
Abstract
Objective
Hyposmia is a sensorial disorder in which patients have a reduced sense of smell. However, there are no effective regimens for the management of this disorder. Therefore, the aim of this study is to evaluate the therapeutic effect of intranasal insulin on olfactory recovery in patients with hyposmia.
Study Design
This is a double-blinded, randomized controlled trial.
Setting
Intervention.
Subjects and Methods
This study was administered on 38 patients with hyposmia according to the inclusion and exclusion criteria. Patients were randomly divided into 2 parallel groups. The intervention and placebo groups underwent endoscopic placement of intranasal insulin gel foam (40 IU) and saline-soaked gel foam into the olfactory cleft, respectively. The procedure was performed twice a week for 4 weeks with butanol threshold testing initially and 4 weeks after treatment.
Results
The Connecticut Chemosensory Clinical Research Center score in the intervention group was significantly higher compared to that of the placebo group after 4 weeks (P = .01). Moreover, no adverse effects were reported in both groups.
Conclusion
Our findings indicated that intranasal insulin (40 IU) administration may trigger the improvement in the olfactory sense and also appears to be free of significant adverse events in this small cohort. However, due to limited research regarding this topic, further studies using a larger population are required.
Hyposmia is a sensorial disorder in which patients have olfactory dysfunction, wherein their sense of smell is impaired. 1 As Murphy and colleagues 2 reported, 7% of the US population has olfactory dysfunction, including elderly adults, with a disease prevalence of over 24%. Olfactory dysfunction may be a result of an influenza-like syndrome infection, and most of the patients have experienced 1 year of nasal inflammation in concomitance with a chronic state of hyposmia. 3 Important issues in complicated hyposmia are nasal polyposis, sinusitis, and coinfection, which in turn might cause underdiagnoses and thus untreated hyposmia. 3 Additional underlying causes of hyposmia are polyps, trauma, and aging. It should also be mentioned that age is associated with hyposmia and may considerably occur in those older than 80 years.2,4 Evidence suggests that hyposmia can affect quality of life and is associated with an increased risk of depression and appetite loss.4-6 On the other hand, other diseases presenting with hyposmia are associated with insulin resistance in the central nervous system. These diseases include diabetes mellitus type 2, Alzheimer’s disease, and obesity. 7 The mechanism of intranasal insulin on the brain is quite clear, as the olfactory bulb is the largest place for the transformation of intranasal insulin in the brain. 8 Recently, similar studies, such as the one conducted by Schöpf et al 9 on human subjects and Zhang et al 10 on mice models, suggested that intranasal insulin administration can be effective in the management of olfactory dysfunctions. There are a few studies, with controversial results, about the effects of insulin on hyposmia. We hypothesize that intranasal insulin administration has a substantial effect on the improvement of hyposmia. Therefore, our study aims to investigate the therapeutic effect of intranasal insulin on olfactory recovery of patients with hyposmia.
Materials and Methods
Ethics
In this prospective, double-blinded, randomized controlled trial, we investigated 38 of 52 hyposmic patients referred to the Amin Hospital (affiliated to Isfahan University of Medical Sciences, Isfahan, Iran) from 2016 to 2017. This study was registered in the Iranian Registry Clinical Trial (No. IRCT2017061712782N15) and was approved by the ethics board of Isfahan University of Medical Sciences (No. 395999). All patients were randomly selected in this study, and written informed consent for participation in the study was obtained from the patients.
Setting
In this study, the Connecticut Chemosensory Clinical Research Center (CCCRC) test was employed to classify patients based on the intensity of their hyposmia. The CCCRC test consists of butanol threshold and odor identification tests. 11 In this study, only the butanol threshold test was performed. All patients were diagnosed based on clinical, physical, paraclinical, and endoscopic evaluations of the nasal cavity. Scoring on the CCCRC test is as follows: normosmic, 6.00 to 7.00; mildly hyposmic, 5.00 to 5.75; moderately hyposmic, 4.00 to 4.75; severely hyposmic, 2.00 to 3.75; and anosmic, 0 to 1.75.
Butanol Threshold Test
There were 2 bottles containing water and a dilated butanol concentration in each stage of the study. The bottles, numbered from 0 to 9, with different concentrations of butanol, were used for the identification of olfactory function. The most concentrated bottle contained 4% butanol (bottle 0). The remaining bottles (bottles 1-9) were dilated with deionized water, and the concentrations lessened in a geometric progression, with a ratio of 1:3. For the test conduction, we instructed the subjects to obstruct their nostril with a finger and then smell the bottles; the aforementioned procedure was repeated for the other nostril. The test was initiated with the lowest concentration of butanol. If the subject accidentally picked the wrong bottle, the next step was to present a higher concentration of butanol along with water. If the patient was able to smell the butanol for 5 times in a row, the score was recorded. The score for the other nostril was recorded in a similar manner. Therefore, the mean scores of the 2 nostrils were considered the CCCRC score. CCCRC scores range from 0 to 9, but in this study, we considered 7 the maximum score. 11
Assessments
We included hyposmic patients aged 18 to 70 years who had a CCCRC score between 2 and 5.75 (mild to severe hyposmia), had a disease duration over 6 months, and provided secured informed consent to participate in the study. Furthermore, patients who had hypoglycemia or diabetes; had been subjected to deep anesthesia; had any medical condition that could affect their sense of smell; had anatomical malformations such as nasal polyposis, septum deviation, acute or chronic rhinosinusitis, choanal atresia, or adenoid hypertrophy; and were normosmic or anosmic were not included in the study. It should be also noted that for our exclusion criteria, we excluded patients who were lost to follow-up, required corticosteroids, dropped out, and presented with severe side effects during the study. After patient enrollments and based on the inclusion and exclusion criteria, the patients were randomly allocated into 2 groups using the OxMAR software: (1) intervention group (n = 19) or patients receiving treatment with insulin (8 males and 11 females, mean age 37.31 ± 13.47 years) and (2) placebo group (n = 19) or under treatment with normal saline (12 males and 7 females, mean age 35.73 ± 15.95 years). Moreover, the patients were also blinded regarding the experimental conditions (insulin and normal saline therapies). Both groups were transferred to the outpatient operation room without anesthetics. The intervention group was treated with 40 units of neutral protamine Hagedorn insulin, which was impregnated on a gel foam and was endoscopically placed in the space between the middle turbinate and nasal septum. The placebo group underwent a similar procedure, in which they were treated with 20 mL normal saline (saline-soaked gel foam) instead of insulin. These procedures were performed by a surgeon blinded to the treatment groups and were done twice a week until week 4 after the first intervention. It is noteworthy to mention that prior to and 20 minutes after the intervention, we measured the serum glucose (mg/dL) and serum insulin (mU/L) levels of the subjects. Patients were followed up 12 hours and 1, 2, and 4 months after the experiment. During the course of the study, 1 patient in the intervention group and 1 patient in the placebo group were lost to follow-up; therefore, they were excluded from the study ( Figure 1 ). The demographic information of patients and additional data were recorded in the checklist. The patients were visited within 12 hours and 4 weeks (1 month), 8 weeks (2 months), and 16 weeks (4 months) after the intervention. Furthermore, the CCCRC was recorded prior to and 4 months after the intervention was done.
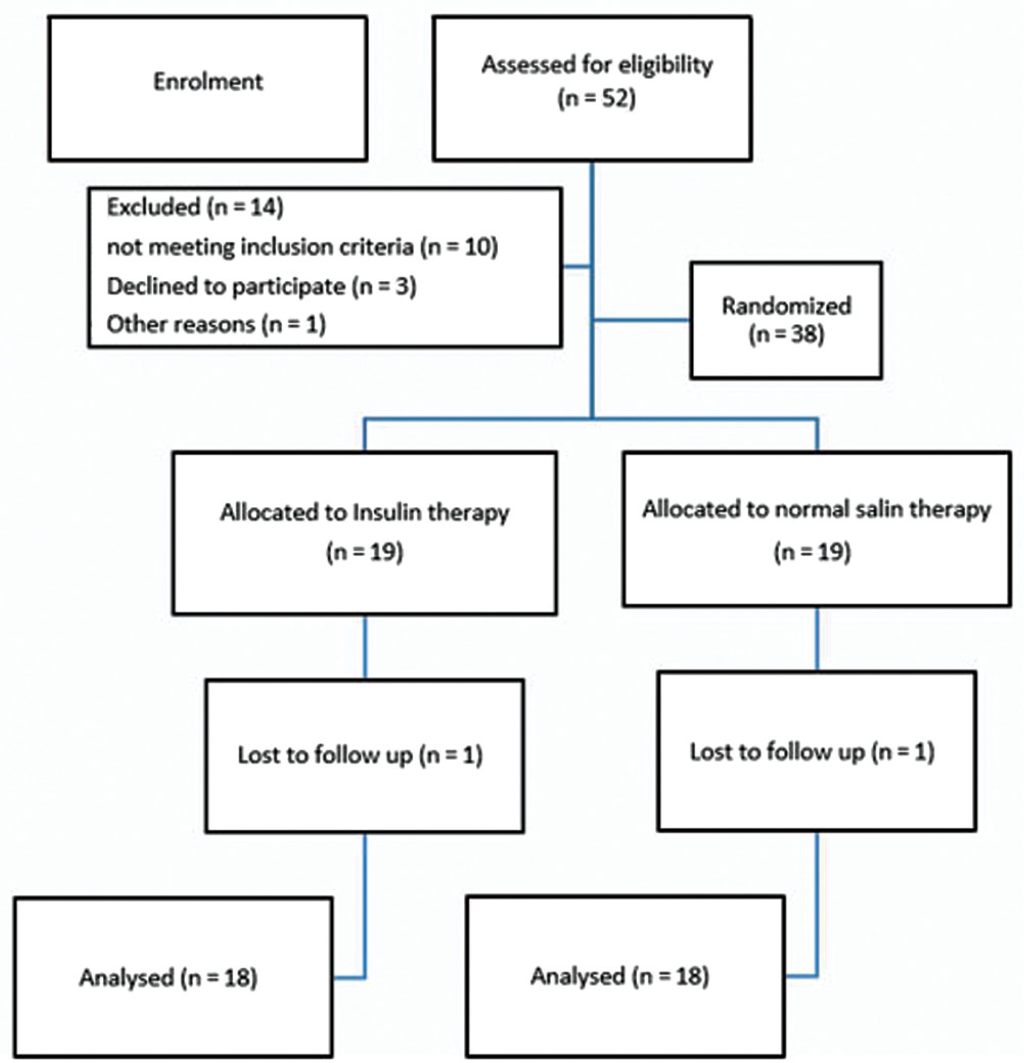
Diagram of the flow of patients through every stage of the study.
Statistics
The sample size was computed based on the sample size estimation formula, in which the confidence level was 95%, the power detection was 80%, and the standard deviation of the n-butanol threshold score was 0.7. In a previous study, the computed least significant difference between 2 groups was 0.4 (between 0.3 and 0.7), in which 38 subjects and 19 subjects were included in each group. 11 The data were analyzed with SPSS version 20 (SPSS, Inc, an IBM Company, Chicago, Illinois). Independent t test, analysis of variance, and Mann-Whitney test were used to determine the relationship between qualitative and quantitative variables; paired samples correlation was used for the comparison of hyposmia before and after the intervention; the χ2 test was used to correlate 2 qualitative variables; and Pearson correlation was used to compare 2 quantitative variables. The data are reported as number (percentage) and mean ± standard deviation. Furthermore, a P value of less than .05 was considered significant.
Results
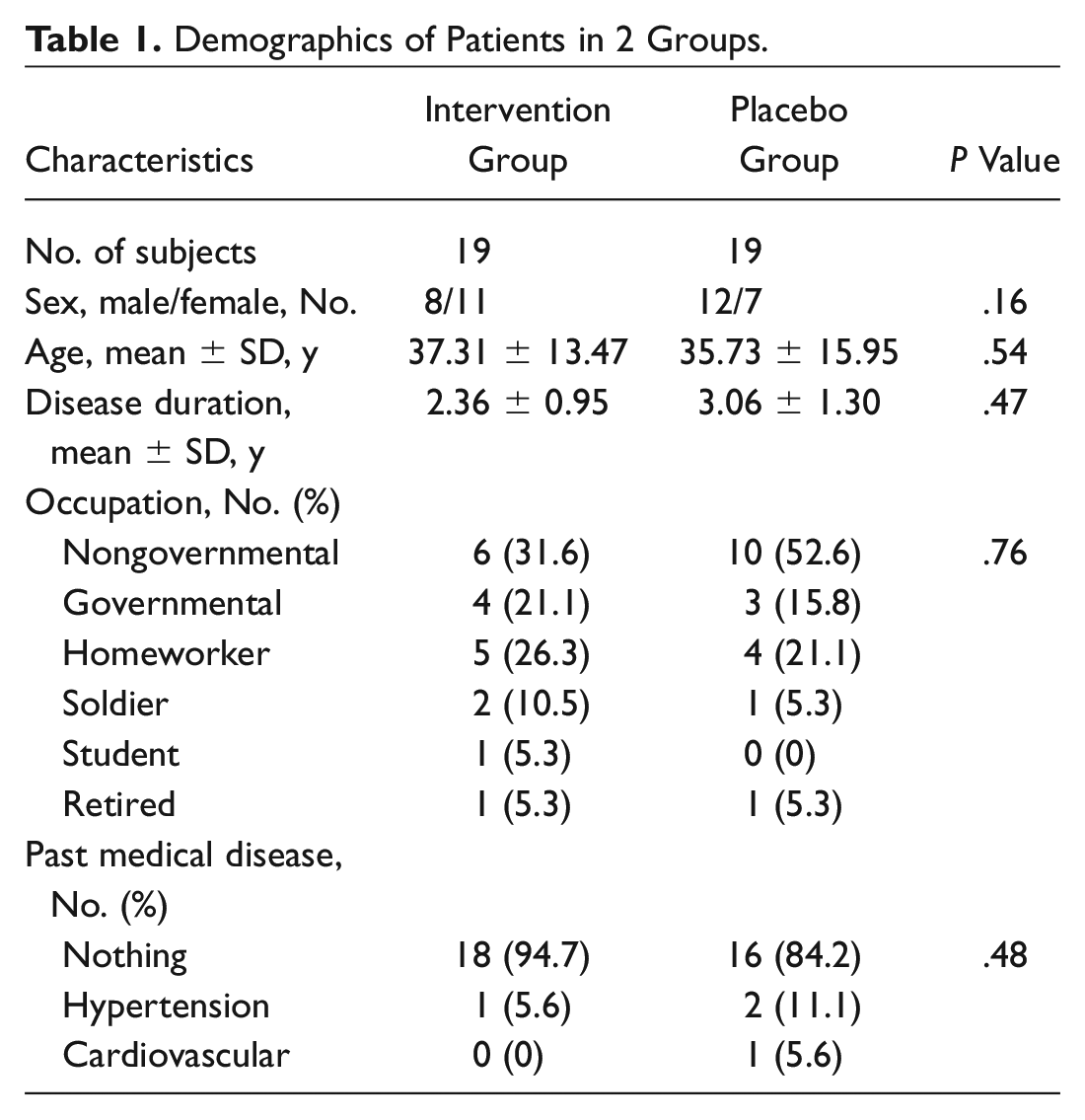
In this study, the mean disease duration in the intervention and placebo groups was 2.36 ± 0.95 and 3.06 ± 1.30 years, respectively. No significant difference was found between the 2 groups in terms of sex (P = .16), age (P = .54), disease duration (P = .47), occupation (P = .79), and past medical condition (P = .48) (other demographics of subjects are summarized in Table 1 ). We measured the CCCRC score in both groups prior to intervention, in which we found mean CCCRC scores of 3.90 ± 0.97 and 3.85 ± 1.03 for the intervention and placebo groups, respectively. Furthermore, based on the results of the Mann-Whitney test, no significant difference existed in the CCCRC score of the 2 groups (P = .89) ( Figure 2 ). The intensities of disease severity in the intervention group were 10.5% for mild hyposmia (5.00-5.75), 63.2% for moderate hyposmia (4.00-4.75), and 26.3% for severe hyposmia (2.00-3.75). On the other hand, the intensities of disease severity in the placebo group were 15.8% for mild hyposmia, 47.4% for moderate hyposmia, and 36.8% for severe hyposmia. Therefore, based on the results of the χ2 test, we found no significant difference in the intensities of disease severity in the 2 groups (P = .61) ( Table 2 ). After 4 months of follow-up, the resulting CCCRC mean scores in the intervention and placebo groups were 5.01 ± 0.74 and 3.83 ± 1.09, respectively. In the Mann-Whitney test, the CCCRC score of the intervention group was significantly higher compared to that of the placebo group (P = .01) ( Figure 3 ). The levels of disease severity in the intervention group were 16.7% for normosmia (6.00-7.00), 50% for mild hyposmia, 27.8% for moderate hyposmia, and 5.6% for severe hyposmia, whereas in the placebo group, the levels were 0% for normosomia, 16.7% for mild hyposmia, 44.4% for moderate hyposmia, and 38.9% for severe hyposmia. Moreover, according to the χ2 test, there was a significant relationship between the 2 groups with regard to disease severity (P = .011) ( Table 3 ). It should also be noted that, based on the paired t test, the change in the CCCRC score of the intervention group after treatment was significant (P < .0001). However, such a significant change in the CCCRC score was not observed in the placebo group (P = .26). In addition, before the intervention, the mean serum glucose levels in the intervention and placebo groups were 85.89 ± 5.93 and 86.84 ± 4.29 mg/dL, respectively. The mean serum insulin levels in the intervention and placebo groups were 1.73 ± 0.17 and 1.77 ± 0.12 mU/L, respectively. No significant differences were found in the serum glucose and serum insulin levels of the 2 groups before treatment (P values were .25 and .36, respectively, according to the independent t test). Twenty minutes after the intervention, the mean serum glucose levels in the intervention and placebo groups were 82.42 ± 6.02 and 86.94 ± 4.26 mg/dL, respectively, and the mean serum insulin levels in the intervention and placebo groups were 1.77 ± 0.14 and 1.66 ± 0.10 mU/L, respectively. Thus, no significant differences were found in the serum glucose and serum insulin levels of the 2 groups after the treatment (P = .15 and P = .40, respectively). Moreover, based on paired samples correlation, serum glucose levels were significantly decreased and serum insulin levels were significantly increased in the intervention group after treatment (both P < .0001). In addition, in the placebo group, no significant difference was found with regard to serum glucose levels (P = .33), but the serum insulin levels were deceased significantly (P < .0001) ( Table 4 ). It is worth mentioning that there were no reported side effects in the administration of intranasal insulin and normal saline in the patients.
Demographics of Patients in 2 Groups.
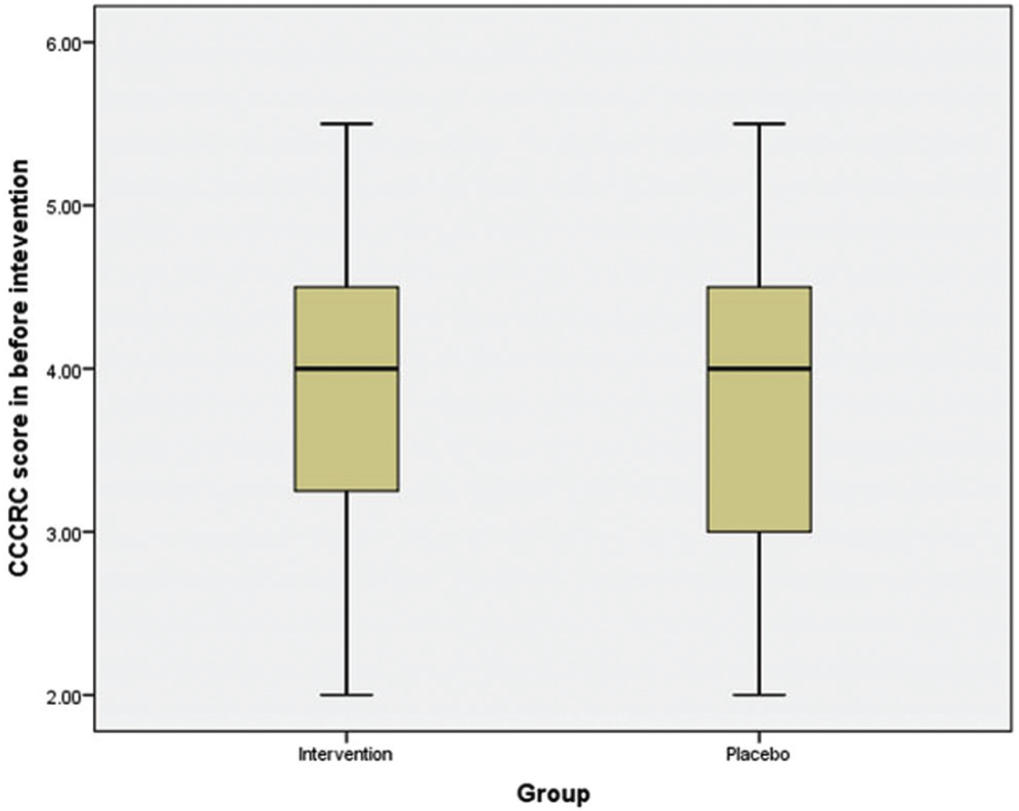
Boxplot of the mean Connecticut Chemosensory Clinical Research Center (CCCRC) score in 2 groups before intervention.
Result of CCCRC Score and Distribution of Subjects in 2 Groups before Intervention.
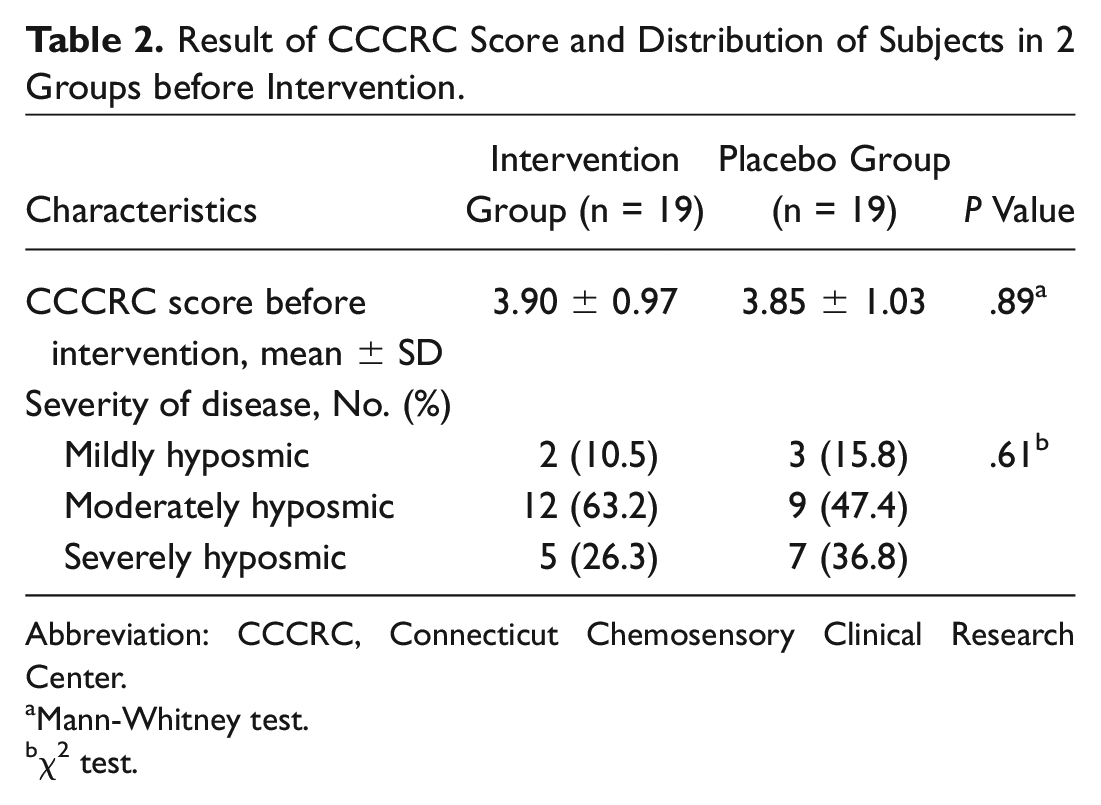
Abbreviation: CCCRC, Connecticut Chemosensory Clinical Research Center.
Mann-Whitney test.
χ2 test.
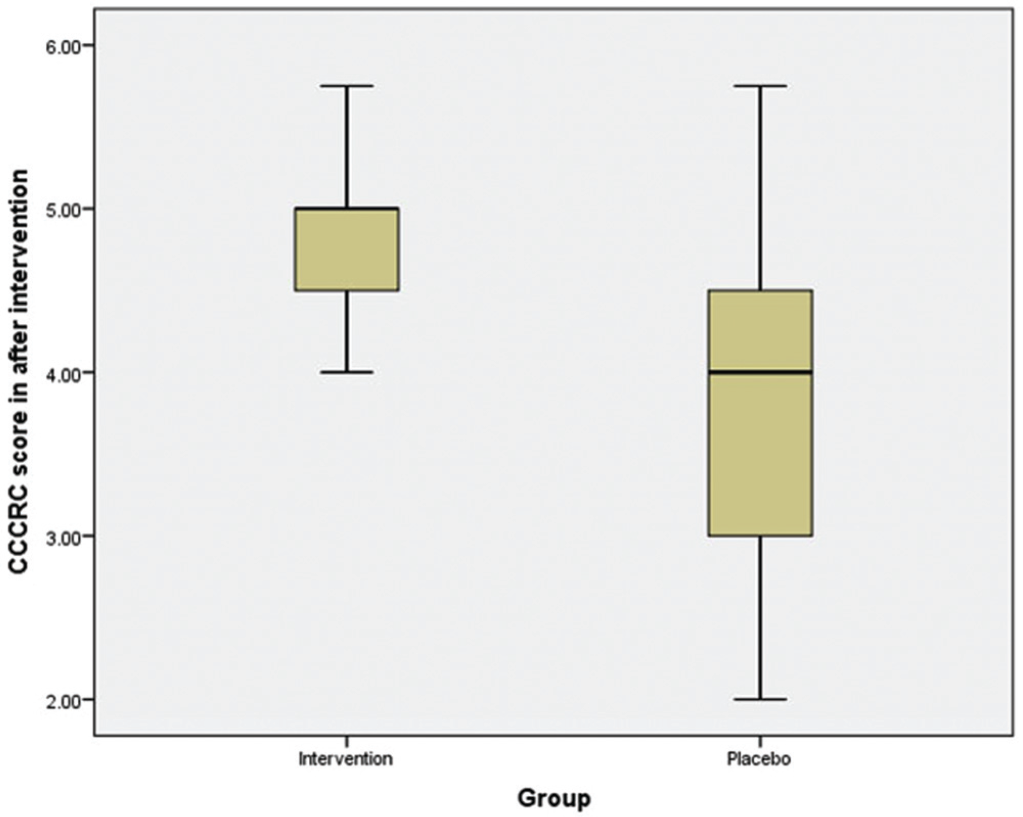
Boxplot of the mean of Connecticut Chemosensory Clinical Research Center (CCCRC) score in 2 groups after intervention.
Result of CCCRC Score and Distribution of Subjects in 2 Groups after 4 Months.
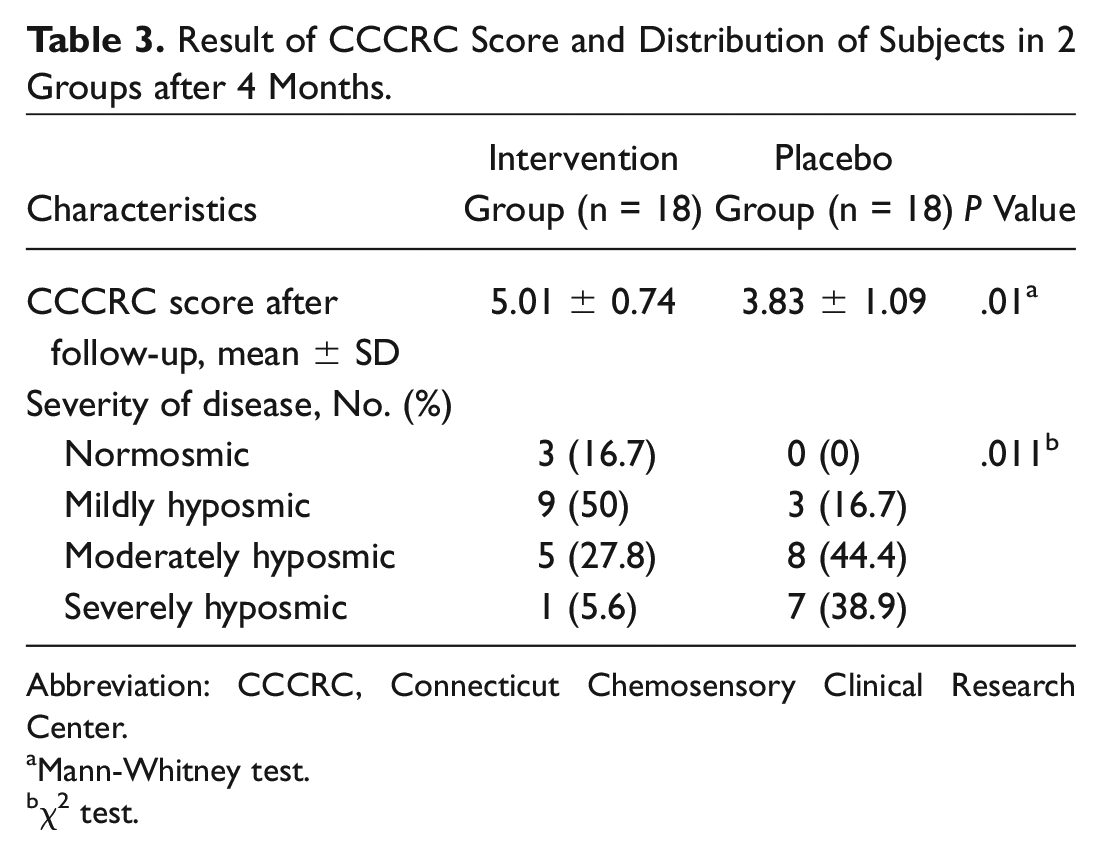
Abbreviation: CCCRC, Connecticut Chemosensory Clinical Research Center.
Mann-Whitney test.
χ2 test.
Mean Blood Sugar and Serum Insulin levels in 2 Groups before and 20 Minutes after Intervention.
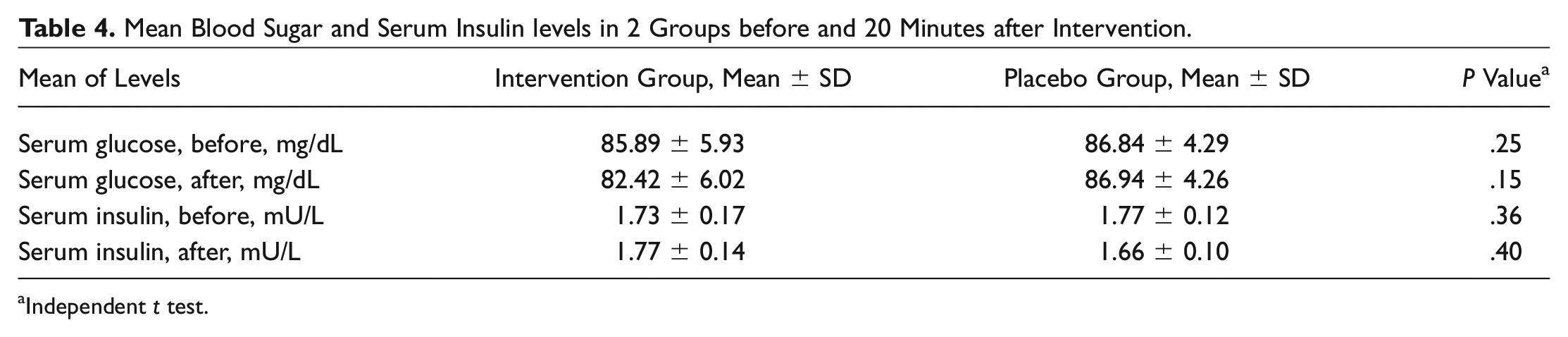
Independent t test.
Discussion
In this study, we investigated the degree of olfactory dysfunction in patients with hyposmia. The results of our study suggest that the administration of 40 IU intranasal insulin yielded a positive significant result in the treatment of patients. Before treatment with intranasal insulin, the mean CCCRC scores of all subjects varied from severe to moderate hyposmic levels. After the interventions, the mean CCCRC score of the intervention group varied from mildly hyposmic to normosmic. All these findings indicate that the administration of intranasal insulin positively and significantly improved the level of hyposmia of the subjects. We also measured serum glucose and serum insulin levels of the patients, and we found that 20 minutes after intervention, the serum glucose levels were decreased and serum insulin levels were increased in the intervention group. Several studies reported that the reduction in growth factor (GF) secretion can lead to hyposmia, as these GFs have stimulatory effects on the olfactory epithelium. A recent study presented the conditions leading to GF-level reductions that may be accompanied by hyposmia. These conditions include but are not limited to trace element and vitamin deficiency, liver disorders, diabetes mellitus, metabolic syndrome, and otolaryngologic and neurodegenerative disorders. Therefore, elevation of GF secretion can be considered for the management of hyposmia.4,12 Some studies have also proposed the role of insulin in increasing GF levels. In line with this, several studies report that insulin, which is a phosphodiesterase enzyme inhibitor, affects the nitric oxide cycle and can therefore cause enhanced levels of GFs such as cyclic guanylate monophosphate (cGMP) and cyclic adenylate monophosphate (cAMP).4,13 In an earlier pilot study, Schöpf et al 9 investigated the effects of intranasal insulin (40 IU) on 10 patients with postinfectious olfactory loss and evaluated their olfactory function through an odor identification test. Furthermore, they demonstrated that intranasal insulin improved the olfactory sensitivity of the patients and that there was a significant improvement in the olfactory function of patients with higher body mass indices. Therefore, they concluded that there may be a relationship between insulin levels in the brain and the level of olfactory dysfunction. A study, in contrast to our findings, was conducted on normosmic patients. This double-blinded study, conducted by Brünner et al, 14 doubted the effect of intranasal insulin (40 IU) in increasing olfactory sensitivity. In this study, a single dose of intranasal insulin resulted in olfactory sensitivity reduction or a decrease in the butanol threshold; however, the patients’ capability to discriminate various odors remained stable, and the authors hypothesized that a reduction in brain glucose levels induced by insulin is responsible for such a negative effect on patients’ sense of smell, but this still remains a matter of dispute. Brünner et al 15 evaluated the effects of intranasal insulin (40 IU) on odor identification through spatial memory of male humans. They found that intranasal insulin can improve the delay in odor identification through spatial memory and that this method did not have any adverse effects or cause an increase in plasma glucose levels. However, intranasal insulin had no effects on odor recognition as well. Furthermore, they suggested that acute intranasal insulin can improve odor identification though spatial memory. In another study, the significant effect of intranasal insulin in improving memory and mood was reported. This study was performed on patients with cognitive disorders such as Alzheimer’s disease. No adverse effects were reported in this study as well. 16 In a study on mice models, the administration of intranasal insulin before surgery was reported to reduce the risk of anesthesia-induced cognitive disease and Alzheimer’s disease. 10 Marks and colleagues 17 evaluated the effect of intranasal insulin administration on memory, anxiety, and olfactory behaviors in mice models, and they reported that intranasal insulin increased olfactory discriminatory ability and memory and reduced anxiety. In line with these finding, Henkin et al 12 used intranasal theophylline for the treatment of hyposmia, in which they found resulting improvement in hyposmia and hypogeusia. They concluded that since theophyline is a phosphodiesterase inhibitor, it can cause an increase in the levels of cAMP and cGMP.
Conclusion
Based on the results of our study, we found that, through a butanol threshold test, intranasal insulin (40 IU) administration was able to increase odor identification. It also improved olfactory dysfunction in patients with hyposmia without any adverse effects. Therefore, we suggest intranasal insulin administration for the therapeutic management of olfactory dysfunction. However, due to limited research on this matter, we recommend the inclusion of larger populations in future studies.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.