
Abstract
Upper aerodigestive tract symptoms are common in patients with obstructive sleep apnea (OSA). It remains unclear whether continuous positive airway pressure (CPAP) improves or worsens these otolaryngology symptoms. As therapy-related side effects limit CPAP adherence, this study aimed to determine if CPAP negatively affects voice, sinonasal, and reflux symptoms of the upper airway. Case series with planned data collection was performed at an academic otolaryngology sleep center. Newly diagnosed patients with OSA were evaluated before and 6 months after initiating CPAP therapy. Data collected included CPAP data download, Reflux Symptom Index (RSI), Epworth Sleepiness Scale (ESS), Voice Handicap Index 10 (VHI-10), Sino-Nasal Questionnaire (SNQ), and oral dryness visual analog scale (VAS). For the 11 CPAP-adherent participants, the RSI significantly improved with CPAP (mean RSI, 22.0-9.5; P = .002); however, the VAS, VHI-10, and SNQ did not change after 6 months of CPAP therapy. In a small sample size, patient-reported voice outcomes (VHI-10) and other upper aerodigestive tract symptoms did not worsen with CPAP; rather, CPAP therapy was associated with a reduction in reflux symptoms.
Keywords
Positive airway pressure (PAP) therapy remains the most commonly used first-line obstructive sleep apnea (OSA) therapy, delivering air pressure to maintain upper airway patency and improve control of breathing and oxygen saturations during sleep. Although effective, outcomes are intimately tied to adherence. PAP therapy has been associated with various side effects, including local symptoms of the upper aerodigestive tract that may preclude adequate long-term adherence.
One concern of our laryngology patients has been the potential deleterious effects of continuous positive airway pressure (CPAP) on voice. The current literature lacks data evaluating the impact of CPAP therapy, positive or negative, on voice-related outcome measures. One study of voice in 18 patients with OSA using nonhumidified CPAP reported worse vocal acoustics (fundamental frequency, jitter, shimmer, noise-to-harmonic ratio, voice turbulence, and habitual pitch) within 2 hours of CPAP use. 1 The study did not report reflux symptoms or quality-of-life measures, so it remains unknown if patients were bothered, or handicapped, by the consequences of PAP therapy on vocal acoustics. The severity of a voice problem is often determined by measuring a patient’s perception of how the voice problem affects his or her life.2,3
Patients with untreated OSA also frequently report laryngopharyngeal symptoms that may result from the disease itself, perhaps related to reflux, vibrational effects of snoring, dryness from mouth breathing, systemic inflammation, or other potential mechanisms. Previous studies have shown that patients with OSA are more susceptible to having gastroesophageal reflux disease (GERD) and that CPAP therapy may reduce nocturnal gastroesophageal reflux (GER) in patients with OSA, likely through changes in lower esophageal sphincter (LES) barrier pressure. 4
This study was conducted to determine whether PAP use negatively affected patient-perceived voice, sinonasal, and laryngopharyngeal reflux symptoms. The secondary objective was to determine if PAP settings correlated with reported symptoms.
Methods
This study was a University of Pittsburgh institutional review board–approved (Positive Airway Pressure and Impact on Voice [PRO13050233]) case series with planned data collection at an academic otolaryngology sleep center. Eligible participants consisted of adults with newly diagnosed moderate to severe OSA, or mild OSA with sleep-related symptoms or comorbidities, who were started on PAP therapy with heated humidification. Exclusion criteria included those with a history of laryngopharyngeal surgery, history of voice therapy, recent use of PAP therapy (within 6 months of enrollment) or other OSA treatment, current vocal fold abnormality (eg, paralysis, lesion), and/or current use of supplemental oxygen.
Five questionnaires were given to the research subjects at the initial baseline visit, 6 weeks post-PAP treatment, and at 6 months post-PAP treatment: Reflux Symptom Index (RSI), Voice Handicap Index 10 (VHI-10), Sinonasal Questionnaire (SNQ), an oral dryness visual analog scale (DRY), and Epworth Sleepiness Scale (ESS).5-8 Additional data included age, sex, body mass index (BMI), diagnostic sleep study data, smoking history, presence of laryngopharyngeal reflux (LPR) disease, medications, comorbid diagnoses, and PAP mask type, pressure and humidity settings, and objective adherence data. Data were analyzed using 2-sided t tests to evaluate interdependencies between PAP therapy and questionnaire outcomes.
Results
Of the 13 participants using PAP therapy, 11 (88.3%) met minimum PAP adherence criteria ( Table 1 ). The group consisted of 38% females and 25% with a smoking history. Adequate pressure effectiveness (apnea-hypopnea index [AHI] <5) was achieved on all participants as confirmed by objective CPAP data monitoring. Subjective OSA outcome measures were also improved on CPAP therapy with a reduction in patient-reported daytime sleepiness (mean ESS reduced from 9.3 to 5.2, P = .008).
Participant Demographics (N = 13).
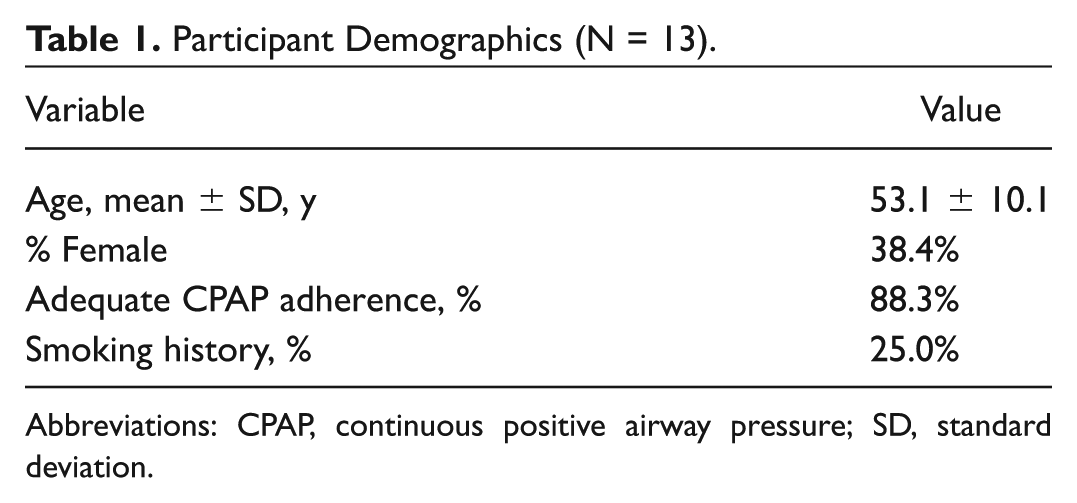
Abbreviations: CPAP, continuous positive airway pressure; SD, standard deviation.
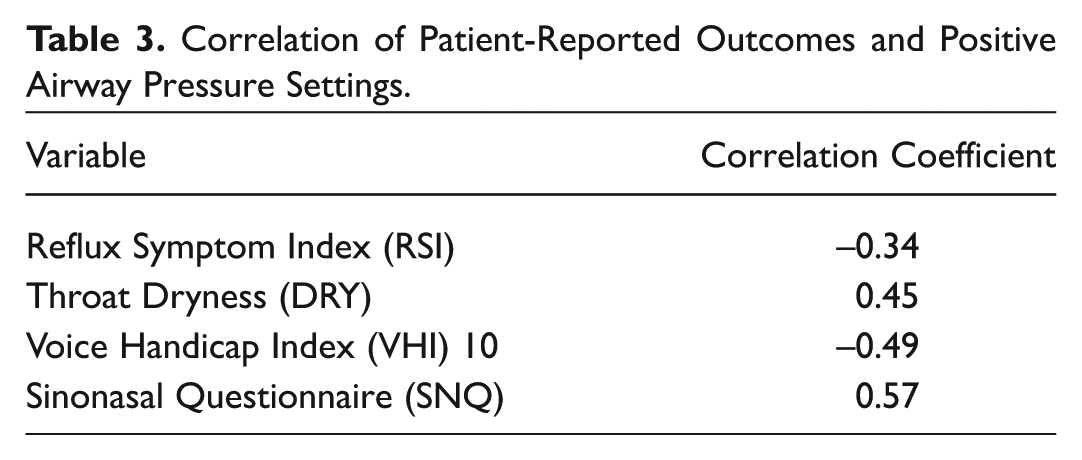
Compared to baseline, mean RSI decreased after 6 months of CPAP therapy (22.0 to 9.5, P = .002), demonstrating a clinically significant reduction in reflux symptoms with OSA treatment. No significant change in oral dryness was observed with CPAP (mean DRY 53.5 at baseline and 33.2 at 6 months, P = .168). Validated questionnaires of voice (VHI-10) and sinonasal (SNQ) symptoms did not significantly change across the study period ( Table 2 ). No significant correlation was found between CPAP settings and patient-reported outcomes ( Table 3 ).
Patient-Reported Outcomes before and after PAP Therapy
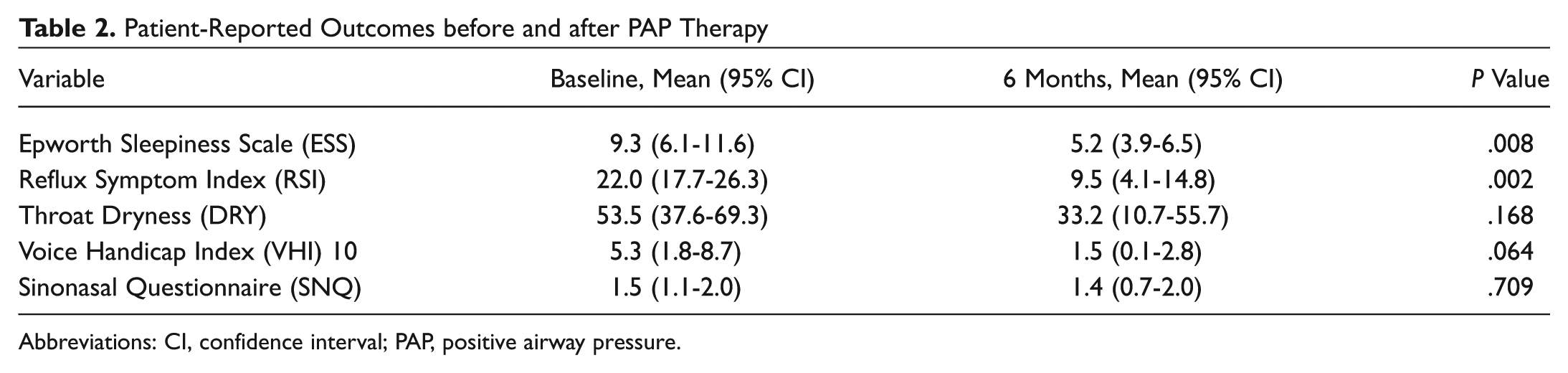
Abbreviations: CI, confidence interval; PAP, positive airway pressure.
Correlation of Patient-Reported Outcomes and Positive Airway Pressure Settings.
Discussion
Although CPAP therapy traditionally has been associated with potential adverse side effects of the upper airway, no significant association was found in our cohort between CPAP initiation and patient-reported voice, sinonasal, or dryness questionnaires. Conversely, patient-reported laryngopharyngeal reflux symptoms substantially improved with CPAP therapy over the 6-month study period. This study supports the growing body of data that OSA may be associated with nocturnal reflux and that OSA treatment may reduce reflux symptoms.
Pepin and colleagues 9 reported that CPAP therapy is associated with congestion, dryness, and rhinorrhea. Another study found that these sinonasal side effects have an underlying inflammatory component, and heated humidification can attenuate these symptoms. 10 Our investigation did not find any correlation between PAP therapy and sinonasal symptoms, including dryness, which may be explained by the use of heated humidification in our group.
Voice changes in the Hamdan et al 1 study were not corroborated in this study’s patient-perceived voice outcomes, which again may be attributable to the use of humidified CPAP in this study. Furthermore, CPAP patients may have a change in acoustic voice measures, but these changes may not be great enough to affect patients’ perception of voice handicap on their daily life. In addition, the improvement in laryngopharyngeal reflux symptoms found in this study could also lead to an improved perception of voice handicap. 11
Follow-up studies with a larger sample size would be useful in supporting the improvement in patient-reported laryngopharyngeal reflux symptoms found in this study, as this study’s major weakness was its small sample size and lack of power to confidently demonstrate a lack of change in voice symptoms. Furthermore, investigations evaluating the effect of mask type and specific CPAP settings on patient perception of voice may provide more insight into causality.
Conclusion
PAP therapy was associated with a reduction in laryngopharyngeal reflux symptoms in CPAP-adherent patients. Patient-reported voice, sinonasal, and throat dryness symptoms did not worsen in the first 6 months of PAP use.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented as a poster at the 2016 AAO-HNSF Annual Meeting and OTO EXPO; September 18-21, 2016; San Diego, California.