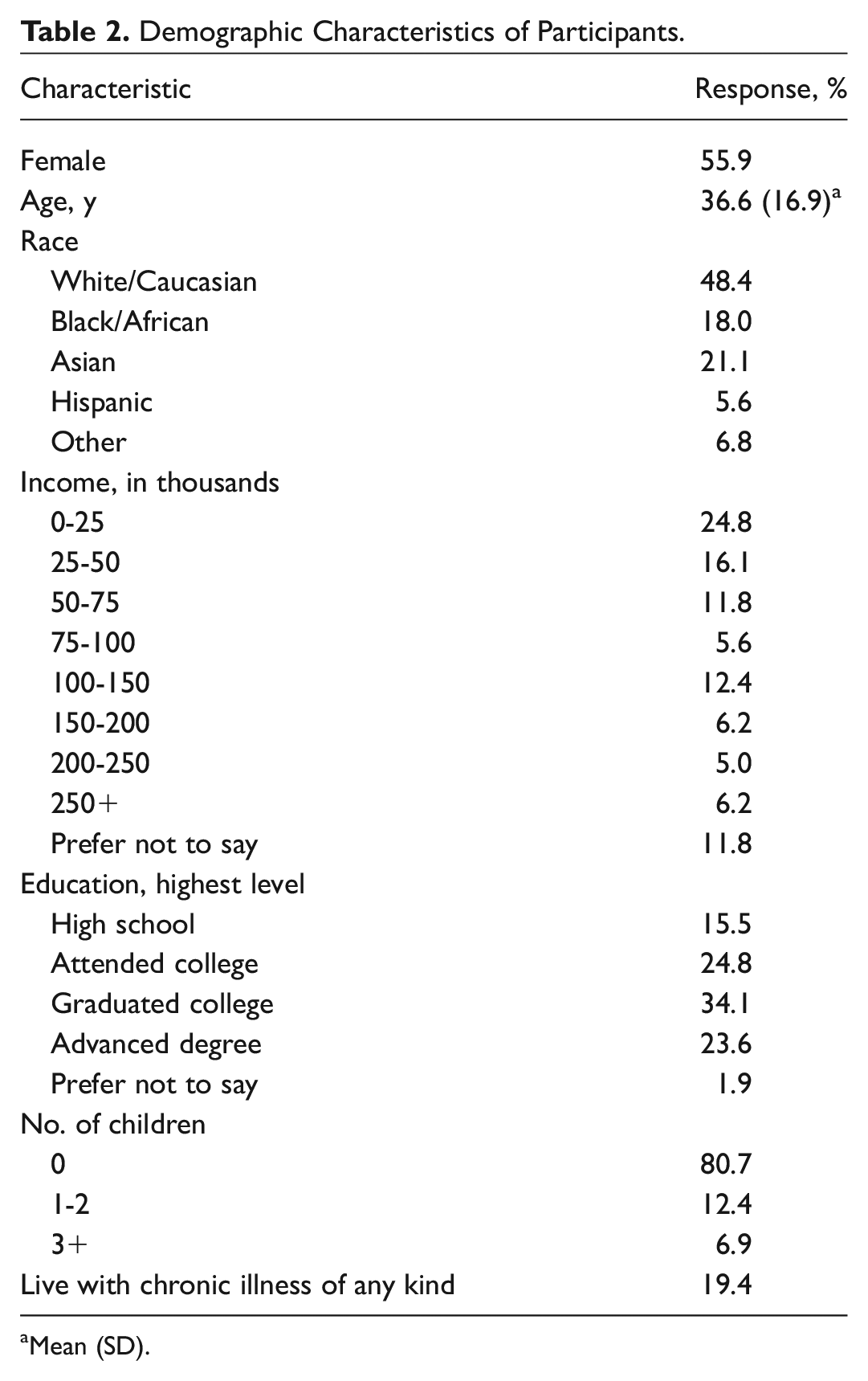
Mean (SD).
Choice Model
Each of the 5 attributes was significant in decision making ( Table 3 ; all P < .05). All were in the expected direction; for example, wait time and cost had negative directionality, indicating decreased overall utility as these attributes increased, whereas physician experience had positive directionality, indicating greater utility within increased physician experience.
Choice Model Based on Conditional Logistic Regression.
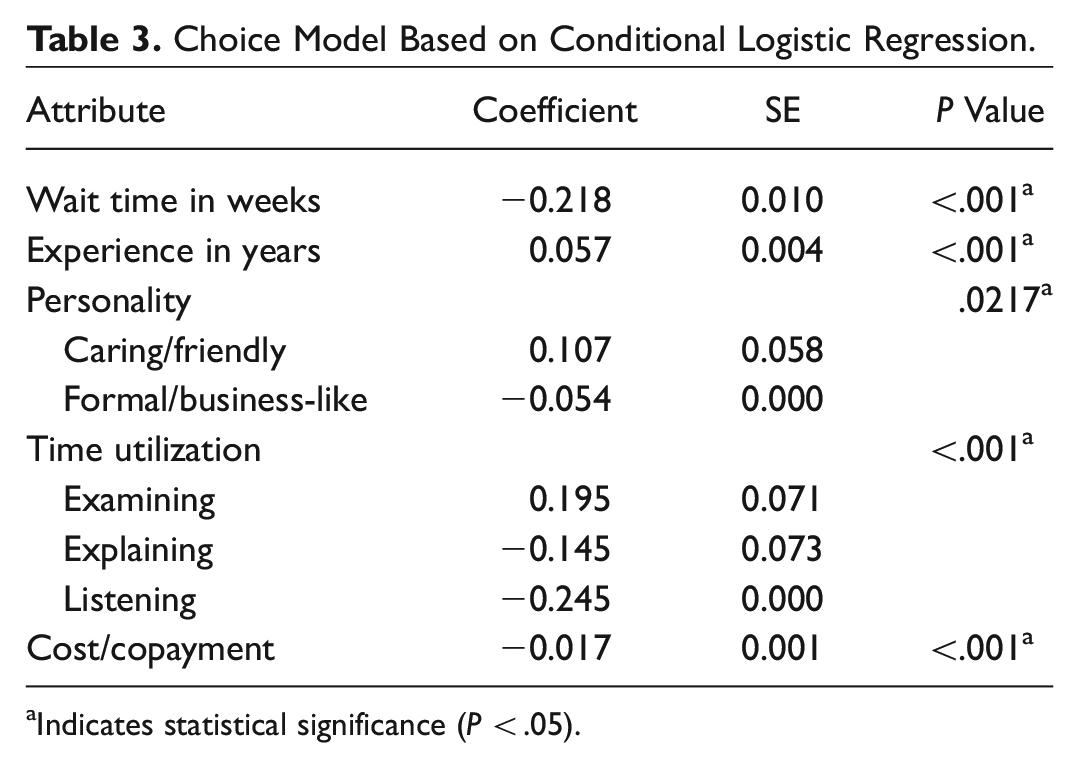
Indicates statistical significance (P < .05).
The relative importance of each attribute is shown in Figure 2 . Cost had the greatest impact on utility in this cohort, with an importance of 32.2%. Wait time and physician experience were also important (26.5% and 24.7%, respectively). Personality of the physician and time utilization were the least important to participants (4.7% and 11.9%, respectively). Within the personality attribute, a caring, friendly, and compassionate physician was preferred to one who was formal, efficient, and business-like ( Figure 3C ). Within the time utilization, patients preferred physicians who perform a thorough examination, as opposed to those who primarily listen or explain ( Figure 3D ).
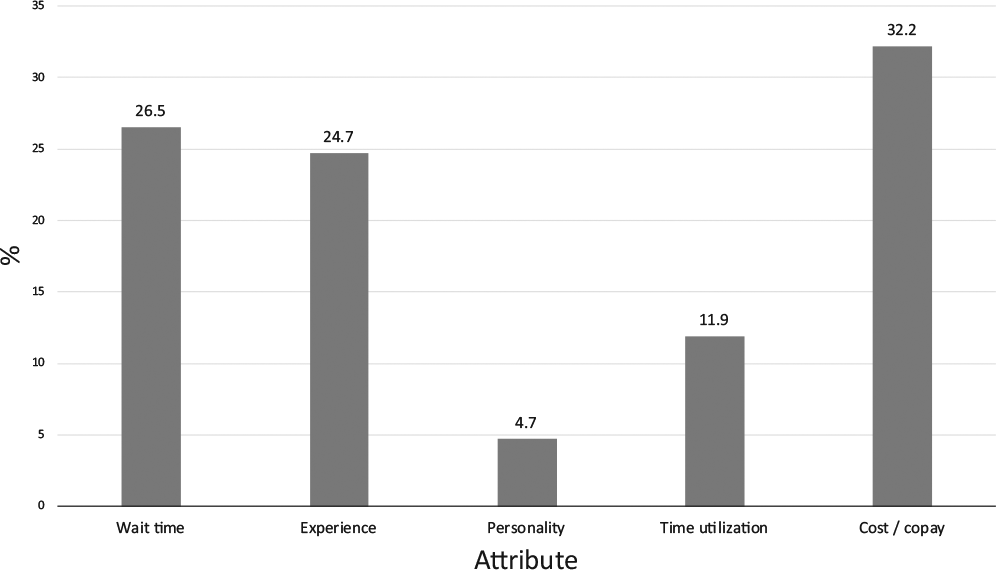
Relative importance of each attribute.
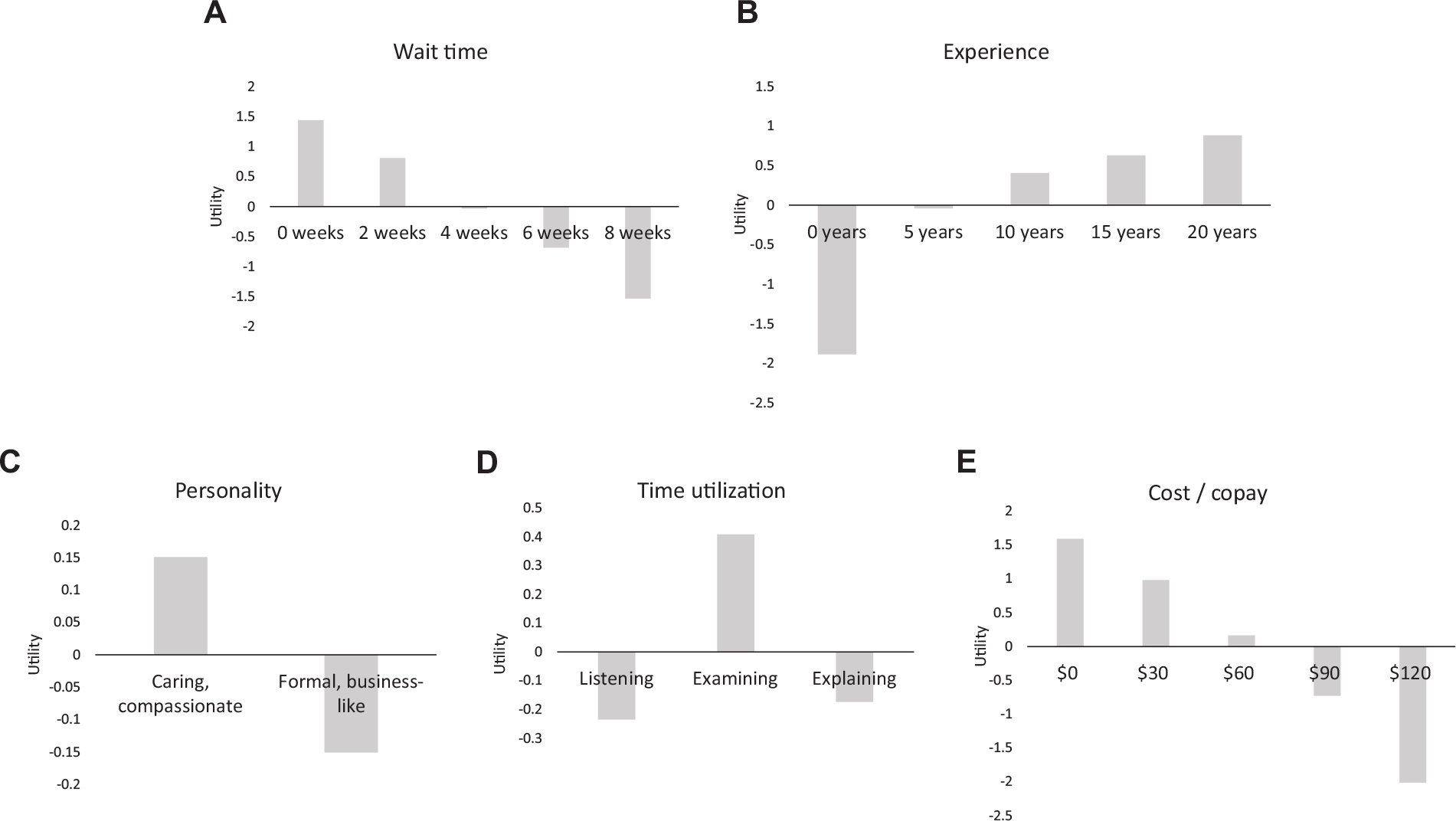
Relative utilities of levels within each attribute: A, wait time; B, experience; C, personality; D, time utilization; E, cost/copay. Higher, positive utilities are preferred to lower, negative utilities.
Demographic characteristics influenced patient preferences. There was a significant interaction between sex and the utilization of time during the clinic visit; women more strongly preferred doctors who examined them (P = .0453), whereas this preference was less pronounced for men. Increasing age was associated with increasing tolerance of wait time (P = .0111). Participants with a higher income more strongly preferred experienced physicians than did those with a lower income (P = .0153). Participants of nonwhite race and those with a college degree were more willing to have an increased wait time (P = .0153 and P = .00250, respectively). Several factors had no significant effect on preferences in the 5 attribute categories, including consequentiality ratings and presence of a chronic illness.
Willingness to Pay
Table 4 illustrates the WTP for incremental changes in attribute levels, keeping all other variables constant. As expected based on importance values, participants were most price sensitive to wait time and experience. WTP to avoid a wait time of 4 weeks was $52, whereas to avoid an 8-week delay it was $99. Subjects were clearly willing to pay for experience, but notably this plateaued at 10 years. Participants preferred a caring and compassionate physician but were willing to pay only a small amount for this ($9).
Willingness to Pay for Changes in Attributes. a
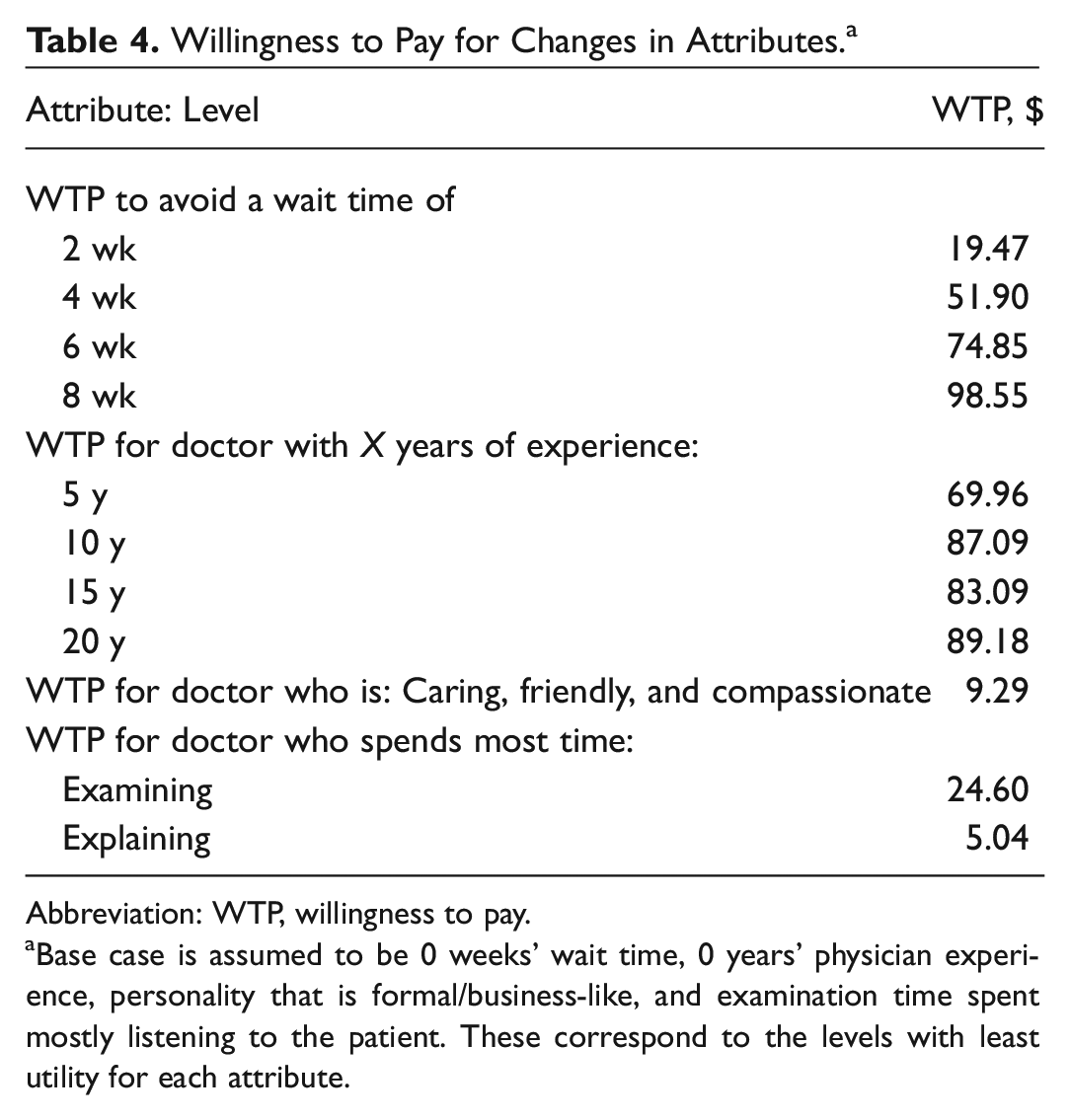
Abbreviation: WTP, willingness to pay.
Base case is assumed to be 0 weeks’ wait time, 0 years’ physician experience, personality that is formal/business-like, and examination time spent mostly listening to the patient. These correspond to the levels with least utility for each attribute.
Validity
Preferences conformed with several principles of internal validity. 14 As seen in Figure 3 , preferences were monotonic across the numeric attributes (wait time, experience, cost/copay); that is, respondents did not prefer worse levels to better levels within an attribute, ceteris paribus. All participants indicated that they understood the format and content of the DCE. Belief in the consequentiality of the survey was high, with 81.5% of participants stating that their answers in the DCE would likely be useful to researchers. The reliability of responses was mixed: in 42.3% of cases, the most important attribute as individually measured with the DCE matched the stated importance as assessed by simple ranking of attributes by the participant, although it is unclear to what degree preferences may have changed during the experiment.
Discussion
For otolaryngology clinic visits, the cost of copayment for the visit, the wait time to see a physician, and the physician’s experience were the most important attributes identified by a sample of 161 members of the general public. Less important were the physician’s personality and the time utilization during the clinic visit, although there was a clear preference for physicians who performed a thorough physical examination. Subjects in this group are willing to pay an extra $52 to avoid a 4-week delay in appointment time, $87 extra for a physician with 10 years of experience (as opposed to 0 years), and $9 extra for a doctor who was caring, friendly, and compassionate. Notably, respondents were willing to pay for increased physician experience up to 10 years; WTP for additional experience after 10 years leveled off. We speculate that experience has diminishing returns to the participants in this survey.
When participants were asked to simply rank the most important of the 5 tested attributes, cost/copayment was rated as the most important attribute by 17.3% of participants, whereas experience was ranked as the most important by 40.5%, which represented the plurality. However, after analysis of the DCEs, cost/copayment was calculated as the most important attribute for 49.1% of participants (vs 20.9% for experience), and it had the highest importance score overall ( Figure 2 ). Previous research has demonstrated that patients may make decisions based on price more than they admit to in simple surveys. 16 For participants who might otherwise be unwilling to place a dollar value on their health and treatment options, DCEs help uncover preferences about money and value indirectly. 17
Our results mirror studies performed in other fields of medicine. A study of primary care patients in the United Kingdom 18 demonstrated that a thorough examination was most valuable to patients, with an incremental WTP of $41, whereas WTP for a physician with a friendly manner was $9. A similar study in the United States demonstrated that technical abilities, rather than interpersonal skills, are more valued in primary care visits. 19 Specialty care has also been studied with stated preference techniques. Wong et al demonstrated that within the field of cancer care, the expertise of the doctor was a significant determinant of value; cancer patients were willing to pay up to $680 for a visit with a specialist. 11 Dermatology patients were found to be willing to wait 2.1 months extra to be seen by a physician with at least 5 years of specialty-specific experience, 12 and previous research from our group demonstrated a strong preference among otolaryngology patients for direct access to specialists in urgent and emergent situations (WTP of $340 per visit).4,20 WTP may vary per country, however; only 19% of self-referred emergency room patients in the Netherlands were willing to pay >50 euros in copayment. 21
Much of these results will be unsurprising to otolaryngologists. Expertise, wait time, and the interpersonal skills of the physician are expected to be important to patients. (Indeed, the goal of qualitative interviewing and pilot testing at the commencement of this project was to rule out unimportant attributes.) But DCEs allow a ranking of the relative importance of these factors in patient decision making—to understand the trade-offs that patients are willing to make and to define the value of individual attributes in monetary terms.2,22 Establishing this value could shape how otolaryngology is practiced. For example, this type of research could be particularly helpful in determining the relative value that patients assign to seeing an attending physician, rather than a resident or physician assistant.
Over the past decade, there has been increasing interest in value-based care and more economic analysis of existing health care programs.23,24 Stated preference research complements this burgeoning field through the elicitation of patient preferences and valuation of health outcomes. On a large scale, such research could inform value-based reimbursements from payers; on a smaller scale, individual practices can use patient preferences to change aspects of care delivery, such as wait times, time utilization, and cost, in an effort to make health care more consumer driven. Otolaryngologists also have the potential to make care more patient-centric by improving key attributes of the outpatient clinic visit, whether by reducing wait times, emphasizing the experience of more senior physicians, or focusing the appointment on physical examination. Finally, the extension of DCEs into goods with out-of-pocket costs, such as hearing aids7,25 or medications for nasal congestion,26,27 has clear implications for product development and pricing.
There are several limitations to this study. We used a convenience sample of volunteers who were younger and more well educated than a typical patient, with a higher proportion of women than men. This limits generalizability to the general population (all of whom are presumed to be potential patients in an otolaryngology clinic). Additionally, although our measures of validity were strong, the measures of reliability demonstrated that the most important stated attribute (experience, in a simple ranking question) and the most important calculated attribute (cost/copay, from DCE questions) matched in only 42.3% of cases. We hypothesize that this may be due to the unwillingness of participants to state explicitly that cost was an important factor. Finally, framing issues continue to be a point of debate in stated preference research, as changes to the presentation of the scenario, attributes, and levels can change the outcome of the experiment.3,28 Appropriate interviewing, pilot testing, literature review, and review by experts were performed in this study to minimize this potential limitation.
Conclusion
Our DCE shows that cost is an important factor to potential patients when considering an otolaryngologist. Patients are willing to pay for otolaryngologists who offer timely appointments, experience, and a thorough physical examination. DCEs enable powerful economic analyses of patient preferences, allowing researchers to quantify the value of health care goods and services. Additional investigation is necessary to further value the care that otolaryngologists provide to patients.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We thank the Harvard Decision Science Laboratory at the John F. Kennedy School of Government for the use of its facilities.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was accepted for presentation at the 2017 AAO-HNSF Annual Meeting & OTO Experience; September 10-13, 2017; Chicago, Illinois.