
Abstract
Objective
To evaluate the voice outcomes of adults diagnosed with vocal fold nodules (VFNs) as children and to assess the impact of speech therapy on long-term voice outcomes.
Study Design
Prospective cohort study.
Setting
Large health care system.
Subjects and Methods
Subjects diagnosed with VFNs as children between the years 1996 and 2008 were identified within a medical record database of a large health care system. Included subjects were 3 to 12 years old at the time of diagnosis, had a documented laryngeal examination within 90 days of diagnosis, and were ≥18 years as of December 31, 2014. Qualified subjects were contacted by telephone and administered the Vocal Handicap Index–10 (VHI-10) and a 15-item questionnaire inquiring for confounding factors.
Results
A total of 155 subjects were included, with a mean age of 21.4 years (range, 18-29). The male:female ratio was 2.3:1. Mean VHI-10 score for the entire cohort was 5.4. Mean VHI-10 scores did not differ between those who received speech therapy (6.1) and those who did not (4.5; P = .08). Both groups were similar with respect to confounding risk factors that can contribute to dysphonia, although the no-therapy group had a disproportionately higher number of subjects who consumed >10 alcoholic drinks per week (P = .01).
Conclusion
The majority of adults with VFNs as children will achieve a close-to-normal voice quality when they reach adulthood. In our cohort, speech therapy did not appear to have an impact on the long-term voice outcomes.
Pediatric vocal fold nodules (VFNs) are fibrous thickenings within the superficial lamina propria, usually located at the anterior third–posterior two-thirds junction.1,2 The formation of these nodules is commonly attributed to chronic voice abuse from inciting factors such as yelling, screaming, and speaking loudly for prolonged periods, thereby leading to the colloquial term to describe these lesions as “screamer’s nodules.”3 -6 The chronic phonotrauma leads to physiologic reactions of edema, hyalinization, fibrosis, and eventual voice mutation. 4 While the majority of studies have supported voice abuse as the main underlying etiology, gastroesophageal reflux disease, nasal allergies, and dehydration may also be contributors, albeit less commonly, and therefore should be evaluated for and addressed.7,8
While behavioral elements have shown to be linked to the formation of VFNs, the immature anatomy of a child’s larynx has also been implicated with a child’s susceptibility to VFNs. In children, the larynx is smaller, with shorter immature vocal folds that lack the 5-layered structure of adult vocal folds. This immaturity leads to floppier vocal folds, which result in higher shear stress leading to phonotrauma.9 -11 For these reasons, it is commonly believed that the majority of pediatric VFNs will resolve as children physically mature into adults.
In the acute setting, pediatric VFNs can negatively affect a child’s quality of life,2,4,10,12,13 although many families report little to no negative sequelae from the VFNs.14,15 With these concerns in mind, up to 85% of otolaryngologists will proceed with treatment, ranging from behavioral therapy, targeted speech therapy, and surgical intervention. 16 However, the benefits of behavior modification and speech therapy have been mixed, and treatments entail regimented therapy over several months requiring a significant commitment from patients and families.2,14 Additionally, surveillance laryngoscopy is difficult, and treatment compliance is often poor where VFNs are likely to recur.2,14,17 In addition, many families do not believe that the dysphonia from VFNs is negatively affecting a child’s quality of life and voice.14,15 In the end, counseling patients and families regarding treatment of VFNs can be challenging.
Ultimately, families are often concerned about the long-term outcomes of VFNs and the role of treatment in the long-term prognosis. Yet, quality data are limited regarding the long-term outcomes of pediatric VFNs on voice quality in adults. In our study, with the hope of assisting otolaryngologists to better guide patients and families in their respective treatment plans, we aimed to evaluate longitudinal outcomes of pediatric VFNs by assessing (1) the voice outcomes of adults who were diagnosed with pediatric VFNs and (2) whether speech therapy interventions had an influence on these voice outcomes.
Methods
This study was approved by the Kaiser Foundation Research Institute’s institutional review board for the protection of human subjects and supported by a grant from the Kaiser Permanente Northern California’s Community Benefit Program. A single-institution prospective cohort study was performed to assess the voice quality of adult subjects who were diagnosed with VFNs as children. Voice quality was measured with a validated instrument, the Voice Handicap Index–10 (VHI-10), and confounding risk factors were assessed via a questionnaire.
Subjects were identified with pediatric VFNs through International Classification of Diseases, Ninth Revision (ICD-9) code 478.5 within an electronic medical database of a single health care organization between 1996 and 2008. Subjects were included if they were 3 to 12 years old at the time of diagnosis, had a documented or coded laryngeal examination based on Current Procedural Terminology code 31575 within 90 days of the diagnosis, were ≥18 years as of December 31, 2014, and were a current Kaiser Permanente Northern California member. To ensure that our cohort had an accurate diagnosis of VFNs, a retrospective review of identified subjects was performed by 2 otolaryngologists to ensure that each subject had a documented laryngeal examination per Current Procedural Terminology code or chart documentation.
Subjects were excluded if they lacked a coded or documented laryngeal examination, if the chart documented diagnosis differed from the ICD-9 diagnosis, and if subjects reported a history of laryngeal surgery or speech therapy as adults.
A research assistant contacted subjects who met the inclusion criteria by telephone. Consent was obtained prior to proceeding with the questionnaires. Subjects were then administered the VHI-10 and a 15-item questionnaire inquiring about speech therapy history at <18 years of age and confounding risk factors that could affect their current voice quality.
Primary statistical analysis focused on whether speech therapy for pediatric VFNs had an impact on adult voice outcomes. We conducted bivariate and multivariable analyses to look for mean VHI-10 differences as well as demographic and clinical differences between the groups (no speech therapy and any speech therapy). Bivariate analysis was conducted with the chi-square or Fisher’s exact test for categorical variables and Student’s t test for continuous variables. Multivariable analysis was performed with the ordinary least squares method to assess the mean VHI-10 score between the groups. The covariates included demographic characteristics (eg, age, sex, and race) and clinical characteristics obtained from the survey questionnaire, including smoking (current or history), weekly alcohol consumption, gastroesophageal reflux disease, asthma requiring inhaled steroids, nasal allergies requiring medications, current antireflux medication use, and history of endotracheal intubation.
Results
We initially identified 420 subjects with pediatric VFNs according to ICD-9 code. In our retrospective review, 79 subjects were excluded due to a lack of a coded or documented laryngeal examination, and 7 were excluded owing to incongruent diagnoses documented within the medical records. A total of 334 subjects met the inclusion criteria. Of these, 144 were unreachable by phone; 27 declined to be surveyed; and 8 were ineligible because of history of laryngeal surgery.
In all, 155 subjects completed the VHI-10 and 15-item confounding factors questionnaire, with a mean age of 21.4 ± 2.6 years (range, 18-29). The male:female ratio was 2.3:1. The mean VHI-10 score for the entire cohort was 5.4 ± 5.7.
Mean VHI-10 scores for those who received speech therapy and those who received no therapy were 6.1 ± 6.0 and 4.5 ± 5.1, respectively. No significant difference in VHI-10 scores was found between treatment groups (P = .08). A summary of VHI-10 score results of the no-therapy and any-therapy groups is shown in Figure 1 . Treatment groups were similar in their composition of confounding risk factors, although the no-therapy cohort did have more patients who consumed >10 alcoholic drinks per week (P = .01). A comparison of characteristics between the cohorts is shown in Table 1 . Multivariable analysis was performed, adjusting for confounding factors and again demonstrating no significant difference between groups in mean VHI-10 scores (P = .11). Additional subanalysis was performed to evaluate the impact of the number of speech therapy sessions received. No significant difference was exhibited between groups who received more or less speech therapy (P = .19). There also was not a significant difference in mean VHI-10 scores between genders (P = .36) and among ethnicities (P = .36).
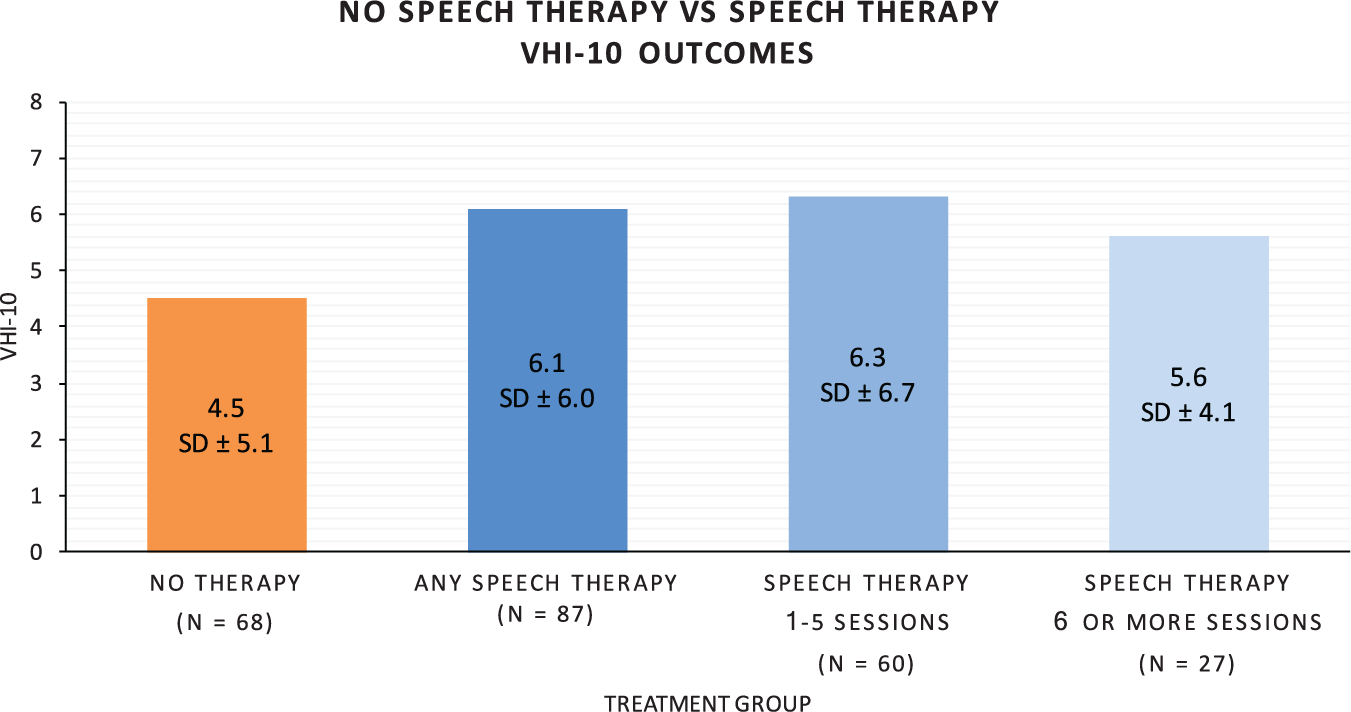
Voice Handicap Index–10 (VHI-10) scores for the study cohorts: no speech therapy and any speech therapy. No significant difference was found (P = .08). Values are presented in mean ± SD.
Confounding Risk Factors Between Groups: No Speech Therapy and Any Speech Therapy. a
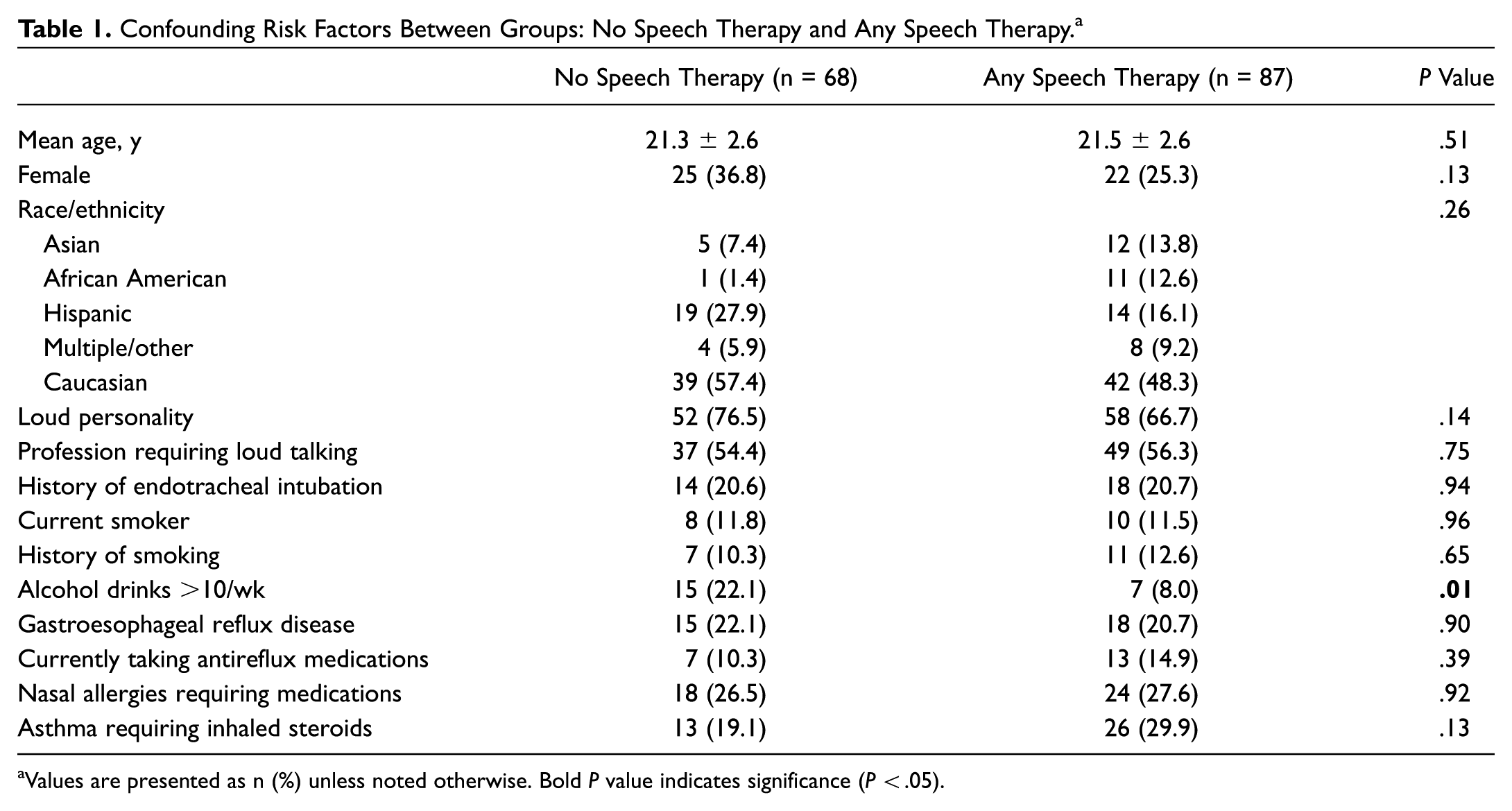
Values are presented as n (%) unless noted otherwise. Bold P value indicates significance (P < .05).
Discussion
This study is the first to our knowledge that utilizes a validated voice assessment instrument in a large cohort to investigate the voice quality of adults who were diagnosed with VFNs as children.
To provide broader context of the voice quality of our cohort, we compared our results with the normative VHI-10 values described by Rosen et al. 18 Our cohort’s mean VHI-10 score was significantly higher than that of their control group (5.4 ± 5.7 vs 3.4 ± 5.7; P < .0018) but significantly better than that of the polyp/nodule/cyst group (5.4 ± 5.7 vs 15.5 ± 7.2; P < .0001). In fact, our cohort’s voice outcomes were better than every other disease subgroup reported by Rosen et al, including reflux. This supports the notion that the majority of adults who had pediatric VFNs will have close-to-normal voice quality in adulthood. A graphic representation of our cohort’s VHI-10 score in relation to each disease subgroup from the VHI-10 normative scores reported in the Rosen et al study is shown in Figure 2 .
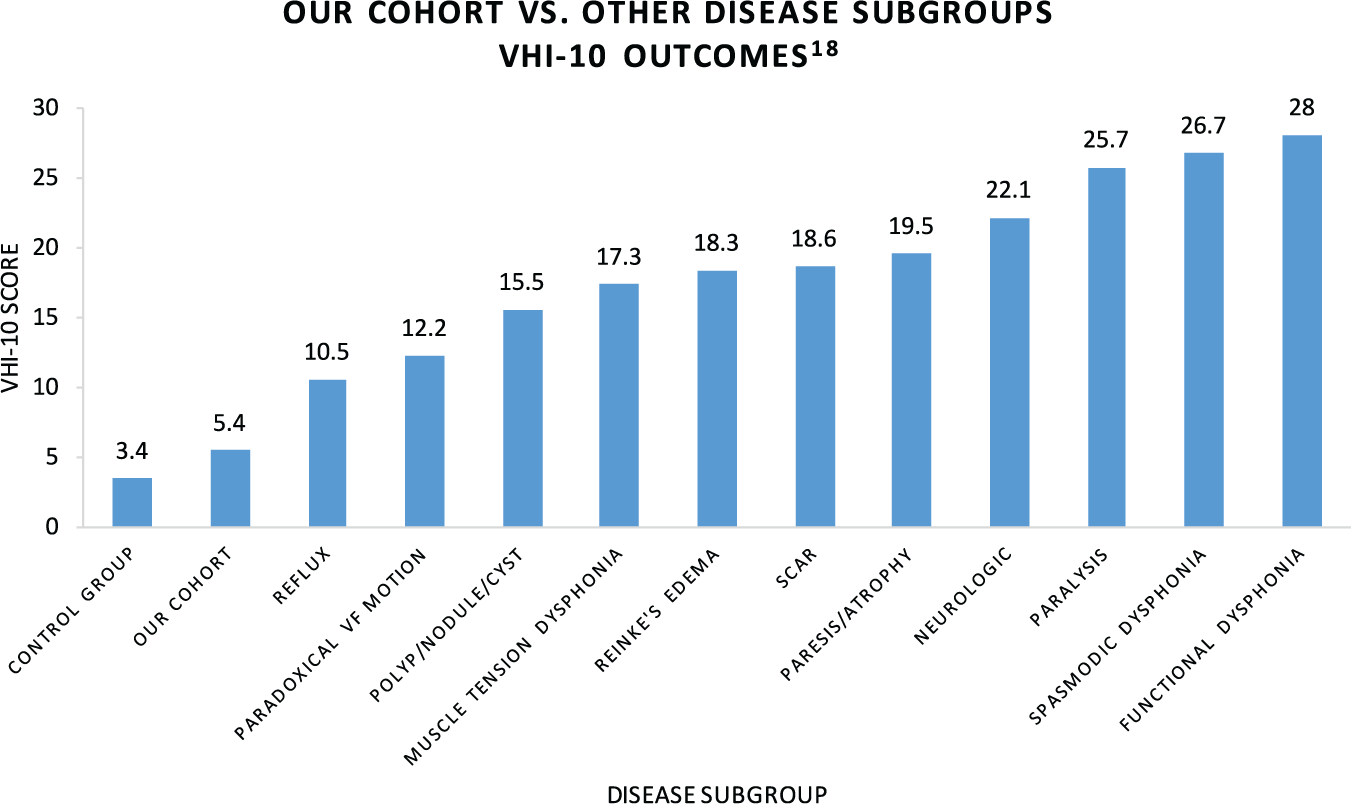
A comparison of the mean Voice Handicap Index–10 (VHI-10) score of our group and the normative scores of each disease subgroup described by Rosen et al. 18
Previous studies exhibited similar postmaturation voice quality outcomes, albeit with less robust methodology. These studies evaluated subjects as postmaturation teens, not as adults, and did not employ validated voice assessment instruments. Mori found that voice quality improved or normalized in the majority of patients after puberty. 14 However, the study did not report the mean age of the postmaturation cohort; it assessed postmaturation status with only 1 dichotomous question; and it did not utilize a validated voice quality assessment instrument. De Bodt et al also found that postmaturation voice quality improved in subjects previously diagnosed with pediatric VFNs. 19 Specifically, 79% of their cohort (n = 91) did not report voice complaints after progression through puberty. Yet, this study was similarly limited by their simplistic postmaturation state assessment, in which they also asked only a single dichotomous question investigating whether a subject proceeded through puberty. The cohort’s mean age of 16 years may in fact be too young to get an accurate perception of postmaturation voice quality. VFNs require time to resolve; therefore, utilizing an older cohort accounts for the lag time of VFN resolution in postmaturation subjects. Also, only 34 of the 91 subjects completed a validated voice assessment, which further limits the power of their results. While these studies do support our conclusion of near-normal voice outcomes for the majority of children as they mature into adulthood, their limitations highlight the necessity of a study that utilizes validated voice assessment instruments and follows subjects well into adulthood, where postmaturation VFN resolution lag time is no longer a factor. Our study resolves these limitations by examining the long-term voice outcomes of an adult cohort with a mean age of 21.4 years old and utilizing the well-validated and widely used VHI-10.
Many families struggle with the cost and, more so, time commitment of speech therapy. The decision to intervene with speech therapy in the setting of pediatric VFNs can be a difficult decision for families. There is also conflicting data on the best treatment for pediatric VFNs. A best practices review was published in 2013 discussing whether voice therapy should be used to treat children with vocal cord nodules. 15 The authors concluded that despite a lack of good evidence, the literature suggests some benefit from an acoustic and perception standpoint. Most studies consider only the short term, and many families are most concerned with long-term voice outcomes. In our study, we sought to examine the long-term impact of speech therapy during childhood on voice quality in adulthood, and we determined that there was no difference between groups receiving speech therapy and no treatment. Clinically, this information could be used to counsel families whose children have VFNs but do not believe that the nodules are affecting their voice and/or quality of life in the short term. Understanding the long-term voice outcomes can help families make the decision to forgo the cost and time associated with speech therapy for VFNs in the absence of immediate concerns.
Limitations of our study are that it relied on questionnaires to assess the voice quality and confounding factors of subjects, making it susceptible to recall bias. The questionnaires were administered via telephone and therefore lacked a clinical examination to assess for current vocal fold appearance. While our cohort had a relatively low VHI-10 score, we cannot make conclusions regarding the current state of their vocal folds and how that may have affected their overall voice quality. Treatment groups were also determined retrospectively and allocated in a nonrandomized fashion, making it subject to selection bias. Patients with less severe disease may have been more likely to proceed without speech therapy, leading to falsely lower the VHI-10 score. However, the mean VHI-10 score for our entire cohort was 5.4 ± 5.7, where we can safely conclude that the majority of patients, regardless of treatment type, will have close to a normal voice handicap as adults. Last, we did not have data regarding the type of speech therapy that patients received, and this could very well reflect high heterogeneity in the speech therapy treatment group. Yet, we do not believe that this dilutes the validity of our results, because it accurately reflects the high heterogeneity of speech therapy interventions utilized in the community.
Strengths of our study are that we had a larger and older cohort as compared with similar studies. While a markedly larger cohort may have delineated a small difference in voice handicap in the therapy versus no-therapy comparison groups, we do not believe that it would be clinically compelling, since the overall VHI-10 for the entire cohort was near normal at 5.4 ± 5.7. In addition, the comparison groups were statistically similar except for alcohol consumption, which did not affect the results of our multivariable analysis. We also utilized a well-validated and commonly used voice quality-of-life instrument with normative values for a range of laryngeal disorders in the VHI-10, which is relatable, robust, and readily accessible for other clinicians. The VHI-10 is based on the Voice Handicap Index, which was the only instrument on voice-related measures reported to meet the Agency for Healthcare Research and Quality’s stringent criteria.18,20 We specifically chose to use the VHI-10 rather than the full VHI since, in our experience, the VHI-10 is the more often implemented voice assessment in clinical practice. With that being said, we did confirm the reliability of our VHI-10 results by concurrently administering the entire VHI for our cohort, where the results mirrored our reported VHI-10 results: no difference between treatment groups and a near-normal VHI score for the entire cohort. Voice quality instruments, including the Grade, Roughness, Breathiness, Asthenia, and Strain Scale and Consensus Auditory-Perceptual Evaluation of Voice, were not included. We did not believe that this diluted our results, since these aforementioned questionnaires are used in a clinical setting and were developed to provide standardized qualitative assessments of a patient’s voice from a clinician’s perspective. Yet, hoarseness in the setting of VFNs is a quality-of-life condition where patient symptoms and level of handicap drive treatment, which was the focus of our study. The VHI-10 therefore provided the most accurate assessment evaluating the global impact of hoarseness on a patient’s quality of life. While our study provides an excellent foundation to investigate the global impact of pediatric VFNs on the voice of adults with a history of pediatric VFNs, future prospective multi-institutional studies should be performed with clinical visits incorporating laryngeal examinations and standardized clinician qualitative assessments of patient voices to better elucidate the clinical resolution of pediatric VFNs once patients are well into adulthood.
Conclusion
The majority of children with pediatric VFNs can expect a near-normal voice quality prognosis as they mature into adults. Neither the presence of speech therapy intervention nor the number of speech therapy sessions influenced the voice quality of our adult cohort. Treatment for pediatric VFNs should focus on addressing short-term voice quality-of-life issues and not be based on long-term voice outcomes.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We sincerely thank Dorothy Ferguson, BEd, for her assistance contacting subjects and administering the study questionnaires.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented as an oral presentation at the 2016 AAO-HNSF Annual Meeting & OTO EXPO; September 18-21, 2016; San Diego, California. This study was also presented at the 100th Annual Pacific Coast Oto-ophthalmological Meeting; June 2016; Kauai, Hawaii.