
Abstract
Objective
To compare the outcomes of epidermal growth factor (EGF) and gelatin sponge patch treatments for traumatic tympanic membrane perforations.
Study Design
Prospective, randomized, controlled.
Setting
University-affiliated teaching hospital.
Subjects and Methods
In total, 141 perforations encompassing >50% of the eardrum were randomly divided into 3 groups: EGF (n = 47), gelatin sponge patch (n = 47), and observation (n = 47). The edges of the perforations were not approximated. The closure rate, mean closure time, and infection rate were evaluated at 6 months and the related factors analyzed.
Results
A total of 135 perforations were analyzed. At 6 months, the closure rates were 97.8%, 86.7%, and 82.2% in the EGF, gelatin sponge patch, and spontaneous healing groups, respectively (P = .054). The mean ± SD closure time was 11.12 ± 4.60, 13.67 ± 5.37, and 25.65 ± 13.32 days in the EGF, gelatin sponge patch, and spontaneous healing groups, respectively (P < .001). In addition, the presence of infection was not significantly associated with rate of closure in any group.
Conclusions
As compared with spontaneous healing, daily application of EGF and gelatin sponge patching reduced the closure time of traumatic tympanic membrane perforations. EGF treatment had a higher closure rate and shorter closure time but resulted in otorrhea. By contrast, gelatin sponge patches did not improve the closure rate or cause otorrhea but required repeated patch removal and reapplication. Thus, the appropriate treatment should be selected according to patient need.
Keywords
Although traumatic tympanic membrane perforations (TMPs) tend to heal spontaneously, most large TMPs have a healing time of approximately 3 to 12 weeks or longer.1,2 TMP may result in residual tinnitus, aural fullness, and conductive hearing loss, thereby affecting the patient’s quality of life. Most patients with large TMPs seek noninvasive treatment to reduce the closure time and quickly improve the associated annoying symptoms. Treatment recommended by the otologist may include patching with biological materials and the topical application of growth factors.3-6 In the otology clinic, a gelatin sponge is the biological material most commonly used to treat traumatic TMPs and chronic dry small perforations.7,8 Epidermal growth factor (EGF) and fibroblast growth factor 2 (FGF2) are the growth factors most commonly used to repair TMPs.3,9,10 EGF stimulates the proliferation of epithelial cells and keratinocytes, while FGF2 induces fibroblast proliferation and revascularization. 11 TMPs are first closed by proliferation of epithelial cells and keratin aggregation, followed by proliferation of fibrous layers.12,13 Santa Maria et al 14 reported that EGF promotes tympanic membrane healing by stimulating keratinocyte proliferation and migration. Thus, EGF preparations are widely used to repair TMPs.3,9,14-16 The safety and efficacy of EGF in the ear have been demonstrated; EGF has no apparent risk of ototoxicity if applied topically to the external and middle ears of animals and humans,3,9,15,16 although large doses may increase the risks of otorrhea and ear discomfort. 17 EGF and gelatin sponge patches are readily available, simple, convenient, and inexpensive. However, to our knowledge, there has been no clinical comparative study of the efficacy of EGF versus gelatin sponge patches in human traumatic TMPs. Thus, we compared the efficacy of gelatin sponge patches and EGF among patients with large traumatic TMPs.
Materials and Methods
This study was reviewed and approved by the Institutional Ethics Review Board of the Wenzhou Medical University of Yiwu Hospital, China. All work was performed in compliance with the Helsinki Declaration. Written informed consent was obtained from all participants.
Subjects were recruited consecutively from patients diagnosed with traumatic TMPs who visited the Department of Otorhinolaryngology–Head and Neck Surgery at the Yiwu Hospital of Wenzhou Medical University between January 2015 and June 2017. The inclusion criteria were as follows: a traumatic TMP, age >16 years, and perforation of at least 50% of the pars tensa. The exclusion criteria were as follows: middle ear infection or severe vertigo at the time of the hospital visit, suspicion of ossicular chain damage or granulation tissue hyperplasia, an additional injury associated with the inability to walk independently (craniocerebral injury in particular), and patient relocation from the region served by our hospital (associated with loss to follow-up).
Age, sex, date of injury, cause of injury, size of the TMP, and presence or absence of otorrhea were recorded at the time of each hospital visit. Each patient was endoscopically examined after cerumen and/or blood clots in the external auditory canal (EAC) were removed with a cotton bud soaked in povidone-iodine solution, and the site and size of the perforation were documented.
The sizes of TMPs were analyzed with ImageJ software (National Institutes of Health, Bethesda, Maryland), and perforation size was graded into large and subtotal perforation (>50% and 75% of the eardrum, respectively). As healing of the perforation is typically associated with successful closure of the air-bone gap,1,7 audiometric examinations were not performed.
The principal investigator, aided by a registered nurse, allocated patients to various treatments with simple random sampling. Specifically, consecutive subjects who met the inclusion criteria and signed the consent form were assigned random numbers generated by SPSS 19.0 for Windows (IBM, Chicago, Illinois), which allocated them to 1 of 3 groups: EGF (n = 47), gelatin sponge patch (n = 47), or observation (n = 47). The closure rate, infection rate, and mean closure time were evaluated at 6 months, and the following were analyzed for their influence on healing outcome: sex, side of the ear, position of the perforation, cause of the injury, size of the perforation, preexisting myringosclerosis, inverted edge, age, duration of perforation, and infection.
Technical Methods
EGF-Treated Group
The EAC was cleaned with a cotton swab soaked in povidone-iodine solution. Two to 3 drops (0.1-0.15 mL) of recombinant human EGF solution (200 mL/20 g; Warnoway gen Pharmaceutical Co, Ltd, Guilin, China) were applied directly to the tympanic membrane once daily to keep the eardrum moist. The edge of the perforation was not approximated, and no scaffolding material was used. In all patients, the eardrops were applied daily at home.
Gelatin Sponge Patch Group
The EAC was cleaned with a cotton bud soaked in povidone-iodine solution. A modified compressed gelatin sponge sheet, larger than the perforation, was soaked in 0.5% (w/v) chlortetracycline ointment and placed onto the tympanic membrane remnant (ie, an onlay technique) to completely cover the perforated area with margins of at least 2 mm. No eardrops were prescribed, and the EAC was not packed. The edges of the perforation were not approximated.
Observation Group
No intervention was offered, but all patients underwent regular follow-up.
Follow-up
The first follow-up was scheduled for 2 to 3 days after the initiation of treatment. We confirmed that all patients in the EGF group self-applied their drops correctly, and we carefully adjusted eardrop dosages to ensure that the eardrum surface remained moist (ie, neither dry nor overly wet). Any inappropriate patient technique was corrected. Thereafter, follow-up was scheduled at least weekly until complete closure of the perforation was achieved or for up to 6 months. Patients were advised to reduce the number of ear drops and to take oral amoxicillin (with or without application of ofloxacin drops) if purulent otorrhea developed. In the gelatin sponge group, the sponge was removed, and a fresh piece of sponge was placed onto the tympanic membrane at each visit. The tympanic membrane was repeatedly examined endoscopically, and color photographs were obtained by an independent blinded clinician at all follow-up visits. Infection was defined as the presence of purulent otorrhea in the EAC or middle ear on clinician examination. The presence of limpid water otorrhea was not classified as an infection.
Statistical Analyses
To calculate the required sample size, the study was powered at 80%, and a type I error of 5% was assumed (α = 0.05, β = 0.20, power: 1 − 0.2 = 0.8). A 15% difference in closure rate among the treatment groups was predicted. The group ratio was 1:1:1; as such, 44 patients were needed per group according to PASS 11.0 software (NCSS Statistical Software, Kaysville, Utah). Assuming a loss of 5%, the number of patients needed per group was 47, giving a total of 141 patients.
All statistical analyses were performed with SPSS 19.0 for Windows. Results are presented as mean ± SD or percentage. We assessed the normality of continuous variables using the Kolmogorov-Smirnov test; normality was considered present if the P value was >.05. Between-group differences were compared by 1-way analysis of variance when the data were normally distributed. Post hoc comparisons among groups were performed with the Bonferroni least significant difference test for homoscedasticity and Dunnett’s T3 test for heteroscedasticity. If the data were not normally distributed, the overall difference was evaluated by Kruskal-Wallis 1-way analysis of variance, and between-group differences were assessed by the Mann-Whitney U test. Correlations between 2 continuous variables were evaluated by Pearson correlation analysis, and chi-square test was used to compare the groups in terms of closure rate, sex, and so on. In post hoc multiple comparisons, P = .0167 (0.05 / 3) was regarded as being indicative of a significant difference. Otherwise, a value of P < .05 was taken to reflect statistical significance.
Results
Demographic Characteristics
A total of 141 patients met the exclusion criteria. Two patients in each group were lost to follow-up ( Figure 1 ). Thus, 135 patients (65 men and 70 women) were analyzed. The left and right ears were affected in 40 and 95 patients, respectively. Each group comprised 45 patients. The mean ages were 35.04 ± 12.04, 34.53 ± 10.83, and 37.47 ± 11.28 years in the EGF, gelatin sponge patch, and spontaneous healing groups, respectively (P = .429). The mean duration of injury was 7.24 ± 14.13, 3.16 ± 2.56, and 3.67 ± 3.46 days in the EGF, gelatin sponge patch, and spontaneous healing groups, respectively (P = .187). Demographic data are shown in Table 1 . The sex ratio, age, side of the ear, cause of the injury, size of the perforation, duration of injury, and preexisting myringosclerosis were similar among the 3 groups.
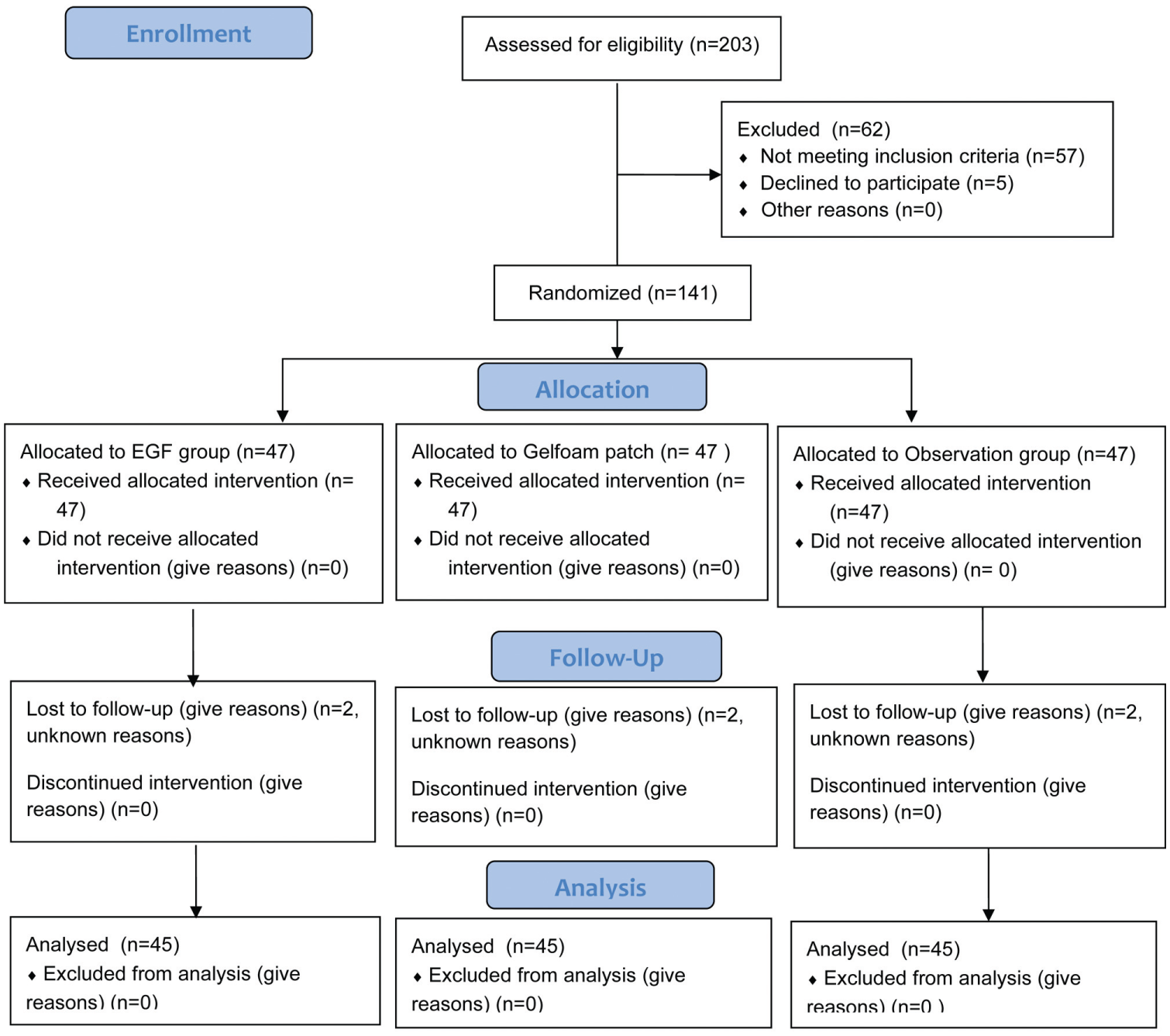
Enrollment, randomization, and follow-up of study participants. EGF, epidermal growth factor.
Demographic Data of EGF, Gelfoam Patching, and Spontaneous Healing Groups.
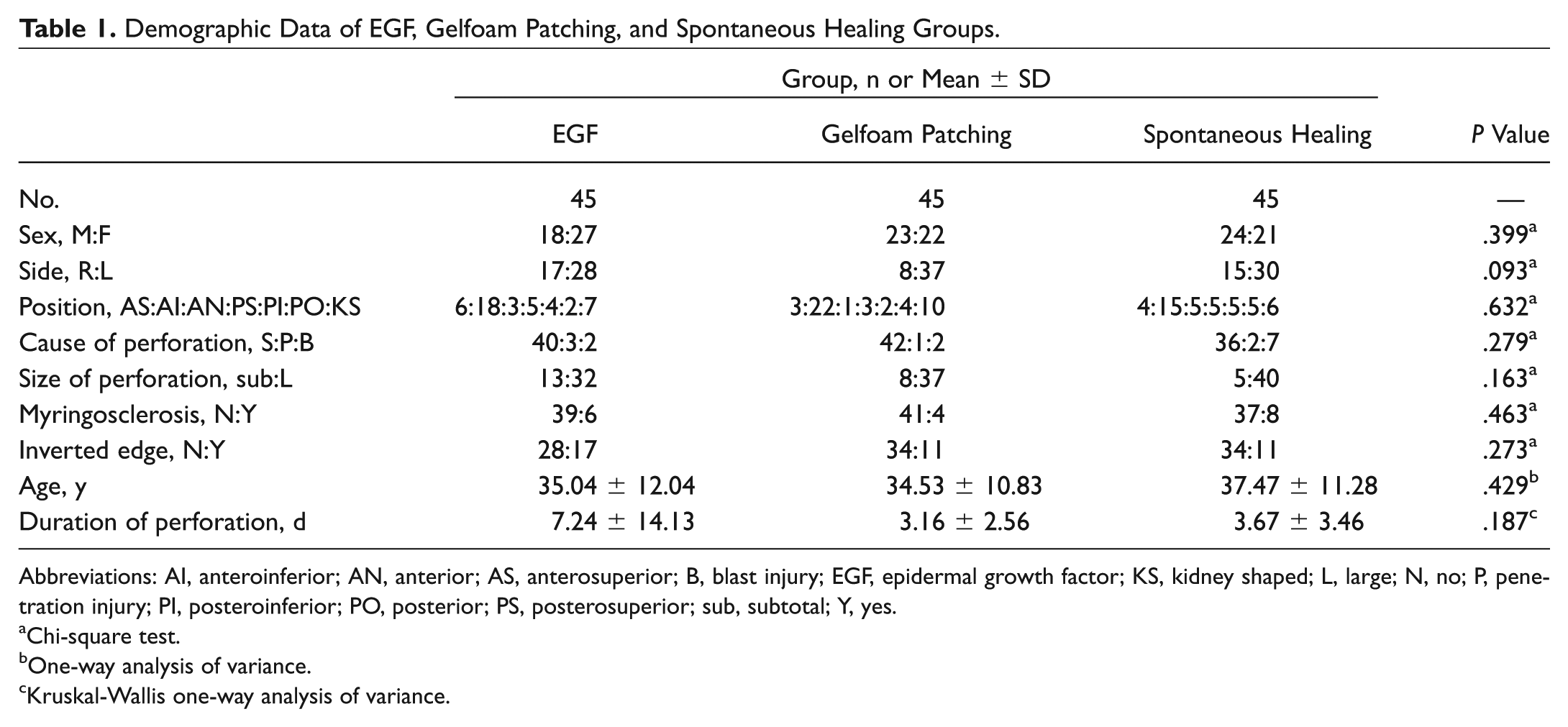
Abbreviations: AI, anteroinferior; AN, anterior; AS, anterosuperior; B, blast injury; EGF, epidermal growth factor; KS, kidney shaped; L, large; N, no; P, penetration injury; PI, posteroinferior; PO, posterior; PS, posterosuperior; sub, subtotal; Y, yes.
Chi-square test.
One-way analysis of variance.
Kruskal-Wallis one-way analysis of variance.
Healing Outcomes
The healing outcomes are shown in Table 2 and Figure 2 . The closure rates were 97.8%, 86.7%, and 82.2% in the EGF, gelatin sponge patch, and spontaneous healing groups, respectively (P = .054). The closure rate differed significantly between the EGF and spontaneous healing groups (P = .009) but not between the other 2 pairings (EGF vs gelatin sponge patch, P = .039; gelatin sponge patch vs spontaneous healing, P = .561). The mean closure time was 11.12 ± 4.60, 13.67 ± 5.37, and 25.65 ± 13.32 days in the EGF, gelatin sponge patch, and spontaneous healing groups, respectively (P < .001). The mean closure time differed significantly between the EGF and spontaneous healing groups (P < .001) and between the gelatin sponge patch and spontaneous healing groups (P < .001) but not between the EGF and gelatin sponge patch groups (P = .071). Figure 3 shows the healing process of 2 patients with a traumatic TMP treated with EGF.
Healing Outcome of EGF, Gelfoam Patching, and Spontaneous Healing Groups.
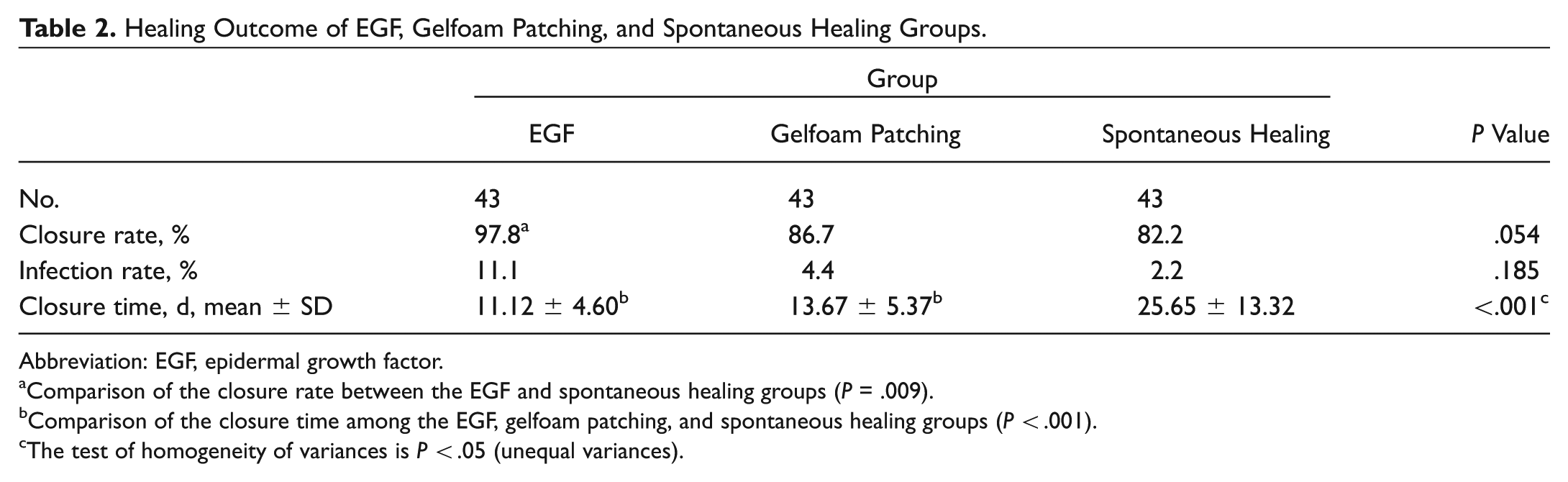
Abbreviation: EGF, epidermal growth factor.
Comparison of the closure rate between the EGF and spontaneous healing groups (P = .009).
Comparison of the closure time among the EGF, gelfoam patching, and spontaneous healing groups (P < .001).
The test of homogeneity of variances is P < .05 (unequal variances).
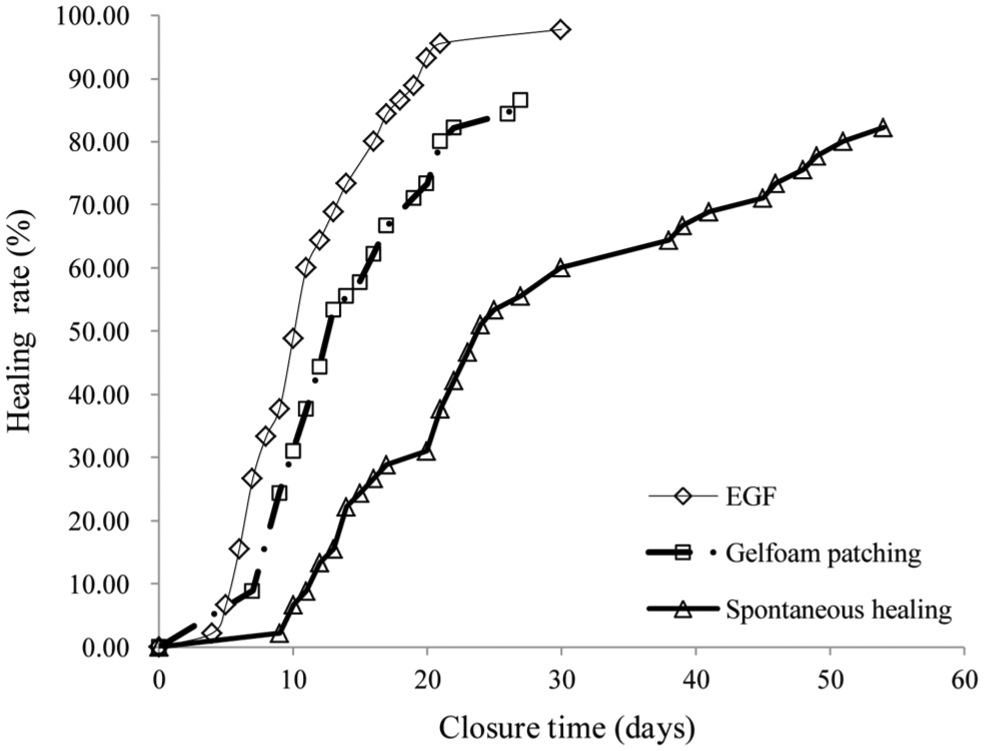
Kaplan-Meier curve of closure time–closure rate of tympanic membrane perforations by 3 groups. EGF, epidermal growth factor.
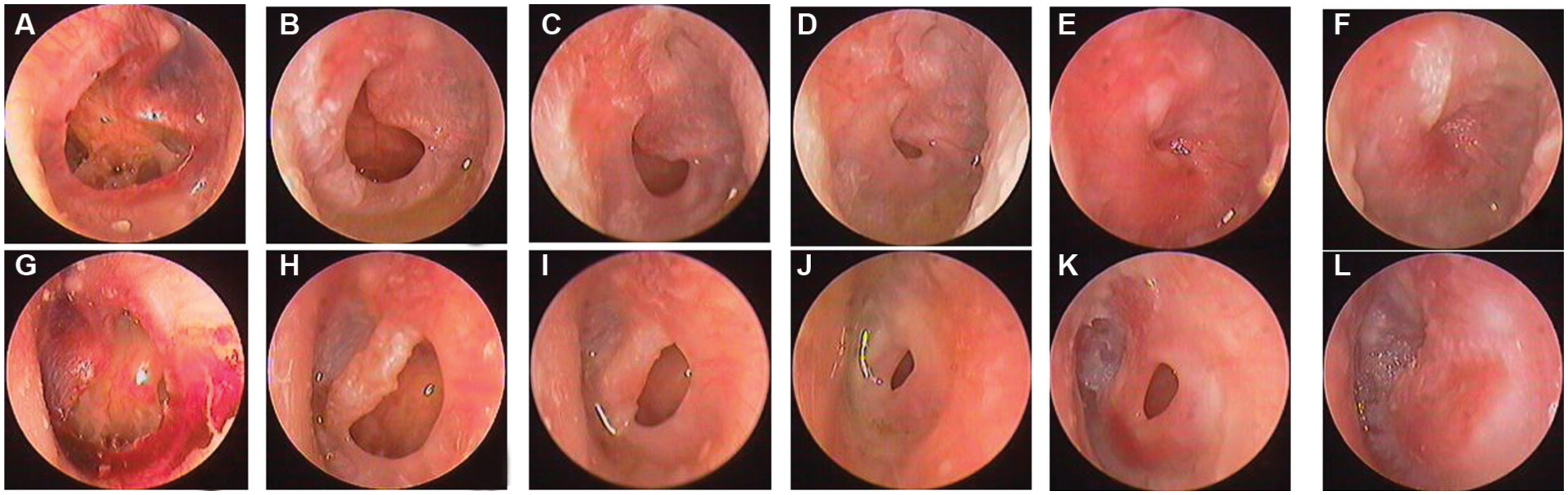
The healing process of a large perforation after topical application of epidermal growth factor for a 28-year-old man: (A) second day after perforation and (B) 7 days, (C) 10 days, (D) 14 days, (E) 17 days, and (F) 21 days after treatment. The healing process of a large perforation after topical application of epidermal growth factor for a 32-year-old woman: (G) first day after perforation and (H) 7 days, (I) 10 days, (J) 14 days, (K) 17 days, and (L) 21 days after treatment.
Factors Related to Healing and Complications
Table 3 shows the factors related to perforation closure. The closure rate was significantly correlated with sex and the side, position, and size of the perforation in the spontaneous healing group (P = .008, .007, .039, and .001, respectively) but not in the EGF or gelatin sponge patch group. In addition, infection, cause, preexisting myringosclerosis, inverted edge, age, and perforation duration were not significantly associated with the closure rate in any group.
Correlation Factors Analysis of Closure Rate of 3 Groups.
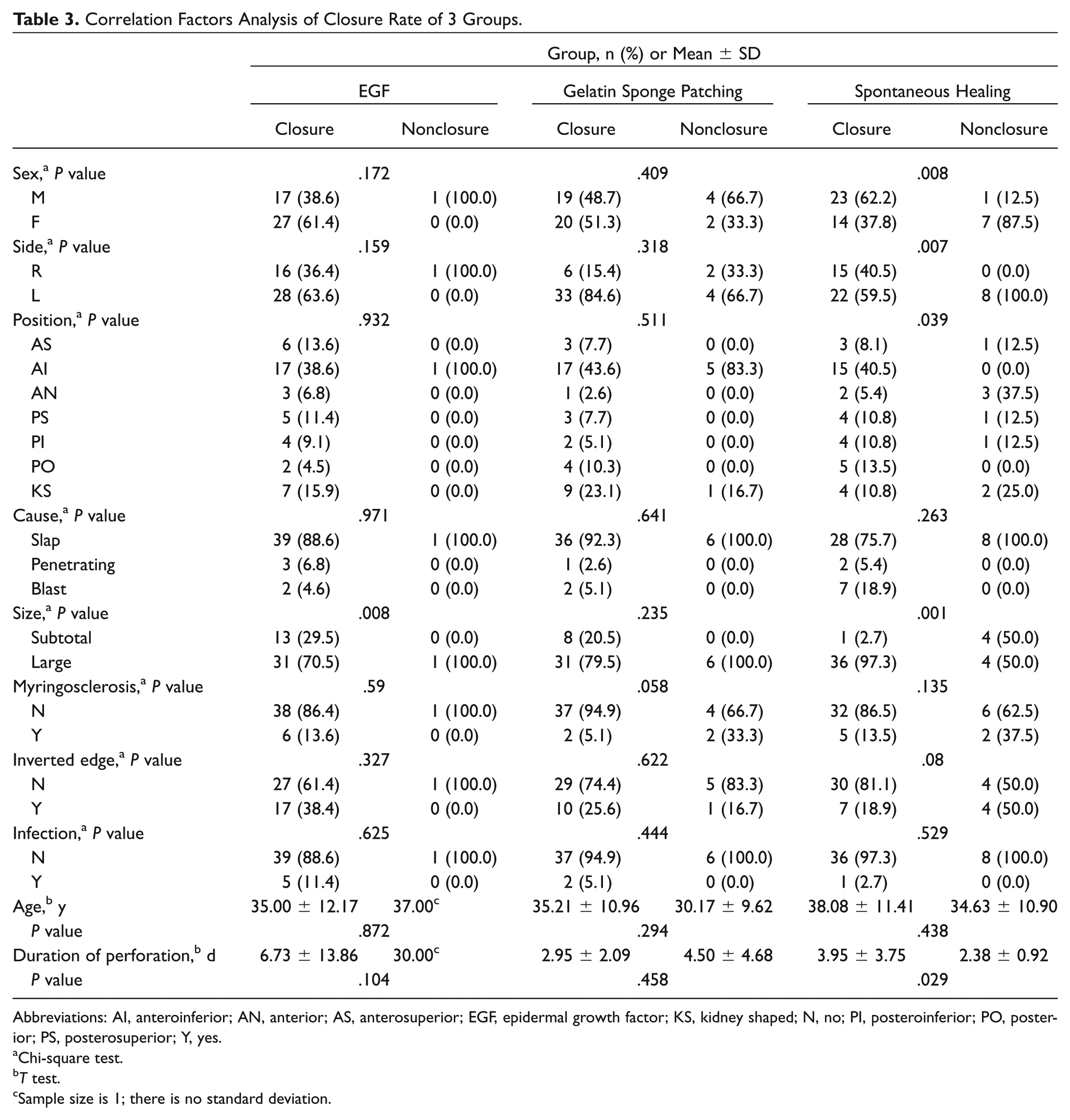
Abbreviations: AI, anteroinferior; AN, anterior; AS, anterosuperior; EGF, epidermal growth factor; KS, kidney shaped; N, no; PI, posteroinferior; PO, posterior; PS, posterosuperior; Y, yes.
Chi-square test.
T test.
Sample size is 1; there is no standard deviation.
Table 4 shows the factors related to perforation closure time. There was a significant correlation between the perforation position and closure time in the EGF group (P = .006) but not in the gelatin sponge patch and spontaneous healing group (P = .195 and .714, respectively). The correlation between perforation size and closure time was significant in the EGF and gelatin sponge patch groups (both P = .002), as was the correlation between infection and closure time in the EGF group (P < .001). By contrast, the latter relationship was not significant in the gelatin sponge patch and spontaneous healing group (P = .825 and .902, respectively). The number of subtotal perforations was very small (n = 5), and only 20% of perforations achieved closure in the spontaneous healing group, which prevented statistical analysis of the influence of perforation size on the spontaneous healing time. No other variable was significantly associated with the mean closure time in any of group.
Correlation Factors Analysis of Closure Time (Days) of 3 Groups.
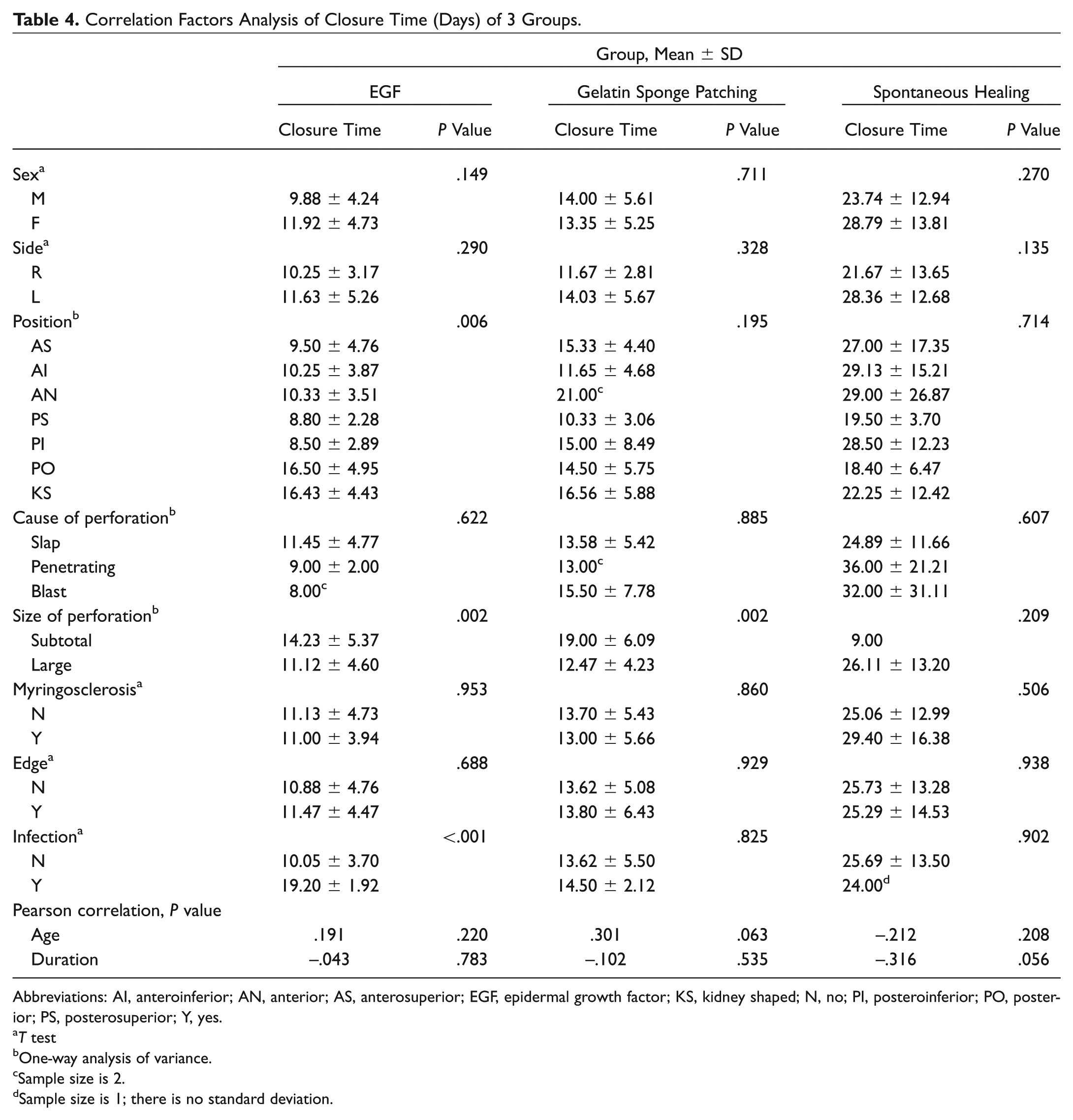
Abbreviations: AI, anteroinferior; AN, anterior; AS, anterosuperior; EGF, epidermal growth factor; KS, kidney shaped; N, no; PI, posteroinferior; PO, posterior; PS, posterosuperior; Y, yes.
T test
One-way analysis of variance.
Sample size is 2.
Sample size is 1; there is no standard deviation.
Complications
The infection rates were 11.1% (5 of 43), 4.4% (2 of 43), and 2.2% (1 of 43) in the EGF, gelatin sponge patch, and spontaneous healing groups, respectively (P = .185; Table 2 ). In pairwise comparisons, the differences were not significant (EGF vs gelatin sponge patch, P = .231; EGF vs spontaneous healing, P = .078; gelatin sponge patch vs spontaneous healing, P = .553). Local pain, dizziness, and hyperplasia of EAC were not seen in either the EGF or gelatin sponge patch group. No middle ear cholesteatoma occurred in any of the groups during follow-up.
Discussion
Traumatic TMPs are common otologic emergencies, particularly in developing countries. Traumatic TMPs have a high spontaneous healing rate; thus, observation is usually recommended.1,18,19 However, the spontaneous healing time of most large traumatic TMPs is typically longer.1,2,18,19 With improved economic conditions and quality of life, almost all patients with traumatic TMPs are able to seek medical attention to close the perforation and thus quickly eliminate the troublesome symptoms of tinnitus and aural fullness.
EGF, a 53–amino acid mitogenic polypeptide present in many mammalian species, is one of several growth factors being investigated for its potential to expedite the healing process. EGF had been used to accelerate the healing of TMPs.9,20,21 In this study, daily topical application of EGF improved the closure rate and reduced the closure time as compared with spontaneous healing but not gelatin sponge patching, possibly due to the small sample size. In this study, the closure rate was 97.8% in the EGF group and 86.7% in the gelatin sponge patch group. The difference in the closure rate between the EGF and gelatin sponge patch groups was 11.1%; that between the EGF and spontaneous healing groups, 15.6%; and that between the gelatin sponge patch and spontaneous healing groups, 4.5%. Biomaterial patching reportedly reduces the closure time but does not increase the closure rate.4,7,15 Thus, recruitment of a larger number of patients may have resulted in a significant difference between the EGF and gelatin sponge patch groups.
The difference in the mean closure time between the EGF and gelatin sponge patch groups was very small, which could be related to the particular properties of these biomaterials. Previous studies suggested that the outward migration of the epithelium and excessive epithelialization may prolong or impede perforation healing.22,23 Gelatin sponge patches provide a scaffold for migration of the epithelium and promote the proliferation of granulation tissue and edema of the epithelial layer at the perforation edge, thereby accelerating TMP closure.7,24 Topical application of exogenous EGF stimulates keratin aggregation in the epithelial corneum and the proliferation of epithelial cells (the stratum corneum is the first layer of the perforation to close 12 ), thereby facilitating healing of the eardrum. Clinical and experimental studies showed that the moist environment provided by ofloxacin ear drops aids eardrum healing17,25-27; however, an experimental study showed that the closure rate of TMPs was higher in an EGF treatment group than in a control saline group (81% vs 25%). 28 Thus, although another randomized experimental arm of patients receiving non-EGF drops was not included in this study, we believed that the effect of EGF on a TMP may well depend on the biological efficacy of the EGF preparation, excluding the effect on eardrum healing of the moist environment provided by the drops.
Single topical application of EGF or FGF2 facilitates healing of the eardrum.3,10,14,17,26,29 However, the 2 growth factors differ in their degree of selectivity, as EGF is very effective in epithelial cells and FGF2 in fibroblasts and vascular endothelial cells.11,30 Theoretically, TMP repair should be faster for patients treated with EGF than with FGF. In an experimental study, the closure rate of large TMPs was lower in the FGF2 group than in the EGF group. 31 However, our clinical studies showed a lower closure rate in the EGF group, although the difference versus the FGF2 group was not significant.17,29 In clinical studies, the sample size, the dose and application frequency of the growth factor, the correct versus incorrect use of ear drops, and the frequency of follow-up after treatment may affect assessments of the therapeutic effect. The incorrect use of ear drops would result in the too large or too small of dose of growth factor, thereby increase the chance of middle ear infection and prolong the healing time or the failure of healing. 17 The optimal dose and frequency of EGF for human TMPs are unclear. Given our experience, we chose a regimen of daily continuous application of 2 to 3 drops (0.1-0.15 mL) of EGF, which was sufficient keep the eardrum environment moist but not dry or watery. However, the optimal dose and frequency of EGF remain to be precisely determined. The safety and efficacy of EGF in the ear were demonstrated.3,9,15,16 Nonetheless, a higher dose of EGF may increase otorrhea and thus the risk of infection and ear discomfort. 17 Although the infection rate did not differ significantly among the 3 groups in this study, the EGF group had the highest infection rate. Interestingly, infection did not interfere with healing in the EGF group but only prolonged the closure time. In addition, local pain, dizziness, and EAC hyperplasia were not seen in the EGF or gelatin sponge patch group, nor did middle ear cholesteatoma develop in any of the patients during follow-up.
Several factors influence eardrum healing. In this study, we found significant correlations between the spontaneous healing rate and sex, as well as the side, position, and size of the perforation. Easier spontaneous healing tended to occur in males and in patients with right-side perforations, most likely because most patients preferred right-sided sleep, 32 which could increase blood flow to the right eardrum. In addition, most of the male patients were younger in observation group, and the spontaneous healing rate is inversely proportional to age. 1 However, the sample size of perforations at the different positions was smaller in the spontaneous healing group; as such, the correlation of spontaneous healing rate and position of the perforation requires further investigation with a large sample. In our study, the spontaneous healing rate of large perforations was 82.2%, which was higher than that reported in the literature.1,2,4 The reasons for this difference could include the following: first, of the 45 large perforations in the observation group, only 5 were subtotal perforations; second, the follow-up time in our study was longer (up to 6 months). Some authors reported a closure rates of 77.8% to 81.8% for large perforations within 3 months of follow-up.1,4,33 The closure rate of TMPs had an increasing trend with increasing follow-up duration. Jellinge et al 18 reported a closure rate of 100% for large perforations after 3 months. An inverted edge and preexisting myringosclerosis were reported to prolong the healing time or lead to healing failure.34,35 However, our findings were not in agreement with this. Camnitz and Bost 5 reported that inverted edges do not affect the healing of TMPs treated with paper patches. Perforation position significantly affected the mean closure time in the EGF group (P = .006) but not in the gelatin sponge patch or spontaneous healing group—perhaps because contact between the EGF solution and the perforations was insufficient, which would be overcome by application of a gelatin sponge patch. In addition, the mean closure time increased significantly with increasing perforation size in the EGF group (P = .002) and gelatin sponge patch group (P = .002). The number of subtotal perforations was very small (n = 5), and only 20% of perforations achieved closure in the spontaneous healing group, which prevented statistical analysis of the influence of perforation size on the spontaneous healing time.
Conclusion
Compared with spontaneous healing, daily application of EGF or gelatin sponge patches reduced the closure time of traumatic TMPs. EGF treatment had the highest closure rate and shortest closure time. Thus, daily application of EGF should be recommended for traumatic TMPs to ameliorate aural fullness and tinnitus and prevent failure of eardrum healing. In addition, EGF treatment is simple, convenient, inexpensive ($4), and noninvasive and can be performed on an outpatient basis. A clinical study to determine the optimum dosage and timing of EGF treatment for traumatic TMPs is warranted.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.