
Abstract
Objective
To evaluate the short- and long-term effects of tricyclic antidepressants (TCAs) and gabapentin in the treatment of unexplained chronic cough (UCC).
Study Design
Prospective cohort.
Setting
Tertiary care hospital.
Subjects and Methods
Patients seen between July 2016 and March 2017 were included following a formal workup and clinical evaluation indicative of UCC. Patients were placed on either a TCA (amitriptyline or nortriptyline) or gabapentin. Leicester Cough Questionnaire (LCQ) and percentage improvement scores were obtained prior to treatment initiation and at 2 and 6 months of neuromodulator treatment. A linear mixed model assessed the change in LCQ score between the 2 treatment time points and baseline scores.
Results
Twenty-eight patients completed a total of 37 neuromodulator trials. Gabapentin demonstrated statistically significant improvement in LCQ scores at 2 months (2.48 points, P≤ .01) and 6 months (5.40 points, P = .01) of treatment as compared with baseline. Patients taking TCAs demonstrated statistically significant improvement of LCQ scores at 2 months of treatment (3.46 points, P≤ .01). However, the majority of patients discontinued treatment, most commonly secondary to the development of tachyphylaxis after 2 months, precluding analysis at 6 months.
Conclusion
While both neuromodulator classes demonstrated short-term benefit, the majority of patients discontinue treatment prior to 6 months, with patients taking TCAs discontinuing more frequently than patients on gabapentin. Future investigations are warranted evaluating tachyphylaxis and the utility of dual treatment therapies designed to address peripheral and central sensory pathways involved in UCC.
Keywords
Approximately 12% to 50% of patients with chronic cough have a negative diagnostic workup or remain refractory to empiric treatment.1,2 In such cases, the cough is considered an unexplained chronic cough (UCC), a term proposed by the American College of Chest Physicians (ACCP). 3 Many patients with UCC demonstrate a form of airway allodynia, characterized by paroxysmal spasms occurring with benign stimuli (“triggers”), such as talking, position change, or odors. 4 This hypersensitivity is believed to arise from a neuropathic process affecting cough reflex sensory circuits, similar to the pathophysiology behind chronic pain. 5 Unsurprisingly, the current pharmacotherapy for UCC includes neuromodulating medications, such as tricyclic antidepressants and gabapentinoids. Of these 2 classes, gabapentin and amitriptyline have the richest history in treating UCC.6,7 While gabapentin was recommended by the ACCP for treating UCC, amitriptyline was not formally recommended, given its lack of studies with validated cough improvement measures. 3 Additionally, few studies have used validated measurements to examine the long-term outcomes of either neuromodulator.8,9 The purpose of this study was to examine the short- and long-term efficacy of tricyclic antidepressants and gabapentin with validated cough measurements.
Methods
Following Cleveland Clinic Institutional Review Board approval, a prospective study was conducted on UCC from July 2016 and March 2017 with patients who were prescribed gabapentin, amitriptyline, or nortriptyline with the intention of completing 6 months of neuromodulator treatment. Participants were initially evaluated in a laryngology clinic or a multidisciplinary cough clinic, consisting of otolaryngology, pulmonology, and speech language pathology evaluation. Patient were assessed per ACCP algorithims 10 (see Supplemental Table S1, available in the online version of the article). Patients were included if their history suggested cough hypersensitivity and they were refractory to empiric treatment for common causes of cough. All other patients, including those who failed to follow up or those whose cough resolved independently, were excluded. Baseline demographics were recorded, including sex, age, duration of cough, comorbidities related to chronic cough, and concurrent speech therapy. Each patient completed a list of questions pertaining to common symptoms and triggers. 11 Figure 1 details the protocol used for neuromodulator selection, drug titration, and follow-up.
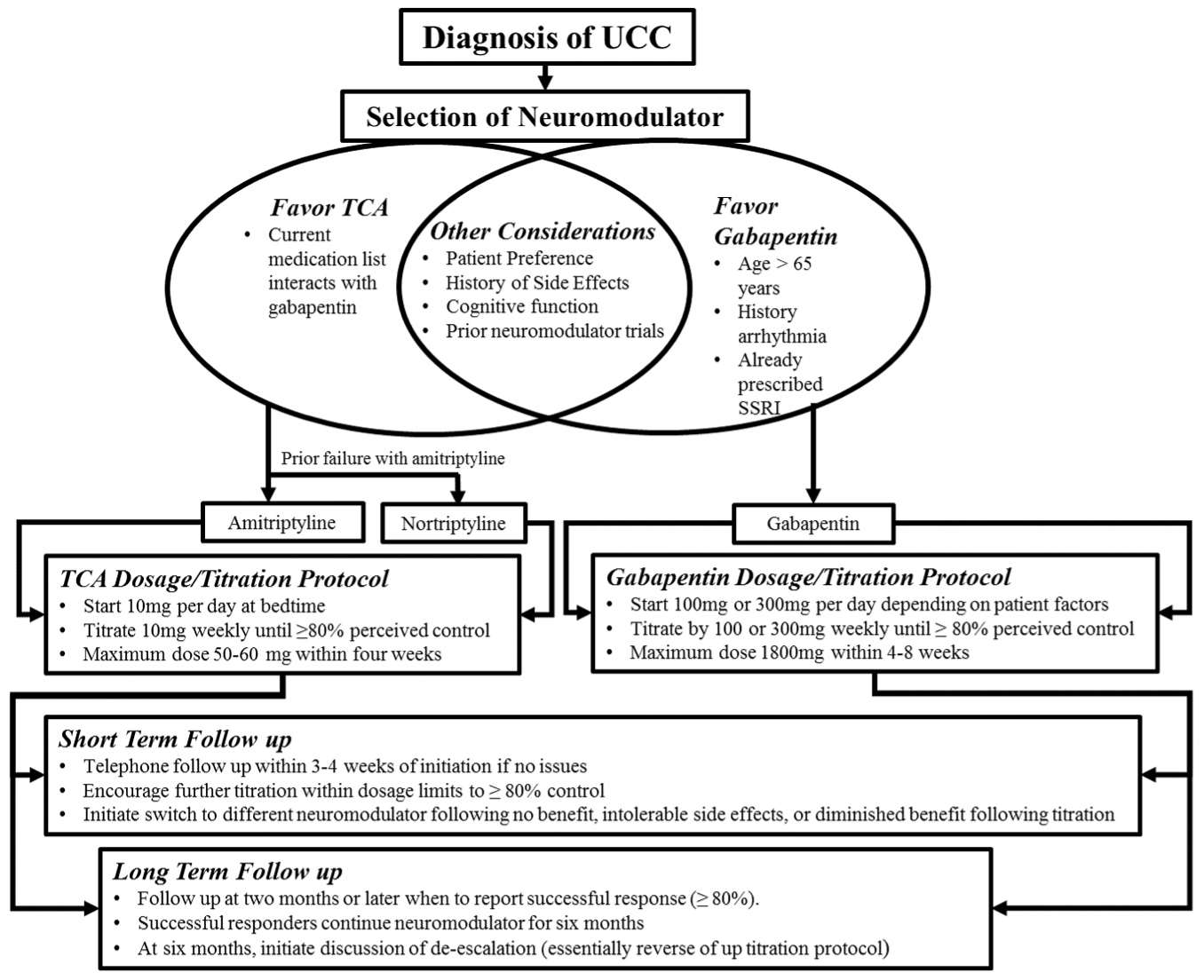
Patient factors determine neuromodulator selection with gradual titration based on response (lowest dose achieving at least 80% perceived cough control) and side effects. Problematic side effects are immediately reported to make treatment adjustments. SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant; UCC, unexplained chronic cough.
Outcome Measures
The Leicester Cough Questionnaire (LCQ) was the primary method of measuring treatment success. The LCQ is a validated measurement of cough severity that provides a score between 3 and 21 based on the physical, psychological, and social burden of a patient’s cough. 12 Lower LCQ scores indicate a cough severely affecting quality of life, while a higher score indicates a more favorable health status. 13 The minimal clinically important difference in LCQ score change is 1.3 points, while moderate and large clinically important differences (MoCID and LCID) are 1.7 and 2.7 points, respectively. 14 LCQ forms were completed prior to treatment initiation (baseline) and at 2 and 6 months of treatment. With each LCQ measurement, a percentage improvement score was also recorded, as it is a common method of measuring subjective cough improvement.9,15,16 When patients discontinued neuromodulator treatment before 6 months, an explanation was sought, such as no therapeutic benefit, intolerable side effects, or the development of tachyphylaxis. We define tachyphylaxis as diminishing benefit from a previously effective neuromodulator. We offered an alternative neuromodulator to patients who quit prior to 6 months, obtaining 2-month LCQ scores from these additional trials if available.
Statistical Analysis
Associations among baseline characteristics, comorbidities, symptoms, and triggers with LCQ scores were investigated with Wilcoxon rank sum tests. LCQ scores tracked over time for the various treatment groups were modeled with a linear mixed model based on an assumption of an autoregressive first-order correlation structure. This model accounts for the repeated measures over time and allows for the inclusion of all patient trials regardless of whether patients completed both the 2- and 6-month LCQs or just the 2-month LCQ. Within this modeling framework, contrast statements investigated the primary comparisons of interest, such as LCQ changes from baseline to 2 months and from baseline to 6 months for the gabapentin and tricyclic antidepressant cohorts. A similar analysis was conducted keeping amitriptyline and nortriptyline separate to ensure similar effect sizes and to rationalize their grouping as tricyclic antidepressants. In addition to demonstrating statistical significance with a 0.05 type I error, change in LCQ had to be greater than the minimal clinically important difference. As it is unclear whether first and subsequent trials are truly interchangeable, a sensitivity analysis was performed that included only initial patient trials. How percentage improvement scores correlated with changes in LCQ scores was assessed with a Pearson correlation analysis.
Results
Patient Population and Demographics
During enrollment, 59 patients with chronic cough were evaluated. Thirty-four demonstrated sufficient evidence through clinical history, diagnostic testing, or previously failed empiric treatment to support a diagnosis of UCC. Two patients with spontaneously resolving coughs and 4 patients who failed to complete 2 months of any neuromodulator treatment were excluded. Therefore, the study cohort consisted of 28 patients, who were predominantly women (57%), who had a mean age of 61 years (range, 34-77 years), and whose mean duration of cough was 7.93 years (range, 2 months to 21 years). Half the cohort reported developing the cough following a resolved upper respiratory illness. Ten patients were previous smokers. Twelve patients agreed to undergo concurrent speech pathology–led cough suppression therapy. Table 1 provides a list of chronic cough–related conditions for which the cohort was previously diagnosed and refractory to treatment. The most common comorbidities reported were gastroesophageal reflux disease, followed by upper airway cough syndrome. Table 2 summarizes the diagnostic workup and prior treatment for all patients. There was no evidence of any association between LCQ change at 2 months and any recorded demographics, comorbidities, or behavioral therapy (all P > .05).
Prior Diagnosed or Suspected Causes of Chronic Cough for Study Cohort (N = 28).
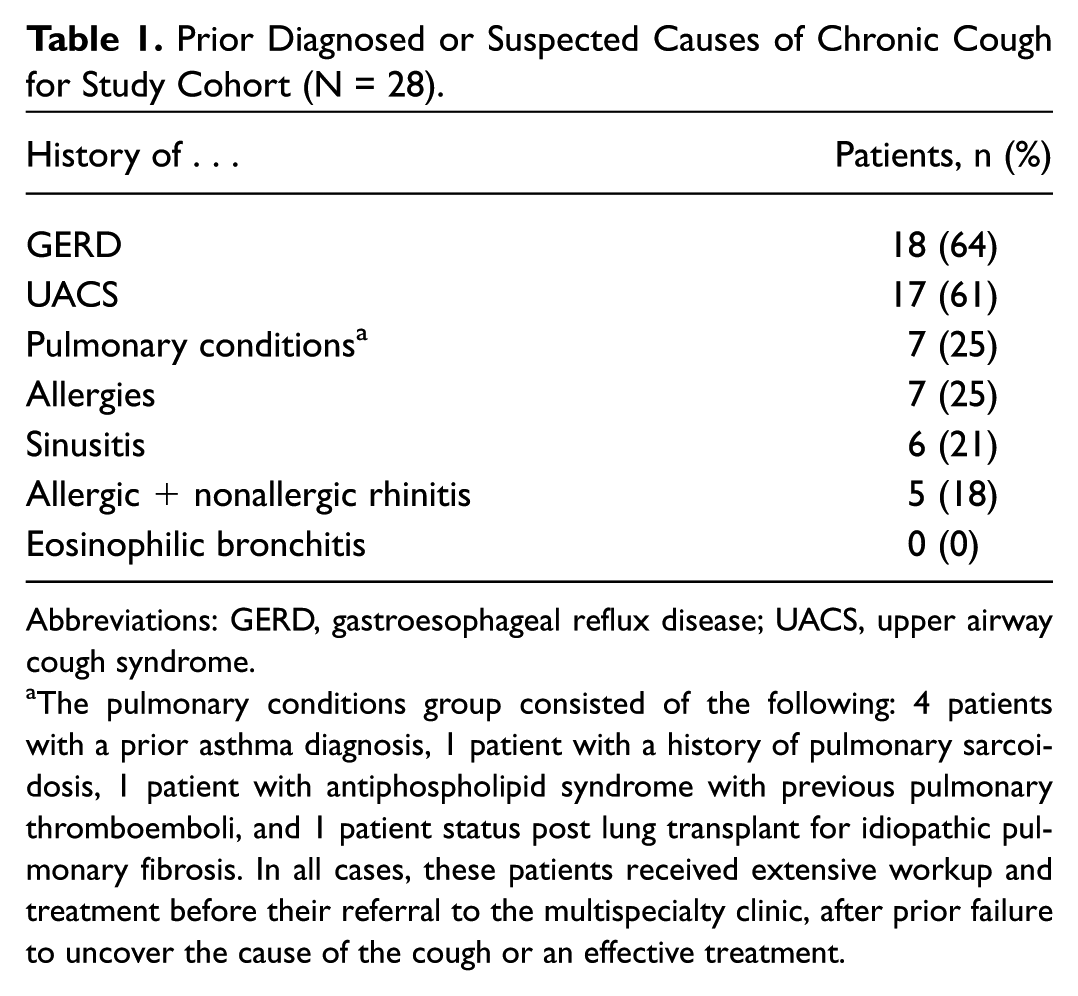
Abbreviations: GERD, gastroesophageal reflux disease; UACS, upper airway cough syndrome.
The pulmonary conditions group consisted of the following: 4 patients with a prior asthma diagnosis, 1 patient with a history of pulmonary sarcoidosis, 1 patient with antiphospholipid syndrome with previous pulmonary thromboemboli, and 1 patient status post lung transplant for idiopathic pulmonary fibrosis. In all cases, these patients received extensive workup and treatment before their referral to the multispecialty clinic, after prior failure to uncover the cause of the cough or an effective treatment.
Diagnostic Workup Summary of Study Cohort. a

The table depicts the number of patients who received formal testing in the organ system specified, did not have formal diagnostic testing but received empiric treatment, or did not have formal testing or complete empiric treatment. The reason for inclusion of patients in the last category is given on the far right. As upper airway cough syndrome, rhinitis, and sinusitis are all diagnosed through clinical examination, all patients effectively had workups for sinonasal pathology during their initial visits. The diagnostic testing performed for each organ system was based on the formal recommendations by the American College of Chest Physicians. 14
Symptoms and Triggers
Table 3 contains frequently reported cough triggers and symptoms. Patients most commonly complained of paroxysmal spasms of coughing (75%), followed by throat irritation and throat clearing (both 71%). The most frequently reported cough triggers were talking and position change (both 79%). Wilcoxon rank sum testing revealed that patients who complained of paroxysmal spasms or dysphonia or had a cough triggered by talking demonstrated significantly better LCQ scores after 2 months of treatment (all P < .05).
Cough Symptoms and Triggers. a
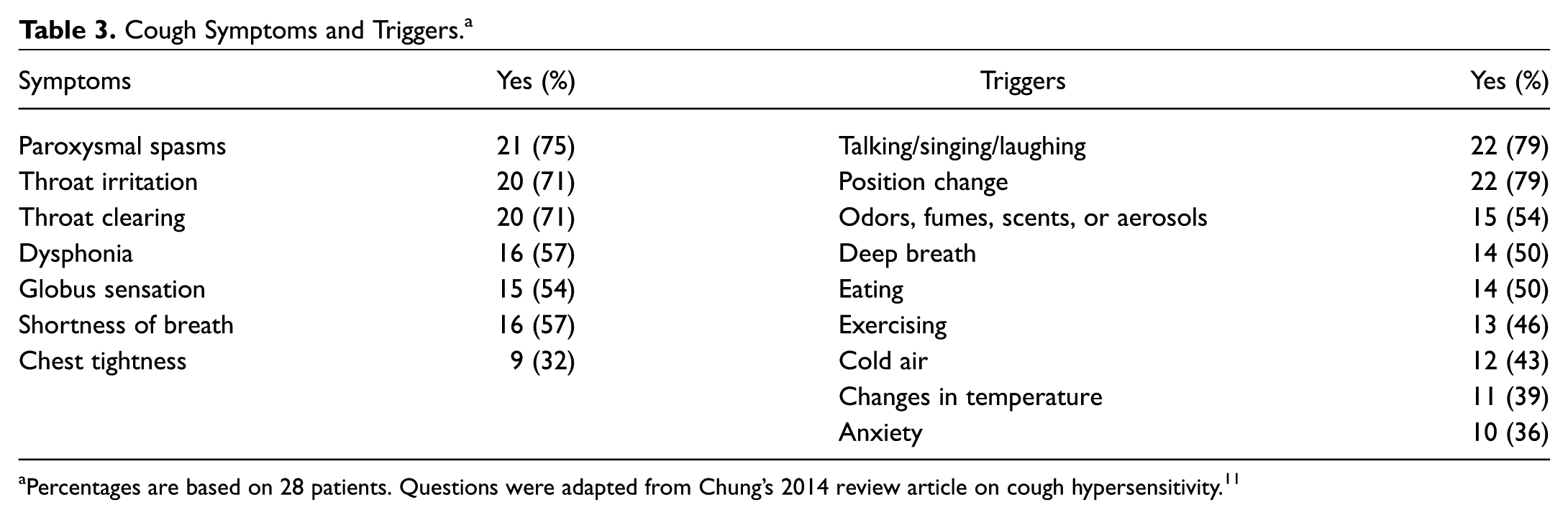
Percentages are based on 28 patients. Questions were adapted from Chung’s 2014 review article on cough hypersensitivity. 11
Neuromodulators and LCQ Improvement
Mean individual and group average LCQ scores for both neuromodulator classes are presented in Figure 2 . Twenty-one patients constituted the gabapentin group, with 19 being in their first neuromodulator trial and 2 completing their trial after discontinuing a tricyclic antidepressant. Nineteen 2-month LCQ scores were obtained from these 21 trials of gabapentin ( Table 4 ). The median change in LCQ for gabapentin through 2 months of treatment demonstrated a significant increase (P < .01) of 2.48 points (600 mg, median; 300 mg, mode), with 11 trials (58%) achieving the MoCID (3 trials) or LCID (8 trials) for the LCQ. Analysis of LCQs from the 17 patients who started the study on gabapentin yielded similar results (2.48-point increase, P = .01). Of these 17 patients, 10 (59%) completed 6 months of treatment, recording a 5.40 increase in LCQ points from baseline (P < .01; 900 mg, median/mode), with 9 (90%) patients achieving the MoCID (2 patients) or LCID (7 patients) for LCQ.
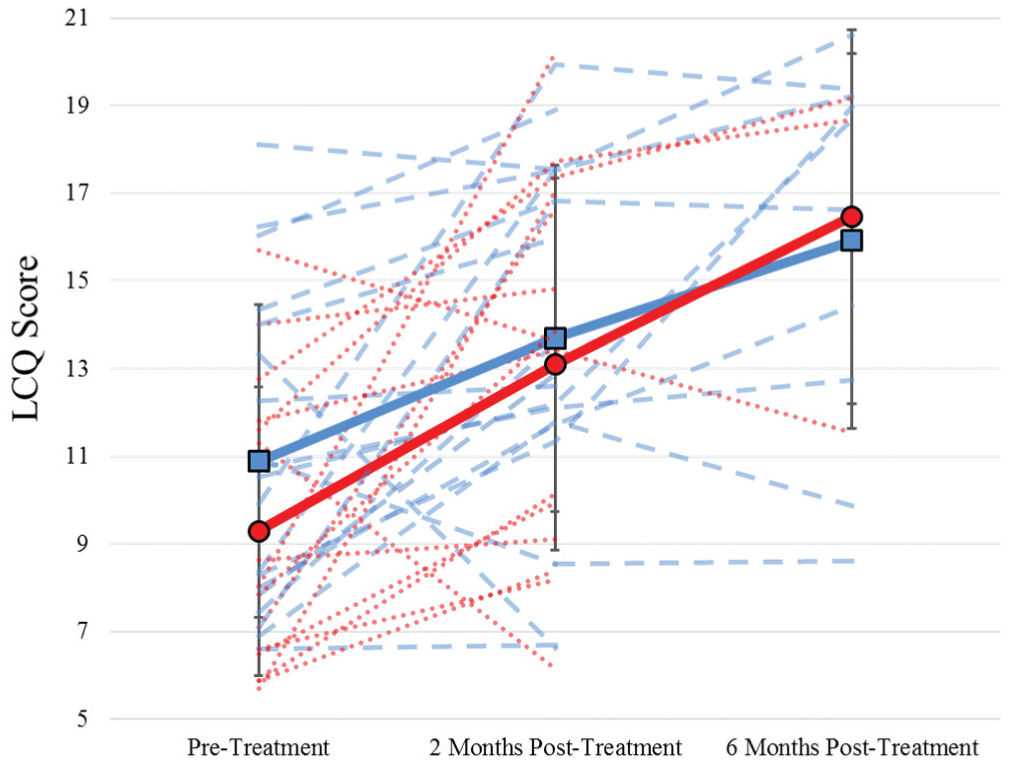
Solid colored lines represent the mean LCQ scores for gabapentin (blue) and tricyclic antidepressants (red), with standard deviations indicated by vertical. The dashed lines represent the individual LCQ scores. LCQ, Leicester Cough Questionnaire.
Neuromodulator Trials. a
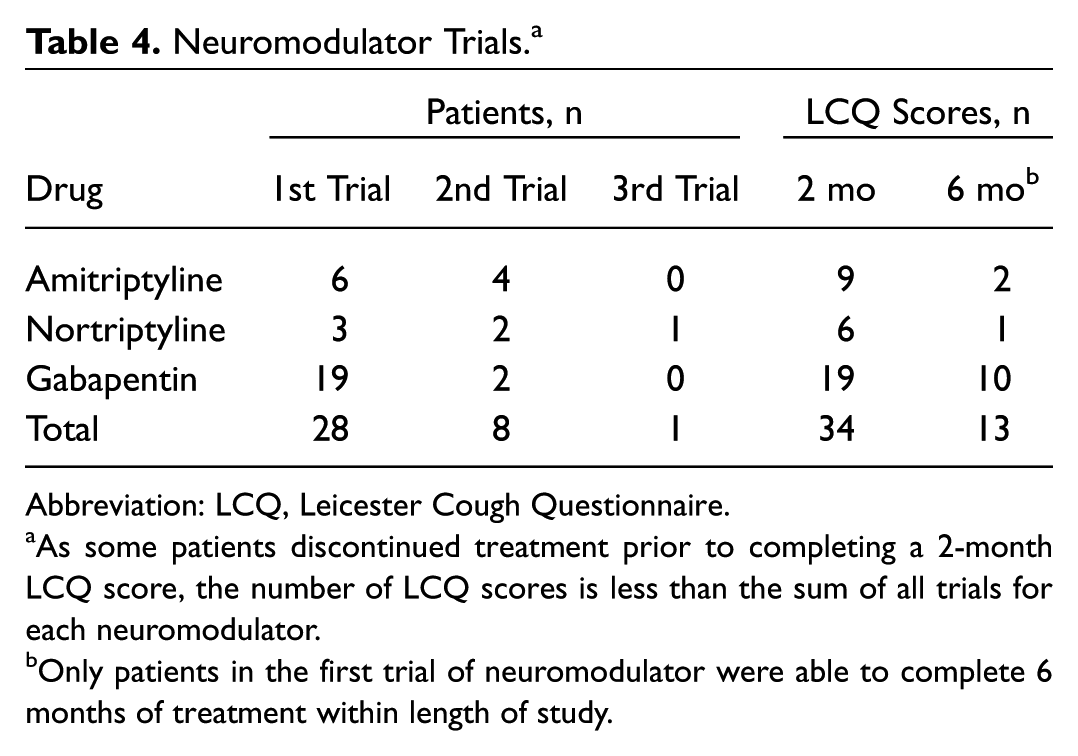
Abbreviation: LCQ, Leicester Cough Questionnaire.
As some patients discontinued treatment prior to completing a 2-month LCQ score, the number of LCQ scores is less than the sum of all trials for each neuromodulator.
Only patients in the first trial of neuromodulator were able to complete 6 months of treatment within length of study.
Nine patients were initially prescribed a tricyclic antidepressant, while 7 tried the drug class after discontinuing gabapentin before 6 months ( Table 4 ). Fifteen 2-month LCQs were obtained from these 16 trials. The median change in LCQ for tricyclic antidepressants at 2 months was a significant (P < .01) 3.46-point increase (30 mg, median/mode), with 9 trials (60%) achieving the MoCID (1 trial) or LCID (8 trials) for the LCQ. Additionally, a secondary analysis of the 9 patients who began the study with a tricyclic antidepressant demonstrated a significant change (4.27-point increase, P < .01). Unfortunately, there was a notable drop-off in the number of patients completing 6 months of treatment, preventing a meaningful analysis of the 6-month scores and leaving only 3 available scores (–0.27, +6.41, and +7.07 points). Upon separate examination of amitriptyline (n = 9) and nortriptyline (n = 6), the observed effects were similar (amitriptyline, 4.27-point increase; nortriptyline, 2.99-point increase), supporting the combination of these tricyclics into 1 group. Despite the improvements with either neuromodulator class, no patient reported complete cough cessation at 2 or 6 months.
Percentage Improvement
Percentage improvement scores were compared with change in LCQ score at 2 and 6 months. There was a significant correlation between the measurements of improvement at 2 months ( Figure 3 ; coefficient, 0.76; 95% CI, 0.53-0.89; P < .001). Another significant correlation was observed at 6 months, although with a much wider confidence interval due to the smaller sample size (0.82; 95% CI, 0.38-0.95; P = .004).
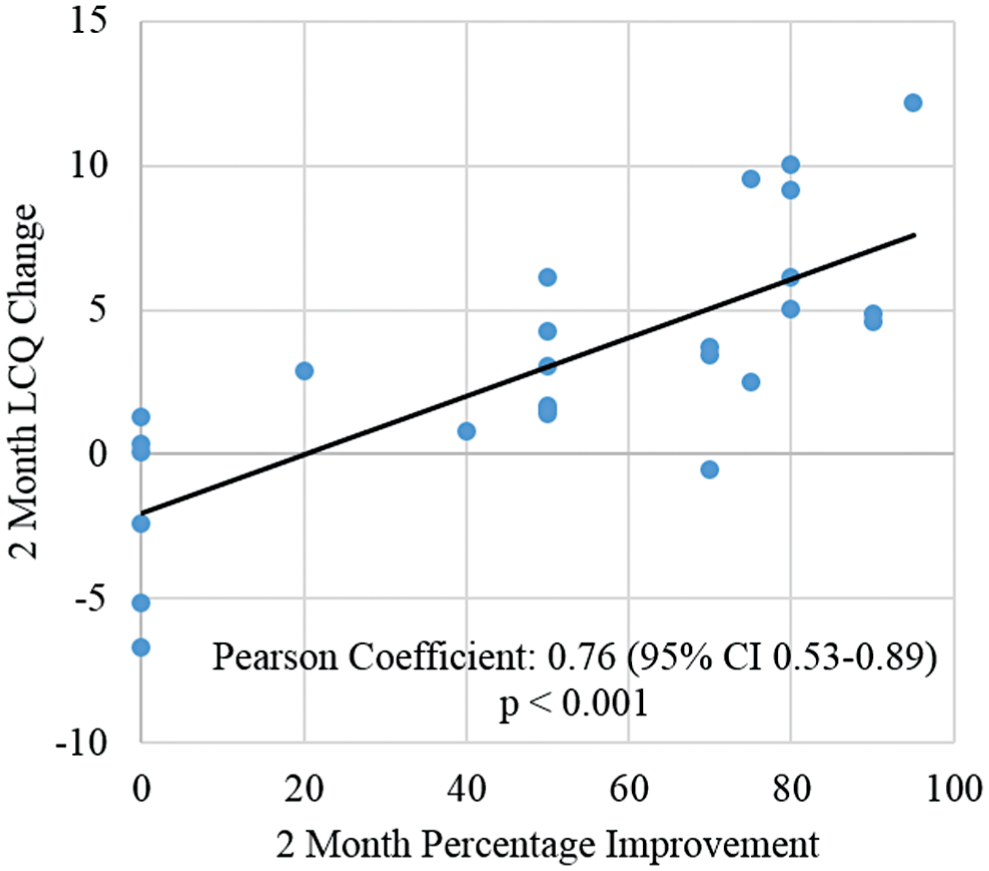
Two-month percentage improvement scores vs 2-month LCQ change. Only results from each patient’s initial neuromodulator trial are included. R 2 = 0.57. LCQ, Leicester Cough Questionnaire.
Overall Outcomes
Of the 13 patients who successfully completed 6 months of treatment with the first neuromodulator prescribed, 4 quit shortly after the data acquisition at 6 months, reducing this total to 9 ( Table 5 ). The majority of treatment failures during the first trial were due to a diminishing therapeutic effect of the neuromodulator over time (labeled “tachyphylaxis”). For all neuromodulator trials, no perceived benefit was the most common cause of drug discontinuation (Supplemental Table S2, available in the online version of the article). Side effects were the least common reason for drug discontinuation (Supplemental Table S3, available in the online version of the article).
Outcomes of the First Neuromodulator Trial. a
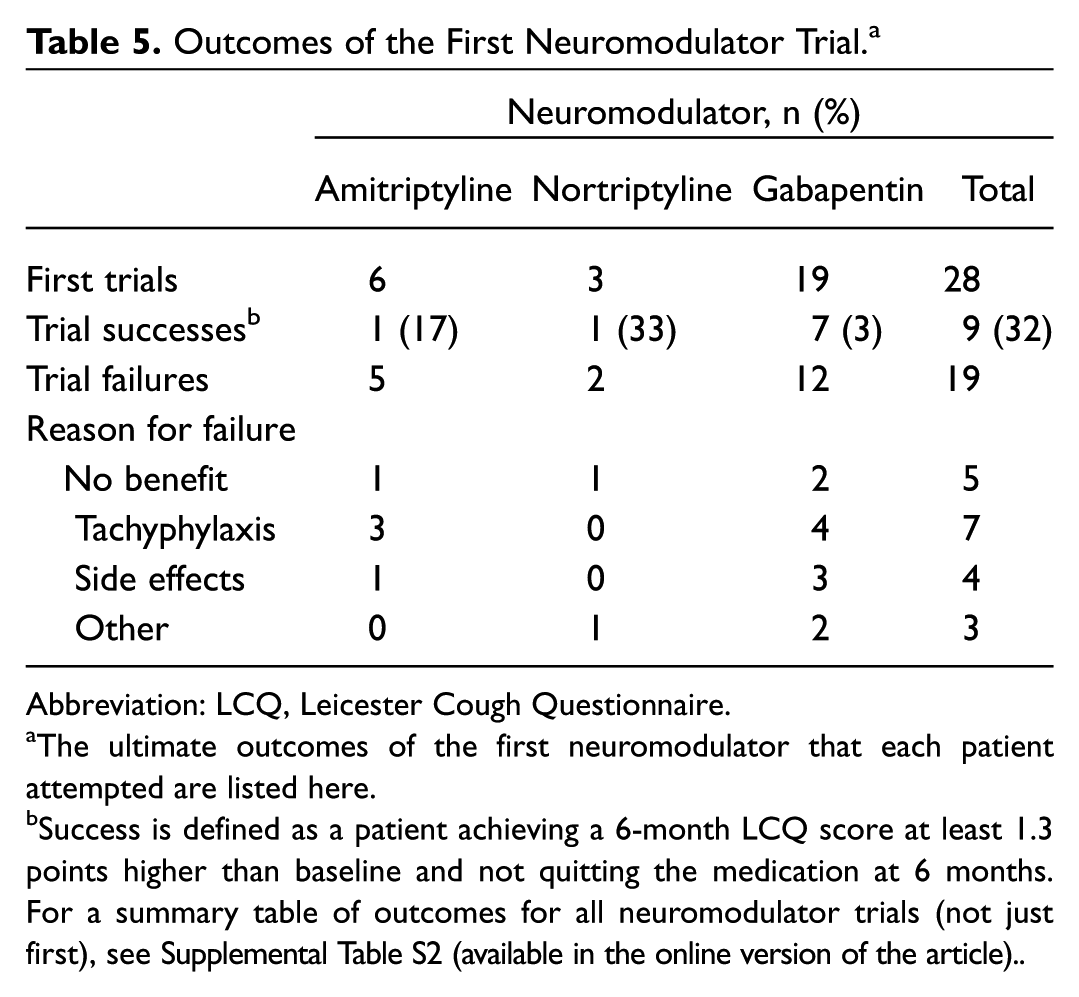
Abbreviation: LCQ, Leicester Cough Questionnaire.
The ultimate outcomes of the first neuromodulator that each patient attempted are listed here.
Success is defined as a patient achieving a 6-month LCQ score at least 1.3 points higher than baseline and not quitting the medication at 6 months. For a summary table of outcomes for all neuromodulator trials (not just first), see Supplemental Table S2 (available in the online version of the article).
Discussion
The origins of UCC are not fully elucidated but are possibly due to repetitive stimulation by noxious stimulants (viral antigens, allergens, adjacent disease processes) causing phenotypic changes in the type or quantity of receptors on afferent airway neurons and leading to increased activation of the cough reflex.4,17 While this explains benign cough triggers, it does not fully explain the paroxysmal coughing bouts observed in the absence of stimuli or the refractory response to maximal empiric treatment of patients with UCC. These other observations point to an additional process, referred to as central sensitization, where the pre– and post–synaptic receptor changes, synaptic remodeling, and neuroinflammation that occur within the sensory circuits of the spinal cord, brainstem, somatosensory cortex, and noradrenergic descending pain modulatory pathways result in a state of neuronal overexcitability that remains after removal of an inciting stimulus.5,18 Recent functional magnetic resonance imaging studies of patients with chronic cough provide evidence that the processes described in models of neuropathic pain are likely occurring in UCC. 17
The neuromodulators are believed to treat the hypersensitivity and central sensitization observed in patients with UCC, as they do for patients with neuropathic pain. While gabapentin is known to classically exert its effect within the central nervous system through inhibition of voltage-dependent calcium channels, more recent investigations demonstrated its ability to increase noradrenergic signaling within the locus coeruleus (brainstem nuclei located upstream of descending pain modulatory pathways).19 -21 Tricyclic antidepressants, which are fundamentally serotonin-norepinephrine reuptake inhibitors, also work in descending pain pathways. 19 Gabapentin is currently recommended by the ACCP for use in UCC. 3 While a randomized placebo-controlled trial of amitriptyline in UCC was performed in 2006, issues with the reporting of the randomization and blinding protocol swayed the ACCP from using the data to make a formal recommendation.3,22 We successfully completed a prospective analysis examining the short- and long-term improvements observed among patients taking a tricyclic antidepressant or gabapentin in the treatment of UCC using the previously validated LCQ as our primary measure. 12 With our LCQ scores, we observed a significant improvement in cough symptoms among patients taking a tricyclic antidepressant. As the majority of these changes were above the LCID for the LCQ (8 of 9 patients), our data support the expectation that patients who benefit from tricyclic antidepressants should experience a robust response to treatment within a short-term period. Gabapentin also demonstrated efficacy through 2 months, consistent with the results of a previous randomized trial. 23 However, only gabapentin maintained efficacy at 6 months, as nearly all patients on a tricyclic antidepressant discontinued by this time, with a lack of benefit the most common reason for discontinuation, accounting for all tricyclic antidepressant trials (Supplemental Table S2, available in the online version of the article). This lack of benefit is not surprising, as the tricyclics are intermittently effective for patients with neuropathic pain.24,25 Although a lack of benefit was also a fairly common reason why patients discontinued gabapentin secondary, nearly 50% of patients who started the study taking gabapentin completed 6 months of treatment (9 of 19). While different sites of actions within the nervous system may be the reason for the difference in lengths of effectiveness between the drug classes, this is speculative.
We observed the development of tachyphylaxis in both gabapentin and amitriptyline. Our a priori decision to assess for tachyphylaxis was determined by past experiences with patients who discontinued an initially efficacious neuromodulator when the drug became ineffective or required dosing titration to a point that they experienced intolerable side effects. While the chronic cough literature alludes to tachyphylaxis, no study directly monitored it.16,26 A recent study found that a downregulation of glutamate transporter 1 (necessary for initiating noradrenergic signaling) in the locus coeruleus was responsible for decreased efficacy of gabapentin in treating central hypersensitivity in rodent neuropathic pain models. 27 As tricyclic antidepressants are believed to work downstream from this site, such a phenomenon occurring in humans would provide an explanation for how both drug classes are affected. 19 More research is needed to determine the true prevalence of tachyphylaxis in this patient population.
Percentage improvement is an easily understandable and efficient method of obtaining a patient’s perceived benefit to cough treatment, as used in several previous chronic cough investigations.9,15,16 Unfortunately, it is not a validated tool for measuring cough response to treatment. 12 This study found a statistically significant correlation between percentage improvement scores and LCQ change at 2 and 6 months. While we believe that our findings support the use of percentage improvement in clinical practice, more formal validation studies are needed before this tool should be employed in clinical studies.
Through our tests of demographics, comorbidities, symptoms, and triggers, we found that patients reporting dysphonia or paroxysmal spasms or having a cough triggered by speech showed significant LCQ score improvement at 2 months (>1.3-point improvement vs those without specific symptoms or trigger, P < .05). This finding likely comes from the improvement in health status gained from improved phonation and removal of fear concerning when the next uncontrollable bout will come. Thus, treatment with neuromodulators has a far-reaching effect on symptom improvement but also a functional change in relation to laryngeal mechanism. We were surprised to find no difference in 2-month LCQ score change among patients receiving concomitant speech therapy, as the literature strongly supports speech therapy for chronic cough treatment.3,28,29 Anecdotally, although speech therapy is offered to all patients, those with the severest coughs are the most willing to undergo a nonpharmacologic intervention. However, baseline LCQ scores between patients who did and did not do speech therapy were similar, which is why we are unable to provide an explanation for this result.
Limitations and Future Directions
There are several limitations to our work. While we made every effort to enroll as many patients with UCC as possible, our cohort consisted of only 28 patients. While the sample appears small, it is relatively the same size as those in other recent prospective cough studies.30 -32 Additionally, we unexpectedly benefited from the additional neuromodulator trials that some of our study participants completed, which provided additional 2-month LCQ scores for analysis. Inclusion of multiple treatment trials was deemed permissible from our findings in a separate retrospective analysis performed on previously treated patients with UCC, where approximately 40% of patients who benefited from neuromodulator treatment did so with their second or third neuromodulator attempt. This benefit often came following failure with a different neuromodulator class, supporting the notion that completely different responses to neuromodulators can be observed within the same patient (unpublished data). As not including subsequent or multiple neuromodulator trials would be ignoring a clinically relevant finding in this patient population, we were obligated to include these additional trials in our primary analysis. Of note, due to the length of the study, only a small subset of patients contributed data for multiple treatment trials. To control for this variation, we performed sensitivity analyses including only the results of the patient’s first neuromodulator trial. While our data are largely consistent through these additional analyses, we do acknowledge the added layer of complexity that comes with including these additional neuromodulator trials, which we again believe points to the difficulty in studying this patient population.
As our study was nonrandomized, with neuromodulator selection based on decision making employed by the senior author in routine clinical practice ( Figure 1 ), we do acknowledge the possible influence of selection bias on our reported outcomes. This precluded us from performing an intergroup analysis between gabapentin and tricyclic antidepressant groups. Despite these limitations, we believe that our study, a prospective analysis on the 2 primary neuromodulator classes used to treat UCC, provides valuable insight for clinicians. Our study demonstrates that the majority of patients with UCC who experience benefit with a neuromodulator have moderate to large clinically important improvements in cough control (as demonstrated by LCQ scores) in the short term. While robust responses to treatment are seen at 6 months, they are sparsely observed, as the majority of patients either develop tachyphylaxis to treatment or become intolerant of side effects. This study comes as gains in our understanding of the pathophysiology underlying UCC provides new drug targets, such as the P2X purinoceptor 3, which has a chiefly peripheral site of action.17,33,34 While the inhibitor was effective at reducing coughing, it did not entirely resolve symptoms, likely from not addressing the central hypersensitivity seen among these patients.17,35 This is essentially the opposite of our findings with gabapentin and tricyclic antidepressants, which are believed to work centrally but not peripherally, explaining why few of our patients experienced complete resolution of their cough. Clearly, future therapeutic interventions are warranted that address peripheral and central sensory changes, either with new drugs or dual treatments (eg, gabapentin + P2X purinoceptor 3 inhibitor).
Conclusion
While tricyclic antidepressants demonstrated short-term efficacy, the majority of patients did not complete 6 months of treatment. Tachyphylaxis was a clinically important finding observed in both drug classes. Percentage improvement scores appear effective at capturing subjective improvement with chronic cough treatment. Investigations of treatment therapies are warranted that address peripheral and central sensory pathways involved in UCC.
Author Contributions
Disclosures
Supplemental Material
OTO768517_suppl_mat – Supplemental material for Short- and Long-term Effects of Neuromodulators for Unexplained Chronic Cough
Supplemental material, OTO768517_suppl_mat for Short- and Long-term Effects of Neuromodulators for Unexplained Chronic Cough by Andrew Jay Bowen, Amy S. Nowacki, Kevin Contrera, Douglas Trask, James Kaltenbach, Claudio F. Milstein, Michelle Adessa, Michael S. Benninger, Rachel Taliercio and Paul C. Bryson in Otolaryngology–Head and Neck Surgery
Footnotes
Acknowledgements
Nurses Nina Chalhoub, Michelle Merriman, and Khalilah Thomas for their assistance in obtaining LCQ in laryngology clinic.
This article was presented at the 2017 AAO-HNSF Annual Meeting & OTO Experience; September 10-13, 2017; Chicago, Illinois.
No sponsorships or competing interests have been disclosed for this article.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.