
Abstract
Objectives
To characterize the incidence of lingual tonsil hypertrophy (LTH) in adults with and without obstructive sleep apnea (OSA) and to determine any potential correlation between them.
Study Design
Retrospective chart review.
Setting
Single-center database, September 2016 to April 2017.
Subject and Methods
Lingual tonsil grade (LTG) determined by awake endoscopy was collected as well as other physical examination findings, such as Friedman tongue position, palatine tonsil size, and neck circumference. STOP-BANG scores and polysomnography data were collected to characterize OSA. Incidence of clinically meaningful LTH (defined as LTG 3 and LTG 4) was compared between OSA and non-OSA groups.
Results
Ninety-three patient charts were studied in total. There was no significant difference between patients with and without OSA in the incidence of clinically meaningful LTH (OSA, 13.5%; non-OSA, 14.6%; P = .872). Patients with and without OSA were compared by grade: LTG 1, 13.5% (OSA) vs 35.6% (non-OSA); LTG 2, 73.1% (OSA) vs 48.8% (non-OSA); LTG 3, 13.5% (OSA) vs 14.6% (non-OSA). There were no significant correlations between OSA status and LTG (ρ = 0.190, P = .069).
Conclusion
The incidence of LTH is uncommon, even among those with OSA, and does not seem to differ between patients with and without OSA. Neck circumference appears to be a better clinical indicator than lingual tonsil tissue for the likelihood of a patient having OSA.
Lingual tonsil hypertrophy (LTH) is much more prevalent and well characterized in the pediatric population,1-3 largely because this lymphoid tissue tends to regress with adulthood. While it has been implicated as a more likely potential cause of obstructive sleep apnea (OSA) in children, 4 its role in contributing to OSA in adults is less clear. Most reports of LTH in adults stem from incidental findings during difficult airway cases,5-8 and the actual incidence of LTH in adults remains unclear.
Few studies have characterized the association of LTH in adults with OSA. Hwang et al 9 reviewed cases of patients with varying degrees of LTH and documented basic demographics as well as Reflux Symptom Index, presence of OSA, and smoking habits. The authors found that while LTH did not appear to be associated with OSA or body mass index (BMI), increased LTH was associated with patients who had higher Reflux Symptom Index, smoked, and were younger. Similarly, in a study that investigated the prognostic factors indicating LTH in adults with OSA, 10 laryngopharyngeal reflux and BMI were found to be significantly associated with the presence of LTH in this population. Despite these associations, it is unclear whether there is a higher prevalence of LTH in adult patients with OSA versus those without OSA.
Lingual tonsillectomy is often performed in patients with clinical evidence of LTH,11-14 oftentimes in an attempt to address the issue of OSA. There is, therefore, a substantial basis to study the incidence of LTH as it pertains to the adult population with and without OSA.
LTH is traditionally graded by examination with awake endoscopy, but there have been reports of measuring lingual tonsil tissue with imaging studies.10,15 The primary aim of this study is to characterize the incidence of LTH in adults with and without OSA to determine whether a relationship exists between LTH and OSA.
Methods
A retrospective chart review included consecutive patients at a single center between September 2016 and April 2017, and the study was approved by the Western Institutional Review Board. Patient data were included in the study if there was documentation of an endoscopic evaluation and grading of lingual tonsil size. Patient data were excluded from the study if (1) there was no documentation of an endoscopic evaluation of lingual tonsils in office and (2) there was no indication of screening for OSA by either polysomnography (PSG) or STOP-BANG questionnaires.
Documentation of lingual tonsil grading as measured by examination with awake endoscopy was collected from each patient chart. Lingual tonsil tissue had been graded according to the Friedman LTH grading system based on the following schematic 16 :
Grade 0: Complete absence of lingual tonsils, base of tongue with visible blood vessels
Grade 1: Lymphoid tissue scattered over tongue, does not cover entire surface of tongue base
Grade 2: Lymphoid tissue covering entire tongue base, limited vertical thickness
Grade 3: Lymphoid tissue covering entire tongue base, vertical thickness between 5 and 10 mm (approximately 25%-75% of height of epiglottis)
Grade 4: Lymphoid tissue covering entire tongue base, vertical thickness approximately 1 cm (rises above tip of epiglottis)
With the current grading system, lingual tonsil grades (LTGs) 3 and 4 are an indication for lingual tonsil removal; as such, clinically meaningful LTH had been defined as LTG 3 or 4 on awake endoscopy. 16
All patients are routinely screened in clinic for OSA with STOP-BANG questionnaires, 17 and these scores were collected from patient charts. PSG data were collected for those patients who had undergone further evaluation for OSA. Patients were identified as having OSA if they had PSG data showing Apnea-Hypopnea Index (AHI) >5. Otherwise, patients who did not have PSG data were characterized as having OSA if they scored as high risk on the STOP-BANG questionnaire. Those with PSG data showing AHI <5 or with STOP-BANG questionnaires showing low to intermediate risk were characterized as having no OSA. The STOP-BANG questionnaire was recently compared and validated against traditional diagnostic sleep studies, which demonstrated that higher STOP-BANG scores had a specificity and positive predictive value as high as 98.3% and 98.5%, respectively, in diagnosing OSA when compared with the gold standard, PSG. 18
Demographic data, including age, sex, and BMI, were collected as well as documented physical examination findings, including Friedman tongue position, tonsil size (palatine), and neck circumference. A multinomial logistical regression was performed evaluating the relationship between LTH and OSA while adjusting for the demographic covariants cited.
The incidence of clinically meaningful LTH defined by endoscopic LTG 3 or 4 was calculated and compared between patients with and without OSA, and a chi-square test was used to determine significance. Patients who had AHI data available were further stratified to mild OSA (AHI, 5.0-14.9 events per hour), moderate (15.0-29.9), and severe (>30.0). Fisher’s 2-sided exact test was also used to identify any significant differences in LTG among patients of varying OSA severity. Significance for all tests was set at P < .05 (SPSS Statistics 20 Software; IBM Inc, Chicago, Illinois).
Results
A total of 118 patient charts were reviewed for this study. Twenty-four patients were excluded because they did not have documentation of LTG by in-office endoscopic examination. One additional patient was excluded due to inadequate data to determine OSA status.
Of the remaining 93 patients who were included in the study, 65 were male and 28 were female. The average age was 42.6 years (95% CI, 40.1-45.1), and the average BMI was 29.0 kg/m2 (95% CI, 27.7-30.2). Ninety patients answered STOP-BANG questionnaires; only 3 patients had PSG data without STOP-BANG scores. Forty-one patients had PSG data available.
Fifty-two patients had OSA on the basis of, first, PSG (n = 37) or, second, high-risk likelihood of OSA on the STOP-BANG questionnaire (n = 15). Forty-one patients did not have OSA on the basis of PSG first (n = 4) or low- or intermediate-risk likelihood of OSA on the STOP-BANG questionnaire (n = 37) second. Of the patients with OSA, there were 39 male and 13 female patients, and the average age and BMI were 45.4 years (95% CI, 42.1-48.8) and 30.8 kg/m2 (95% CI, 29.0-32.5). Of the patients without OSA, there were 26 male and 15 female patients, and the average age and BMI were 38.5 years (95% CI, 34.9-42.2) and 26.3 kg/m2 (95% CI, 25.0-27.5). Age was significantly lower (P = .006) and BMI significantly less (P < .001) in patients without OSA.
All patients but 3 had equal LTG between the right and left sides: 2 had LTG 2 and LTG 3, and 1 had LTG 1 and LTG 2. Clinically meaningful LTH was defined by awake endoscopy grade 3 or 4, and the 2 patients who had LTG 2 and LTG 3 between sides were characterized as having clinically meaningful LTH.
Patients with OSA (n = 52) and without OSA (n = 41) were compared by grade: LTG 1, 13.5% (n = 7) with OSA versus 35.6% (n = 15) without; LTG 2, 73.1% (n = 38) with OSA versus 48.8% (n = 20) without; LTG 3, 13.5% (n = 7) with OSA versus 14.6% (n = 6) without ( Table 1 ). There were no significant correlations between OSA status and LTG (ρ = 0.190, P = .069). There was also no significant difference in the incidence of clinically meaningful LTH as defined by awake endoscopy grade 3 or 4 between patients who did and did not have OSA (P = .872).
Distribution of Lingual Tonsil Grades by Awake Endoscopy between Patients with and without OSA.
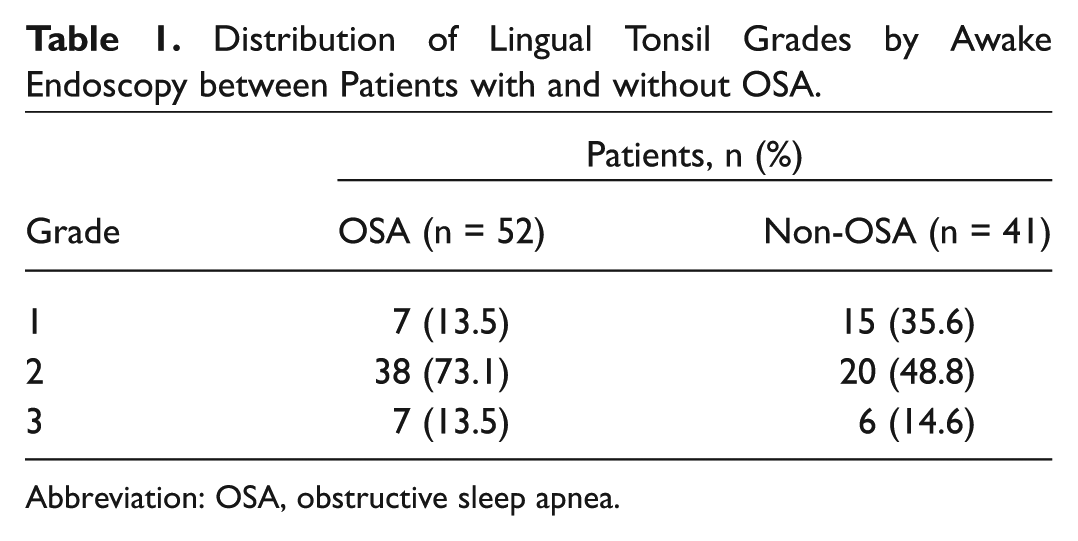
Abbreviation: OSA, obstructive sleep apnea.
Of the 41 patients who had PSG data, 4 did not have OSA; 17 had mild OSA (AHI, 5.0-14.9 events per hour); 8 had moderate OSA (15.0-29.9); and 12 had severe OSA (>30.0). There was no significant correlation in awake endoscopic grading of LTH (ρ = −0.219, P = .169) between those with mild OSA and those with moderate or severe OSA as characterized by PSG.
Multinomial regression controlling for covariants, including age (P = .127), sex (P = .434), Friedman tongue position (P = .657), tonsil size (P = .176), neck circumference (P = .152), and BMI (P = .662), demonstrated that none of these demographic variables significantly affected the relationship between LTH and OSA.
STOP-BANG scores did not correlate significantly with LTG (ρ = 0.133, P = .211).
Discussion
The incidence of LTH is not common in the general adult population, and this study indicates that it is prevalent at potentially equal rates even among those with OSA. The results demonstrate similar incidences of LTH between the adult population with OSA (13.5%) and without OSA (14.6%). The most common method to diagnose LTH is through awake endoscopy showing lingual tonsils with grade 3 or 4. However, lingual tonsil tissue can also be measured by means of imaging studies, such as computed tomography and magnetic resonance imaging.3,15 The results of this study indicate no difference in lingual tonsil tissue between patients with and without OSA when lingual tonsils are measured by awake endoscopy. Even when the incidence of clinically meaningful LTH was compared (LTG 3 or 4), there was still no significant difference between patients with and without OSA.
While some advocate excising lingual tonsil tissue grades 3 and 4, 16 other studies support the removal of any degree of lingual tonsil tissue hypertrophy.11,12 OSA is likely the result of multilevel obstruction, and the presence of hypertrophic lingual tonsil tissue does not necessarily dictate the lingual tonsils as a contributory site to OSA. Even among patients without OSA, lingual tonsil may still be hypertrophied without causing obstruction.
Not surprising, neck circumference was significantly greater in patients with OSA than in those without OSA. Note, however, that the same principle does not hold true with LTG and the likelihood of a patient having OSA.
Furthermore, despite lingual and palatine tonsils both making up the tonsillar lymphoid tissue that may be potential sites of obstruction in OSA, there does not appear to be any correlation between hypertrophy in one region contributing to hypertrophy in another.
A major limitation of this study is that not all patients were properly screened for OSA with PSG. Because the study aimed to investigate the incidence of LTH in OSA and non-OSA populations, patients who did not have clinical or physical examination findings indicating a possibility of OSA were not unnecessarily subjected to participate in an overnight PSG test. Along the same lines, this study is limited by the small sample of patients with AHI values. However, in an attempt to encompass both patient populations in the study, STOP-BANG questionnaires were used as an alternative, albeit less precise, screening method to detect potential OSA. To be conservative in characterizing patients without PSG as having OSA, only those indicating high risk on the STOP-BANG questionnaire (scores 5-8) were included in the OSA group.
Conclusion
The incidence of LTH is relatively low in the general adult population and even among those with OSA. While LTH can be sometimes be a potential site of obstruction causing OSA, there does not appear to be a direct correlation between the presence of LTH in patients with and without OSA. OSA is most likely a disease entity that involves multilevel obstruction, and the lingual tonsils may or may not play a direct role.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.