
Abstract
Objective
The purpose of this review is to describe the recent advances in identifying possible factors involved in the pathogenesis of spasmodic dysphonia. Spasmodic dysphonia is a task-specific focal laryngeal dystonia characterized by irregular and uncontrolled voice breaks. Pathogenesis of the disorder is poorly understood.
Data Sources
PubMed, Google Scholar, and Cochrane Library.
Review Methods
The data sources were searched using the following search terms: (spasmodic dysphonia or laryngeal dystonia) and (etiology, aetiology, diagnosis, pathogenesis, or pathophysiology).
Conclusions
Several potential etiological factors have been proposed by epidemiological, genetic, and neuropathological studies. Spasmodic dysphonia is a rare disorder primarily affecting females beginning in their 40s. Vocal tremor co-occurs in 30% to 60%. Large cohort studies identified risk factors such as a family history of neurological disorders including dystonia and tremor, recent viral illness, and heavy voice use. As none are rare events, a complex interactive process may contribute to pathogenesis in a small proportion of those at risk. Consequences to pathogenesis are neurological processes found in spasmodic dysphonia: loss of cortical inhibition, sensory processing disturbances, and neuroanatomical and physiological differences in the laryngeal motor control system.
Implications for Practice
Diagnosis of spasmodic dysphonia usually includes speech and laryngoscopic assessment. However, as diagnosis is sometimes problematic, measurement of neurophysiological abnormalities may contribute useful adjuncts for the diagnosis of spasmodic dysphonia in the future.
Spasmodic dysphonia (SD) is a task-specific focal laryngeal dystonia characterized by irregular and uncontrolled voice breaks that interrupt normal speech flow. These are accompanied by effortful phonation. In 1971, Moore described SD as an intermittent clasping of the vocal folds causing disruption of the flow of speech. 1 Over 65% of those affected are females, at an average age of symptom onset of 45 years.2,3 There are 2 general types of SD: adductor spasmodic dysphonia (AdSD), characterized by a harsh, strain-strangled voice with breaks on vowels in speech, and abductor spasmodic dysphonia (AbSD), characterized by prolonged voiceless consonants before vowels.
SD is rare disorder with an estimated prevalence of 1 per 100,000. 4 The diagnosis of SD can be challenging, and the pathogenesis is unknown. Most of the current research into SD is focused on management strategies. The objective of this review is to describe the recent advances in identifying possible pathogenic factors and new potential techniques for characterizing SD.
Methods
A thorough review of the literature was conducted using 3 data sources (PubMed, Google Scholar, and Cochrane Library) between November 2016 and April 2017 to investigate the pathogenic factors of SD. The data sources were searched using the following search terms: (spasmodic dysphonia or laryngeal dystonia) and (etiology, aetiology, diagnosis, pathogenesis, or pathophysiology). Only articles available in English or German were retrieved. The articles were then analyzed for relevance, and articles primarily investigating treatment strategies of SD or other types of dystonia were excluded. Any contemporary review of the literature carries the risk of bias inherent in each individual article. Although the authors were inclusive in selection of the articles, there is still the potential for selection bias. Last, there is a potential of bias in interpretation of the reviewed articles presented by the authors. Every attempt was taken to minimize these biases and present the information objectively.
Pathogenic Factors
Initial reports of SD hypothesized a psychosomatic cause for the dysphonia; however, in 1960, Robe et al 5 reported that of 10 patients diagnosed with SD, all had signs of central nervous system (CNS) abnormalities. Nine of 10 had irregular discharge in their right temporal region on electroencephalography, 8 had transient leg or arm weakness, and 4 had familial neurological diseases. Further evidence pointing toward a neurological component came when Dedo 6 temporarily paralyzed the recurrent laryngeal nerve (RLN), followed by sectioning, and found a return to normal voice in half of the treated patients. A recent case-control study has also added to evidence for a neurological basis. 7
Early electromyographic studies indicated abnormalities in the motor control system. 8 These findings were followed by attempts to treat the dystonic movements using botulinum neurotoxin (BoNT) injections into affected muscles. BoNT inhibits release of acetylcholine from the presynaptic terminal into the neuromuscular junction, causing a temporary paralysis. Early results showed a beneficial effect of BoNT in improving voice symptoms following BoNT injections,9,10 and BoNT remains the primary treatment for SD today. Several studies have shown that treatment with BoNT improves acoustic, aerodynamic, and perceptual characteristics of the voice (described in more detail in part 2). The primary improvements are reduced voice breaks, reduced time to read a sentence, and improved control of speech intensity and prosody. Airflow rates also increase within a few days after BoNT injection, plateauing after a few weeks. 11 A mechanism by which BoNT improves SD symptoms appears to be through decreasing the activation of local muscle fibers, reducing vocal fold adduction. 12 Interestingly, BoNT may also have CNS modulating effects, as evidenced by normalization of aberrant CNS activity after BoNT injection 13 and a reduction of spasms in noninjected laryngeal muscles on both sides of the larynx when only one muscle was injected on one side of the larynx. 14 Some authors have hypothesized that this may be due to retrograde transmission of BoNT along the peripheral nerves to modulate the CNS. 12 These findings help highlight some more complex neural network processes that are involved in the pathophysiology of SD. However, these results need to be viewed with some caution. BoNT primarily affects the injected laryngeal muscles, and as such, any type of mechanism resulting in abnormal muscle activation would be altered.
Epidemiological Risk Factors
Following an expert panel review, the development of a diagnostic test was identified as a high priority for use in conducting epidemiological studies. 15 In a 200-patient case history profile, Izdebski et al 16 suggested that SD was not a psychogenic or behavioral disorder but that patients with SD had significant histories of extensive voice use. In another patient survey, Schweinfurth et al 2 compared 168 patients with SD with a first-degree relative control group with no reported environmental or geographical differences. They found a 79% female predominance and average age of onset at 45 years. Interestingly, 65% of patients previously had measles or mumps, compared with a 15% national average at the time. Thirty percent of patients associated the onset of SD with a recent upper respiratory tract infection and 21% with a major life stressor. There was also a greater frequency of writer’s cramp in the SD group (26%) vs 4% in the control group. Using a questionnaire, Tanner et al 7 compared 150 patients with SD to 136 patients with other voice disorders (excluding SD and vocal tremor) to identify risk factors uniquely associated with SD. They found a personal and family history of cervical dystonia and tremor to be significantly associated with SD, indicating a possible genetic risk factor (discussed later). Also associated with SD was a personal history of sinus and throat illnesses, mumps, rubella, dust exposure, extensive voice use, and a family history of meningitis. 17 The authors suggested an association between viral illnesses and the nervous system disorder. Viral illnesses have been associated with numerous peripheral and CNS diseases: Ramsay Hunt syndrome causing facial nerve paralysis, viral-induced unilateral vocal fold paralysis, 18 and long-term sequelae can arise following meningitis and encephalitis. Most viral illnesses resolve without identifiable long-term consequences, although some can remain dormant in the CNS. However, many viral illnesses are common and SD is rare. Perhaps some viral CNS infections lead to subtle changes in the brain and the laryngeal motor control system that may predispose to developing focal dystonias. 17
Table 1 (adapted from Murry 1 ) summarizes some of the risk factors for SD identified in several studies examining large cohorts of patients with SD.2,16,17,19-23 A frequently identified external factor from these studies was stress. An important caveat with this pathogenic factor is the variation in stress responses experienced by different people, as well as its subjective nature. This makes objective or quantitative measurement difficult. A study by Kiese-Himmel and Zwirner 24 failed to identify any clinical psychopathology in a cohort of patients with SD. One hypothesis for this mechanism of stress-related SD onset may be related to neural plasticity: Dauer et al 25 speculated that painful stimuli cause synaptic changes in the basal ganglia, which can predispose or lead to the development of dystonias, including SD.
Risk Factors for Spasmodic Dysphonia from Large Cohort Studies. a
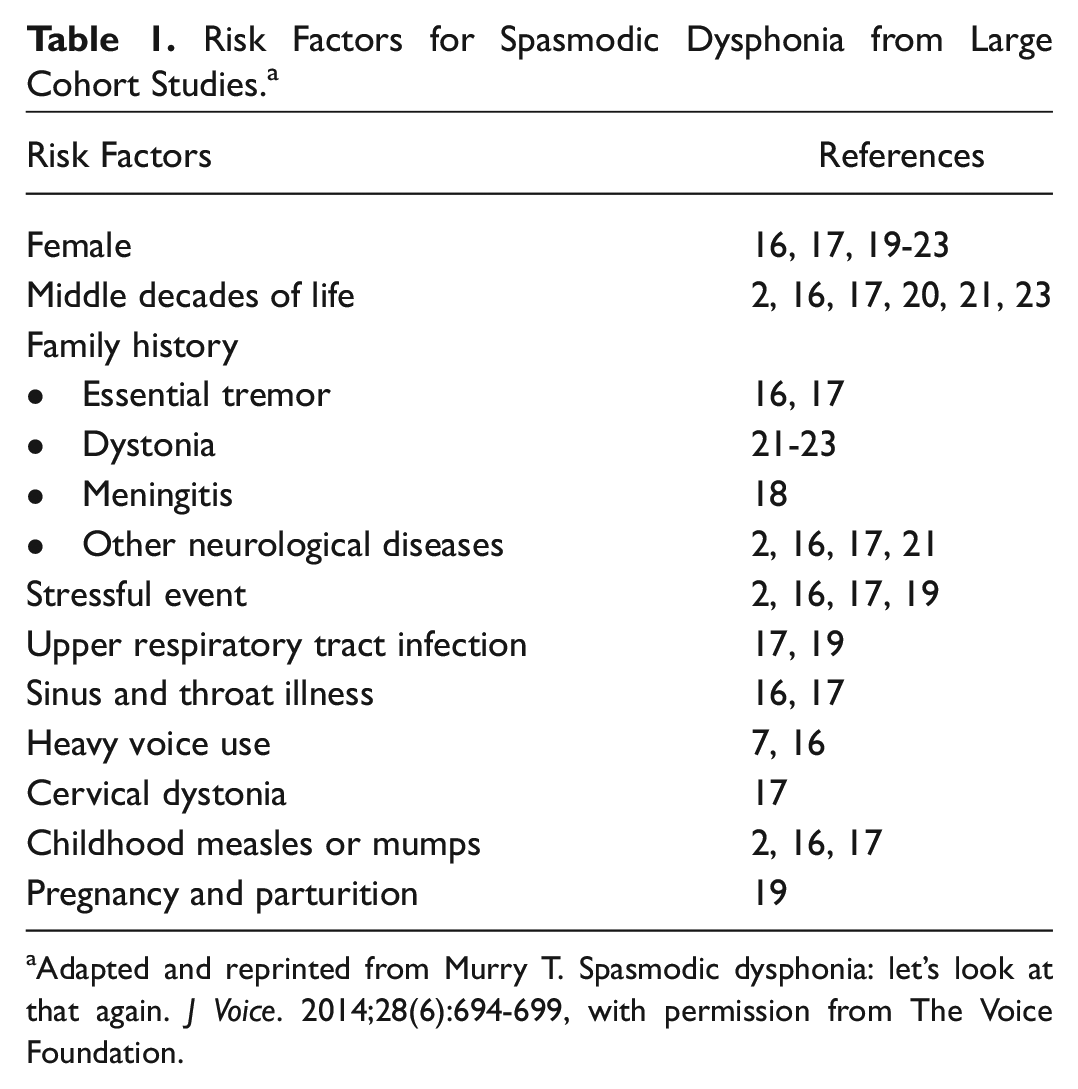
Adapted and reprinted from Murry T. Spasmodic dysphonia: let’s look at that again. J Voice. 2014;28(6):694-699, with permission from The Voice Foundation.
Additional risk factors included recent upper respiratory tract infection, family history of neurological disorders (adding further evidence to a neurological component), parturition, and, in some cases, recent surgery and vocal overuse. 23 All of these are frequent events in the general population and cannot account for a rare disorder. Vocal tremor often coexists with SD. This can range from 29% reported by Tanner et al 7 compared with 54% of patients with AdSD in another study by Patel et al. 20 There was a large sex disparity in the latter study, with 60% of females and 32.8% of males with AdSD having concurrent vocal tremor. 7
Childs et al 19 further examined the differences between sudden and gradual onset of SD. Forty-five percent of people with SD had sudden onset, defined as symptoms occurring within a week. They found that only 2% of people with gradual onset of SD could identify a trigger, compared with 77% of those with a sudden onset. Women were more likely to have both a sudden onset and an identifiable trigger.
Some environmental factors may provoke or trigger the development of SD in a subpopulation of patients and could contribute to a double-hit pathogenesis. It remains to be determined whether or not environmental factors may play a role in the development of SD. 19 Such factors have to be viewed with some caution, as “correlation does not imply causation.”
Epidemiological risk factors for SD, while not necessarily showing any causative relation, may be very valuable in identifying a typical or “at-risk” patient population for SD. Given the frequent difficulty in diagnosing SD, these risk factors may help determine the diagnosis where an otherwise clear picture may not exist.
Genetic Factors
There is growing interest in identifying genetic contributions toward SD, coming from evidence that polymorphisms in generalized dystonia-causing genes can affect the risk of developing focal or segmental dystonia.21,26 Three genes have been found related to different forms of dystonia.
The TUBB4A gene has been shown to contribute to an autosomal-dominant dysphonia combined with oral-lingual and other types of dystonia, with onset in the second to third decade.26,27 This type of dysphonia tends to be “whispering” in quality and is distinct from the usual form of either AdSD or AbSD. The TUBB4A gene is responsible for tubulin β-4 chain proteins, major components of microtubules. Mutations can lead to hypomyelination with atrophy of the basal ganglia and cerebellum (H-ABC). 28
THAP1 gene mutations can cause a generalized form of dystonia, DYT6, which can have frequent laryngeal features. The THAP1 gene is an endothelial cell proliferation regulator and may have an effect on apoptosis. 29 Genetic screening studies of THAP1 in SD patients without generalized dystonia have found only a couple of patients with rare variants of THAP1.21,30,31
TOR1A gene mutations can lead to an early onset autosomal dominant dystonia, DYT1, characterized by either childhood or early onset dystonia that results in generalized dystonia. The TOR1A mutation was the first mutation discovered that causes generalized dystonia. 32 This exerts its effect by causing dysfunction of either the D1 direct or indirect pathway. 33
A recent study examined each of these mutations in SD. Of the 86 patients with SD examined by de Gusmao et al, 21 15% had a definitive family history of neurological disorders, and 5 patients had a first-degree relative with focal dystonia. Genetic screening found none of the 86 cases had disease-causing mutations in TUBB4A and TOR1A, while 2 (2.3%) patients tested positive for novel/rare variants in THAP1.
Thus, the diagnostic yield for indiscriminate genetic screening was low in nonselected and even selected groups of patients with SD. As with other types of dystonias, there may be sporadic and genetically determined types of SD. While genetic contributors to SD are an interesting field of SD research, only weak evidence for a clear link between specific genes and dystonia involving the larynx has been found thus far in a few families. Given the recent advances in identifying genetic patterns in other focal and generalized dystonias, this field needs further attention in SD research with the advent of less expensive methods of genetic testing.
Neurologic Factors
Most recent evidence suggests that SD is a type of focal dystonia,15,34 but the neuropathophysiological mechanism still remains unclear. Dystonia is a group of disorders characterized by involuntary muscle contractions, which can be either intermittent or sustained. They can affect a wide range of muscles. The most common focal dystonia is cervical dystonia, followed by blepharospasm and oromandibular dystonia. 34 Dystonia is generally considered a basal ganglia disorder, 35 characterized by overactivity of the indirect and direct pathway, with reduced internal globus pallidus activity. This can in turn lead to enhanced thalamocortical activation. 35 The direct and indirect pathways pass through parts of the basal ganglia and usually send inhibitory signals from the internal globus pallidus to the thalamus and cortex (via GABA and dopaminergic neurotransmission). Thus, reduced internal globus pallidus activity can lead to increased cortical activity. 36
Recent studies have also demonstrated cerebellar involvement in certain focal dystonias. 37 Using cerebellar continuous theta-burst stimulation protocol (cTBS), a type of transcranial magnetic stimulation, a reduction in primary motor cortex excitability was demonstrated in cervical dystonia but not in focal hand dystonia. 37 This indicated that the influence of the cerebellum in the pathophysiology of various forms of dystonia may vary. The authors concluded that reduced cerebellar modulation over the primary motor cortex is related to the body area affected by the dystonia, rather than being a pathophysiological mechanism common to all dystonias. 37
There seem to be 3 different neurological mechanisms involved in the pathophysiology of SD: loss of cortical inhibition, sensory input disturbances, and neuroanatomical changes.
Reduced cortical inhibition
Evidence from other types of focal dystonia have shown reduced cortical inhibition, measured by differences in short-interval intracortical inhibition (SICI) and shortened cortical silent periods (CSPs). 38 A shorter CSP has been found in regions responsible for other focal dystonias, including focal hand dystonia, cervical dystonia, 39 blepharospasm, and oromandibular dystonia. 38 This suggests that pathophysiological mechanisms in focal dystonias may be a dysfunction of the GABA-ergic inhibitory interneurons within the motor cortex.
Using transcranial magnetic stimulation, Samargia et al 38 measured CSP in the masseter and the first dorsal interosseous (FDI) muscle in AdSD, MTD (muscle tension dystonia), and controls. They found shorter CSPs in the masseter in AdSD in comparison with MTD and controls. Similarly, the CSP in the FDI was shorter in AdSD than MTD and the controls, but the MTD group also had a shorter CSP than the controls. Thus, both patient groups may have some deficit in cortical inhibition that manifests in slightly different ways and can also explain why these disorders can frequently coexist.
This shorter CSP suggests less cortical inhibition in unaffected muscles, indicating a more global, widespread GABA dysfunction. In a case of neuroleptic-induced symptoms of secondary SD, clozapine, a GABA antagonist, reduced symptoms following administration. 40 However, reports of GABA-modifying drugs benefiting idiopathic SD remain limited to a select few cases.
In an Internet accessed questionnaire completed by self-identified patients with SD, Kirke et al 41 found that of 531 patients, 55% reported significant subjective improvement on the voice symptoms after alcohol consumption. While the mechanism of alcohol effect in isolated dystonias has not been established, its positive influences may be due to modulation of GABA-ergic transmission. The authors also suggest that as functional abnormalities have been found in SD not only in the basal ganglia but also in the cerebellum and sensorimotor cortex, alcohol may exert its GABA-ergic effects at multiple levels. 41
Further indication of neurotransmitter dysregulation is derived from evidence that dystonia can be present in up to 30% of patients with Parkinson’s disease and occurs in 60% of patients with young-onset type Parkinson’s. 42 However, the laryngeal symptoms of hypophonia that accompany most patients with Parkinson’s disease do not resemble the voice symptoms in SD and often are not benefited by antiparkinsonian therapy. 43 Other evidence comes from case reports of antipsychotics, such as haloperidol, causing acute laryngeal dystonic reactions. 23 Antipsychotics exert their effect by inhibiting dopaminergic pathways. With the introduction of second-generation antipsychotics, these reactions have become more rare. 43 A dopaminergic abnormality has also been investigated by Simonyan et al 44 using positron-emission tomography (PET). Using the radioligand raclopride, they studied striatal dopaminergic neurotransmission and found that, compared with healthy controls, patients with SD had bilaterally decreased binding of raclopride to striatal dopamine D2/D3 receptors by 29%. In addition, these patients had worsening dopaminergic function during speech production in the left striatum. 44
Sensory-processing disturbances
Sensory-processing disturbances for visual temporal discrimination but not for tactile spatial discrimination were found in SD in comparison with healthy controls. 45 Other studies have found sensory-processing abnormalities in other focal dystonias: a higher somatosensory temporal discrimination threshold (STDT) was found in patients with cervical dystonia than in healthy controls. 46 Laryngeal sensory abnormalities have not been examined in SD but were found in patients with Parkinson’s disease. 47 As other types of focal dystonias have also shown deficits in the spatial domain, with impaired fingertip orientation sensitivity, 48 such studies of laryngeal sensory functioning are needed in SD. 13 However, studies of laryngeal sensorimotor reflexes in SD have shown decreased inhibition of late laryngeal adductor responses in AdSD 49 and in AbSD, 50 indicating that inhibitory mechanisms were impaired for laryngeal sensory reflexes in SD.
Functional neuroimaging studies in SD
Neurophysiological studies using PET have shown reduced activation in the heteromodal sensory areas during speech in persons with AdSD compared with volunteers. These deficits were reversed following treatment with BoNT injection. 13 However, functional magnetic resonance imaging studies found increased activation in the primary somatosensory cortex, basal ganglia, thalamus, and cerebellum during vocalization in SD. These differences tended toward a positive correlation with symptom severity. 51 It is not clear to what degree the difference in tasks or imaging methodologies contributed to these difference in results.
Neuroanatomical differences
Using volumetric segmentation and voxel-based morphometry of magnetic resonance images, significant reductions in whole-thalamic gross volume were found in cervical and laryngeal dystonia compared to healthy, age-matched controls. 52 This was the only region reduced and was a common finding in both forms of focal dystonia, although they involved different body regions. 52 No difference was found between SD and cervical dystonia, and thus it seems that reduced gross thalamic volume may be involved in both dystonias but does not dictate the site of symptoms. 52 However, this gross anatomical method cannot be used to identify specific reductions in volume or particular thalamic nuclei or neuronal subpopulations.
Focal altered microstructural integrity along the right genu of the internal capsule of the corticobulbar and corticospinal tract (CBT/CST) was found using diffusion tensor imaging and in neuropathological investigation of 1 case of SD. 53 Deficits along the CBT/CST can alter neural control between cortical and subcortical brain regions that are essential for voluntary voice production ( Figure 1 ).
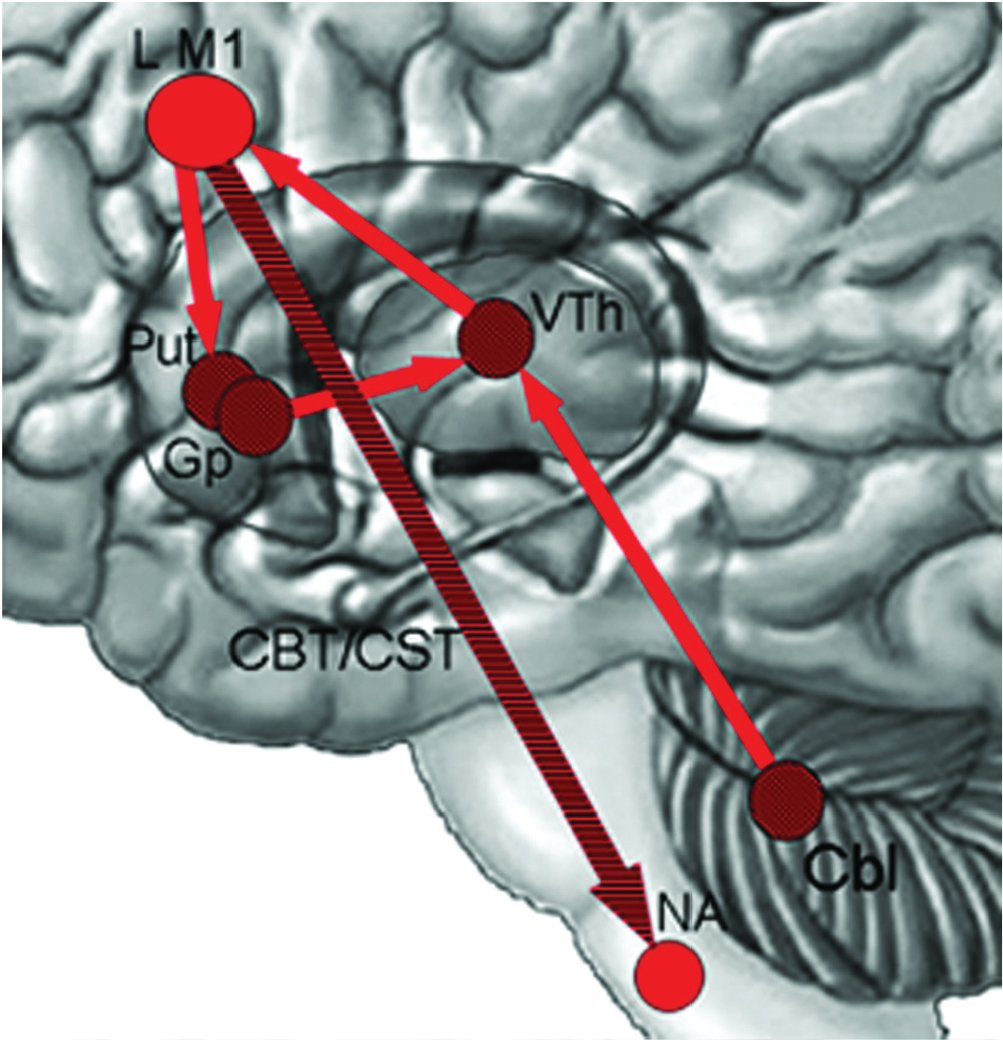
Neural network of voluntary laryngeal control: LM1 (laryngeal motor cortex) to phonatory motor nuclei (nucleus ambiguous, NA), descending via the corticobulbar/corticospinal tract (CBT/CST). Cbl, cerebellum; Gp, globus pallidus; Put, putamen; VTh, ventral lateral thalamus. Reproduced, with permission by Oxford University Press and the author, from Simonyan K, Tovar-Moll F, Ostuni J, et al. Focal white matter changes in spasmodic dysphonia: a combined diffusion tensor imaging and neuropathological study. Brain. 2008;131:447-459. © Oxford University Press 2007.
Multiple studies have demonstrated abnormalities in cortical inhibition, as evidenced by a shorter CSP and GABA-ergic dysfunction, sensory-processing disturbances, and neuroanatomical findings. Not only do these differences help define the neuropathological processes involved in SD, but they may also be considered possible adjuncts in cases of SD that present diagnostic challenges. These neurological abnormalities may also be targets for future treatment of patients with refractory SD.
Conclusion
SD is a complex disorder likely due to a multifactorial etiology, including neurological, genetic, and environmental factors. Epidemiological risk factors have been suggested from several large cohort studies. The most commonly identified characteristics are females in their middle decades of life, a family history of neurological diseases including dystonia, recent life stressors, upper respiratory tract infections, and a history of childhood measles or mumps. Knowledge of these risk factors for SD may be very valuable in identifying a typical or “at-risk” patient population for SD. They may contribute to a diagnosis of SD in patients where a clear clinical picture may not exist. Some of these risk factors, including viral illnesses, also point toward neural pathway dysfunctions as an etiological factor in the pathogenesis of SD. In patients with a genetic predisposition, some of these risk factors, such as viral illnesses, may lead to the development of SD.
Some genetic contributors have been suggested as contributing to the pathogenesis of focal dystonias, but a clear link with SD remains elusive. This may be a fruitful area for future research, with the advent of further developments in this field.
There are likely multiple neurological processes involved in the pathophysiology of SD: reduced cortical inhibition, sensory-processing and reflex disturbances, and neuroanatomical findings at several different levels. Thus, SD should be considered an integrative system disorder, rather than a disorder with a single pathological focus. Some of these neural abnormalities, such as reduced CSP for the masseter and visual temporal discrimination testing, could possibly be exploited as diagnostic adjuncts in the future. Others, such as neurotransmitter dysregulation, may provide treatment targets for long-term benefits in patients with SD.
The pathogenesis of SD may be viewed as a multiple-hit mechanism, with endogenous predispositions and environmental triggers contributing to produce the underlying abnormalities.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This work was previously presented as a poster at the American Laryngological Association’s 2017 Spring Meeting at COSM; April 26-28, 2017; San Diego, California.