
Abstract
An objective evidence-based review of the metrics used to evaluate applicants entering our field ultimately found these figures to have upward trends without any major correlation to performance in residency. The rise of these metrics coincides with a yearly drop in senior applicants, and in 2017, nearly 10% of programs did not match their contingent. The causes of unmatched spots must be examined to ensure that the field of otolaryngology can continue to grow and attract medical students who will excel in our field. Considerations into revising the applicant selection process, early introduction and mentorship within the otolaryngology field, and changes to the current otolaryngology interview process are discussed.
As we prepare for a new interview season, we reflect on the stress and self-doubt that many of us faced when applying for an otolaryngology training position. Many current applicants are struggling with these same pressures and questions of self-worth, which Dr Schmalbach mentions in her timely letter to the editor. 1 Often, these questions boil down to simply “Am I good enough?” While this question has likely plagued applicants for years, this interview season feels different.
We have found ourselves at a crossroads as a specialty. Almost 10% of all programs did not fill their contingent in the 2017 match. While it is too early to know if this is simply an aberrant data point, a study of yearly trends demonstrates sequentially fewer ear, nose, and throat applicants per year. 2 Now that the forum on this topic has been broached, we must question ourselves again, now as otolaryngologists: Are we good enough?
After much discussion and a literature review trying to pinpoint the cause of unmatched spots, we hypothesize that there are 2 contributing factors: (1) medical students’ perception of what is required to successfully match in otolaryngology and (2) a selection process that is cumbersome and too narrowly focused on metrics that do not necessarily correlate to future performance as a clinician. We believe that we must try to establish short- and long-term goals to begin to address these issues.
Otolaryngology program directors report that United States Medical Licensing Examination (USMLE) scores, Alpha Omega Alpha status, clerkship grades, and interest in research are among the most important factors in deciding which applicants to interview. 3 In their discussion, Bowe et al presented the limitations of these ever-increasing metrics and their lack of association with performance in residency. 2 These trends may help explain why at 1 medical school, 80% of queried students felt that it was impossible or near impossible to match into otolaryngology. 4
In the face of this seemingly unobtainable ideal, and aided by an electronic application, motivated students began to apply to increasing numbers of programs. The addition of program-specific paragraphs to the application in 2015 was a well-intentioned effort to encourage applicants and programs to convey mutual interest. Despite this, there has been an increase in the number of applicants interviewing/ranking ≥16 programs ( Figure 1 ). With a quarter of applicants doing so in 2016, the result is a narrower pool of applicants considered for a fixed number of positions. This is reflected by the fact that the average number of ranked applications per position that are needed to fill a program increased from 4.4 to 7.1 between 2013 and 2017. 5
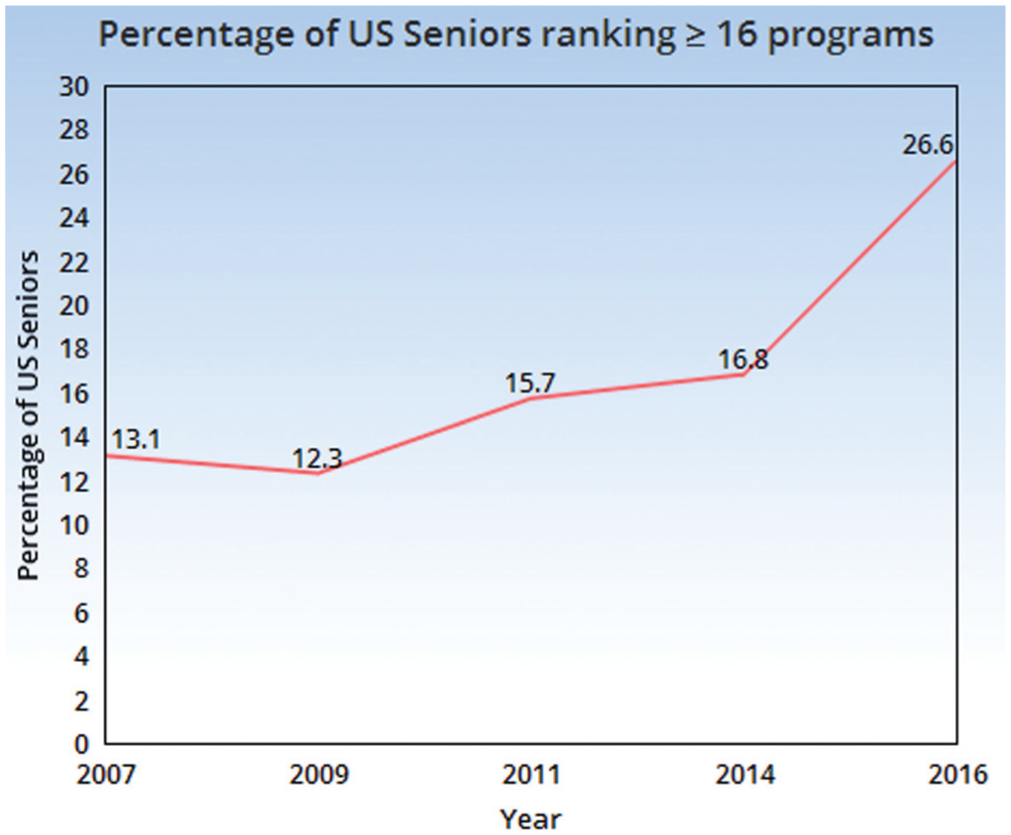
Percentage of US seniors ranking ≥16 programs. Information obtained from Charting Outcomes in the Match for the years 2007, 2009, 2011, 2014, 2016 (Washington, DC: National Resident Matching Program).
The immediate concern is that programs are interviewing the same group of applicants. We cannot blame applicants for taking as many interviews as possible. Rather, programs should articulate their unique mission clearly and identify applicants who fit their current and prospective identity, a process that is difficult through a generic application. This means that not every top applicant deserves strong consideration if interview spots and resources are limited.
The other concern is that, in the pursuit of finding and developing future academicians, the talent pool is artificially limited further by our selection process. It goes without saying that without innovation, we stagnate. Most, however, will say that academics is a calling. Only a third of residents expect to pursue an academic career track. 6 With the average residency having about 3 residents a year (2.77 per program), 3 designing a selection process focused on identifying and recruiting that lone resident seems shortsighted. This stresses the inherent conflict between departmental goals and residency program goals, the latter of which should be creating thoughtful, competent surgeon-physicians regardless of practice setting.
One change that we can consider making is declaring a fixed schedule of interview days for the entire specialty. If, for instance, programs scheduled their interviews among 12 preset days, this would limit the number of interviews to a maximum of 12 per applicant. We know empirically that 12 interviews show a steady >90% match rate and may also allow programs to truly gauge applicant interest. The result would be a more intentional interview process for applicants, rather than the “shotgun approach” of interviewing at every possible program in hopes of matching. Additionally, this would help to reduce overlap and address the concern that programs are interviewing the same handful of applicants.
Without a doubt, there have been several positive changes to our field for which we should be proud. We have become more diverse, with a larger number of minorities and women entering our field. As we strive toward inclusion, however, we are losing a different type of diversity—that of thought. We have self-selected those with early interest, research, and high board scores at the risk of excluding those with unique callings, skills, and viewpoints. This is done despite data to suggest that those with high performance in some nonacademic pursuits perform better during residency.7,8
Long term, we would benefit from greater access to our specialty. Our approach is too limited in scope and often focuses on publications and high USMLE scores. We should focus on a message that inspires individuals to apply to our specialty, not one that discourages them. Second, we should build medical student interest groups by increasing resident and attending participation. We can do this not only in person but via social media. At our institution, we are building subsidized pipeline programs to allow nontraditional students to participate in nonacademic tracks within the department, such as global health and leadership. Programs such as these not only increase exposure to our specialty and department but also help build lasting relationships, bolster applicant resumes, and provide opportunities to nontraditional applicants.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.