
Abstract
Objective
To determine the predictors of length of stay (LOS), readmission within 30 days, and unplanned return to the operating room (OR) within 30 days in head and neck free flap patients.
Study Design
Case series with chart review.
Setting
Tertiary academic cancer hospital.
Subjects and Methods
All head and neck free flap patients at The Ohio State University (OSU, 2006-2012) were assessed. Multivariable logistic regression to assess the impact of patient factors, flap and wound factors, and intraoperative factors on the aforementioned quality metric outcomes.
Results
In total, 515 patients were identified, of whom 66% had oral cavity cancers, 33% had recurrent tumors, and 28% underwent primary radiotherapy. Of the patients, 31.5% had a LOS greater than 9 days, predicted by longer operative time, oral cavity and pharyngeal tumor sites, blood transfusion, diabetes mellitus, and any complication. A total of 12.6% of patients were readmitted within 30 days predicted by absent OSU preoperative assessment clinic attendance and any complication, and 14.8% of patients had an unplanned OR return predicted by advanced age.
Conclusions
When assessing quality metrics, adjustment for the complexity involved in managing patients with head and neck cancer with a high comorbidity index, clean contaminated wounds, and a high degree of primary radiotherapy is important. Patients seen in a preoperative assessment clinic had a lower risk of readmission postoperatively, and this should be recommended for all head and neck free flap patients. Quality improvement projects should focus on predictors and prevention of complications as this was the number one predictor of both increased length of stay and readmission.
Keywords
Both public and private insurance payment models have recently been interested in pay for performance to allow for continuous measurement, display, and improvement of important quality metrics. The Donabedian model for assessing quality of care involves measurement of (1) structure measures, such as hospital and surgeon volume; (2) process measures, such as appropriate use of antibiotics; and (3) outcomes, such as readmission and emergency department visits. 1 The focus in the early years of quality improvement has been on outcome measures, which are the most easily tracked and are considered the “bottom line.” Head and neck free flap reconstructive surgery quality metrics have not been thoroughly examined despite having similar mortality and complication rates to other high-risk procedures that have been studied such as coronary artery bypass graft surgery, general surgery and thoracic high-risk procedures, and major cancer surgery.2-4
With the upcoming implementation of bundled payments in many parts of the United States and Canada, as a form of pay for performance, it will be important to control for key patient, surgical, and institution variables that may influence measured outcomes. These outcomes have typically included metrics such as length of stay (LOS), return to the operating room (OR), and unplanned readmission within 30 days of discharge. While predictors of free flap failures have been extensively studied, it is unlikely that these alone will provide a quality metric given the complexity in assessing this outcome reliably. 5 Therefore, we sought to assess outcomes that have historically been the focus of quality improvement metrics and bundle payment strategies in the head and neck oncology population receiving free flap reconstruction.
The objective of this study was to determine predictors of LOS, readmission within 30 days, and unplanned return to the OR within 30 days, important outcomes that are considered quality metrics and can be used for future quality improvement projects in head and neck oncology. Identifying predictors of these outcomes will allow for appropriate risk adjustment in pay for performance models and could potentially be the impetus for quality improvement initiatives.
Methods
Study Population
This was a retrospective review from 2006 to 2012 assessing the outcomes for all reconstruction procedures (including patients who required secondary reconstruction for osteoradionecrosis, fistula, etc) performed by 4 head and neck oncologic reconstructive surgeons (T.N.T., A.A., E.O., and M.O.). Electronic health records (EHRs) were used to abstract most relevant data points, which were well documented given that the EHR was the primary system for charting at our institution during the study years in question, while the remaining data were collected via review of archived paper records. This allowed us to assess all admission records, operative reports, orders, and clinic progress notes. Chart abstraction was performed by 2 independent reviewers (B.T., J.S.) independent of the attending surgeon, and surgeons were blinded to their individual outcomes. The study protocol was approved by the Institutional Review Board and Office of Responsible Research Practices at The James Cancer Hospital and Solove Research Institute of The Ohio State University Comprehensive Cancer Center.
Postoperative Course
Prior to February 17, 2009, all patients were admitted to the intensive care unit (ICU) after surgery. After this date, most head and neck free flap patients were transferred directly to the “specialty-specific floor” after surgery unless they received a craniotomy or thoracotomy. The specialty-specific floor has a nurse to free flap patient ratio of 1:2, and we have previously described the safety and cost savings related to this transition of structure of care. 6 At our institution, the usual postoperative flap protocol includes flap checks every hour for the first 24 hours followed by every 2 hours for the next 24 hours and then every 4 hours for the remainder of the inpatient stay. Tracheostomy tube change and downsize occurs on postoperative day 5, followed by capping and decannulation when appropriate. In patients with mucosal reconstruction, on postoperative day 6, a speech-language pathology assessment is performed for potential oral intake if appropriate on postoperative day 7. This is often delayed to 10 to 14 days in patients who have previously received radiotherapy with or without chemotherapy, and in some cases, patients are sent home with a nasogastric tube or gastrostomy tube for a delayed oral trial in clinic at 2 to 3 weeks.
Covariates
Patient covariates included age, sex, Ohio State University (OSU) preoperative assessment clinic (OPAC) consult, thorough medical history assessment including Charlson comorbidity index (CCI) and specific assessment of diabetes mellitus (DM), coronary artery disease, peripheral vascular disease, chronic obstructive pulmonary disease, chronic kidney disease, hepatic disease, obesity, hypothyroidism, and malnutrition. Also captured was smoking and alcoholism history.
Flap and wound factors included type of flap, defect type, whether the wound bed had been exposed to preoperative radiotherapy with or without chemotherapy, recurrent tumor status, and tumor pathologic and operative features. Intraoperative factors assessed included flap ischemia time, total OR time, estimated blood loss, and amount of crystalloid, colloid, packed red blood cells, and fresh-frozen plasma used. Also measured was whether the patient had any complication (medical or surgical) prior to discharge such as wound infection (cellulitis or abscess) or healing concerns (dehiscence or fistula), flap loss, and any medical complications such as myocardial infarction, pulmonary embolus, stroke, and Clostridium difficile colitis.
Outcomes
Our outcomes included an LOS of greater than 9 days. We chose to dichotomize this outcome because in our flap protocol, most patients should be discharged in 9 days or less even if they had a minor complication. Furthermore, because we are studying quality metrics, we felt that this would be a good target LOS for most of our free flap patients. For this variable, the analysis was also performed with LOS as a continuous variable to confirm no changes to the results or conclusions from the dichotomization of this outcome. Our secondary outcomes included (1) readmission within 30 days to any institution and (2) unplanned return to the OR within 30 days.
Statistical Analysis
Covariates were compared for each outcome using a univariable logistic regression model (given the binary outcomes) and were considered for the multivariable analysis using a backward selection algorithm if univariable P value was less than or equal to .10. Collinearity of variables was assessed prior to simultaneously entering them into our multivariable analysis to prevent the formation of an unstable regression model. All regression model results are reported as a variable estimate with associated standard error and P value. Statistical significance was defined by a 2-sided P value of .05. All analyses were performed using SAS version 9.2 (SAS Institute, Cary, North Carolina).
Results
Study Subjects
The characteristics of the 515 patients are presented in Table 1 . Our cohort had a mean (standard deviation [SD]) average age of 60.1 (12.8) years, and 66% were male. A significant proportion (28%) had primary radiotherapy with or without chemotherapy, 33% of tumors were recurrent, and the cohort had a high mean (SD) age-adjusted CCI at 5.0 (2.3). Seventy-eight percent of patients were current or previous smokers, and 38% were diagnosed with alcoholism at the time of surgery. Most tumors were mucosal squamous cell carcinomas (75%), and most defects were of the oral cavity, including maxillary defects (66%). Because a subset of patients had surgery during a time period where patients were routinely admitted to the ICU postoperatively, 28% of patients required a postoperative ICU stay. However, after the change in protocol to admit patients direct to a specialty-specific floor, less than 10% of patients required an ICU stay.
Patient Demographics and Clinical Characteristics (n = 515). a
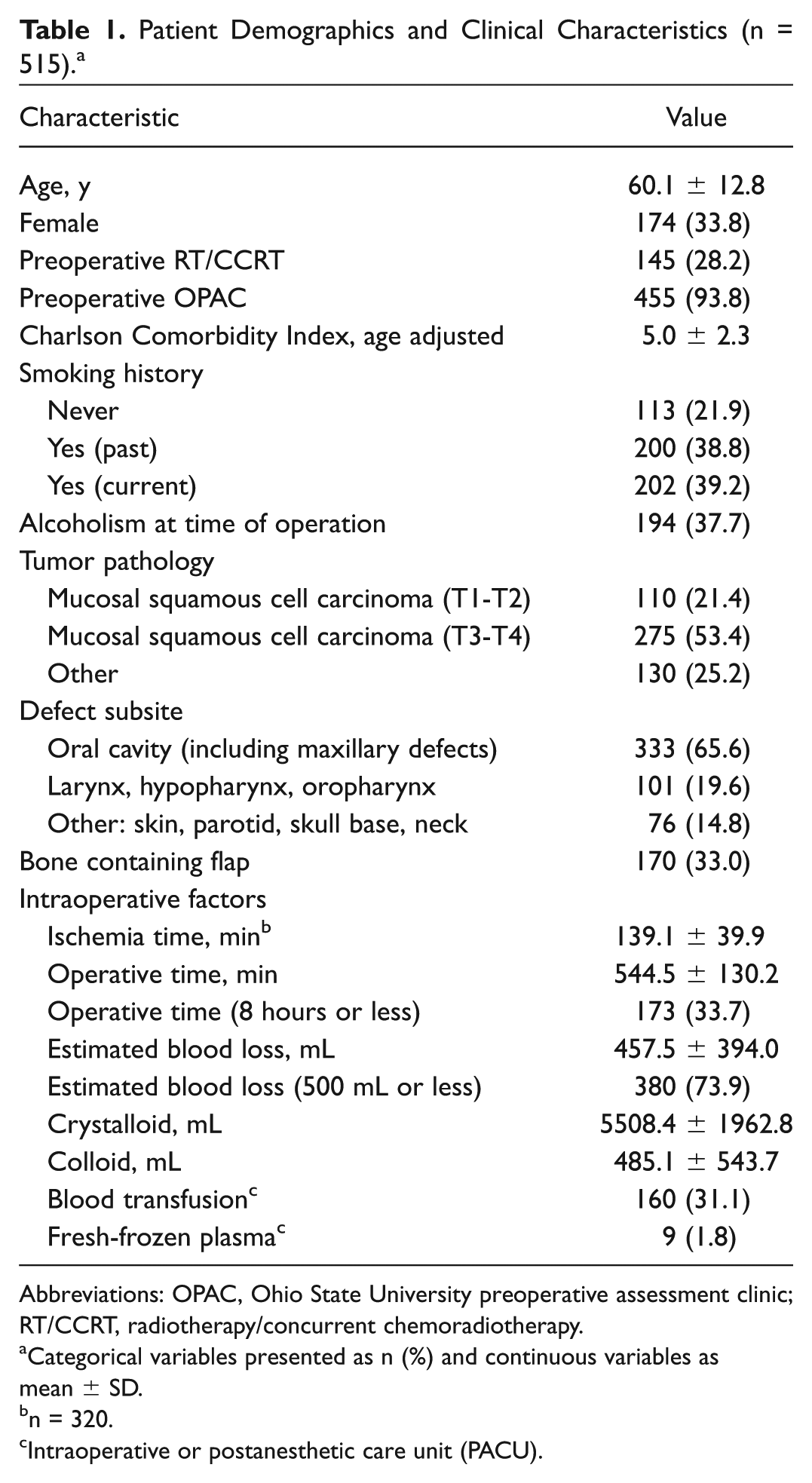
Abbreviations: OPAC, Ohio State University preoperative assessment clinic; RT/CCRT, radiotherapy/concurrent chemoradiotherapy.
Categorical variables presented as n (%) and continuous variables as mean ± SD.
n = 320.
Intraoperative or postanesthetic care unit (PACU).
Outcome summary
The primary and secondary quality metric outcomes are presented in Table 2 : LOS greater than 9 days (31.5%), unplanned readmission within 30 days (12.6%), and return to the OR within 30 days (14.8%). Although complication rate and flap loss are not our quality metric outcomes, these are reported due to their importance in assessing our overall cohort. Our cohort had a high (40.6%) overall complication rate, which included all surgical and medical complications. Our free flap failure rate was 3.5%, and inpatient mortality rate was 1.6%.
Perioperative and Postoperative Complication (Outcome) Summary. a
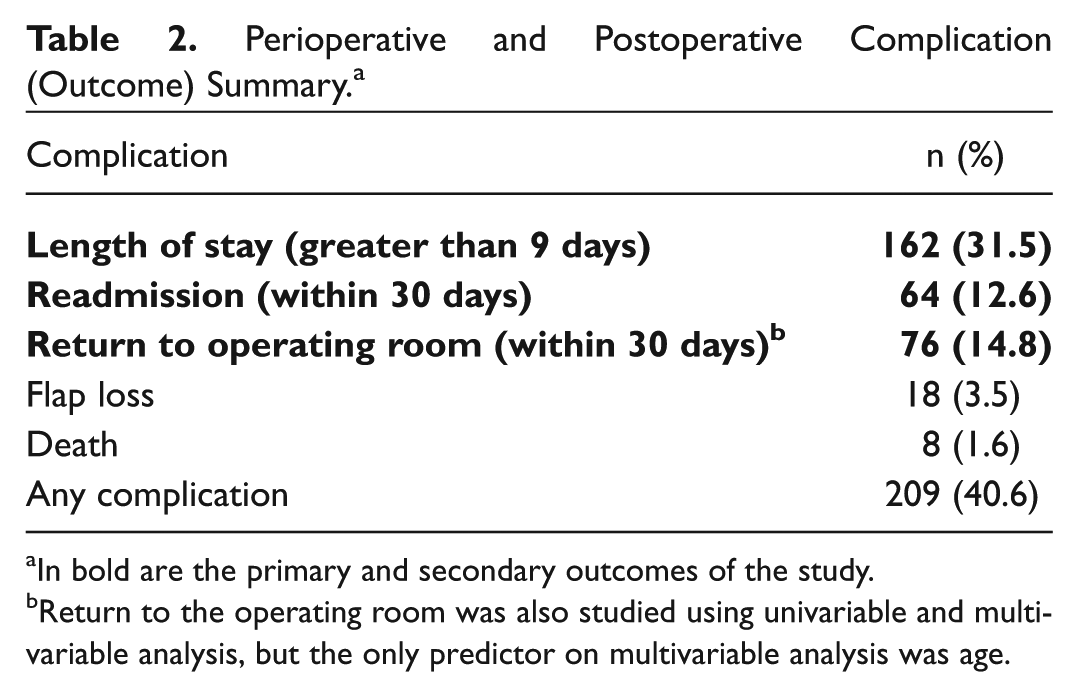
In bold are the primary and secondary outcomes of the study.
Return to the operating room was also studied using univariable and multivariable analysis, but the only predictor on multivariable analysis was age.
LOS
The univariable and multivariable logistic regression predictors of LOS greater than 9 days are presented in Table 3 . Multivariable analysis demonstrated that length of OR time (P < .01), tumor site (oral cavity and larynx/hypopharynx; P < .01), packed red blood cell transfusion (P < .01), history of diabetes (P < .01), and the development of any complication (P < .01) were all significant predictors of LOS greater than 9 days.
Univariable and Multivariable Predictors of LOS >9 Days (31%). a
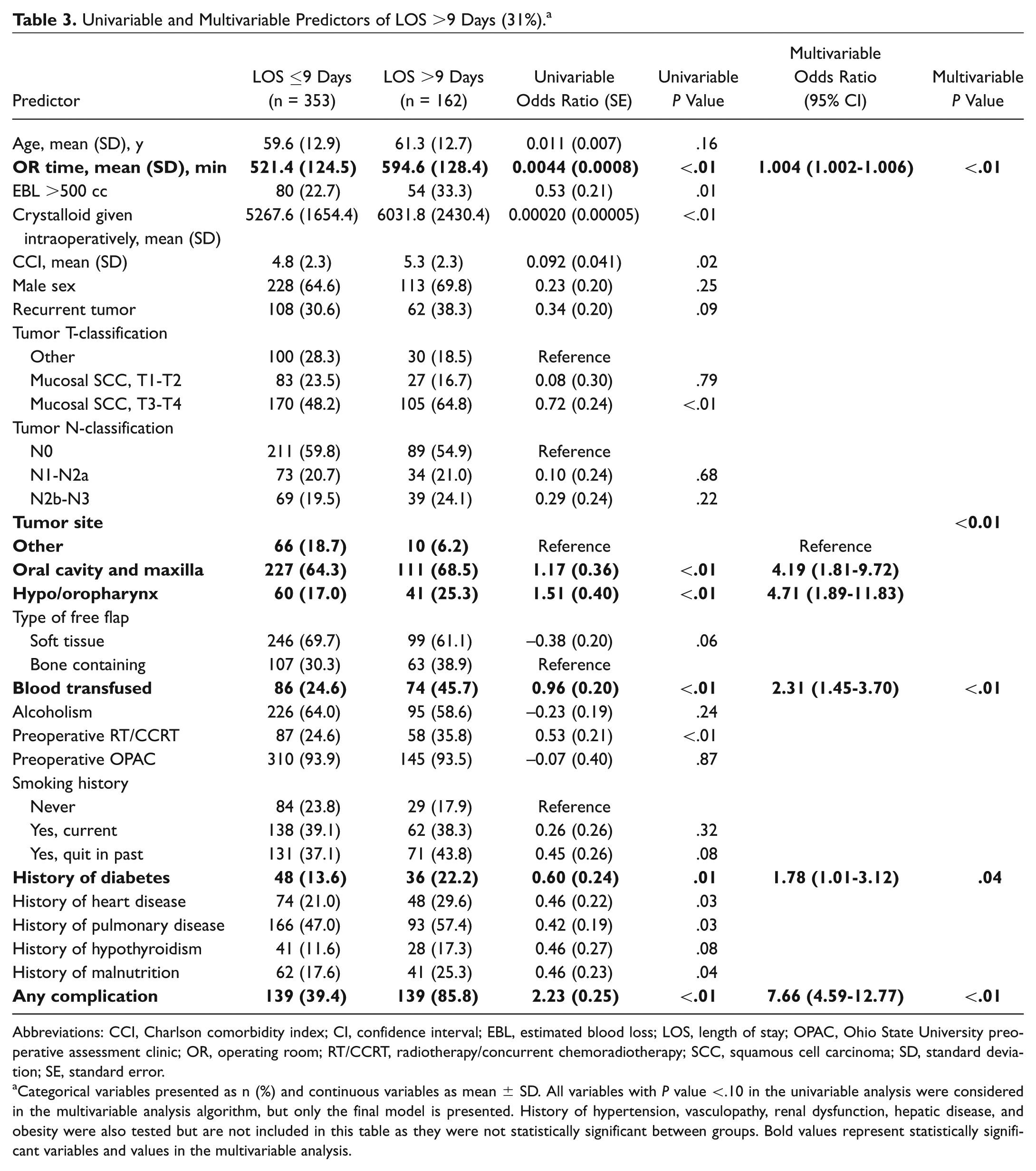
Abbreviations: CCI, Charlson comorbidity index; CI, confidence interval; EBL, estimated blood loss; LOS, length of stay; OPAC, Ohio State University preoperative assessment clinic; OR, operating room; RT/CCRT, radiotherapy/concurrent chemoradiotherapy; SCC, squamous cell carcinoma; SD, standard deviation; SE, standard error.
Categorical variables presented as n (%) and continuous variables as mean ± SD. All variables with P value <.10 in the univariable analysis were considered in the multivariable analysis algorithm, but only the final model is presented. History of hypertension, vasculopathy, renal dysfunction, hepatic disease, and obesity were also tested but are not included in this table as they were not statistically significant between groups. Bold values represent statistically significant variables and values in the multivariable analysis.
We performed a conversion of OR time from minutes to hours to allow for easier interpretation of the results. For each hour increase in OR time, odds of LOS being greater than 9 days increased multiplicatively by 1.25 (95% confidence interval [CI], 1.12-1.40). Those with sites classified as oral cavity (including maxilla) and larynx/hypopharynx/oropharynx had greater odds of LOS being greater than 9 days compared to those with nonmucosal subsites with an odds ratio of 4.19 (95% CI, 1.81-9.72) and 4.71 (95% CI, 1.89-11.83), respectively. Those with blood transfused had greater odds of LOS being greater than 9 days (OR, 2.31; 95% CI, 1.45-3.70). Those with a history of diabetes had a greater odds of LOS being greater than 9 days (OR, 1.78; 95% CI, 1.01-3.12). The predictor that resulted in the greatest odds of LOS being greater than 9 days was the development of any major or minor complication (OR, 7.66; 95% CI, 4.59-12.77). The analysis was repeated using LOS as a continuous variable and gave similar results, not changing our conclusions in this section.
Readmission
The univariable and multivariable logistic regression predictors of readmission within 30 days are presented in Table 4 . Multivariable analysis demonstrated that not having an OSU preoperative assessment clinic (OPAC) consult (P < .01) and the development of any complication (P < .01) were predictors of readmission.
Univariable and Multivariable Predictors of Readmission within 30 Days (13%).
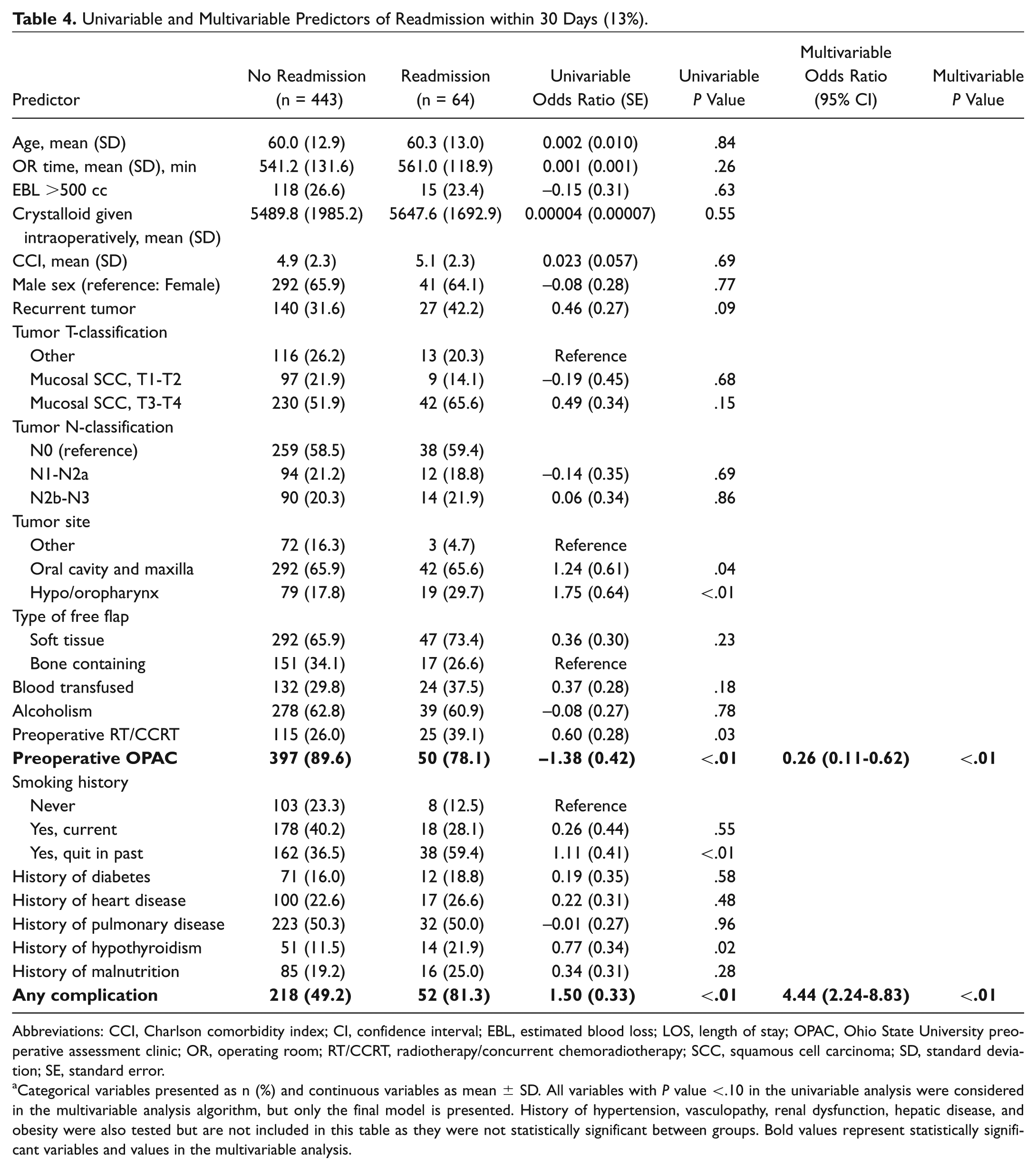
Abbreviations: CCI, Charlson comorbidity index; CI, confidence interval; EBL, estimated blood loss; LOS, length of stay; OPAC, Ohio State University preoperative assessment clinic; OR, operating room; RT/CCRT, radiotherapy/concurrent chemoradiotherapy; SCC, squamous cell carcinoma; SD, standard deviation; SE, standard error.
Categorical variables presented as n (%) and continuous variables as mean ± SD. All variables with P value <.10 in the univariable analysis were considered in the multivariable analysis algorithm, but only the final model is presented. History of hypertension, vasculopathy, renal dysfunction, hepatic disease, and obesity were also tested but are not included in this table as they were not statistically significant between groups. Bold values represent statistically significant variables and values in the multivariable analysis.
Those without OPAC and with any complication were at greater odds of being readmitted with an odds ratio of 3.79 (95%, CI 1.62-8.85) and 4.44 (95% CI, 2.23-8.83), respectively.
Return to the OR
Univariable analysis demonstrated 2 predictors of return to the OR within 30 days: advanced age and larynx/hypopharynx tumor subsites. On multivariable analysis, only age was a statistically significant predictor of unplanned return to the OR.
Discussion
Our series demonstrates a high rate of LOS greater than 9 days (31.5%), readmission (12.6%), and return to the OR within 30 days (14.8%). LOS was predicted by OR time, blood transfusion, mucosal tumor site, history of diabetes, and the development of any complication. Readmission was predicted by lack of preoperative assessment consultation and by any major or minor complication. Return to OR within 30 days was only predicted by advanced age. These key predictors are useful in some cases for risk adjustment (ie, age, diabetes, tumor subsite) and for future quality improvement targets (ie, preoperative assessment referral, complications).
Nearly a third (31.5%) of our patients had LOS greater than 9 days, and few studies have assessed this as a quality metric with the goal of assessing predictors. It has been previously demonstrated that structures of care, such as surgeon and hospital volume, are stronger predictors of LOS. 7 However, most of the studies looking at the relationship between structures of care and LOS have not studied patients undergoing complex reconstruction. Patients who receive tracheotomies have been demonstrated to have a longer LOS, and this may explain why the mucosal subsites had a higher LOS.8,9 Furthermore, patients with mucosal subsites and clean contaminated wounds are at a higher risk of developing wound complications compared to patients with clean wounds, and this has been previously demonstrated to be a predictor of increased LOS in this population.9,10 To our knowledge, this is the first comprehensive multivariable analysis to assess preoperative, intraoperative, and postoperative predictors of LOS in head and neck reconstructive surgery. Patients with diabetes should be managed with aggressive blood sugar control both pre- and postoperatively. Prevention of complications and early management of these complications can prevent extended LOS even when the stay will be longer than 9 days. When wound complications do occur, many of our patients require complex and diligent wound care, and from a health economic perspective, it may be worthwhile to develop a mobile advanced wound care team to visit patients at home with the goal of decreasing their LOS. Further study is required to assess whether wound complications are in fact responsible for the majority of these differences in quality metric outcomes and, if so, further assessment of how outcomes for this patient population should be addressed separately.
The readmission rate in this study (12.6%) is within the reported rate in the literature (5.1%-26.5%) in the head and neck oncology population.11-16 However, only 2 of these studies focused on patients with head and neck microvascular reconstruction in the National Surgical Quality Improvement Program (NSQIP) database demonstrating a 9% to 10% readmission rate, comparable to our results.13,16 Our predictors of readmission included a lack of preoperative OPAC consultation and any complication. Other studies have shown age, 11 DM,11,14 comorbidity index, 13 stage of disease,11,13,16 blood transfusion,13,14 cancer subsite (particularly larynx/hypopharynx),13,16 and preoperative radiotherapy as important predictors. 12 Graboyes et al 12 also identified emergency department (ED) visit within 30 days and chyle leak during index admission to be important predictors of readmission. This is not surprising given that ED visit and readmission are strongly collinear. These studies demonstrate several important variables that need to be considered for risk adjustment in pay-for-performance models such as DM, comorbidity index, stage of disease, cancer subsite, and preoperative radiotherapy. Our study demonstrates that OPAC assessment may be beneficial, and the reasons for this should be explored in future studies. It is possible that patients who did not receive OPAC assessment underwent an operation on an urgent or emergent basis and that these patients may present higher levels of risk, although this is rare at our institution. Alternatively, OPAC assessment may have optimized our patients medically, thus preventing medical complications in a population that would otherwise not seek medical attention and that is associated with a high comorbidity burden, often undiagnosed. During our study years, a single hospitalist saw the majority of our patients in the preoperative clinic and also assessed their medical comorbidities during their inpatient stay. The better results associated with our preoperative assessment may be due to this dedicated hospitalist model, but this requires further study. Above all, wound complications appear to be the biggest predictor of readmission, which has been previously and consistently demonstrated in the medical literature. 16 Beyond trying to prevent wound complications, many of these can be managed on an outpatient basis. A mobile nurse-led head and neck wound care team may be a beneficial adjunct in high-volume practices. This has yet to be developed and implemented and would ultimately need a formal assessment with regard to effectiveness, patient satisfaction, and cost-effectiveness.
Although some studies have studied unplanned reoperations in head and neck oncology, 17 only 1 study in the literature assessed this outcome in microvascular reconstruction specifically, and this study did not focus on head and neck cancer or reconstructive patients. 18 This study demonstrated a 12.9% reoperation rate. Reoperation was strongly associated with complications and was also predicted by American Society of Anesthesiologists Score and prolonged OR time. The main indications for reoperation in this study were debridements (38%), microvascular procedures (29%), and flap revisions (27%). Another study using NSQIP studied patients with head and neck cancer undergoing free flap reconstruction and reported a 17.9% 30-day reoperation rate. 19 Predictors of reoperation included wound (ie, infections and dehiscences) and medical complications (ie, pneumonia, myocardial infarction, and sepsis). Visceral flaps and hypoalbuminemia were also predictors of return to the OR. These data, taken together with our results, demonstrate the importance of early identification and prevention of complications in improving this quality metric. Increased patient education with access to a nurse navigator who can arrange urgent clinic visits while bypassing the ED could prevent readmission and reoperation but requires additional resources. Early follow-up phone calls and telemedicine after discharge could also potentially catch wound complications early and prevent them from requiring surgical intervention with aggressive antibiotic treatment and wound care.
The results of this study must be interpreted in the context of its design. This study has a relatively smaller sample size than what could be achieved with a similar study design using NSQIP. Unfortunately, NSQIP data are not as granular as our data set and have an inherent bias in that only certain institutions contribute data to this database. Also, NSQIP data have not been able to reliably predict complications, which is a key determinant of our quality metrics.20-22 Furthermore, the NSQIP risk calculator underestimated return to OR by 24%. 22 Our study does not assess many other dimensions of quality but uses clinical epidemiological methods to identify predictors of adverse quality metrics. Many of these predictors are not modifiable and are therefore not amenable to quality improvement initiatives. Nonetheless, identifying these factors is critical in implementing pay-for-performance models that allow for appropriate risk adjustment. Furthermore, having baseline metric data is useful moving forward as quality improvement interventions are designed to try to improve these rates.
A specialty-specific (head and neck reconstructive) NSQIP is being developed and thus far has been demonstrated to have excellent internal validity. 23 However, such an integrated system is very costly on an annual basis, limiting its ability for widespread use in the arena of head and neck oncology. 24 Our study adds to the literature by identifying key factors that both on face validity and on multivariable analysis should be included as part of the risk adjustment strategy in any quality metric assessment. We need to shift away from studying free flap failure, 25 a rare complication that has been extensively studied, and move toward quality metrics that are easier to measure, are important to patients and health administrators, occur frequently, and can be targeted with quality improvement interventions. There has been a call for measurement of complication rates and unplanned reoperations as quality metrics in head and neck cancer surgery. 26 The ultimate goal as we develop quality metrics, publicly report them, and pay for higher performance is to improve outcomes and benefit our patients. Physicians, particularly surgeons, are competitive and, once offered data as well as the quality improvement tools, will continuously try to improve their outcomes, as has been demonstrated in other jurisdictions. 24
In conclusion, we have identified several actionable items to study using quality improvement methodology to improve outcomes in this population. Many nonactionable predictors of complications in our study should be corroborated in other databases and used to risk-adjust reported quality metrics.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the 2017 AAO-HNSF Annual Meeting and OTO Experience; September 10-13, 2017; Chicago, Illinois.