
Abstract
Objective
This study was performed to determine whether the efficacy and safety of medical management of uncomplicated peritonsillar abscess (PTA) presenting in the emergency department is equivalent to medical plus surgical therapy.
Study Design
Case series with chart review.
Setting
Southern California Permanente Medical Group (SCPMG).
Subjects and Methods
Upon successful completion of a prospective study comparing medical treatment (MT) to surgical treatment (ST) of PTA in 2008, MT was adopted by 12 SCPMG centers while 7 centers continued standard surgical drainage. Clinical outcomes are now reviewed on a random sampling of 211 patients with PTA treated with MT and 96 patients treated with ST between 2008 and 2013 at the respective medical centers. Patients were treated with intravenous (IV) fluids, weight-appropriate IV ceftriaxone, clindamycin, and dexamethasone, and then discharged on clindamycin × 10 days (MT). Patients in the ST group received MT but also surgical drainage. Primary end points were complication rates and failure rates.
Results
MT and ST resulted in no significant difference in treatment success or complications. However, patients in the MT group obtained significantly less liquid opioid prescriptions (MT, 30.8 ± 5.65; ST, 77.75 ± 13.41; P < .0001), reported fewer sore days (MT, 4.48 ± 0.27; ST, 5.77 ± 0.49; P = .0004), and required less days off from work (MT, 3.4 ± 0.44; ST, 4.9 ± 0.82; P = .044).
Conclusions
Compared to ST, MT appears to be equally safe and efficacious, with less pain, opioid use, and days off work, especially if patients with PTA present without trismus. MT for PTAs reduces the possibility of surgical complications, as well as the cost and inconvenience associated with ST.
Keywords
Peritonsillar abscess (PTA) is the most common deep space infection of the head and neck. PTAs have an incidence of 30 per 100,000 with about 45,000 new cases annually. The annual cost of treating PTAs has been estimated at over $150 million. 1 The predominant hypothesis for the pathophysiology of PTA is failure of drainage of bacteria from tonsillar crypts during acute tonsillitis, leading to migration of bacterial pathogens along lymphatic channels to adjacent structures. 2 Unchecked, this can lead to peritonsillar cellulitis, formation of a phlegmon, and finally abscess formation in the peritonsillar space. Untreated, PTA may progress with airway compromise, extension to deep neck spaces, bacteremia, and sepsis.
The earliest description of surgical drainage was in the 14th century by the French surgeon Guy de Chauliac and later by Chassaignac, who first reported “tonsillectomy à chaud” (quinsy tonsillectomy) in 1859. 3 Since then, surgical therapy for PTA in the United States has migrated from more aggressive approaches (quinsy tonsillectomy) to more conservative approaches such as incision and drainage (I&D) and needle aspiration (NA).4,5 Proponents of tonsillectomy argue that surgery is an expedient way of simultaneously treating the PTA and preventing recurrence, while proponents of conservative measures have argued that quinsy tonsillectomy is fraught with too high a rate of hemorrhage. 4 Those who favor I&D further argue that patients begin oral intake sooner than those who undergo NA. 4 In contrast, NA proponents have argued that quinsy tonsillectomy and I&D pose too great a hemorrhage risk to patients, and the success rate of NA is the same. In fact, failure rates of surgical intervention range from 6% to 20% while outcomes between the various techniques have been reported to be roughly equivalent.4-11
Several studies have shown benefits of steroid therapy and have suggested that PTA may be treated effectively with medical therapy alone.12-14 In 1 randomized trial, Ozbek et al 12 showed that after NA and inpatient admission for intravenous (IV) antibiotics, those receiving steroids instead of placebo had significant improvement in a number of clinical outcome measures, including improvement in trismus, resolution of fever, improved oral intake, and decreased length of hospital stay. A group working with the Indian Health Service in Arizona published a case series of purely medical therapy using high-dose steroids, antibiotic therapy with cephalexin, parenteral hydration, and anti-inflammatory therapy. They found this regimen successful in 96% of patients. Of the 98 patients in the study group, 2 underwent eventual NA and 2 were treated with I&D. 15
Given this background, a prospective, randomized pilot trial was performed comparing clinical outcomes of uncomplicated patients with PTA treated with either medical or surgical therapy. 16 This 2008 analysis revealed no significant difference in any of the outcomes: pain, time before oral intake, or time before returning to work. 16 A process improvement (PI) project was then implemented throughout Southern California Kaiser Permanente (SCPMG) using the following medical treatment (MT) algorithm for adult patients with uncomplicated PTAs (pediatric patients were treated with weight-appropriate dosages):
At time of diagnosis in the emergency department (ED):
D5 ½ normal saline, 1-L bolus
Dexamethasone 10 mg IV
Ceftriaxone 2 g IV
Clindamycin 600 mg IV
After discharge:
Clindamycin 300 mg per os (PO) qid × 10 days
Patients are observed in the ED for 1 to 2 hours after medication administration.
If patients are not significantly improved with the ability to take liquids by mouth, they undergo needle aspiration or incision and drainage.
Patients are followed up in the Department of Head and Neck Surgery the following day. If patients are significantly better, they are discharged. If they are not significantly better, they are either surgically drained or given another round of fluids, dexamethasone and ceftriaxone. After this second round of medications, if patients are not significantly improved with the ability to take liquids by mouth, they undergo surgical drainage.
Over the subsequent 5 years, 12 SCPMG service centers adopted medical therapy for the treatment of PTA while 7 continued standard surgical therapy. According to treatment location analysis, 92% of all PTAs treated at these 7 service centers between 2008 and 2013 were drained, while 92% of all PTAs treated at the 12 other service centers were exclusively treated with medical therapy and not surgical therapy. Given this split in PTA treatment at the different service centers, clinical outcomes of randomly selected patients with PTA treated medically or surgically could be examined with the proviso that patients in both groups received the same medications and that the only difference between the groups was whether or not they were surgically drained. We hypothesized that complication and failure rates would be equivalent with either form of PTA therapy.
Methods
Upon Kaiser institutional review board approval (10246), a chart review of PTA treatment outcomes throughout the SCPMG system from January 2008 to January 2013 was performed ( Figure 1 ). A total of 6782 patients were diagnosed clinically with a PTA by ED physicians during this period (International Classification of Diseases, Ninth Revision [ICD-9] code 475). Of these, 6132 (90%) were treated without a surgical intervention Current Procedural Terminology (CPT) code, while 650 (10%) were treated in the ED with a surgical intervention code (CPT 42700, 42999 or ICD-9 28.0). We narrowed the search down to 1747 patients with PTA who, according to the coding and documentation in their chart, had uncomplicated PTAs and received therapy exactly according to the PI protocol (MT). We reviewed these 1747 patients’ charts to see who received the same MT regimen but who also received standard surgical drainage at one of the 7 service centers where surgery was routinely performed, and 96 patients were identified (surgical treatment [ST]). Outcomes for these 96 ST patients were then compared to 211 randomly selected out of the 1747 MT patients treated without drainage at the other 12 service centers where medical therapy was primarily implemented. Both MT and ST patients were seen by an otolaryngologist at follow-up.
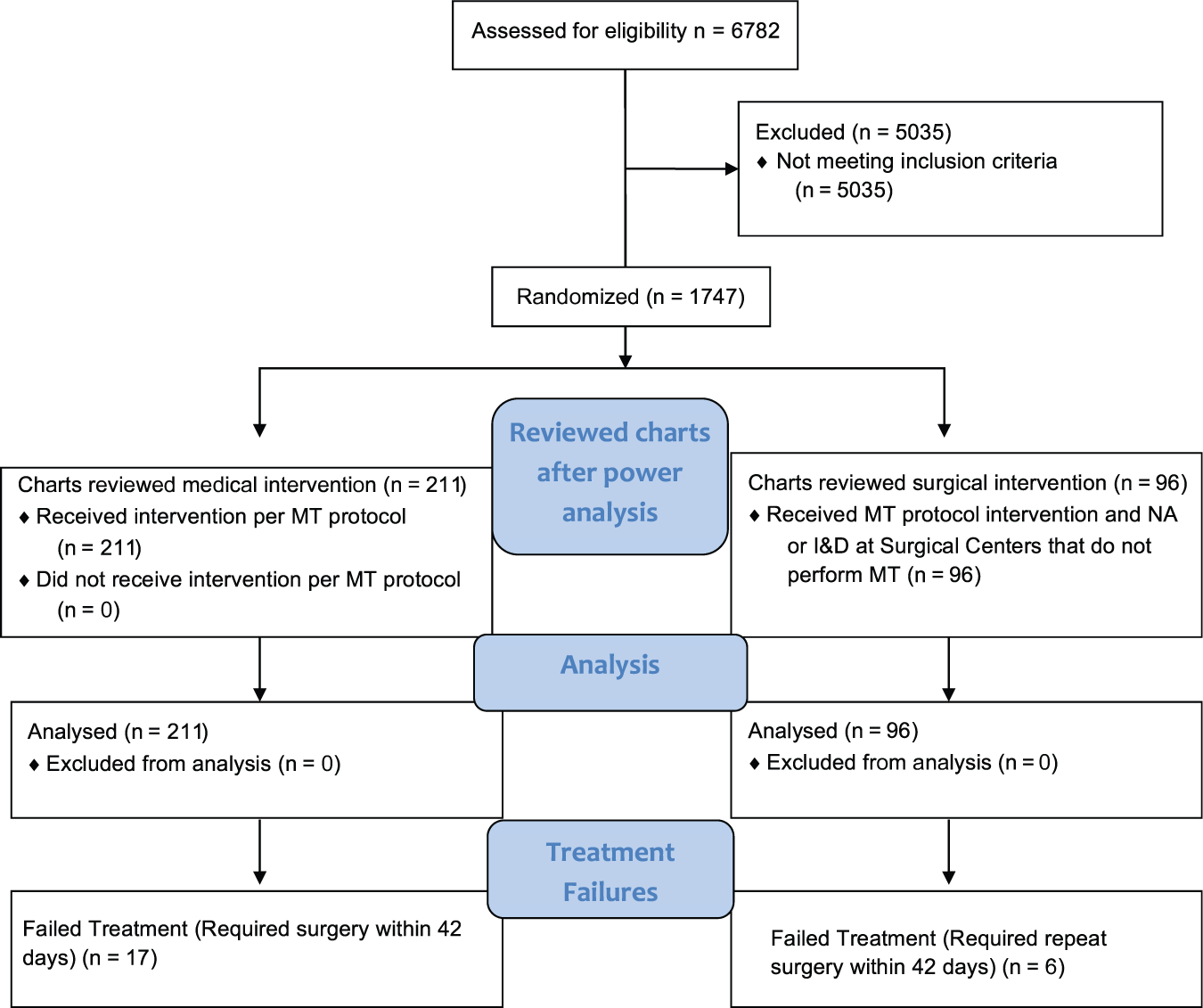
A chart review of peritonsillar abscess (PTA) treatment outcomes throughout the Southern California Kaiser Permanente system from January 2008to January 2013 was performed as above. I&D, incision and drainage; MT, medical treatment; NA, needle aspiration.
Using a priori power calculations, we had determined that at least 84 patients would be required in each ST and MT group to detect a statistically significant difference at the .05 level (with 80% power) between the 2 groups in each of the following outcome measures: pain, the volume of opioid prescribed, average number of sore days, days off of work, failure rates, and complication rates. In performing power calculations for pain outcomes, we looked for a 1-point difference in pain scores assuming a common standard deviation of 2 points and a 25-percentage point difference in proportions.
Attention was placed on early time points following presentation when there was the highest chance of a complication or failure. The following variables were recorded from charts on initial presentation, 1 to 2 hours after treatment, and at 1, 2, 3, 7, and 42 days after presentation: age, sex, hospital location, date, pain (1-10), history of fever, temperature, trismus, uvular deviation, toleration of liquids or solids, number of self-reported sore days (number of days that patients experienced pain after initial therapy), number of days until PO intake, volume of pus during surgery, difficulty breathing, bleeding, number of days off work, number or volume of opioid dispensed in first 42 days after diagnosis, number of clinic visits in first 42 days from diagnosis, failure of therapy, and complications. To ensure that enough time had elapsed for failure to occur, failure in each of the MT and ST groups was defined as a surgical procedure being performed within 42 days of the initial visit. Coded complications associated with PTAs were searched for in each group, including aspiration, bacteremia, hemorrhage, mediastinitus, parapharyngeal abscess, retropharyngeal abscess, sepsis, shortness of breath, syncope, palpitations, and weakness.
Statistical analyses, including Pearson χ2 tests, Wilcoxon rank-sum tests (WRSTs), Fisher exact tests, and logistic regression analysis, were performed on the data. Univariate comparisons between groups involved Pearson χ2 tests and Fisher exact tests for categorical variables and WRSTs for ordered (including continuous) variables. Noninferiority of MT vs ST was defined as no significant difference in outcomes. Multivariate analyses were performed to account for potential confounding variables. However, duration of symptoms prior to presentation, treatment received prior to presentation, history of narcotic use, patient weight, microbiology data, and specific type of surgical procedure were not recorded and, as such, are a limitation to this analysis.
Results
Baseline Characteristics
No statistically significant difference in the following baseline parameters could be identified at any time point: age, age range, sex, level of pain on a scale of 1 to 10, temperature, or the ability to eat liquids or drink solids ( Table 1 ). Patients in both groups did not have a PTA closer than the previous 12 months.
Baseline Characteristics of the MT and ST Groups, Establishing Equivalency (P > .05). a
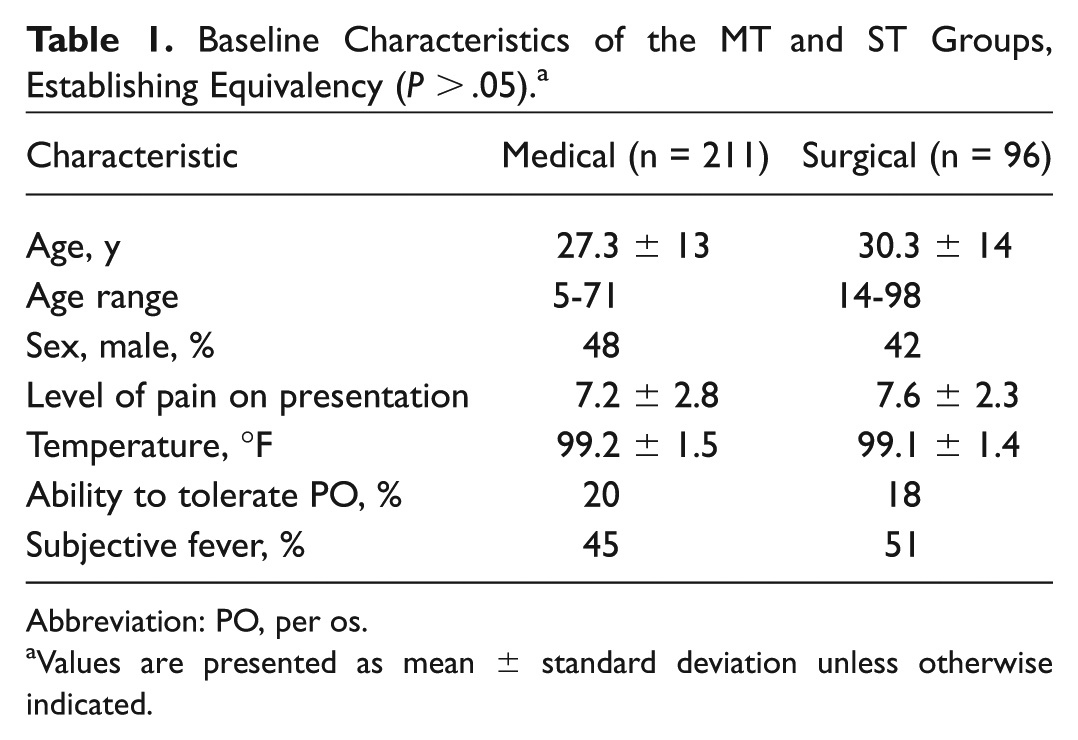
Abbreviation: PO, per os.
Values are presented as mean ± standard deviation unless otherwise indicated.
Volume of Opioid Prescription, Average Number of Sore Days, and Days Off Work
There was no statistically significant difference in volume of narcotic pain medication per prescription (acetaminophen/hydrocodone; MT = 213 mL, ST = 231 mL, P = .45 [WRST]). The dose of liquid medication was 15 to 25 cc every 4 to 6 hours as needed for pain. There was, however, a statistically significant difference in the volume of narcotic refilled between the groups ( Figure 2A ). Not only did the MT group have significantly fewer refills, but the MT group also demonstrated statistically less total liquid opioid prescribed (P < .0001).
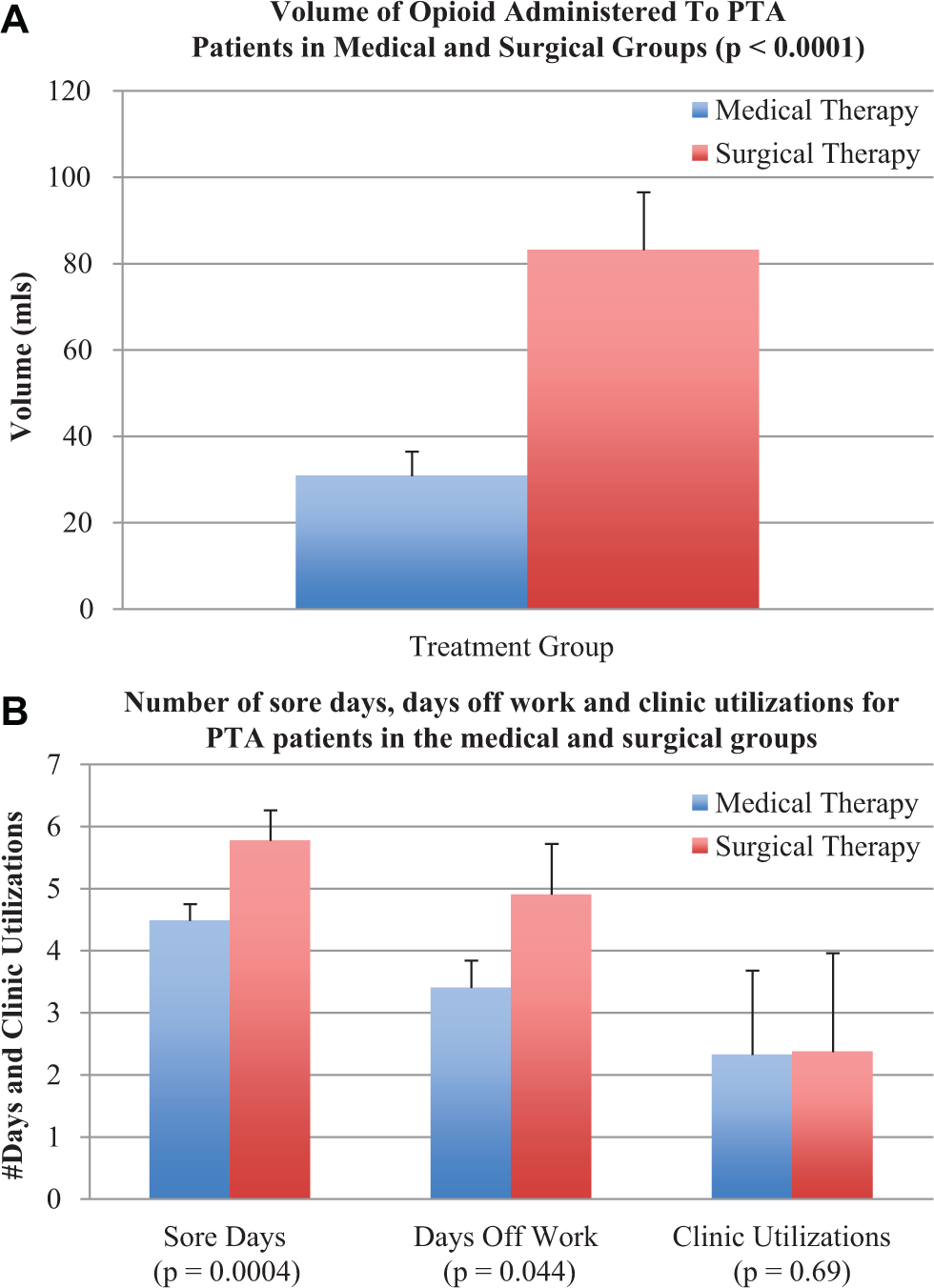
Distinguishing outcome measures between medical and surgical therapy for peritonsillar abscesses (PTAs). The data are as follows: opioid volume (medical treatment [MT] 30.84 ± 5.65 vs surgical treatment [ST] 77.75 ± 13.41; P < .0001), sore days (MT 4.48 ± 0.27 vs ST 5.77 ± 0.49; P = .0004), days off (MT 3.4 ± 0.44 vs ST 4.9 ± 0.82; P = .044), and clinic visits (MT 2.32 ± 1.36 vs ST 2.37 ± 1.59, P = .69).
MT patients also had significantly fewer “sore days” (P = .0004) and days off work (P = .044) compared to the ST group ( Figure 2B ). No statistically significant difference in any other outcome measure could be identified.
Complication and Failure Rates
The number of PTA-associated complications and diagnoses was recorded ( Table 2 ), along with the day on which the occurrence was noted. If the complication is not listed in Table 2, then it was not associated with PTA treatment in either group. No difference in complication rate could be determined, although there were more surgically related complications associated with a procedure. Seventeen patients (8.1%) in the medical group had a procedure reported within 42 days of diagnosis, and 6 surgical patients (6.2%) required a second procedure within 42 days, and these were considered treatment failures. There was no statistically significant difference in failure rates between the ST and MT groups (8.1% vs 6.2 %, P = .58) out to 42 days. No comorbidities such as diabetes predisposing these patients to failure could be identified, although it is possible that a predisposing factor toward failure was noncompliance or antibiotic resistance to clindamycin.
Associated Diagnoses in the Medical and Surgical Groups and the Day of Occurrence. a
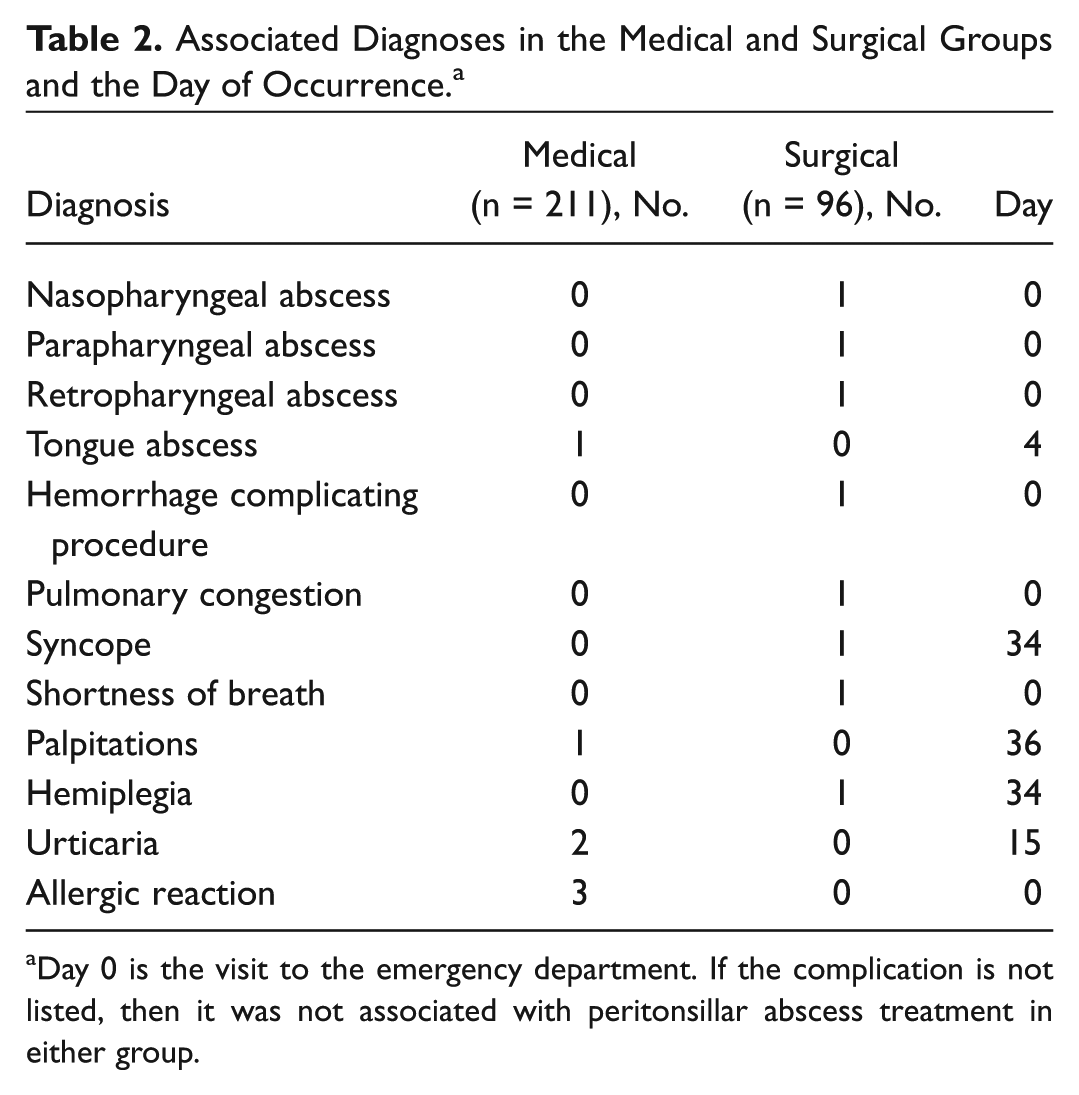
Day 0 is the visit to the emergency department. If the complication is not listed, then it was not associated with peritonsillar abscess treatment in either group.
Patients with Trismus
To address the issue of selection bias and evaluate whether patients who received ST had presented with greater severity than those in MT and therefore had worse outcomes, we looked at the subset of patients with PTA who had trismus.
There were 39 (18.4%) cases of trismus in the MT group and 44 (45.8%) in the ST group ( Table 3 ). Patients with trismus at presentation were more likely to have ST than MT (odds ratio, 3.8; 95% confidence interval, 2.2-6.5; P < .0001). In the MT group, 36 (92%) patients with trismus did not have a procedure, and 3 of the 39 subsequently received a procedure after the initial presentation (7.7% failure rate). Three of the 44 (6.7%) in the ST group had trismus at 24 hours, requiring a second procedure.
Patients with Peritonsillar Abscess Who Had Trismus. a
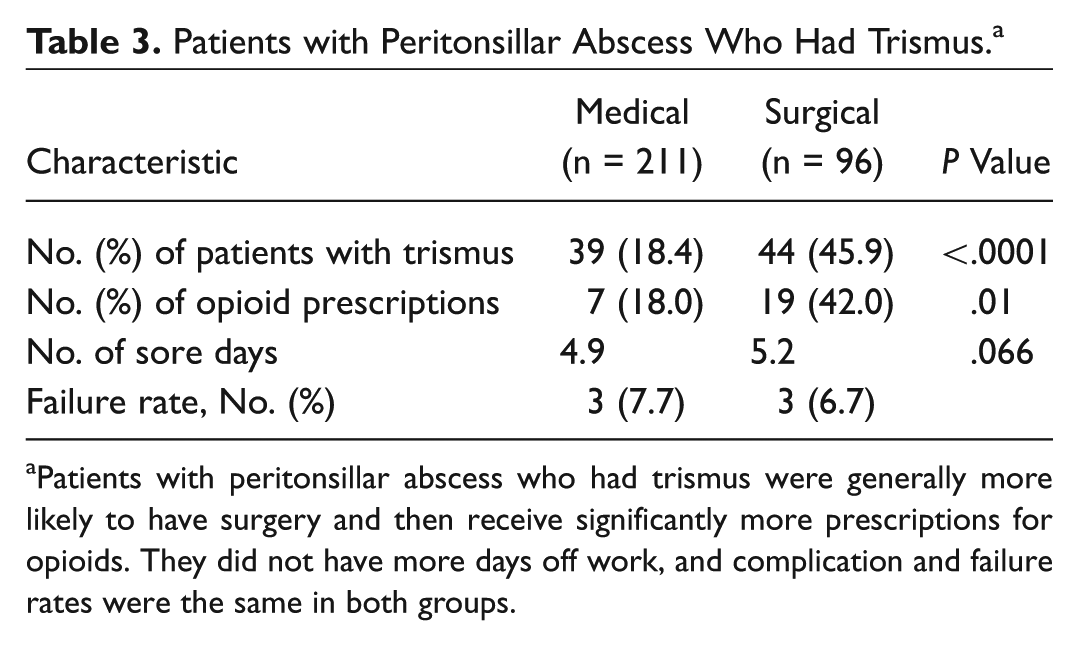
Patients with peritonsillar abscess who had trismus were generally more likely to have surgery and then receive significantly more prescriptions for opioids. They did not have more days off work, and complication and failure rates were the same in both groups.
Patients with trismus received a larger volume of pain medication than those without (P = .002 [WRST]), and patients with trismus who received ST received more opioid prescriptions than those treated with MT alone (P = .01) ( Table 3 ). There was no statistically significant difference in the number of sore days between the trismus groups (P = .066 [WRST]; 4.9 days MT, 5.2 days ST).
Discussion
Justification behind Treating PTAs with MT
Although I&D and NA have been the mainstay of PTA therapy for decades in the United States, they carry the risk of failure to drain the abscess, surgical complications, added cost, and discomfort to the patient, as well as a recurrence rate of 6% to 20%.4-11,17 The literature indicates there is no significant difference in efficacy between I&D and NA.4-9 These 2 techniques are essentially interchangeable from a success standpoint and also carry similar risks.4-9 Since PTAs typically begin as a cellulitis and progress to the phlegmon stage prior to maturing to an abscess, many patients who come to the ED do not have an abscess yet. In these cases, when I&D or NA is attempted, no pus is aspirated or expressed, and patients are exposed to the risk of an unnecessary procedure.
Basis for Antibiotic Choice and Use of Steroids
The literature is unclear with regard to the appropriate choice of antibiotics when treating a PTA. PTAs are known to be polymicrobial in nature.18-21 The most common organisms have been reported to be group A Streptococcus and Fusobacterium. 21 However, several studies have reported PTAs with penicillin-resistant infections with rates up to 58%,18-21 and broad-spectrum antibiotic therapy has shown superiority over single-agent protocols. 6 For these reasons, ceftriaxone plus clindamycin were given as the antibiotics of choice. This combination provides broad-spectrum activity, covering gram-negative and gram-positive organisms and anaerobes, although antibiotic resistance is certainly rising. Ceftriaxone is given because it penetrates tissues, lasts 24 hours, and gives the patient prolonged, broad-spectrum coverage until the patient begins outpatient clindamycin. To improve symptoms and decrease the inflammatory response, dexamethasone is given in concert with ceftriaxone and clindamycin. In randomized, prospective trials, dexamethasone has been shown to significantly lower pain and improve trismus, dysphagia, body temperature, and hours of hospitalization.12-14
There are very few studies in the literature to support the contention that our specific medical algorithm not only results in the same safety and efficacy results as ST but also results in significantly better measures of morbidity. 22 The study by Lamkin and Portt, 15 which first described MT, was a case series without an adequate justification of cephalexin as an antibiotic choice, no description of their method of data collection, and no routine follow-up of patients. In 2014, Chau et al 13 published a randomized, prospective, double-blinded placebo-controlled trial with 41 patients examining the efficacy of NA + 48 hours of IV clindamycin ± 10 mg IV dexamethasone, followed by outpatient clindamycin for 12 days. At 24 hours, the study found that the 21 patients receiving dexamethasone had significantly less pain than the 20 patients who received placebo. There was also a trend at 24 hours for patients receiving dexamethasone to return to normal activities and dietary intake. However, all these effects disappeared by 48 hours, and there was no examination of whether or not NA was necessary.
Trismus Subgroup Analysis
The authors acknowledge that the question of medical vs surgical treatment of PTAs cannot be adequately addressed with this case series; rather, a prospective, randomized trial is needed. Case series with chart review can have limitations related to selection bias, coding errors, and omissions. It could be suggested that patients with less severe disease were selected to receive the MT pathway and, as a function of their severity, had lower pain scores, used less pain medication, had shorter time before tolerating oral intake, had fewer days off of work, and had fewer treatment failures. If this were true, disease severity and not the selected treatment would explain the differences noted. The ED physicians in this study almost uniformly made the diagnosis of PTA based on history and physical examination rather than ordering an ultrasound or computed tomography (CT) scan, and this may confound the results since there may have been more abscess patients vs cellulitis patients in the ST group.
However, selection bias in this study design is offset by the fact that particular centers within SCPMG did not adopt the MT algorithm but performed ST as part of their standard practice. In addition, when we controlled for individual medical centers that preferred ST, there was no apparent predilection for patients with trismus to have a procedure. In other words, the data indicate that more patients with trismus just happened to go to the surgical centers, and the surgical centers consistently performed ST in preference to MT regardless of symptomatology.
One possible explanation why more patients with PTA were documented to have trismus at the surgery centers is that head and neck surgeons were primarily doing the charting for the procedures at these locations and as a group are generally more apt to document trismus than ED physicians, who were primarily charting at the medical centers. The literature confirms that differences in charting occur across specialties, 23 and statistical analysis reveals that the proportion of head and neck surgeons who treated ST patients was significantly greater than in the MT group (P < .0001).
To further address the potential of selection bias, we compared outcomes of the subgroup of patients with trismus in both the MT and ST groups. The data indicate that the complication and failure rates are the same in both groups, but the patients with trismus treated with MT required less overall opioid usage.
Conclusions
When comparing a random sampling of 211 patients with PTA treated with MT at 12 service centers to 96 treated with ST at 7 surgical service centers between 2008 and 2013, no difference could be found in complication or failure rates, nor could any difference be identified in the time until tolerating liquids or solids. MT demonstrated statistical superiority in the amount of liquid opioid prescribed, the average number of sore days, and days off from work. Patients with trismus required less opioids when treated with MT. These findings are tempered by the limitations of this case series and could simply be due to the fact that patients with more severe disease received surgical therapy and therefore had worse outcomes. However, our data suggest numerous potential advantages to MT over ST for initial treatment of uncomplicated PTAs, especially if they present with less severe disease in a setting in which they can be seen by an otolaryngologist the next morning. Surgical intervention is not necessarily required to achieve resolution of pain, resume oral intake, and return to work. Procedural risks, patient discomfort, and added costs can be avoided. In fact, using the MT protocol between 2015 and 2016, 89% of 1979 patients with PTA presenting to SCPMG emergency departments were treated with MT. Future study with a randomized, prospective trial should be conducted in which objective criteria for PTA diagnosis are employed with an ultrasound or CT scan, abscess size and microbiology data are recorded, and in which only one surgical technique is employed in the ST group.
Author Contributions
Disclosures
Footnotes
Acknowledgements
The authors thank Linda Mackinnon, MPH, for her efforts in performing the chart reviews and data acquisition.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.