
Abstract
Objective
Home oximetry is commonly used to screen for obstructive sleep apnea (OSA) in children; however, normal oxygen desaturation levels by disease severity are not well known. It was our objective to determine if oxygen saturation levels differed by OSA severity category in children and if these differences were similar for preteen children and adolescents.
Study Design
Retrospective case series of children undergoing polysomnography from September 2011 to July 2015.
Setting
Tertiary pediatric hospital.
Subjects and Methods
Six- to 18-year-olds (preteen, 6-12 years old; adolescent, 13-18 years old). Chi-square, Wilcoxon rank sum test, and Kruskal-Wallis testing were used to compare variables between age groups.
Results
The study included 342 children with a mean age of 11.3 ± 2.4 years (range, 6.5-17.5) and a mean body mass index of 25.6 ± 9.2 kg/m2 (78 ± 29 percentile); 61% were white, 35% were black, and 4% were other or unknown. Of the children, 48% were female, and this was not a significant difference between age groups (P = .81). Overall, 50% of the children had no OSA, 32% mild, 10% moderate, and 8% severe. When compared with the younger children, the adolescents had a longer sleep time (P = .014) and a higher mean obstructive apnea-hypopnea index (3.53 ± 5.1 vs 3.03 ± 6.1 events per hour, P = .02). The 3% and 4% oxygen desaturation indices were not significantly different between age groups when accounting for OSA severity.
Conclusion
Adolescents have longer sleep times and higher obstructive apnea-hypopnea indexes than preteens, but oxygen saturations and desaturation indices were similar. This supports current triage algorithms for children with OSA, as we found no significant age-based differences.
Keywords
Pediatric sleep-disordered breathing occurs in up to 20% of children, while its most severe form, obstructive sleep apnea (OSA), occurs in 2% to 4% of children. The gold standard for diagnosis of OSA is polysomnography (PSG). However, in the United States, PSG is expensive, and there is a limited number of sleep laboratories that can appropriately evaluate pediatric patients. Long wait times for evaluation may lead to delays in diagnosis. Sequelae of OSA include neurobehavioral changes, cardiovascular disease, depression, metabolic syndrome, and somatic growth impairment. 1
Oximetry data have been employed to assess for sleep-disordered breathing/OSA and have shown a high positive predictive value (PPV) but low negative predictive value (NPV) for the diagnosis of OSA.2,3 When compared with PSG, oximetry is much more affordable, is more easily available, and can often be done in the home setting where sleep quality may more closely reflect a baseline sleep. This, in turn, can result in more timely testing, which can reduce the interval between diagnosis and treatment and lessen the morbidity associated with OSA. 4 The output for oximetry is most commonly reported as the oxygen desaturation index (ODI), measured as the amount of time spent with a 3% or 4% desaturation from the patient’s baseline. The ODI has been validated as a useful screening tool for the presence and severity of OSA in children.5-7
While normal PSG has been described in adolescents, home oximetry has been primarily evaluated in preteen children, and there are no published data that report typical ODI findings for adolescents. In addition, normal oxygen desaturation levels by disease severity are not well described for children with OSA. It was our objective to determine if oxygen saturation levels differed by OSA severity in children and if these differences were similar for preteens and adolescents.
Materials and Methods
Study Subjects
We carried out a retrospective case series of pediatric patients between the ages of 6 and 18 years who underwent PSG between September 2011 and July 2015 at Cincinnati Children’s Hospital Medical Center (CCHMC). All sleep studies were carried out in a pediatric sleep laboratory. We included consecutive children who underwent standard diagnostic PSG, which was recorded on the PSG software TWin (Grass Technologies, Pleasanton, California). PSG is ordered routinely in the sleep clinic for children who snore or have signs of sleep-disordered breathing. However, the children referred by the otolaryngologists (representing approximately 10% of the clinical volume) are more likely to have comorbidities, fewer daytime symptoms, or small tonsils. Children were excluded if they underwent a positive pressure PSG titration study, an oxygen titration study, or an extended montage electroencephalogram study or had <2 hours of total sleep time. Approval for the study was obtained from the CCHMC Institutional Review Board.
Overnight PSG
All patients underwent an overnight PSG in a pediatric sleep laboratory at CCHMC. The following parameters were recorded simultaneously: body position, bilateral electrooculogram, ≥3-channel electroencephalogram, chin electromyogram, anterior tibialis electromyogram, tracheal microphone, electrocardiogram, pulse oximetry, thoracic and abdominal inductance plethysmography, and nasal pressure transduction. Scoring of the PSG was performed with standard criteria as defined by the American Academy of Sleep Medicine. 8 Sleep stage and respiratory scoring were performed by a certified sleep technician and a board-certified sleep physician. An obstructive apnea was defined as a cessation or decrease in airflow or a decrease in the sum channel from inductive plethysmography by >90% of the preceding breath. An obstructive hypopnea was defined as a decrease in airflow or a decrease in the sum channel from inductive plethysmography by >30% when compared with the preceding breath, which was associated with an oxygen desaturation ≥3%, an arousal, or an awakening. All obstructive events were ≥2 breaths’ duration. The number of apneas (including central apneas) and hypopneas per hour were calculated and reported as the apnea-hypopnea index (AHI). The obstructive AHI (oAHI) was defined as the number of obstructive apneas and hypopneas per hour. Oxygen desaturation indices were measured at the 3% and 4% levels relative to the baseline saturation for each individual. After artifact was found in the original sample, the SaO2 signal was resampled at 1 Hz. Desaturations of 3% and 4% were identified in the resampled signal, and desaturations at a <60% threshold were excluded as artifact.
Clinical Definitions
Subjects were considered to have OSA if their PSG showed an oAHI ≥1 event/hour, with oAHI ≥1 and <5 classified as mild OSA, ≥5 and <10 classified as moderate, and ≥10 classified as severe. Non-OSA snoring was seen in the absence of apneas or hypopneas.
Oximetry Evaluation
The oxygen saturation nadir was defined as the lowest oxygen saturation data point during an obstructive episode.
Statistical Analysis
Data distributions were reported as means with standard deviations, medians with ranges for continuous variables, and frequencies with percentages for categorical variables. Patients were stratified into groups based on age: preteen children (6- to 12-year-olds) and adolescents (13- to 18-year-olds). Differences in the demographic characteristics between the age groups were tested with chi-square for categorical variables or 2-sample t test for continuous variables. Because the oximetry and polysomnographic parameters were not normally distributed, the distributions of these factors were also reported as medians with the interquartile ranges. Differences in these factors between the groups were tested with the Wilcoxon rank sum test. Differences across OSA disease severity regarding oximetry and PSG parameters were tested with the Kruskal-Wallis test. This analysis was also stratified by age group (6-12 and 13-18 years) to understand whether a difference existed in the association with the parameters and OSA severity by age group. Differences by age group in the desaturation indices for each OSA category were tested with a Wilcoxon rank sum test. Reported P values were then adjusted for multiple comparisons with the Bonferroni correction.
Results
Overall, 342 children were studied; 266 were aged 6 to 12 years. Female patients accounted for 47.5% (n = 160) of the study group. The mean overall body mass index percentile was 77.9 ± 28.6 and was statistically but not clinically significantly higher for younger children (78.8 ± 27.9) than for adolescents (75.0 ± 31.2, P = .034). Demographic data for the entire cohort can be found in Table 1 .
Demographic Data for Children Undergoing Polysomnography: Preteenager and Adolescent Groups.
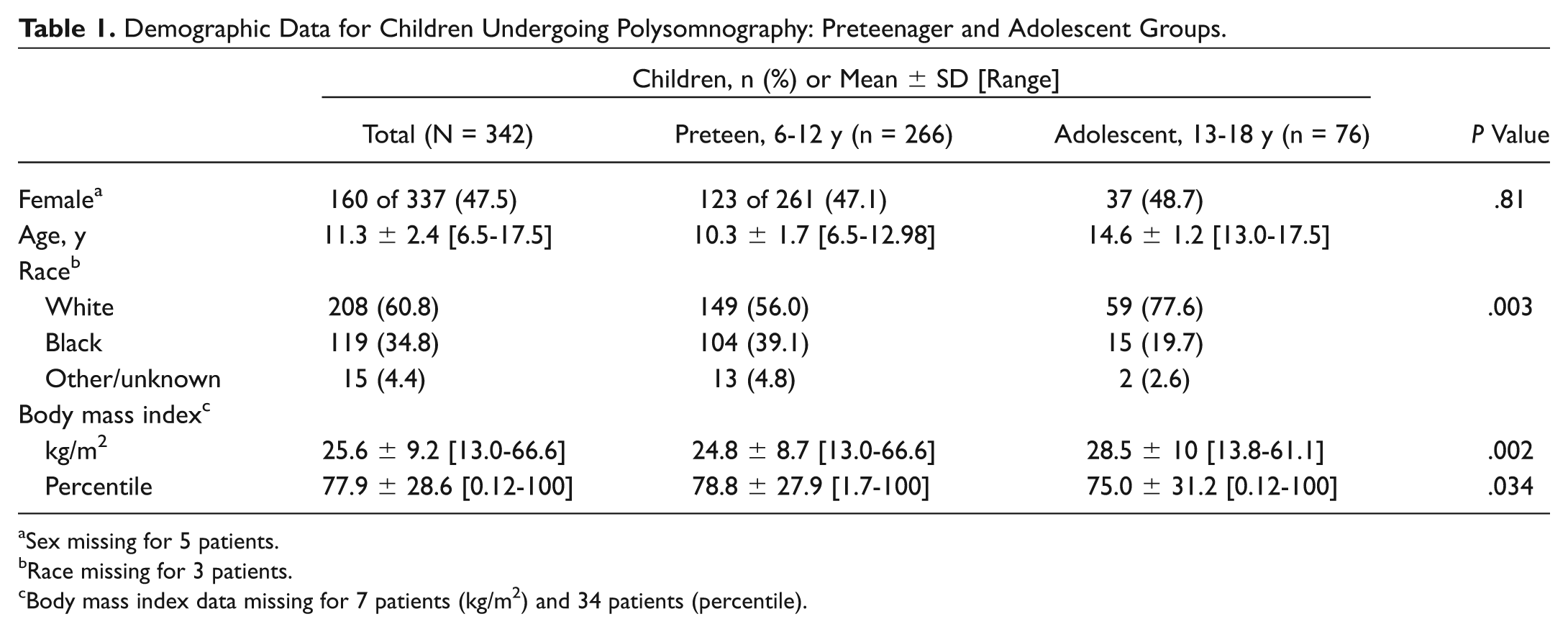
Sex missing for 5 patients.
Race missing for 3 patients.
Body mass index data missing for 7 patients (kg/m2) and 34 patients (percentile).
Oximetry and PSG parameters can be found in Table 2 . When compared with the younger children, the adolescents had a longer sleep time (P = .014) and a higher mean oAHI (3.53 ± 5.1 vs 3.03 ± 6.1 events/hour, P = .02). Neither the saturation indices nor the time with oxygen saturation <80% or <90% differed significantly between the groups. A scatter plot comparing ODI with AHI demonstrated a high correlation between the variables ( Figure 1 , correlation coefficient = 0.92).
Oximetry and Polysomnographic Parameters Comparing Those in the Preteenager Group and the Adolescent Group.
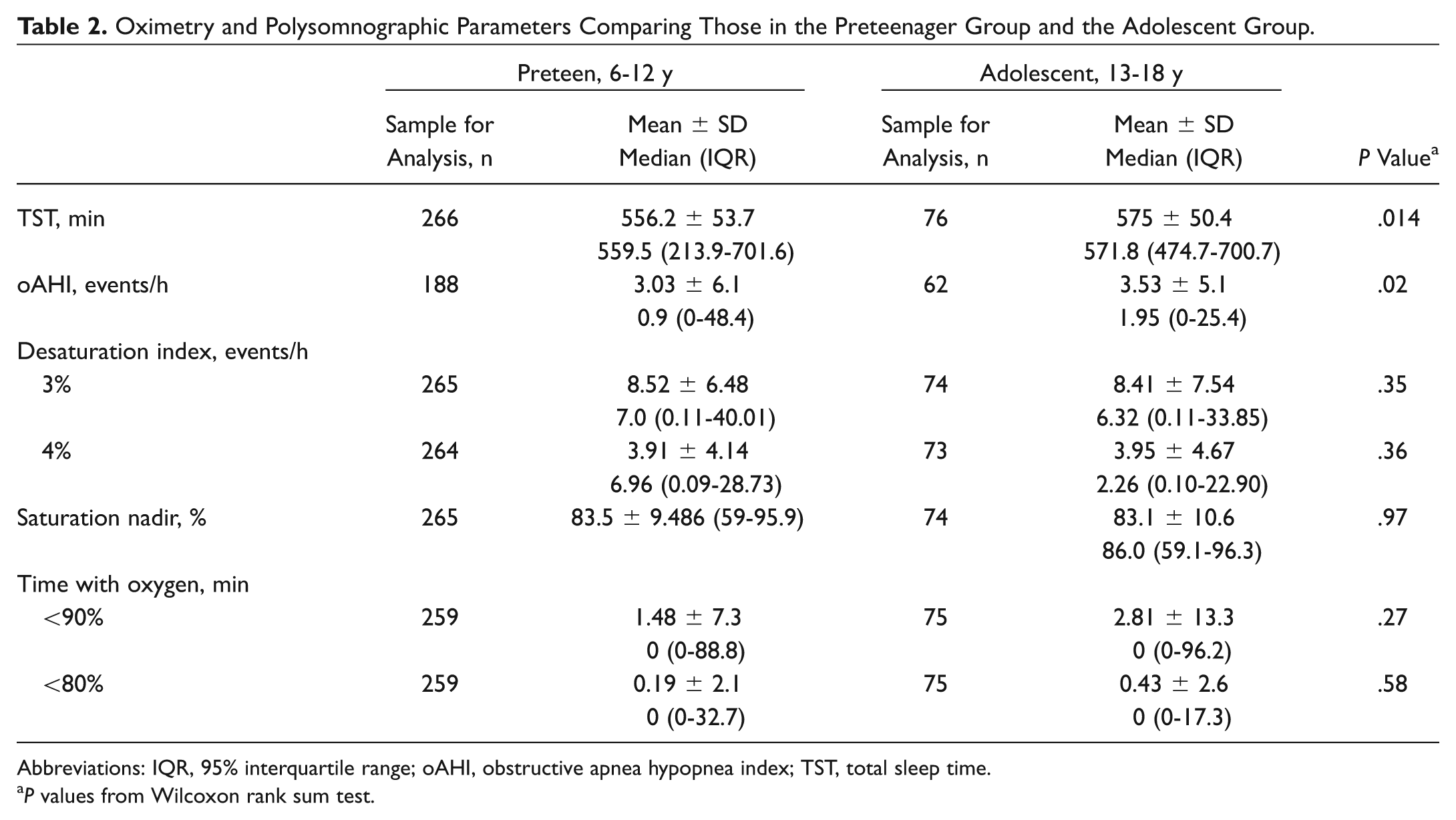
Abbreviations: IQR, 95% interquartile range; oAHI, obstructive apnea hypopnea index; TST, total sleep time.
P values from Wilcoxon rank sum test.
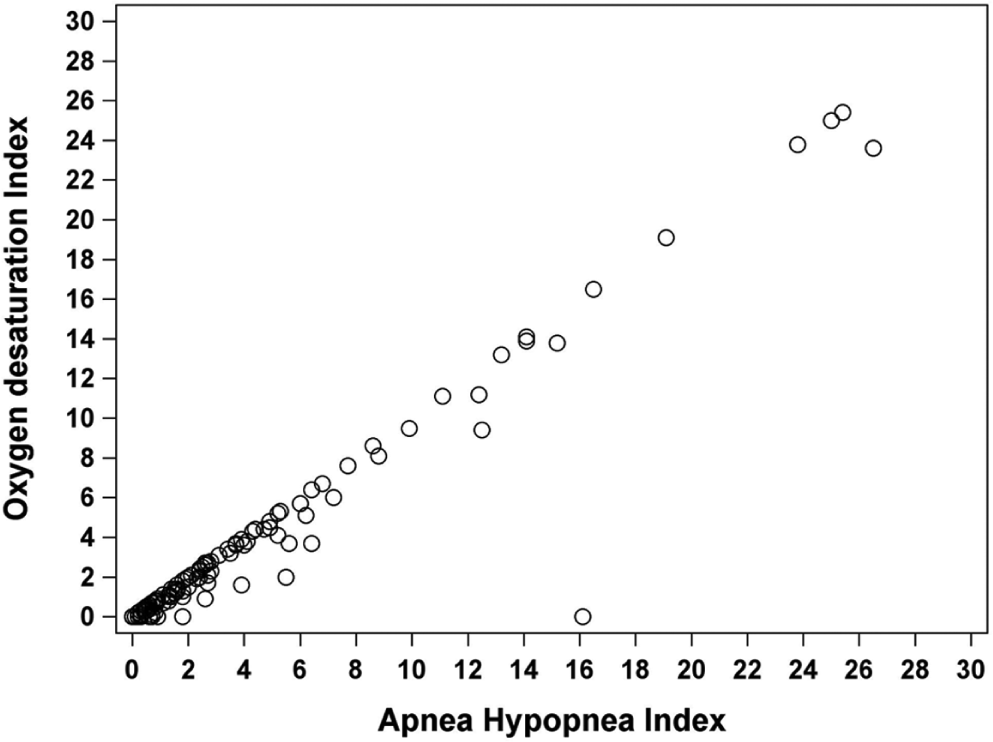
Scatter plot demonstrating the relationship between the oxygen desaturation index and the apnea-hypopnea index for children between 6 and 18 years of age. Correlation coefficient = 0.92.
Table 3 details the oximetry and PSG parameters for children by OSA disease severity. There was no difference in total sleep time by disease severity (P = .34). However, the desaturation indices worsened with the degree of OSA severity at the 3% and 4% desaturation levels. Children without OSA had a median 3% desaturation index of 4.66 events/hour; those with mild OSA, 8.07 events/hour; those with moderate OSA, 10.36 events/hour; and those with severe OSA, 22.28 events/hour (P < .0001). At the 4% desaturation index cutoff, children without OSA had a median 1.64 events/hour; those with mild OSA, 3.19 events/hour; those with moderate OSA, 4.17 events/hour; and those with severe OSA, 13.97 events/hour (P < .0001). Time spent with saturations <90% had a median of 0 for each age group across OSA severities, although the interquartile ranges increased with worsening OSA severity (P < .0001). This was also true at the time spent with saturations <80% cutoff (P < .0001).
Oximetry and Polysomnographic Parameters for All Children (6-18 Years Old), by Disease Severity, Comparing Those with and without Obstructive Sleep Apnea.
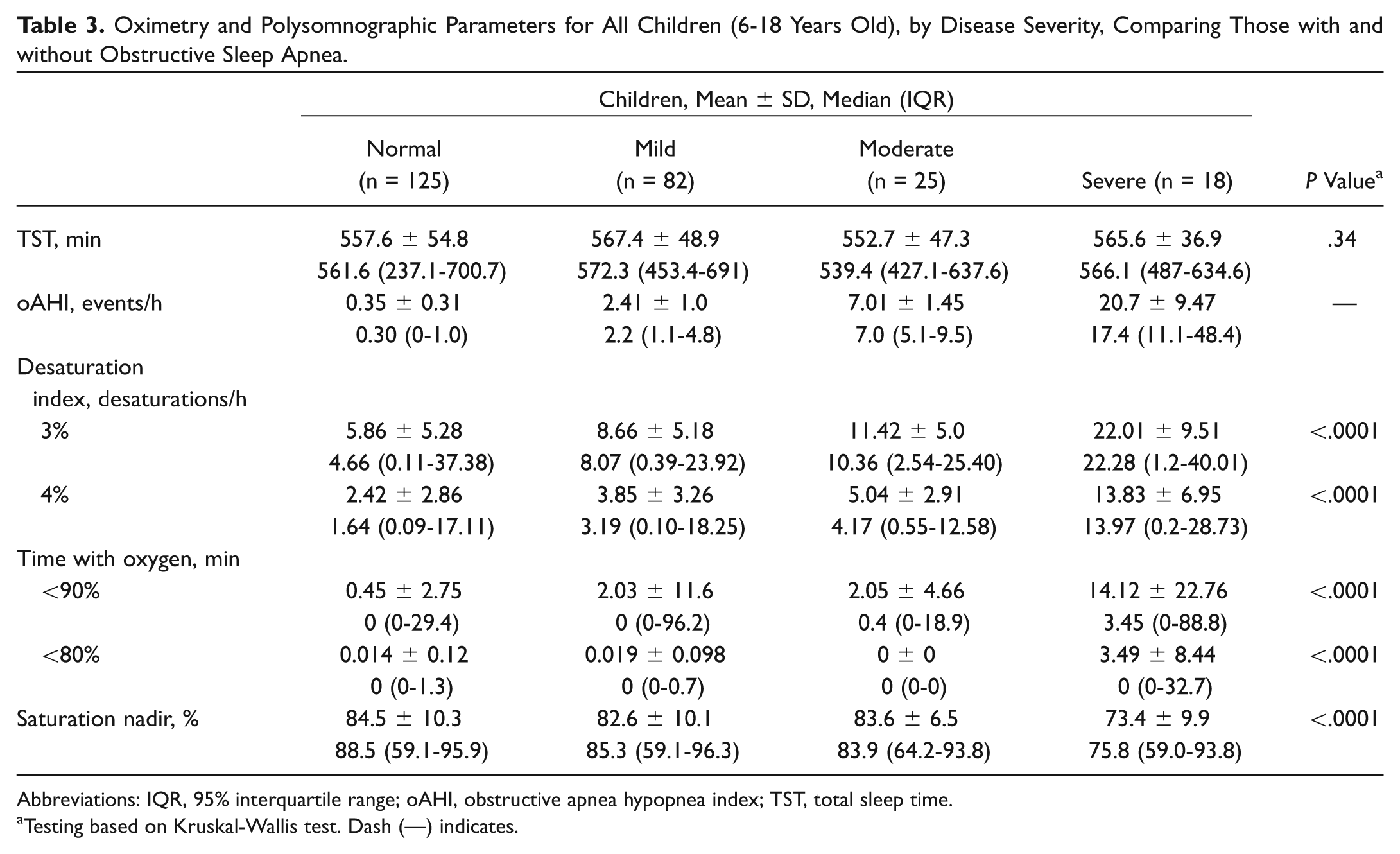
Abbreviations: IQR, 95% interquartile range; oAHI, obstructive apnea hypopnea index; TST, total sleep time.
Testing based on Kruskal-Wallis test. Dash (—) indicates.
Tables 4 and 5 detail the oximetry and PSG parameters for the age groups individually. The median 3% desaturation indices for the 6- to 12-year-old children (normal = 5.05 events/hour, mild OSA = 8.29, moderate OSA = 11.58, and severe OSA = 12.43) were significantly higher than those for the 13- to 18-year-olds only for those with moderate OSA (P = .013); this was not significant when adjusted for multiple comparisons (P = .052; normal = 3.75 events/hour, mild OSA = 7.99, moderate OSA = 8.48, and severe OSA = 21.13). There was no significant difference in median 4% desaturation indices between the 6- to 12-year-olds (normal = 1.67 events/hour, mild OSA = 3.35, moderate OSA = 5.03, and severe OSA = 13.99) and the 13- to 18-year-olds (normal = 1.25 events/hour, mild OSA = 2.91, moderate OSA = 3.37, and severe = 13.96). The saturation nadir was significantly different across severity groups among the preteens (P = .0001), but for the older age group, there was no significant difference by OSA severity (P = .38). However, the difference is significant between adolescents with no sleep apnea and severe OSA (P = .0003). Time with saturations <80% and <90% overall increased with increasing disease severity in both age groups (P < .005).
Oximetry and Polysomnographic Parameters for Children between 6 and 12 Years of Age with and without Obstructive Sleep Apnea by Disease Severity.
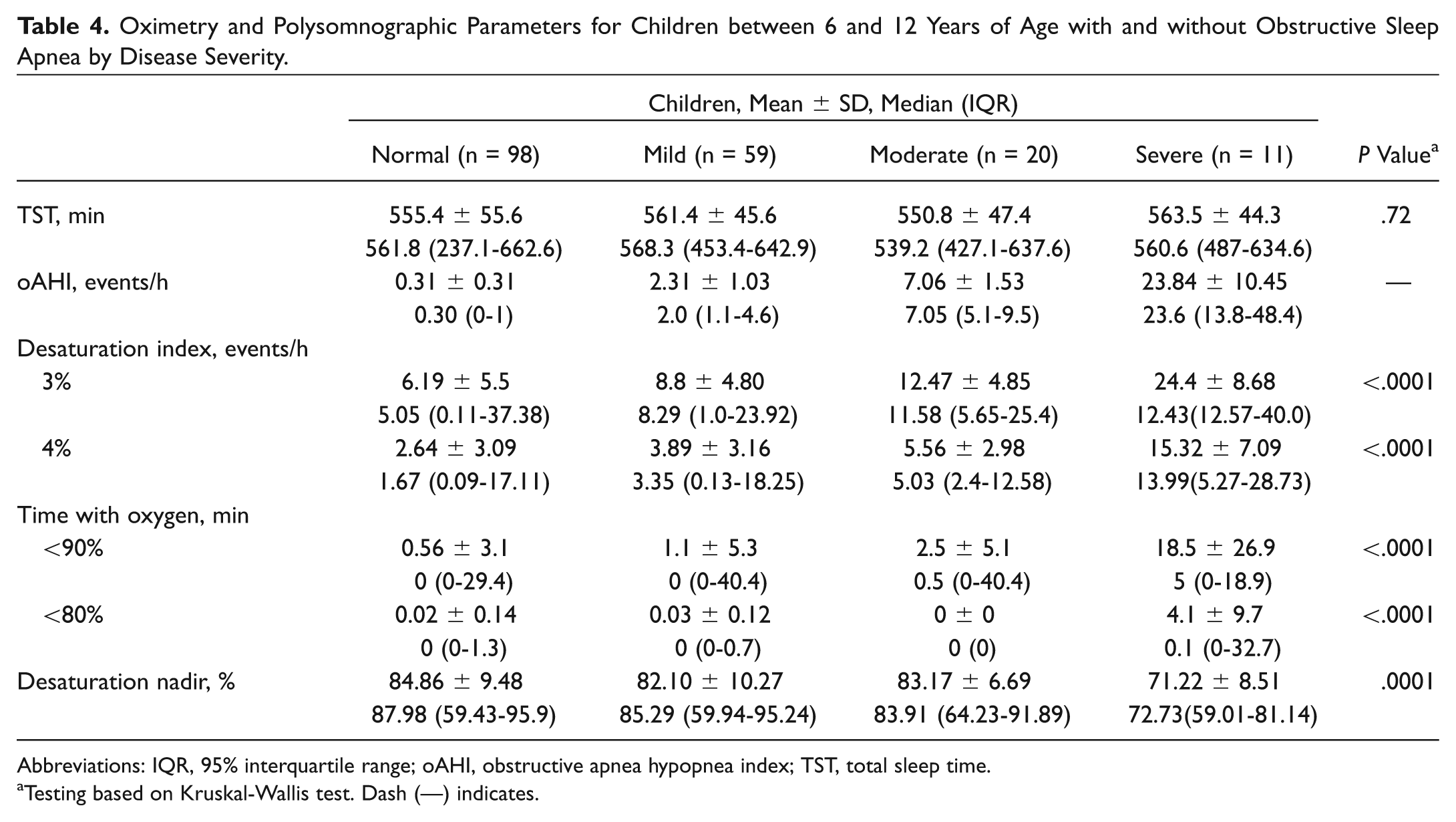
Abbreviations: IQR, 95% interquartile range; oAHI, obstructive apnea hypopnea index; TST, total sleep time.
Testing based on Kruskal-Wallis test. Dash (—) indicates.
Oximetry and Polysomnographic Parameters for Children between 13 and 18 Years of Age with and without Obstructive Sleep Apnea by Disease Severity.
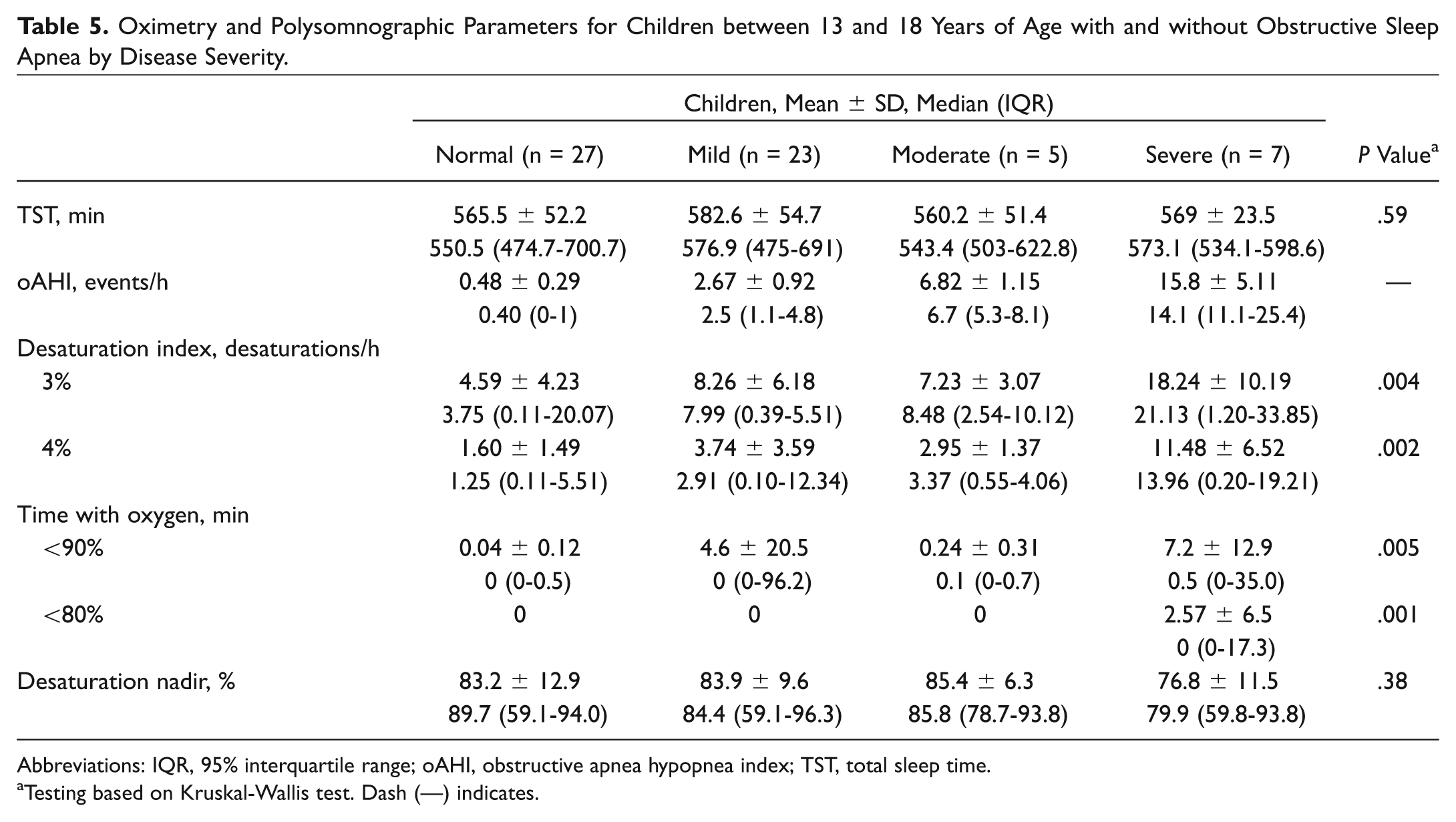
Abbreviations: IQR, 95% interquartile range; oAHI, obstructive apnea hypopnea index; TST, total sleep time.
Testing based on Kruskal-Wallis test. Dash (—) indicates.
The correlations between ODI and AHI for the entire study population are shown in Table 6 with 95% CIs. For an AHI ≥5 with an ODI cutoff >2.40 the sensitivity was 88.5%, specificity 41.5%, PPV 60%, and NPV 78.5%. For an AHI ≥1 and with an ODI cutoff >1.19, the sensitivity was 93%, specificity 56%, PPV 31%, and NPV 97%.
Correlation between ODI and AHI in Children between 6 and 18 Years of Age (95% CI). a
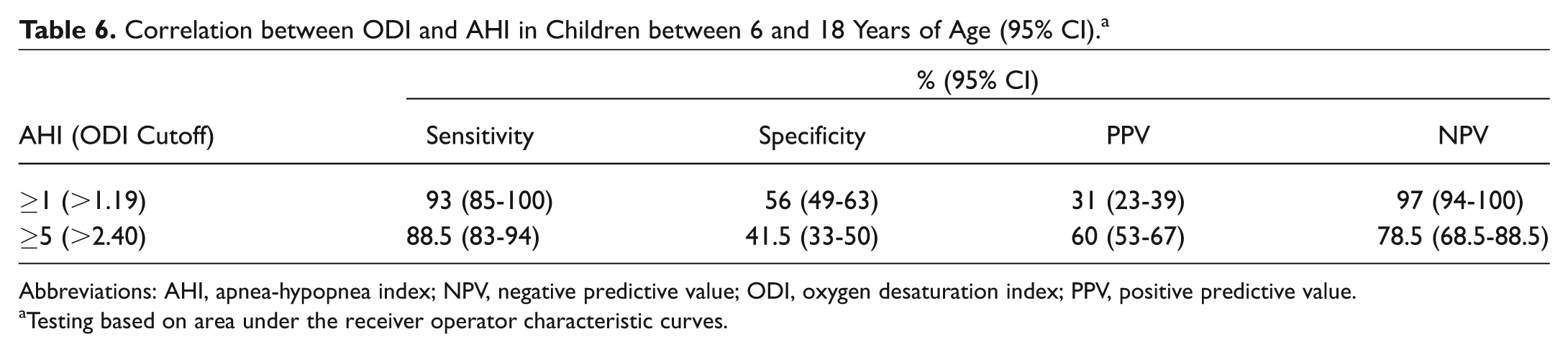
Abbreviations: AHI, apnea-hypopnea index; NPV, negative predictive value; ODI, oxygen desaturation index; PPV, positive predictive value.
Testing based on area under the receiver operator characteristic curves.
Discussion
In this study of 342 children, we compared the relationship between oxygen saturation levels and OSA disease severity in preteen children and adolescents. In both age groups, we found that increasing OSA severity correlated with higher desaturation indices, more time with oxygen saturations <80%, and more time with oxygen saturations <90%.
We found that the adolescents (defined as 13- to 18-year-olds for this study) had significantly longer sleep times and an overall higher median oAHI than younger children. However, there was no significant difference between age groups for the ODIs at either the 3% or 4% cutoff and no significant difference in time with oxygen saturations <80% or time with oxygen saturations <90%. As expected, the oxygen saturation nadir decreased significantly with worsening OSA levels in the younger children. This same trend was seen in the adolescents but was not found to be significant. This is possibly due to the small sample size in this group, as <10 adolescents were included in the moderate and severe OSA groups.
Brouillette et al showed the high PPV (97%) of nocturnal oximetry in 210 patients with OSA. 2 The children in their study ranged in age from 6 months to 17 years, but data were not analyzed by age. Following that landmark study, the utility of oximetry has been repeatedly demonstrated in the literature. Suarez et al reinforced the utility of pulse oximetry in a cohort of 75 children with OSA between the ages of 2 and 16 years. 3 Tsai et al reported on the value of the ODI when evaluating 130 children with OSA (ages, 3-12 years). 5 In a separate study of 78 children with OSA, ages 21 months to 13.8 years, Chang et al used ODI to create an algorithm to be used for triaging treatment of OSA. 6 Of note, none of these studies evaluated patients by age subgroup as we did in the present study.
Because there was no significant difference between the age groups in our study with the 3% and 4% ODI, we chose to analyze the sensitivity, specificity, PPV, and NPV for the entire population. Our data show a high sensitivity (88.5%) when based on an ODI cutoff of 2.40 in evaluating for moderate OSA (AHI ≥5). Tsai et al used a cutoff of 3.5 for moderate OSA and calculated a sensitivity of 83.8%. 5 Chang et al used an ODI cutoff of 1 for AHI >1 and found 78% sensitivity. 6 For mild OSA with a cutoff of 2.5, Tsai et al found a 77.7% sensitivity. In the present study, a cutoff of 1.19 showed a high sensitivity (93%) and NPV (97%).
We think that these data could be useful when evaluating children for possible surgical intervention. The high sensitivity and NPV of the ODI suggest a convenient screening tool for OSA that may be achieved with simple pulse oximetry. We found that for children with similar OSA severity, the ODI was not significantly different between the age groups. Based on these findings, preteen children and adolescents may continue to follow the same treatment algorithms for OSA. However, further study of the impact of the differences in ODI and their correlation with secondary outcomes of OSA, such as neurocognitive and pulmonary dysfunction, is warranted to determine if they predict differences in ultimate patient outcomes.
Our study has several limitations. A single PSG system was used for data acquisition, which may suggest that these data are less generalizable; however, there are no known significant differences in validated PSG software outcomes. Second, a selection bias existed because many patients with a high likelihood of OSA were triaged directly to surgery without need for confirmatory testing based on history and physical examination alone. This bias more closely reflects the clinical decision making of standard otolaryngologist practice. It also likely explains the underrepresentation of severe OSA patients. Finally, oxygen saturation levels were more severe than expected based on literature norms. The data were reanalyzed to decrease as much noise in the oximetry signal as possible, and periods of artifact were identified and excluded. However, the use of home oximetry for a similar analysis, instead of the oximetry data from a PSG, may be useful to determine if this is due to normal variation or is an artifact of the oximetry equipment used in our American Academy of Sleep Medicine–accredited sleep laboratory. In spite of these limitations, these data provide a first look at differences in ODI between preteen and adolescent children with OSA.
Conclusion
As expected, the oxygen saturation nadir decreased significantly with worsening OSA levels in the younger children. This same trend was seen in the adolescents but was not found to be significant. We found that adolescents have a longer total sleep time and higher overall oAHIs than do preteen children, but the oxygen saturations and oxygen desaturation indices were similar between the groups. The fact that there is no significant difference in absolute oximetry values by age suggests that this method is just as valid in adolescents (on whom there is very little literature) as it is in younger children, who have been more extensively studied. This supports current triage algorithms for children with OSA.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2016 AAO-HNSF Annual Meeting & OTO EXPO; September 18-21, 2016; San Diego, California.