
Abstract
Objective
To examine the adverse events and time to diagnosis of in-office laryngeal biopsy (IOB) procedures.
Study Design
Retrospective cohort study.
Setting
Outpatient clinic–tertiary referral medical center.
Subjects and Methods
A total of 390 IOBs were included in this study. Data on demographic characteristics, outcomes, and complications were collected. Complications were classified as severe—necessitating further intervention or admission—or mild and self-limited. Delay in diagnosis, assessed as a complication of IOB, was calculated as the time from initial examination to final diagnosis.
Results
Of 390 IOBs, 4 (1%) had complications: epistaxis (n = 2), vocal fold hematoma (n = 1), and aspiration event (n = 1). There were no reports of complications at follow-up. The sensitivity of IOB versus direct laryngoscopy biopsies was 77.8%, and the specificity was 95.1%. When the IOB showed malignancy as a final diagnosis, time to diagnosis was 10.7 days (95% CI, 8.6-12.8). When IOB pathology results changed from benign or carcinoma in situ to malignant (squamous cell carcinoma) by direct laryngoscopy, time to diagnosis was longer: 49.1 days (95% CI, 38.1-60.1) and 36.1 days (95% CI, 15.1-57.1; P < .05), respectively.
Conclusions
In this cohort, IOBs appear to be free of significant adverse events. IOBs for suspicious laryngeal lesions shorten the time to diagnosis and treatment for the majority of patients; the minority showed a small and insignificant delay.
Keywords
In-office laryngeal procedures have become a major diagnostic and therapeutic option for laryngeal diseases.1-3 Availability and cost-effectiveness of such procedures are much higher than for those in the operating room. 4 However, the setting of the outpatient clinic is less favorable for addressing immediate complications, such as laryngeal edema, laryngospasm, upper airway obstruction, aspiration, and bleeding. Moreover, the transnasal passage of a larger endoscope used in these procedures (work channel or EndoSheath slide-on) increases the risk for epistaxis and discomfort; this may jeopardize procedure success and elevate complication rate.
Safety and tolerance were examined retrospectively in 116 patients who underwent in-office biopsy (IOB) of the larynx (n = 73), oropharynx (n = 35), and hypopharynx (n = 8). 5 This and other teams reported no severe (if any) complications in IOB procedures.5-10
In an assessment of the accuracy of laryngeal IOBs, sensitivity was 69.2%, and specificity was 96.1%. 11 Patients with a biopsy negative for malignancy require further evaluation and need to be schedule for a second biopsy under general anesthesia. A malignant result in the second biopsy changes the patients’ management and prognosis. The need to take 2 biopsies can cause delay in diagnosis and may influence patients’ health.
Reducing the diagnostic evaluation period is one the most important factors in laryngeal cancer evaluation, treatment, and, consequently, prognosis. Postponing laryngeal biopsy is the major obstacle in this equation. Transnasal flexible laryngeal biopsy results in a reduction in diagnostic workup time, thereby increasing diagnostic efficiency. Time to treatment was found to be 24.2 days in successful transnasal fiberoptic laryngoscopy (TFL) biopsies, as opposed to 48.8 days when the biopsy was unsuccesful. 5
In cases of head and neck squamous cell carcinoma (SCC), a 4-week delay in treatment was reported to result in a significant increase in tumor volume and progression. 12 A delay >40 days in the early stages increased the risk of local failure13-15 and neck failure and decreased survival.16,17 Head and neck SCC with a longer waiting time was a significant negative prognostic factor. 18 Yet, the outcome of diagnostic and therapeutic delay on survival is inconclusive, and the duration of delay that is detrimental is not clear. 19
In a daily laryngeal outpatient clinic, IOBs are everyday activities. Our aim was to assess the safety of an in-office laryngeal biopsy procedure at our center and review and summarize the relevant literature.
Patients and Methods
Study Population
Patients’ medical records were reviewed for demographic characteristics, outcomes, and complications. Based on the literature, complications were categorized as severe or mild. Severe complications included laryngospasms that necessitated further intervention or admission to the hospital, airway obstruction, and laryngeal hemorrhage. Mild complications included hematoma, aspiration, and pain.
The Institutional Review Board of the Rambam Health Care Campus approved the study (approval 0021-17 RMB).
In-Office Laryngeal Biopsy Procedures
All the in-office procedures were performed in an outpatient clinic within the hospital area. The personnel comprised 1 or 2 physicians and a nurse. The protocol for these procedures included local anesthesia of the nasal cavity (tetracaine 2% mixed with oxymetazoline hydrochloride 0.05%), the soft palate (spray lidocaine hydrochloride 10%), and the larynx (lidocaine 2% inserted through the working channel of the EndoSheath). 11 Using a flexible endoscope, the surgeon inserted a 2-mm-diameter biopsy forceps through the working channel (laryngeal biopsy forceps; Medtronic) and took the biopsies. In most procedures, >1 specimen was collected and sent in formalin for pathology analysis. Patients remained in the clinic for 30 minutes for observation. A nurse took vital signs.
After repeated endoscopy of the airway ensured no obstruction, swelling, or bleeding, the patients were discharged. The first follow-up visits were scheduled for 2 to 4 weeks after the procedures.
Lesions for IOB were either suspicious or benign appearing. Suspicious lesions included leukoplakia, erythroplakia, ulceration, exophytic mass, and a lesion on an immobile vocal fold. Benign lesions included polyps, nodules, Reinke space edema, and findings compatible with chronic laryngitis due to reflux. Figure 1 shows our routine management for patients with suspicious lesion of the vocal folds.
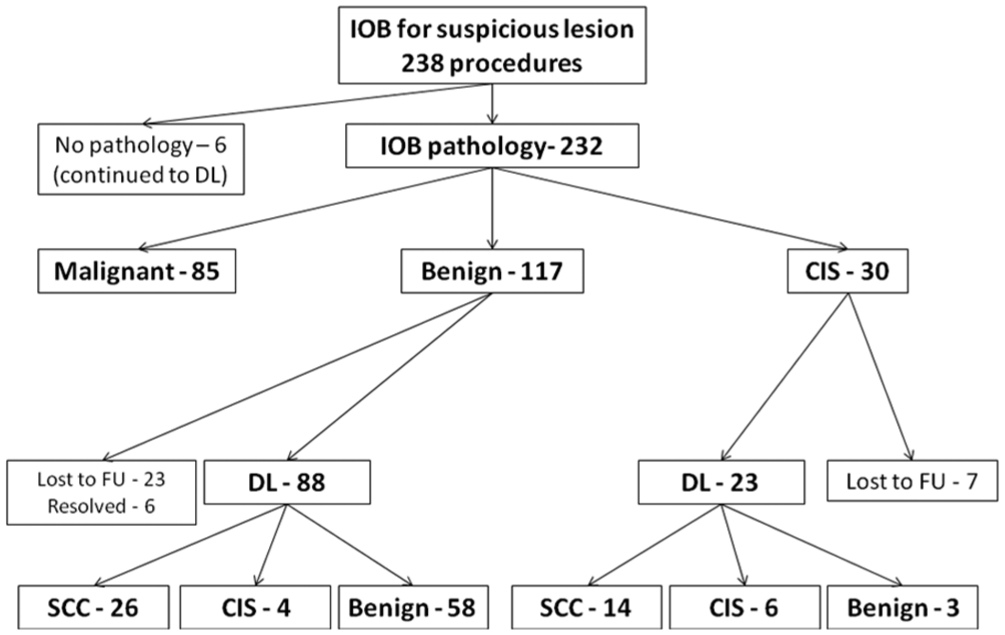
Management of laryngeal suspicious lesions. CIS, carcinoma in situ; DL, direct laryngoscopy; FU, follow-up; IOB, in-office biopsy; SCC, squamous cell carcinoma.
We considered a pathologic result of SCC as a definitive diagnosis, and patients proceeded directly to treatment without undergoing biopsy by direct laryngoscopy (DL). Patients with benign pathology or carcinoma in situ (CIS) on IOB proceeded to DL for definitive diagnosis. Sensitivity and specificity of IOB for suspicious lesions were calculated by categorizing the pathologic results as benign and malignant (malignant results included CIS and SCC). 11 Time to diagnosis was calculated for 142 of 238 patients with suspicious lesions that were treated at the Rambam Health Care Campus between June 2013 and January 2017. These patients underwent the biopsies by the senior and skilled laryngologist (either J.T.C. or L.B.) to avoid experience biased. Only 113 patients completed the full diagnostic workup.
Statistical Analysis
The summary of demographic descriptors was by means (and 95% CI) for continuous variables and by percentages of total procedures for categorical variables. We considered P values <.05 statistically significant.
Results
A total of 355 patients underwent 390 IOBs. The mean age was 63.6 years (95% CI, 62.3-64.9), and the male:female ratio was 4.3:1. Twenty-nine patients had 2 in-office laryngeal biopsies, and 3 patients had 3 biopsies at separate times. Of 390 IOBs ( Figure 1 ), 238 were for a suspicious lesion and 152 for a benign-appearing lesion. For 232 of 238 IOBs (97.5%) for suspicious lesions, pathologic results were available. All patients with benign or CIS results were referred to DL for final diagnosis. A malignant result in IOB was considered diagnostic and final. Eighty-five patients were diagnosed with malignancy; 83 had invasive squamous carcinoma; 1 had T-cell lymphoma; and 1 had chronic lymphocytic leukemia.
All 85 patients proceeded directly to treatment: 53 patients received radiation with or without chemotherapy, and 32 patients were referred for surgery. The 117 (50.4%) patients with benign pathology were referred to DL. Twenty-three patients refused to undergo DL and biopsy, and in 6 patients, the lesion resolved spontaneously. Of the 88 patients with benign results in IOB who underwent DL, pathology was benign in 58 (65.9%), SCC in 26 (29.6%), and CIS in 4 (4.5%). IOB pathology was CIS in 30 patients (13%); they were all referred to DL. Of the 23 patients with CIS in IOB who underwent DL, the pathology was benign in 3 (13%), SCC in 14 (60.9%), and CIS in 6 (26.1%). The sensitivity of IOB as compared with DL biopsies was 77.8%, and the specificity was 95.1% ( Table 1 ).
Sensitivity and Specificity of IOB vs DL Biopsy for Laryngeal Suspicious Lesions. a
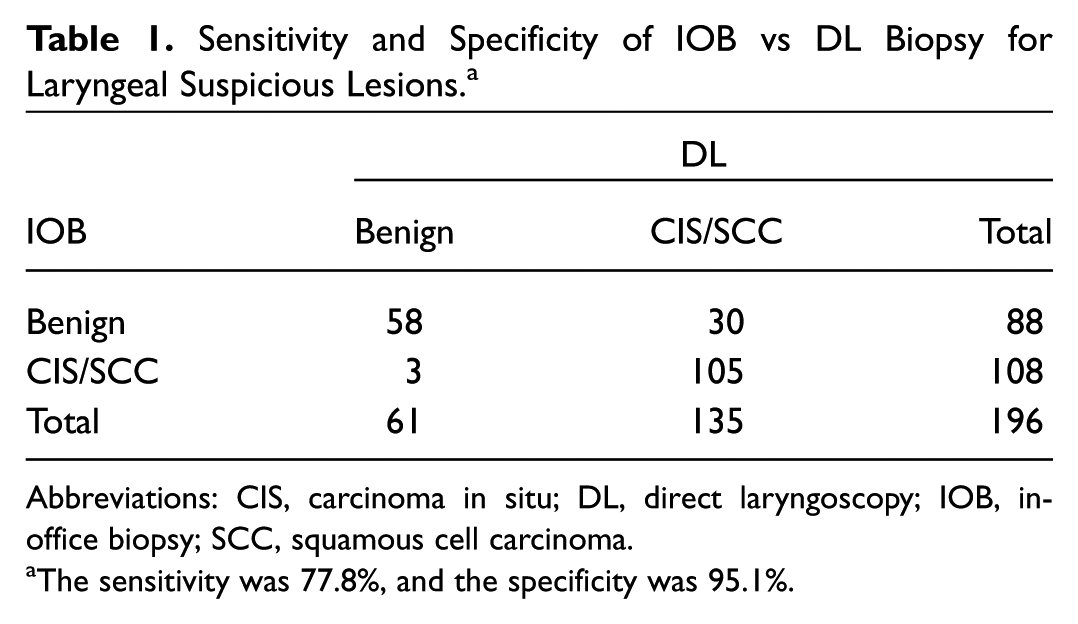
Abbreviations: CIS, carcinoma in situ; DL, direct laryngoscopy; IOB, in-office biopsy; SCC, squamous cell carcinoma.
The sensitivity was 77.8%, and the specificity was 95.1%.
Complications
For the 390 IOB procedures, we report only 4 mild complications (1%). The complications comprised epistaxis (n = 2) that ceased spontaneously, hematoma in the vocal fold that was due to a strong cough before the biopsy (n = 1), and an aspiration event that resolved spontaneously (n = 1). There was no severe complication.
Considering delay in diagnosis as 1 of the complications of the IOB procedure, we calculated time to final diagnosis ( Table 2 ): 113 patients with suspicious lesions who underwent the biopsies and completed the full diagnostic workup were enrolled in the final timing calculation.
Time to Diagnosis.
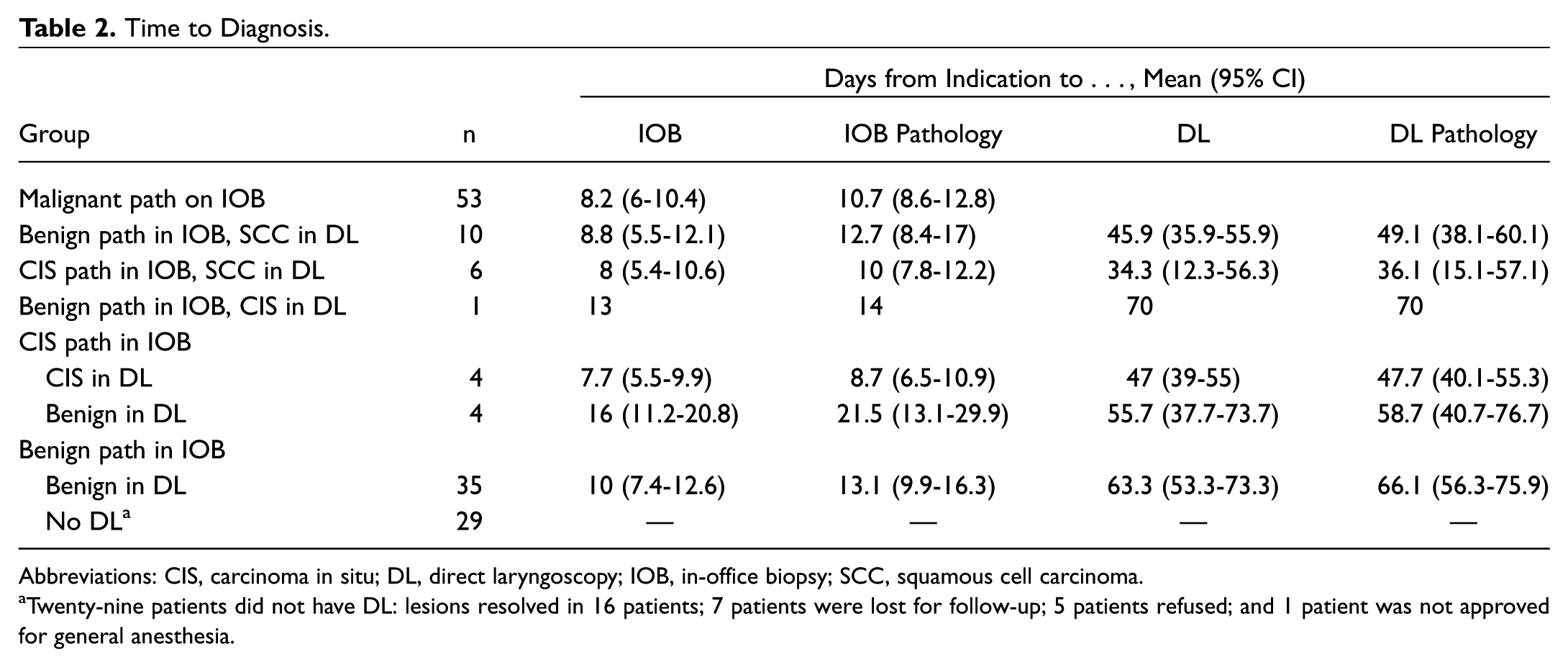
Abbreviations: CIS, carcinoma in situ; DL, direct laryngoscopy; IOB, in-office biopsy; SCC, squamous cell carcinoma.
Twenty-nine patients did not have DL: lesions resolved in 16 patients; 7 patients were lost for follow-up; 5 patients refused; and 1 patient was not approved for general anesthesia.
Twenty-nine patients with benign IOB results did not continue to DL: the lesion resolved in 16 patients; 7 patients were lost for follow-up; 5 patients refused DL; and 1 was not approved for general anesthesia.
When the IOB showed malignant pathology as a final diagnosis, the time to diagnosis was 10.7 days (95% CI, 8.6-12.8; n = 53). For all patients who had DL pathology results at a higher level of malignancy than their IOB pathology results, the time to diagnosis was significantly higher than that of the other patients who underwent IOB (P < .005). This included patients whose pathology results changed from benign by IOB to CIS by DL—70 days (n = 1), patients whose pathology results changed from benign by IOB to SCC by DL—mean 49.1 days (95% CI, 38.1-60.1; n = 10) and patients whose pathology results changed from CIS by IOB to SCC by DL—mean 36.1 days (95% CI, 15.1-57.1; n = 6).
There were no reports of complications at 1-month follow-up.
Discussion
Laryngeal procedures under local anesthesia have progressively been replacing operations under general anesthesia.1-4 Yet local anesthesia procedures bear some risk. The procedures reported by our group were performed as is customary, and their success was in concordance with the results in the literature. 8
We report a very low rate of complications for IOB (4 of 390, 1%), all of which were mild. Likewise, no severe complications for IOB reported in the literature ( Table 3 ). We note that the alternative to IOB is biopsy under general anesthesia. General anesthesia itself, with intubation, carries risks of injuries to the vocal folds. Such injuries include hematoma,20-23 edema,22,23 and granuloma, 23 which also result in impaired voice quality.20,21 We conclude that IOB can be safely performed in routine care in the outpatient clinic.
Complications of In-Office Laryngeal Biopsies: Review of the Literature.
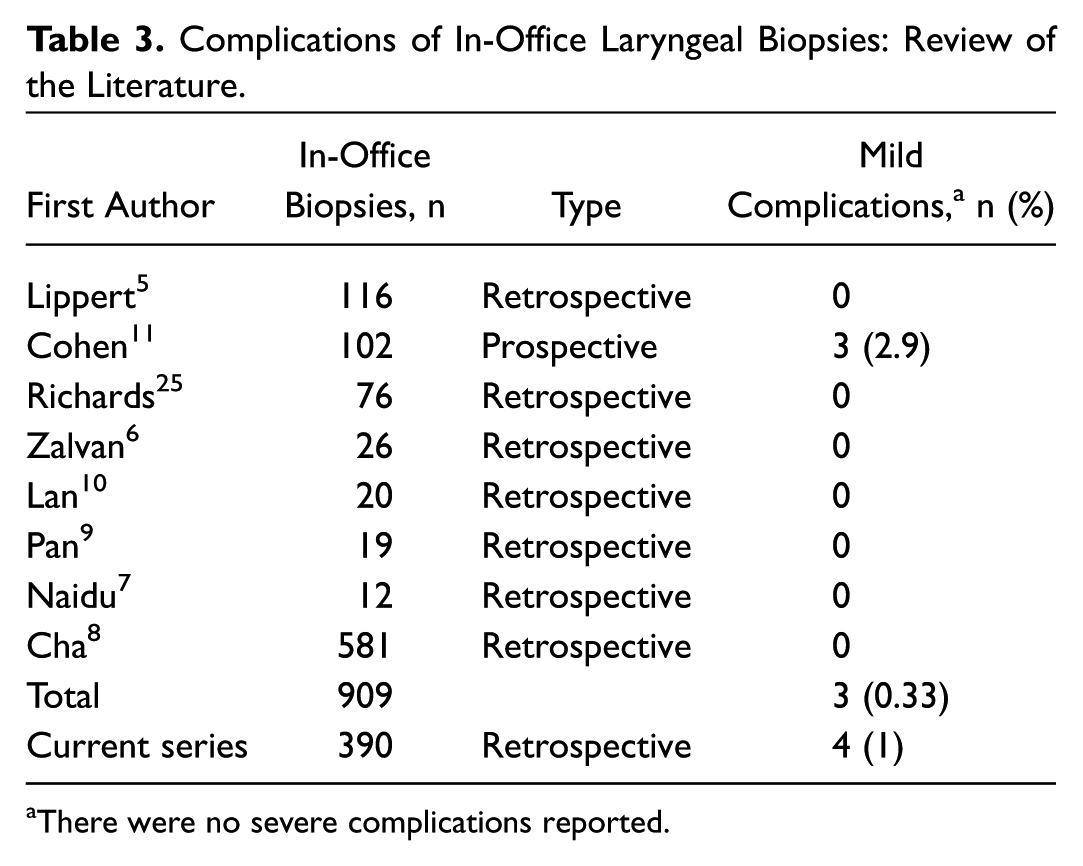
There were no severe complications reported.
The main risks for late complications in IOB are delayed diagnosis and erroneous diagnosis, which impair treatment and may increase mortality risk. Although many laryngologists and otolaryngologists remove suspicious-looking lesions without getting a biopsy first, in our hospital, formal laser cordectomy without a biopsy is not the common practice. As others, we perform excisional biopsy to remove the entire lesion, but getting an IOB first allows us to perform a definitive laser cordectomy in the first operating room procedure.
In our hospital, the availability of in-office laryngeal biopsy is within 1 week, and the availability of DL for suspicious laryngeal lesions is 1 month. Time from the biopsy until pathology report is 2 to 6 days. We found that of our group, patients who underwent IOBs for suspicious lesions received their definitive malignant diagnosis in 10.7 days (95% CI, 8.6-12.8). These patients did not have any delay in diagnosis. In fact, their diagnosis was faster by 3 to 4 weeks than the time to diagnosis by DL biopsy. IOBs for suspicious laryngeal lesions diminished the period to the final diagnosis and treatment in most cases (61 of 113). Some patients, however, had delay in the diagnosis (11 of 113). This delay is partly explained by the fact that many of our patients had substantial comorbidities and the preparation of such patients for general anesthesia is frequently time-consuming. Time to diagnosis was measured in IOBs performed by senior authors only, which may also cause selection bias.
Attaining true pathology results of in-office laryngeal biopsies is extremely important concerning suspicious lesions. The sensitivity of IOB in our cohort was 77.3%.
We agree with previous work 11 stating that IOB has a tendency to underestimate the severity of suspected lesions. Any degree of dysplasia should be considered potentially malignant. Therefore, every patient with benign pathology or any degree of dysplasia in IOB should be referred to DL for definitive pathology.
Specificity of IOB was high, 94.7%, yet overestimated for 3 patients. For 1 of them, SCC was diagnosed on DL 3 months later. For the other 2, the tumor was probably excised with adequate margins in the IOB. Indeed, even in vocal fold SCC resection with proven inadequate margins, re-resection was shown to have benign pathology. 24
In the IOB-CIS group, DL biopsy demonstrated underestimation for most patients. Yet the majority were suitable for microlaryngoscopy with CO2 laser cordectomy and progressed directly to the therapeutic surgery during the DL biopsy.
In conclusion, in-office laryngeal biopsies appear to be free of significant adverse events, with low rates of complications. IOBs for suspicious laryngeal lesions shorten the time to diagnosis and treatment in the majority of patients; the minority showed a small and insignificant delay.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.