
Abstract
The American Academy of Otolaryngology—Head and Neck Surgery Foundation has published a supplement to this issue of Otolaryngology–Head and Neck Surgery featuring the “Clinical Practice Guideline: Evaluation of the Neck Mass in Adults.” To assist in implementing the guideline recommendations, this article summarizes the rationale, purpose, and key action statements. The 12 recommendations developed emphasize reducing delays in diagnosis of head and neck squamous cell carcinoma; promoting appropriate testing, including imaging, pathologic evaluation, and empiric medical therapies; reducing inappropriate testing; and promoting appropriate physical examination when cancer is suspected.
Neck masses are common in adults, but often the underlying etiology is not easily identifiable. While infections cause most of the neck masses in children, most persistent neck masses in adults are neoplasms. Malignant neoplasms far exceed any other etiology of adult neck mass.1-3
As used in this guideline, a neck mass is defined as an abnormal lesion (congenital or acquired) that is visible, palpable, or seen on an imaging study. The guideline development group (GDG) further qualified neck masses as any mass below the mandible, above the clavicle, and deep to the skin, although it may involve the overlying skin secondarily. Neck masses may develop from infectious, inflammatory, congenital, traumatic, benign, or malignant neoplastic processes. Importantly, an asymptomatic neck mass may be the initial or only clinically apparent manifestation of head and neck cancer, such as squamous cell carcinoma (HNSCC), lymphoma, or thyroid or salivary gland cancer. Evidence suggests that a neck mass in the adult patient should be considered malignant until proven otherwise.1-8
Timely diagnosis of a neck mass due to metastatic HNSCC is paramount because delayed diagnosis directly affects tumor stage and worsens prognosis.9-11 Unfortunately, despite substantial advances in testing modalities over the last few decades, diagnostic delays are common. Forty years ago, patients with a neck mass experienced an average of a 5- to 6-month delay from the time of initial presentation to the diagnosis of malignancy. 12 Today, studies continue to report delays as long as 3 to 6 months.13-15
The epidemiology and clinical presentation of mucosal HNSCC have changed recently. Coupled with the substantial morbidity and mortality of this disease, metastatic mucosal HNSCC is the focus of this guideline. However, a malignant neck mass can result from other disease entities, including lymphoma and skin, thyroid, and salivary gland cancer. The workup outlined in the action statements of this guideline may be applied to any cancer that has metastasized to the neck without an obvious primary.
Mucosal HNSCC may originate in the oral cavity, oropharynx, hypopharynx, nasopharynx, or larynx. Occult metastatic spread from the primary cancer to the regional lymph nodes and continued tumor growth within the lymph nodes result in a neck mass. In 2016, an estimated 62,000 people will be diagnosed with HNSCC. 16 The incidence of HNSCC of the oropharynx particularly is on the rise—in part as a consequence of infection with the human papilloma virus (HPV). For these reasons, expediting the diagnosis of HNSCC is the principal quality improvement opportunity of this guideline.
The incidence of HPV-positive HNSCC of the oropharynx has more than doubled, whereas the incidence of HPV-negative cancers has decreased by half. 17 The rate of HPV-positive HNSCC of the oropharynx (tonsil and base of tongue) is rising so rapidly that by 2020 the incidence of HPV-positive oropharyngeal cancer is estimated to exceed that of HPV-positive uterine cervical cancer.18,19 Patients affected with HPV-positive oropharyngeal HNSCC often present with neck metastasis without an obvious primary malignancy. Two features of HPV-positive HNSCC may contribute to delayed diagnosis. First, as compared with patients with traditional HNSCC, which is HPV negative, patients with HPV-positive tumors are younger and often lack tobacco and alcohol exposure, the 2 most common classic risk factors. Second, because cervical metastases from HPV-positive HNSCC may be cystic, they are often mistaken for branchial cleft cysts, further contributing to delay in diagnosis.20,21
Currently, there is only 1 evidence-based clinical practice guideline to assist clinicians in evaluating an adult with a neck mass. 8 Additionally, much of the available information is fragmented, disorganized, or focused on specific etiologies. In addition, although there is literature related to the diagnostic accuracy of individual tests, there is little guidance about rational sequencing of tests in the course of clinical care. This guideline strives to bring a coherent, evidence-based, multidisciplinary perspective to the evaluation of the neck mass with the intention to facilitate prompt diagnosis and enhance patient outcomes.
Guideline Purpose
The primary purpose of this guideline is to promote the efficient, effective, and accurate diagnostic workup of neck masses to ensure that adults with potentially malignant disease receive prompt diagnosis and intervention to optimize outcomes. Specific goals include reducing delays in diagnosis of HNSCC; promoting appropriate testing, including imaging, pathologic evaluation, and empiric medical therapies; reducing inappropriate testing; and promoting appropriate physical examination when cancer is suspected.
The target patient for this guideline is anyone ≥18 years with a neck mass. The target clinician for this guideline is anyone who may be the first clinician whom a patient with a neck mass encounters. This includes clinicians in primary care, dentistry, and emergency medicine, as well as pathologists and radiologists who have a role in diagnosing neck masses. This guideline does not apply to children.
This guideline addresses the initial broad differential diagnosis of a neck mass in an adult. However, the intention is only to assist the clinician with a basic understanding of the broad array of possible entities. The intention is not to direct management of a neck mass known to originate from thyroid, salivary gland, mandibular, or dental pathology as management recommendations for these etiologies already exist.22,23 This guideline also does not address the subsequent management of specific pathologic entities, as treatment recommendations for benign and malignant neck masses can be found elsewhere.23,24 Instead, this guideline is restricted to addressing the appropriate workup of an adult patient with a neck mass that may be malignant to expedite diagnosis and referral to a head and neck cancer specialist.
The GDG sought to craft a set of actionable statements relevant to diagnostic decisions made by a clinician in the workup of an adult patient with a neck mass. Furthermore, where possible, the GDG incorporated evidence to promote high-quality and cost-effective care.
Methods
General Methods
This guideline was developed with an explicit and transparent a priori protocol for creating actionable statements based on supporting evidence and the associated balance of benefit and harm as outlined in the third edition of the American Academy of Otolaryngology—Head and Neck Surgery Foundation’s (AAO-HNSF’s) guideline development manual. 25 The GDG consisted of 21 panel members representing experts in advanced practice nursing, clinical pathology, consumer advocacy, emergency medicine, general practice medicine, general surgery, head and neck surgery and oncology, otolaryngology, oral and maxillofacial surgery, physician assistants, and radiology.
Literature Search
The recommendations in this clinical practice guideline are based on systematic reviews identified by a professional information specialist using an explicit search strategy. Additional background evidence included randomized controlled trials (RCTs) and observational studies, as needed, to supplement the systematic reviews or to fill gaps when a review was not available. An information specialist conducted 2 systematic literature searches from December 2015 through February 2016 using a validated filter strategy to identify clinical practice guidelines, systematic reviews, RCTs, and comparative studies. The following search terms were used: (“Neck”[mh] AND “Cysts”[mh]) OR (“neck mass”[tiab] OR “neck masses”[tiab] OR “neck lesion”[tiab] OR “neck lesions”[tiab] OR “neck cyst”[tiab] OR “neck cysts”[tiab] OR “neck lump”[tiab] OR “neck lumps”[tiab] OR “neck swelling”[tiab] OR “cystic neck”[tiab] OR “lateral adenopathy”[tiab] OR “cervical lymphadenopathy”[tiab] OR “salivary gland lesion”[tiab] OR “salivary gland lesions” [tiab] OR “neck growth”[tiab] OR “neck growths”[tiab] OR “neck abscess”[tiab] OR “neck abscesses”[tiab]) AND (“Diagnostic Imaging”[mh] OR “Diagnosis, differential”[mh] OR “differential diagnosis”[tiab] OR “diagnosis”[Subheading] OR “Biopsy”[mh] OR “fine needle”[tiab] OR FNAB[tiab] OR imaging[tiab] OR measurement[tiab] OR examination[tiab] OR assessment[tiab] OR evaluation[tiab] OR diagnosis[tiab] OR “Delayed Diagnosis”[mh] OR “delayed diagnosis”[tiab] OR “diagnostic delay”[tiab] OR misdiagnosis[tiab] OR misdiagnosed[tiab] OR “missed diagnosis”[tiab] OR workup[tiab] OR “work-up”[tiab] OR “Referral and Consultation”[mh] OR referral[tiab] OR referrals[tiab] OR identification[tiab]) AND (“1980/01/01”[PDAT] : “2016/12/31”[PDAT]) NOT (“child”[mh] OR child[tiab] OR childhood[tiab] OR children[tiab] OR “pediatrics”[Mh] OR pediatric[tiab] OR paediatric[tiab] OR “infant”[Mh] OR infant[tiab] OR infants[tiab] OR infantile[tiab] OR prenatal[tiab] OR perinatal[tiab] OR fetal[tiab]) AND (“Practice Guideline”[ptyp] AND systematic[sb] AND (Randomized Controlled Trial[ptyp] OR randomized[tiab] OR randomised[tiab]); (“Head and Neck Neoplasms/epidemiology”[Mesh] OR “Head and Neck Neoplasms/etiology”[mh] OR “Head and Neck Neoplasms/diagnosis”[mh]) AND (“Papillomaviridae”[Mesh] OR “human papillomavirus” [tiab] OR hpv[tiab] or “HPV-mediated”[tiab] OR “HPV-associated”[tiab] OR “HPV-related”[tiab]) AND (“1980/01/01”[PDAT] : “2016/12/31”[PDAT]) NOT (“child”[mh] OR child[tiab] OR childhood[tiab] OR children[tiab] OR “pediatrics”[Mh] OR pediatric[tiab] OR paediatric[tiab] OR “infant”[Mh] OR infant[tiab] OR infants[tiab] OR infantile[tiab] OR prenatal[tiab] OR perinatal[tiab] OR fetal[tiab]) AND “Practice Guideline”[ptyp] AND systematic[sb] (Randomized Controlled Trial[ptyp] OR randomized[tiab] OR randomised[tiab]) AND (Comparative Study[ptyp] OR comparative[tiab])
The English-language searches were performed in multiple databases, including PubMed (MEDLINE), EMBASE, CINAHL, Cochrane Library, National Guideline Clearinghouse, NICE UK, and CMA Infobase (Canada). In certain instances, targeted searches for lower-level evidence were performed to address gaps from the systematic searches identified in writing the guideline from April 2016 through November 2016.
The initial search for clinical practice guidelines identified 11 guidelines. After removal of duplicates and irrelevant references, the total was 6 guidelines. Quality criteria for including guidelines were (a) an explicit scope and purpose, (b) multidisciplinary stakeholder involvement, (c) systematic literature review, (d) explicit system for ranking evidence, and (e) explicit system for linking evidence to recommendations. The final data set retained 3 guidelines that met inclusion criteria.
The initial search for systematic reviews identified 103 systematic reviews or meta-analyses. After removal of duplicates and irrelevant references, the total was 27 articles. Quality criteria for including reviews were (a) relevance to the guideline topic, (b) clear objective and methodology, (c) explicit search strategy, and (d) valid data extraction methods. The final data set retained was 10 systematic reviews or meta-analyses that met inclusion criteria.
The initial search for RCTs identified 20 RCTs. After removal of duplicates and irrelevant references, the total was 14 articles. Quality criteria for including RCTs were (a) relevance to the guideline topic, (b) publication in a peer-reviewed journal, and (c) clear methodology with randomized allocation to treatment groups. The total final data set retained 6 RCTs that met inclusion criteria.
The initial search for comparative studies identified 143 studies. After removal of duplicates and irrelevant references, the total was 140 articles. The quality criterion for including comparative studies was relevance to the guideline topic. The total final data set retained 51 comparative studies that met inclusion criteria.
In a series of conference calls, the GDG defined the scope and objectives of the proposed guideline. During the 12 months devoted to guideline development ending in August 2016, the GDG met twice, with in-person meetings following the format previously described 25 and using electronic decision-support software (BRIDGE-Wiz; Yale Center for Medical Informatics, New Haven, Connecticut) to facilitate creating actionable recommendations and evidence profiles. 26 Internal electronic review and feedback on each guideline draft were used to ensure accuracy of content and consistency with standardized criteria for reporting clinical practice guidelines. 27
AAO-HNSF staff used the Guideline Implementability Appraisal and Extractor to appraise adherence of the draft guideline to methodological standards, to improve clarity of recommendations, and to predict potential obstacles to implementation. 28 Guideline panel members received summary appraisals in September 2016 and modified an advanced draft of the guideline.
The final guideline draft underwent extensive external peer review, including a period for open public comment. All comments received were compiled and reviewed by the panel’s chair, and a modified version of the guideline was distributed and approved by the GDG. The recommendations contained in the guideline are based on the best available data published through April 2016. Where data were lacking, a combination of clinical experience and expert consensus was used. A scheduled review process will occur at 5 years from publication or sooner if new compelling evidence warrants earlier consideration.
Classification of Evidence-Based Statements
Guidelines are intended to reduce inappropriate variations in clinical care, to produce optimal health outcomes for patients, and to minimize harm. The evidence-based approach to guideline development requires that the evidence supporting a policy be identified, appraised, and summarized and that an explicit link between evidence and statements be defined. Evidence-based statements reflect both the quality of evidence and the balance of benefit and harm that is anticipated when the statement is followed. The definitions for evidence-based statements are listed in Tables 1 and 2 .
Strength of Action Terms in Guideline Statements and Implied Levels of Obligation.
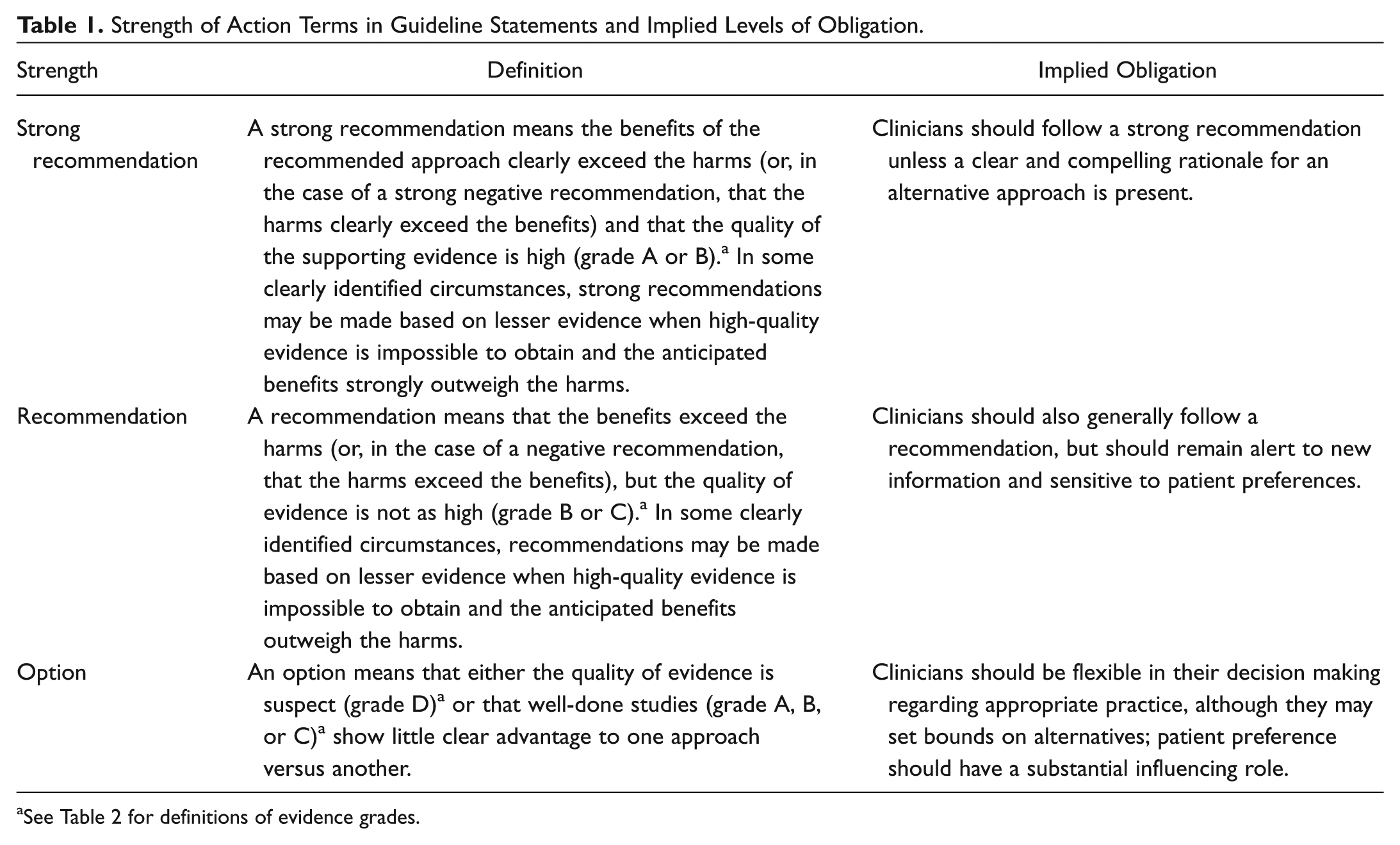
See Table 2 for definitions of evidence grades.
Aggregate Grades of Evidence by Question Type. a
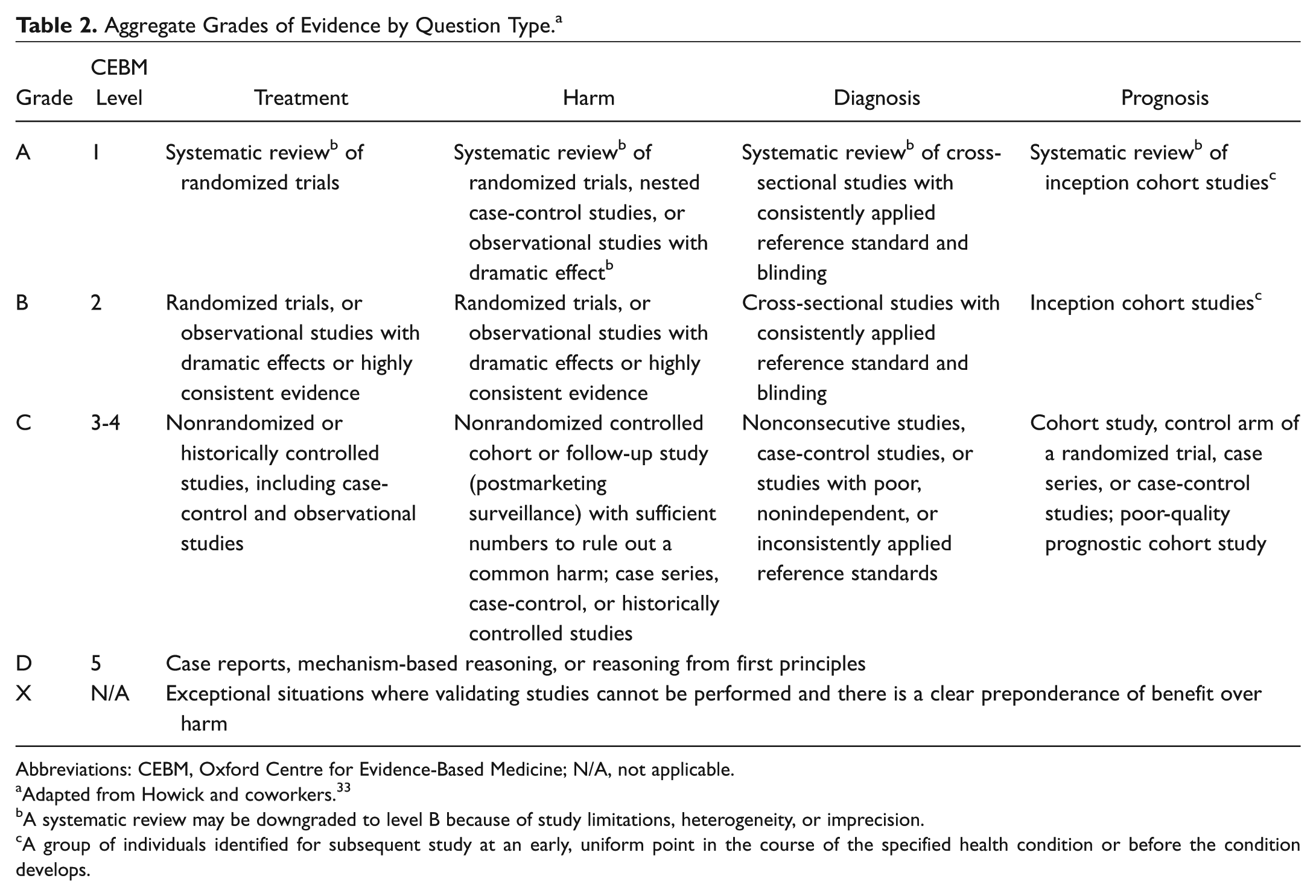
Abbreviations: CEBM, Oxford Centre for Evidence-Based Medicine; N/A, not applicable.
Adapted from Howick and coworkers. 33
A systematic review may be downgraded to level B because of study limitations, heterogeneity, or imprecision.
A group of individuals identified for subsequent study at an early, uniform point in the course of the specified health condition or before the condition develops.
Guidelines are never intended to supersede professional judgment; rather, they may be viewed as a relative constraint on individual clinician discretion in a particular clinical circumstance. Less frequent practice variation is expected for a strong recommendation than might be expected with a recommendation. Options offer the most opportunity for practice variability. 29 Clinicians should always act and decide in a way that they believe will best serve their individual patients’ interests and needs, regardless of guideline recommendations. Guidelines represent the best judgment of a team of experienced clinicians and methodologists addressing the scientific evidence for a particular topic. 30
Making recommendations about health practices involves value judgments on the desirability of various outcomes associated with management options. Values applied by the GDG sought to minimize harm and diminish unnecessary and inappropriate therapy. A major goal of the panel was to be transparent and explicit about how values were applied and to document the process.
Financial Disclosure and Conflicts of Interest
The cost of developing this guideline, including travel expenses of all panel members, was covered in full by the AAO-HNSF. Potential conflicts of interest for all panel members in the past 5 years were compiled and distributed before the first conference call and were updated at each subsequent call and in-person meeting. After review and discussion of these disclosures, 31 the panel concluded that individuals with potential conflicts could remain on the panel if they (1) reminded the panel of potential conflicts before any related discussion, (2) recused themselves from a related discussion if asked by the panel, and (3) agreed not to discuss any aspect of the guideline with industry before publication. Last, panelists were reminded that conflicts of interest extend beyond financial relationships and may include personal experiences, how a participant earns a living, and the participant’s previously established “stake” in an issue. 32
Guideline Key Action Statements
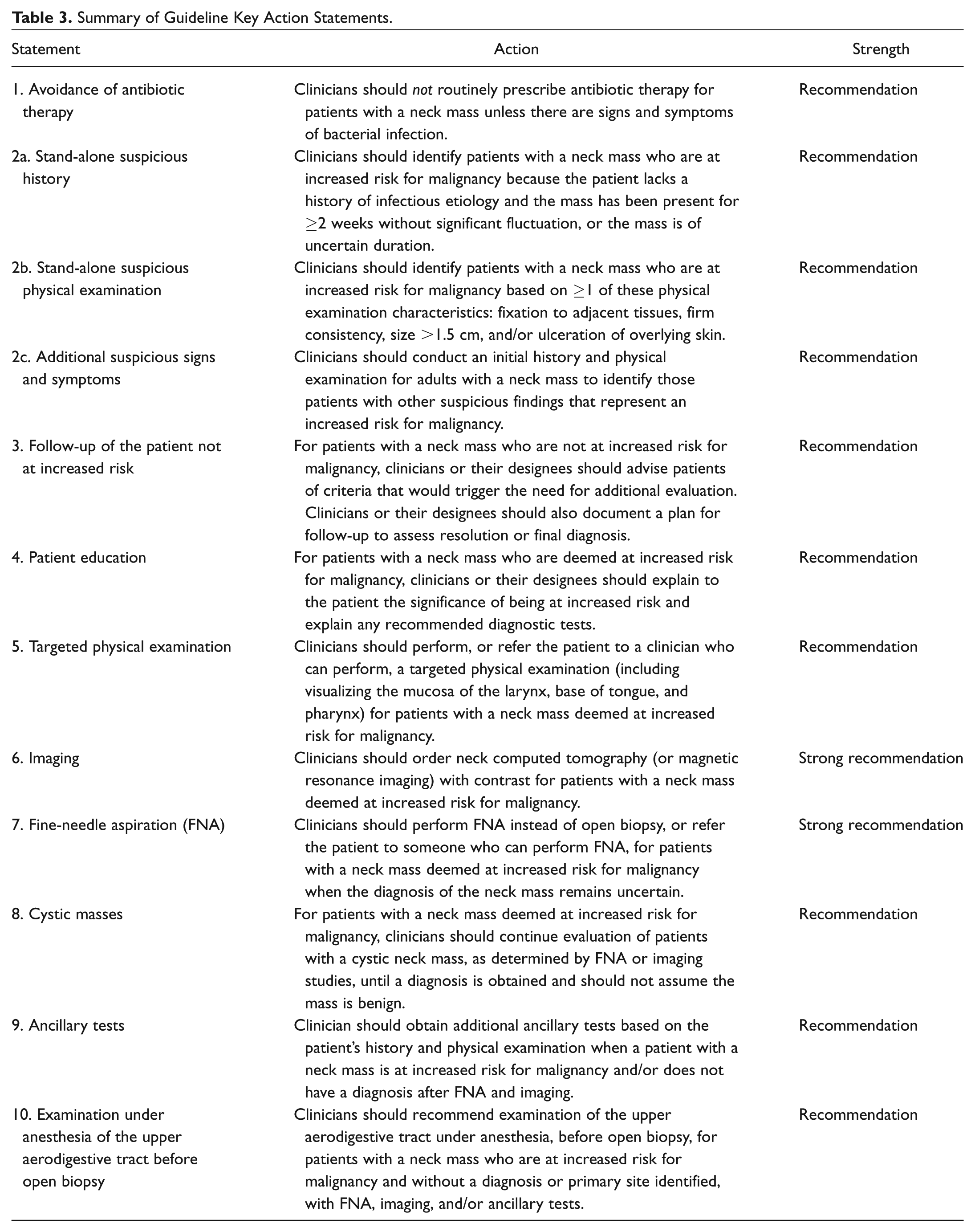
Each evidence-based statement is organized in a similar fashion: a key action statement in bold, followed by the strength of the recommendation in italics. Each key action statement is followed by an “action statement profile” that explicitly states the quality improvement opportunity, aggregate evidence quality, level of confidence in evidence (high, medium, low), benefit, harms, risks, costs, and a benefits-harm assessment. Additionally, there are statements of any value judgments, the role of patient preferences, clarification of any intentional vagueness by the panel, exceptions to the statement, any differences of opinion, and a repeat statement of the strength of the recommendation. Several paragraphs subsequently discuss the evidence base supporting the statement. An overview of each evidence-based statement in this guideline can be found in Table 3 , and the relationship among the statements is depicted in Figure 1 .
Summary of Guideline Key Action Statements.
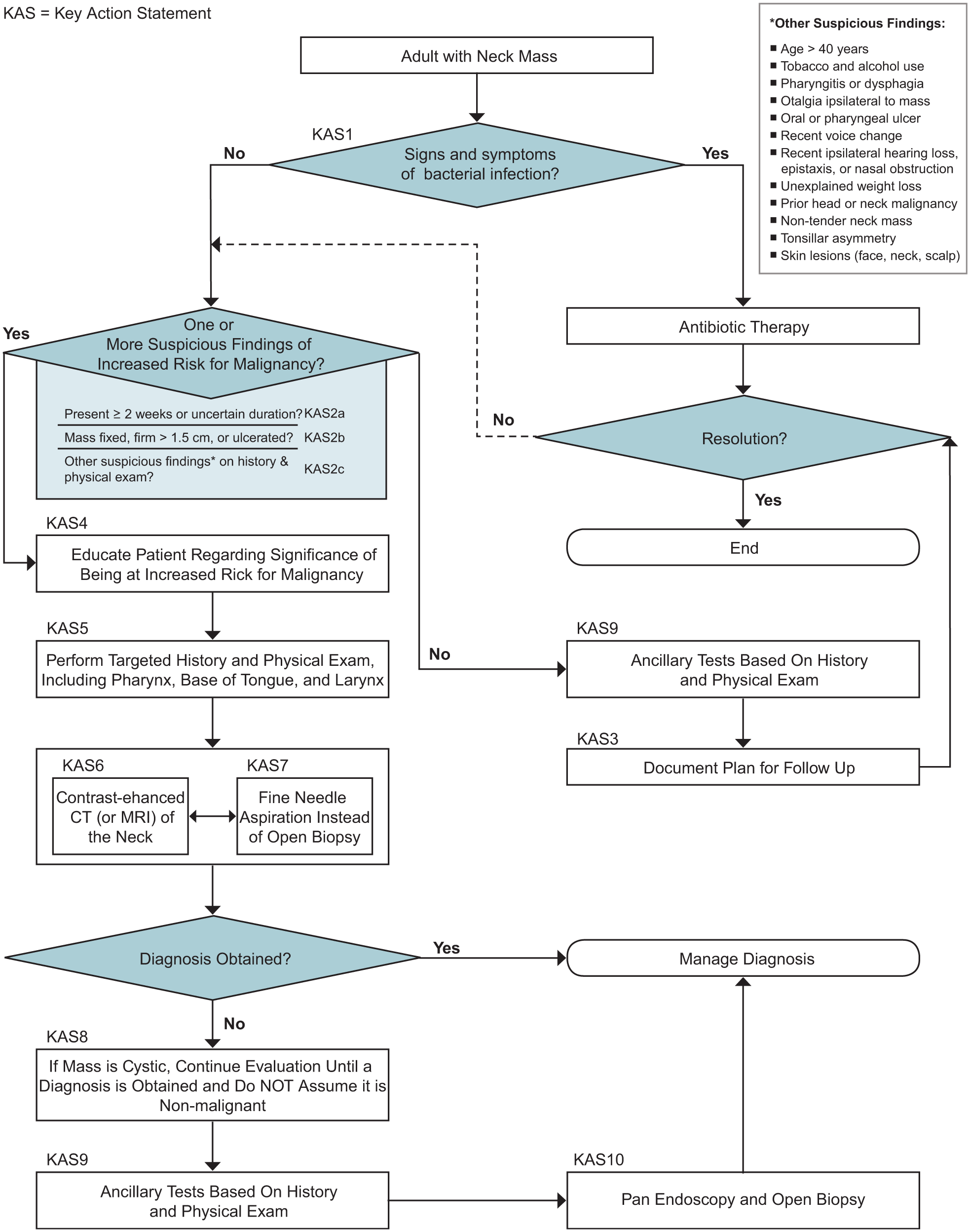
Algorithm depicting the relationship among the key action statements (KASs). CT, computed tomography; MRI, magnetic resonance imaging.
The role of patient preferences in making decisions deserves further clarification. The role for patient preference depends on the clinical evidence behind each statement. Statements with clinical evidence that clearly demonstrates a benefit have less of a role for patient preference as compared with statements with a less convincing evidence base. Although some statements may have little room for patient preference, clinicians should provide patients with clear and comprehensible information to explain the clinician’s recommendation to facilitate patient understanding and informed decision making. In cases where evidence is weak or benefits unclear, shared decision making—where the management decision is made by a collaborative effort between the clinician and an informed patient—is extremely useful. Factors related to patient preference include (but are not limited to) absolute benefits (number needed to treat), adverse effects (number needed to harm), quality of life, cost of drugs or procedures, and frequency and duration of treatment. Certain, less tangible factors should be considered, such as religious and/or cultural beliefs and patients’ social situations.
Action Statement Profile
Action Statement Profile
Characteristics Suspicious for Malignancy in the Presence of a Neck Mass.
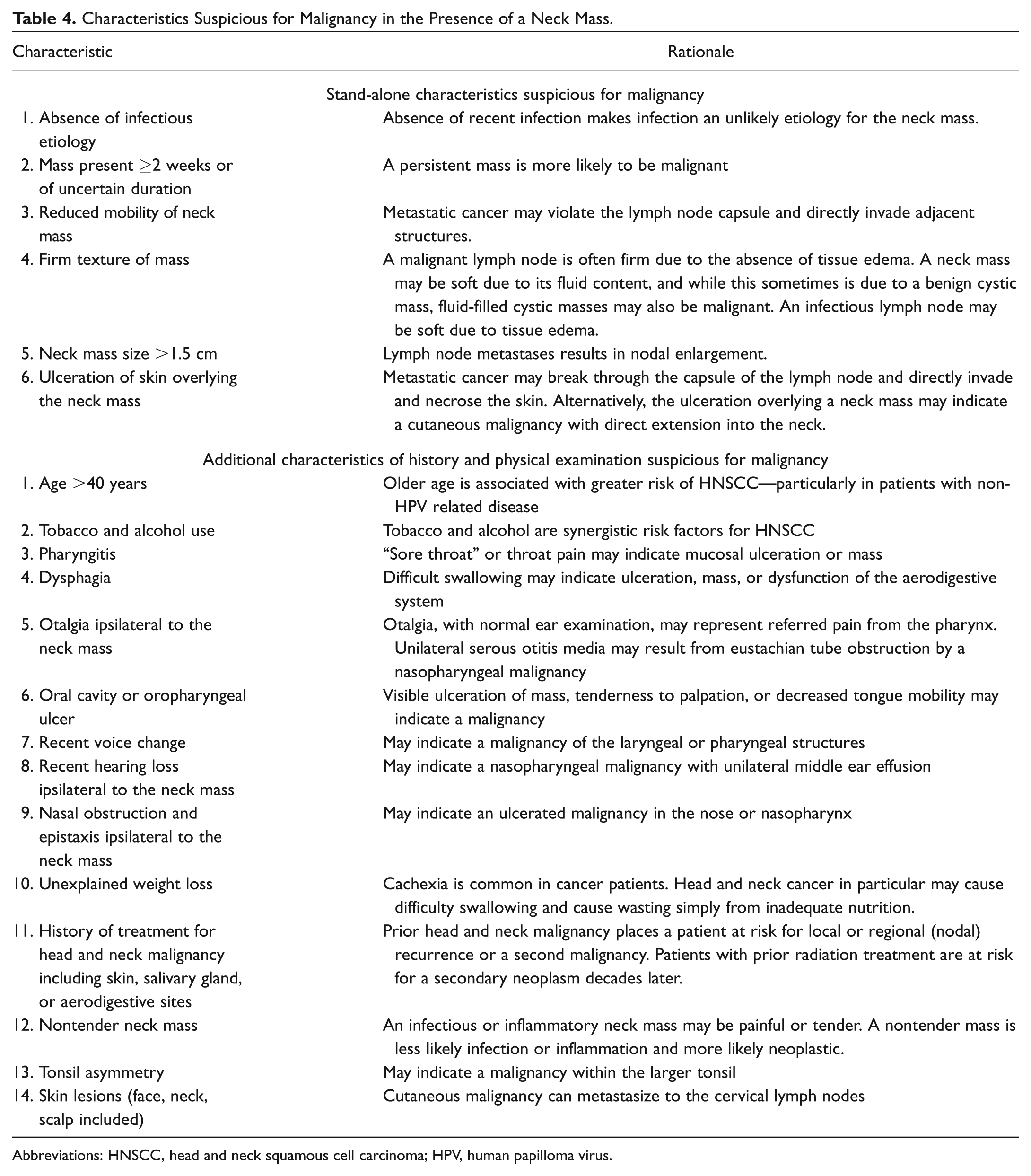
Abbreviations: HNSCC, head and neck squamous cell carcinoma; HPV, human papilloma virus.
Action Statement Profile
Action Statement Profile
Action Statement Profile
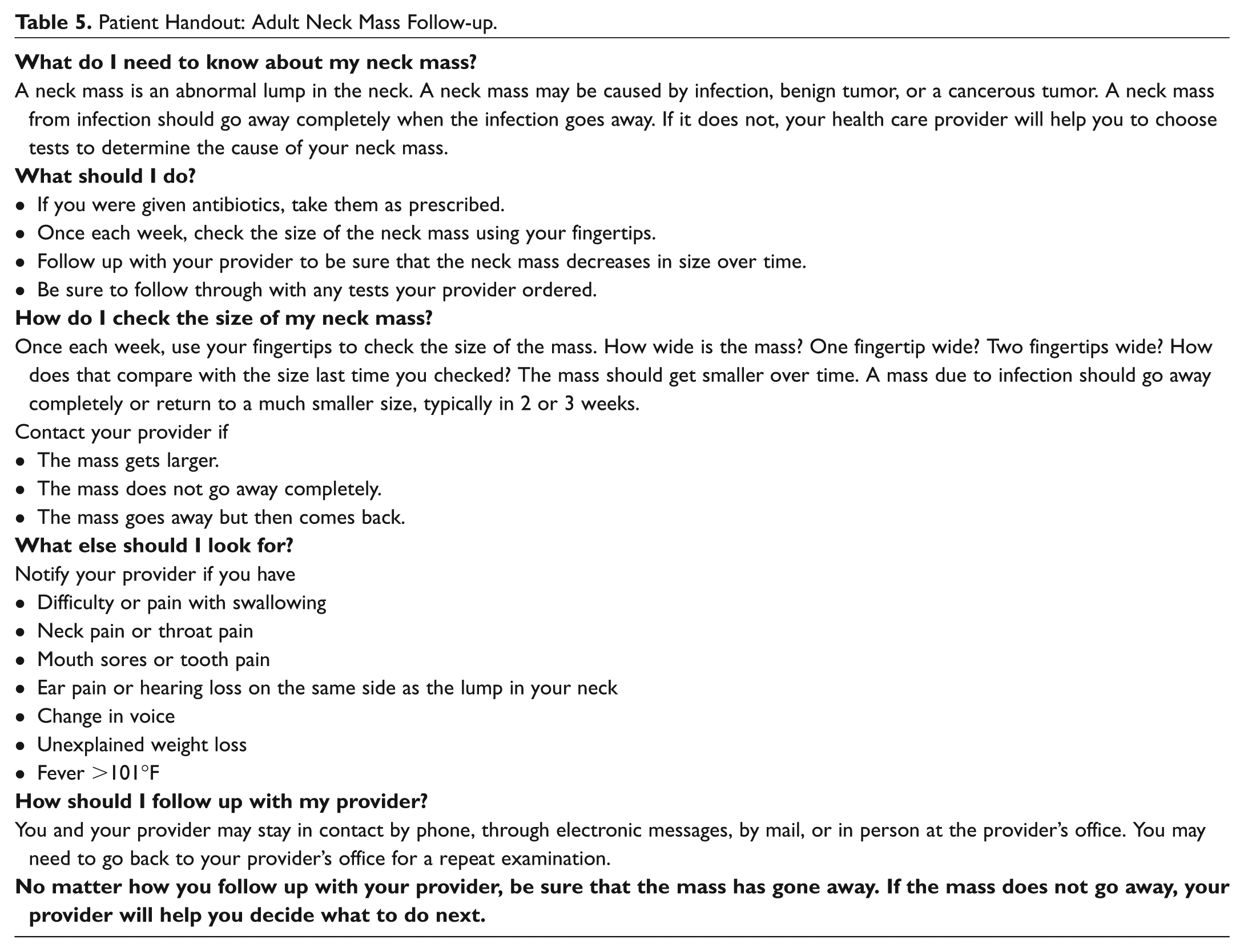
Patient Handout: Adult Neck Mass Follow-up.
Action Statement Profile
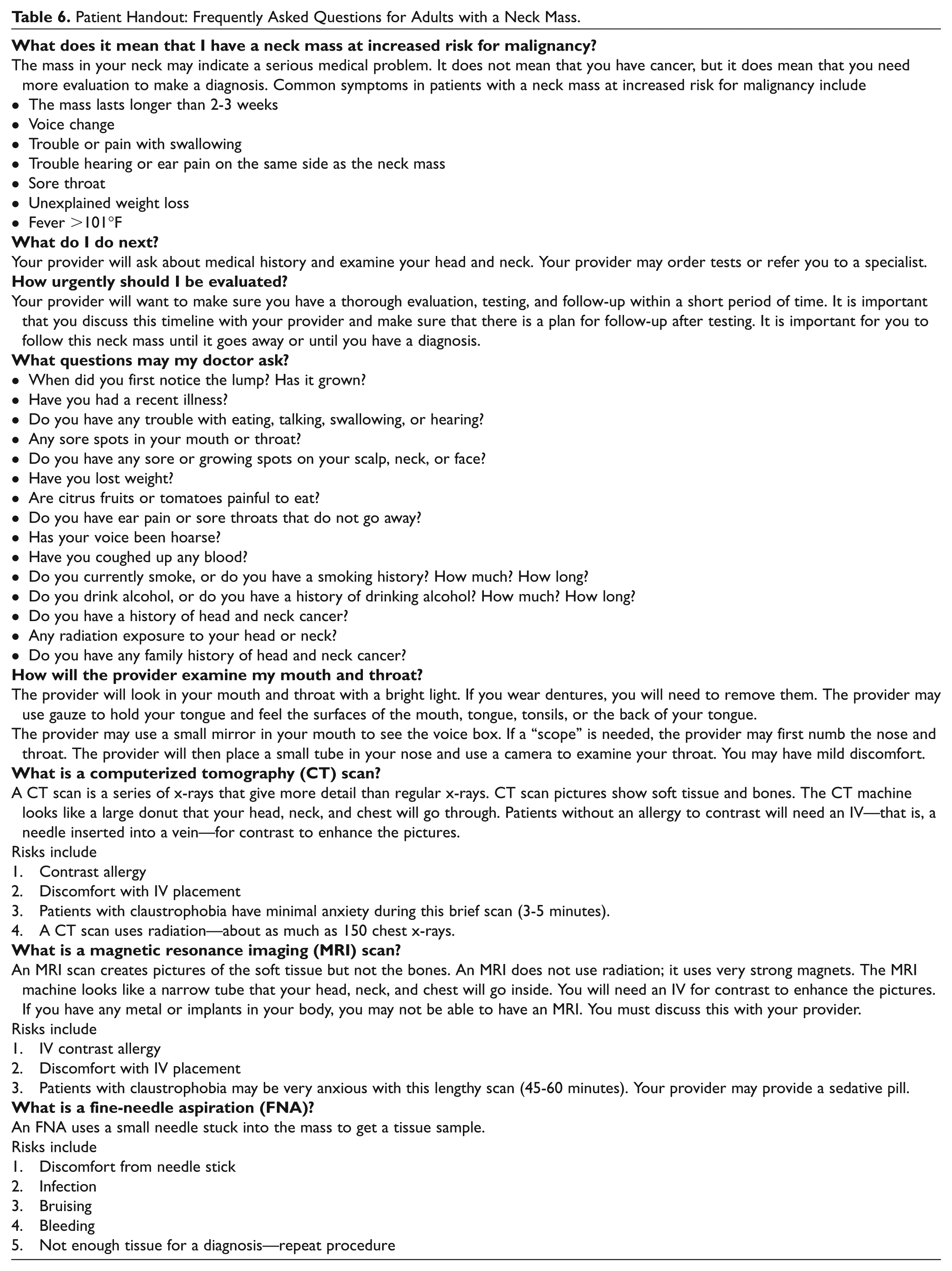
Patient Handout: Frequently Asked Questions for Adults with a Neck Mass.
Action Statement Profile
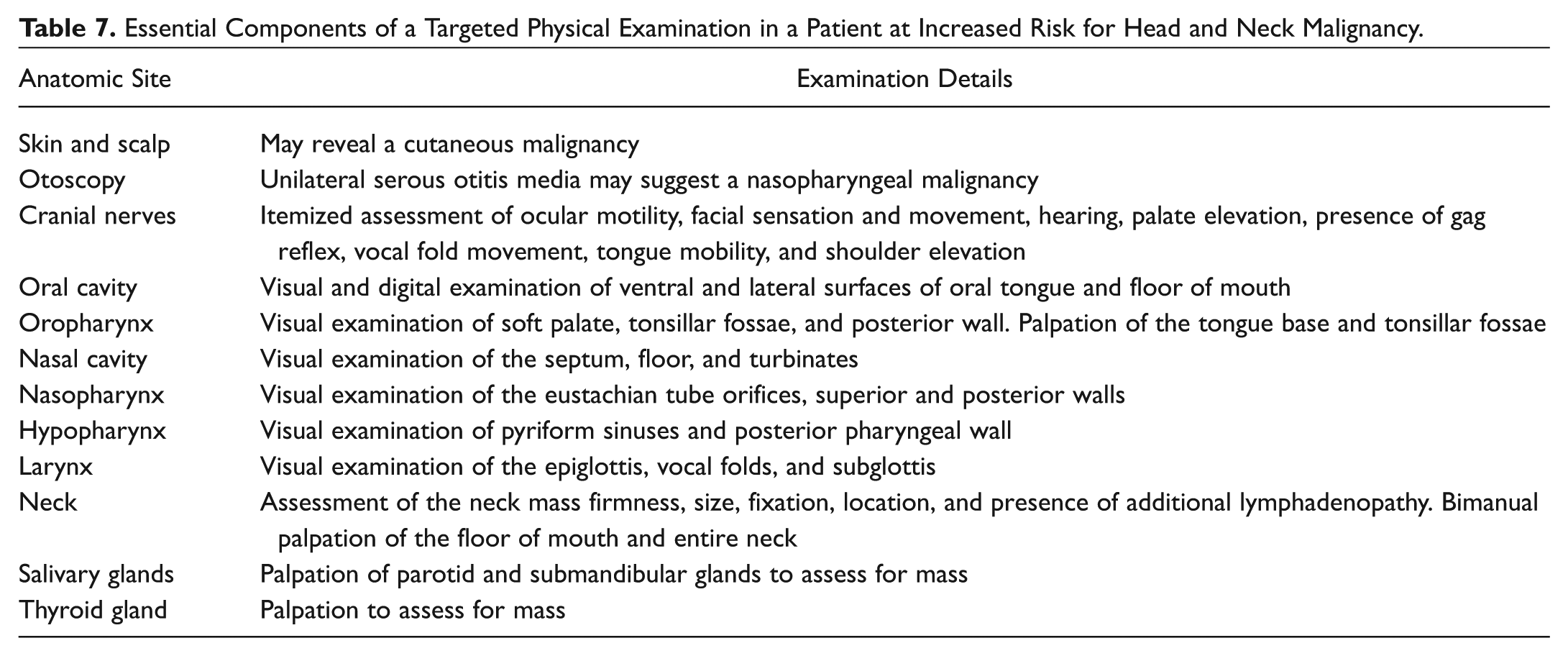
Essential Components of a Targeted Physical Examination in a Patient at Increased Risk for Head and Neck Malignancy.
Action Statement Profile
Action Statement Profile
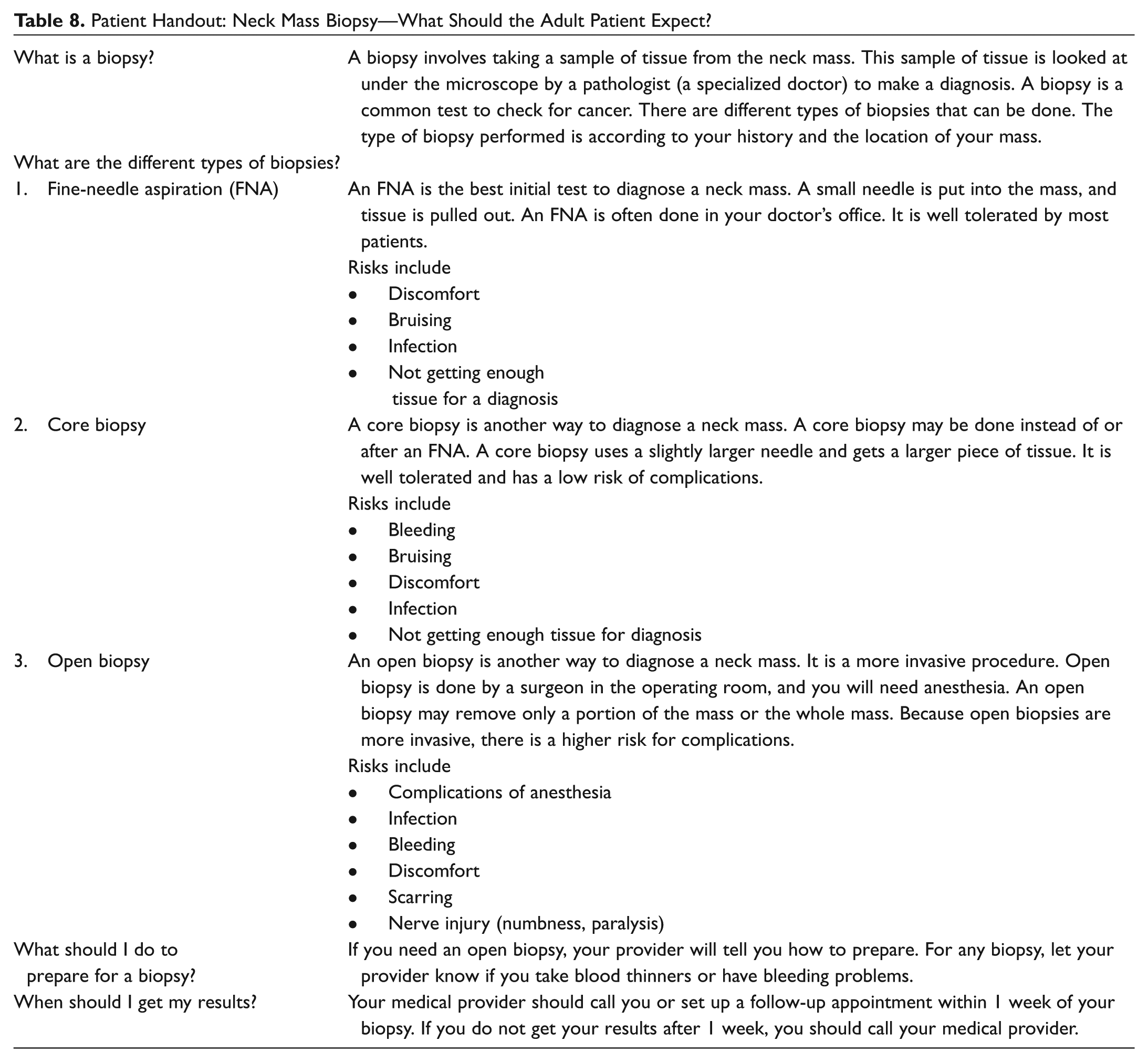
Patient Handout: Neck Mass Biopsy—What Should the Adult Patient Expect?
Action Statement Profile
Action Statement Profile
Action Statement Profile
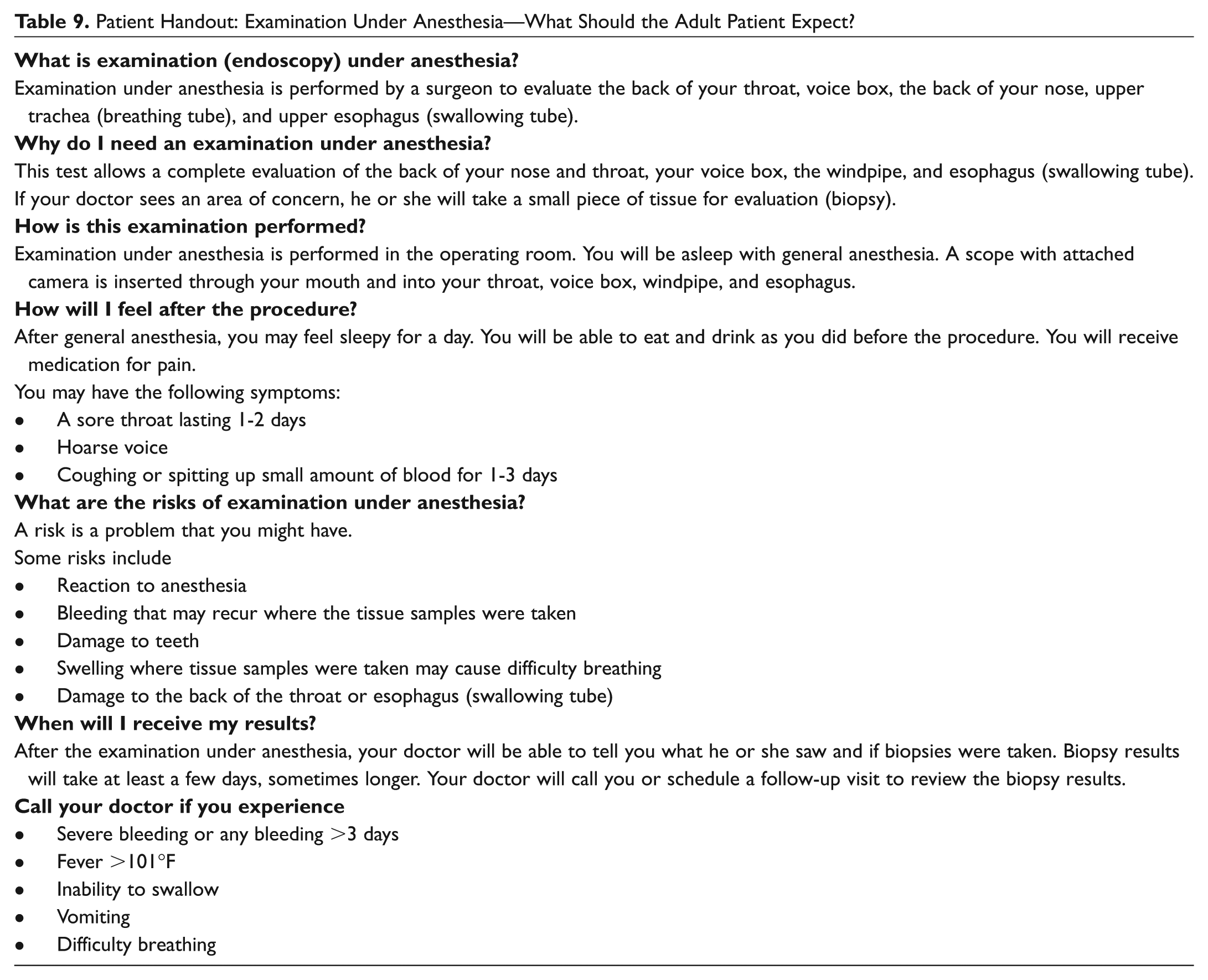
Patient Handout: Examination Under Anesthesia—What Should the Adult Patient Expect?
Author Contributions
Disclosures
Footnotes
Acknowledgements
We gratefully acknowledge the support of Jean C. Blackwell, MLS, for conducting the literature searches, as well as graphic designer Jackie Cole for her work in creating some of the images within the guideline.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
The clinical practice guideline is provided for information and educational purposes only. It is not intended as a sole source of guidance in evaluating neck masses. Rather, it is designed to assist clinicians by providing an evidence-based framework for decision-making strategies. The guideline is not intended to replace clinical judgment or establish a protocol for all individuals with this condition and may not provide the only appropriate approach to diagnosing and managing this program of care. As medical knowledge expands and technology advances, clinical indicators and guidelines are promoted as conditional and provisional proposals of what is recommended under specific conditions but are not absolute. Guidelines are not mandates; these do not and should not purport to be a legal standard of care. The responsible clinician, in light of all circumstances presented by the individual patient, must determine the appropriate treatment. Adherence to these guidelines will not ensure successful patient outcomes in every situation. The American Academy of Otolaryngology—Head and Neck Surgery Foundation emphasizes that these clinical guidelines should not be deemed to include all proper treatment decisions or methods of care or to exclude other treatment decisions or methods of care reasonably directed to obtaining the same results.