
Abstract
Objective
To describe how deductible health plans affect parental decision making for common pediatric otolaryngology operations.
Study Design
A cross-sectional survey study.
Setting
Tertiary care pediatric hospital.
Subjects and Methods
Caregivers of patients aged <18 years were surveyed to assess factors in decision making related to common otolaryngologic surgical procedures, including outpatient tympanostomy tubes and adenotonsillectomy, between July 2015 and June 2016. Children in foster care and those who underwent nonelective surgery were excluded. Decision-making factors were statistically analyzed with univariate and multivariate ordinal logistic regression.
Results
A total of 155 caregivers completed the survey. The median age of the patient at the time of the surgery was 3 years. Surgical procedures included tympanostomy tube placement (51%), adenotonsillectomy (37%), tympanostomy tube placement with adenotonsillectomy (10%), and other (2%). The mean ± SD annual deductible per child was $1870 ± $140, and the mean maximum out-of-pocket expense was $3833 ± $235. The odds of having the deductible or out-of-pocket expense affect surgical decision making was greater for those covered under a high-deductible health plan (odds ratio = 2.27; 95% CI, 1.25-4.12; P = .007).
Conclusion
High-deductible health plans and out-of-pocket expenses can influence parental decision making for common otolaryngology operations, such as tympanostomy tube placement and adenotonsillectomy. Future studies are needed to determine if such policies affect access to care in the pediatric population.
Escalating health care costs have led to consumer-directed insurance policies, including high-deductible health plans (HDHP). Such policies aim to reduce utilization and total medical costs by partially reallocating health care expenditures to patients and families. The number of employees covered by a HDHP in 2006 was 4% and increased to nearly 20% in 2013.1,2 Such cost-sharing plans can impose significant financial burden and jeopardize the provision of adequate care to vulnerable populations, particularly children. 3 Approximately 5 million individuals enrolled in a HDHP are <20 years old.1,2,4 Many families are attracted to a HDHP because of lower premiums, yet such plans can lead to greater total expenses for many commercially insured families due to out-of-pocket (OOP) costs. The increasing prevalence of a HDHP may create a financial burden for middle- and lower-income families. 5 Lower-income families in a high-deductible health care plan may be more likely than higher-income families to have cost-related delays in care. 1 These findings lead to the concern that when faced with unmet high deductibles, many parents of pediatric patients may elect to forgo treatment that is considered highly effective.
Adenotonsillectomy and myringotomy with tube placement are the most common pediatric outpatient surgical procedures performed in the United States annually. 6 Adenotonsillectomy is the primary surgical treatment for sleep-disordered breathing among children and has been shown to lead to improvements in respiratory parameters and behavior.7,8 Delayed myringotomy with tympanostomy tube placement in children with persistent middle ear effusion may negatively affect learning and language development. 9 While previous research focused on parent experience and decision making in adenotonsillectomy 10 or tympanostomy tube surgery, 11 few studies specifically gauged how a family’s expenses affect parental decision making.
The present study investigates the impact of the recent proliferation of the HDHP on parental decision making for common pediatric otolaryngology surgical procedures. We aim to determine whether caregivers with high deductibles or OOP expenses are less likely to have their children undergo an operation as compared with families with lower deductibles. Our hypothesis is that children of families who belong to a HDHP will be more likely to delay or avoid common otolaryngology procedures.
Methods
This study was approved by the Institutional Review Board at Intermountain Healthcare and University of Utah. A cross-sectional study was performed in a multihospital network with a standardized accounting system. Patients <18 years old were identified who had undergone tympanostomy tube placement, adenoidectomy, tonsillectomy, and/or lingual tonsillectomy at a tertiary pediatric hospital between July 2015 and June 2016. We created the survey questions with input obtained from researchers experienced in survey design at the University of Utah Study Design and Biostatics Center. The survey included 5-point scale questions developed for caregivers to evaluate for factors in decision making related to their child’s surgery, as well as demographics and respondent-reported health plan costs. A cover letter was sent to the child’s caregiver who was responsible for health care decisions, and the survey was sent via email. Children in foster care and those who underwent nonelective surgery were excluded. Incomplete surveys were also excluded. The primary outcome variable was the extent to which the caregiver’s surgical decision making was affected by deductible health expenses.
A dichotomous variable was constructed whereby a HDHP was defined as being >$2600 based on 2016 Internal Revenue Service definition of the minimum annual for a family HDHP. 12 Those with a deductible amount <$2600 were defined as having a low-deductible health plan. Classification of self-reported income was based on findings published for Utah residents in the 2015 US Census Bureau 13 ; thus, the cohort was divided into 3 groups based on annual household income: low-income group (below the 2015 federal poverty level [FPL] of $24,250), intermediate-income group (between the 2015 FPL and median income for Utah, $62,912—which is 260% of the 2015 FPL), and high-income group (above the median income for Utah or 260% of the 2015 FPL).
Simple bivariate statistics were used for comparison of patient characteristics and survey responses to assess whether the respondents’ deductible or OOP influenced their decision toward surgery. For categorical variables, we used the chi-square or Fisher’s exact test, as appropriate. For ordered categorical variables, we used the Wilcoxon-Mann-Whitney test. We also used the Wilcoxon-Mann-Whitney test for our continuous variables, as each had a visibly skewed distribution. The study outcome was whether “deductibles and/or out-of-pocket expenses impact the medical decision making on whether or not to have surgery for my child” (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree). Given that the survey question was an ordered categorical scale, we fit an ordinal logistic regression to determine what factors influenced this outcome. This model provides an odds ratio that is interpreted as the odds of scoring higher on the 5-point scale for each 1-unit increase in the predictor variable. Statistical analysis was performed with Stata 15 (StataCorp, College Station, Texas).
Results
A survey was sent to the caregivers of 1340 patients who underwent surgery between July 2015 and June 2016. There were 163 respondents and 155 (11.5%) fully completed surveys. The median age of the patient at the time of the surgery was 3 years. The elective surgical procedures performed were tympanostomy tube placement (51%), adenotonsillectomy (37%), tympanostomy tube placement with adenotonsillectomy (10%), and a combination of tubes, adenoidectomy, or lingual tonsillectomy (2%). The mean ± SD household income was $84,193 ± $5815. The mean annual deductible per child was $1870 ± $140, and the mean maximum OOP expense was $3833 ± $235 per child. At the time of surgery, 112 (72%) had not yet met their deductible.
Table 1 provides the respondents’ attitudes toward the impact of having met the annual deductible on decision for surgery. While 59% reported that the deductible did not affect their decision to have surgery, 41% would have waited until their deductible was met or they had saved sufficient money before their child would have had surgery. Table 2 summarizes the results of the survey. There were 57 (37%) respondents covered under a HDHP. Overall, 64 (41%) respondents had a yearly household income of less than the median, and 9 (6%) had an income under the poverty level for Utah. Medical decision making by parents with less than the median income was more likely to be affected by the high deductible and OOP than by parents with greater than the median income (P = .01).
“If Your Child’s Annual Deductible Had Not Been Met, What Impact Would This Have on Your Decision for Surgery?” (n = 155).

“Deductibles and/or Out-of-Pocket Expenses Impact the Surgical Decision Making for My Child.” a
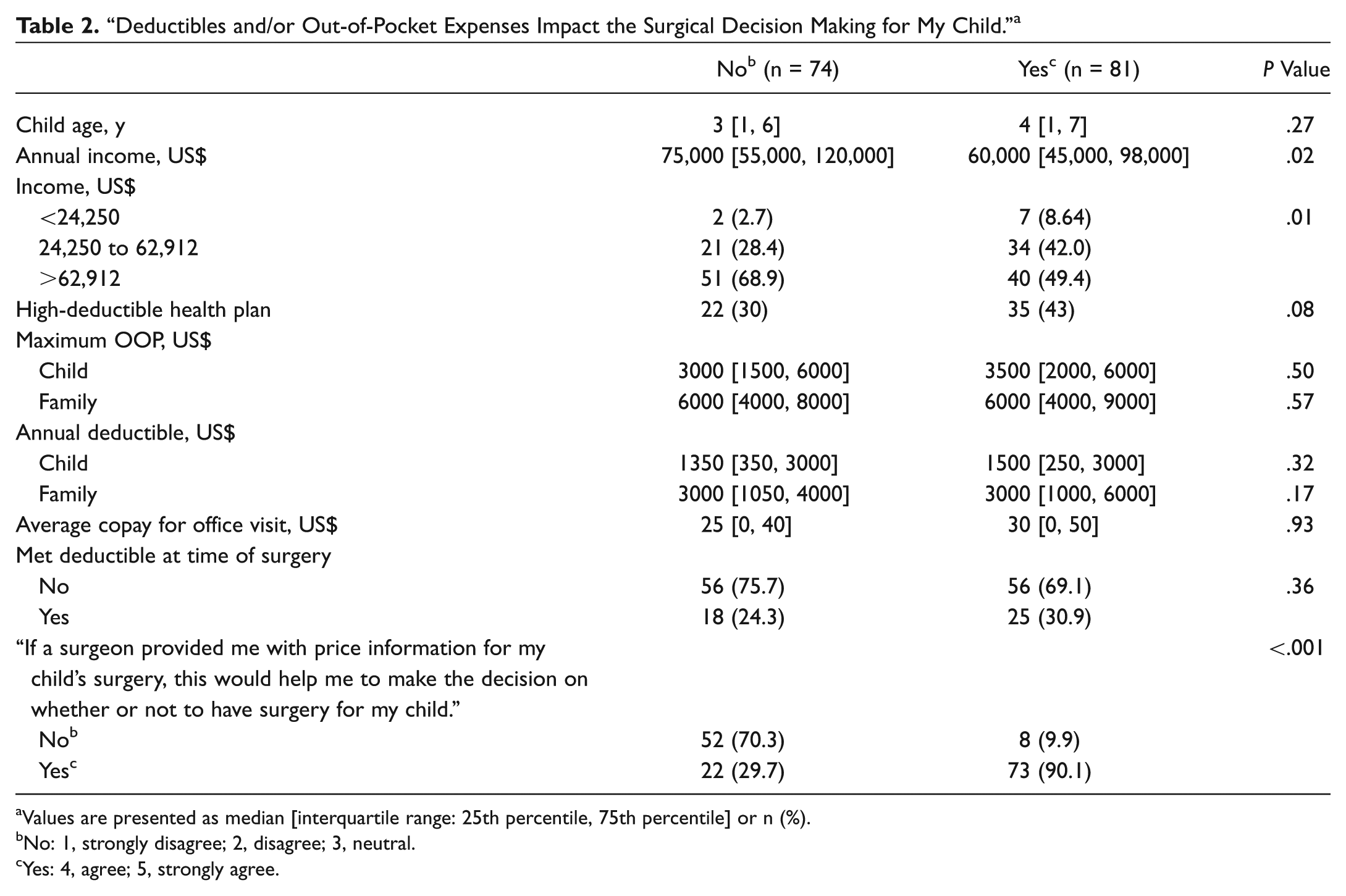
Values are presented as median [interquartile range: 25th percentile, 75th percentile] or n (%).
No: 1, strongly disagree; 2, disagree; 3, neutral.
Yes: 4, agree; 5, strongly agree.
Regression model results are displayed in Table 3 . The univariate results include 1 predictor variable per model, and the full multivariate model simultaneously includes all predictor variables in the table. The results are consistent with the multifactorial nature of the data in that many factors are simultaneously important to parents when considering whether to have or not have surgery for their child. When modeled as a single predictor, the factor cannot achieve statistical significance, as there exists too much residual variability in the outcome to isolate its effect. Only the strongest predictor, HDHP, was statistically significant, wherein it increased the impact on surgical decision making (odds ratio [OR] = 2.27; 95% CI, 1.25-4.12; P = .007). In the multivariate model, factors demonstrated to be important in decision making were coverage under a HDHP (adjusted OR = 2.42; 95% CI, 1.25-4.12; P = .007), meeting the deductible prior to surgery (adjusted OR = 1.94; 95% CI, 1.00-3.75; P = .047), and high-income category (adjusted OR = 0.21; 95% CI, 0.06-0.72; P = .01).
Univariate and Multivariate Ordinal Logistic Regression Model for the Outcome Variable Survey Question. a
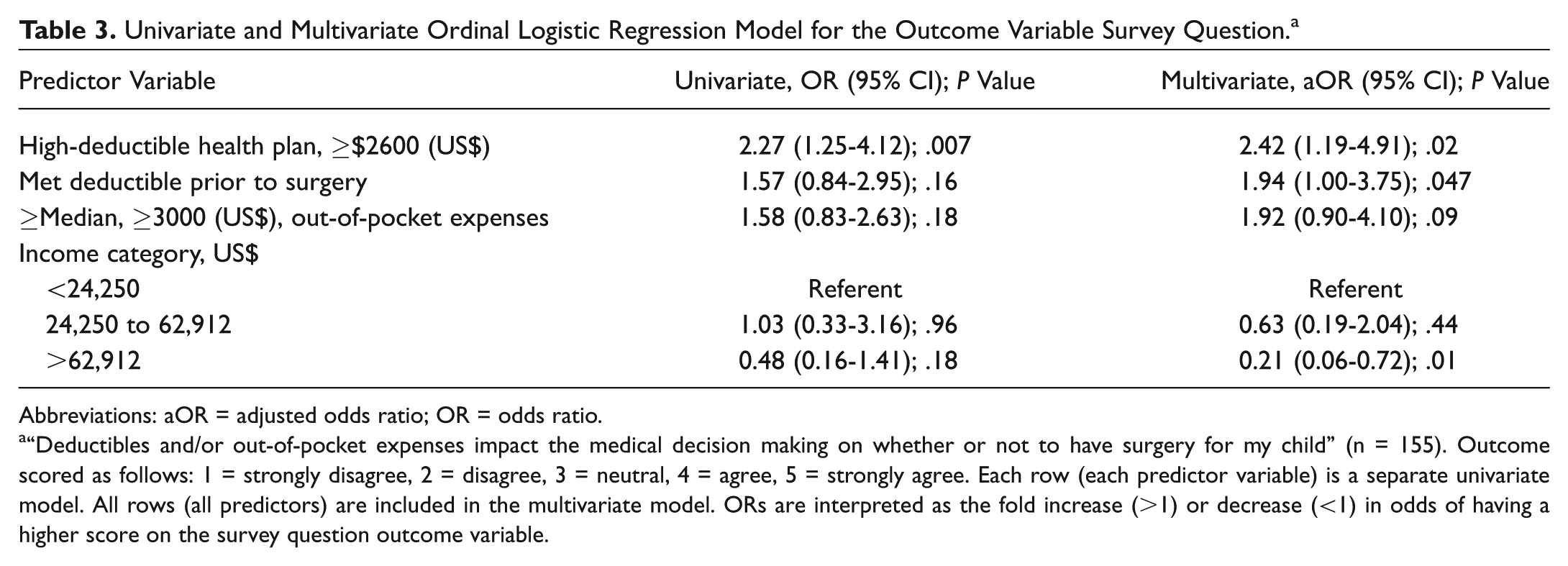
Abbreviations: aOR = adjusted odds ratio; OR = odds ratio.
“Deductibles and/or out-of-pocket expenses impact the medical decision making on whether or not to have surgery for my child” (n = 155). Outcome scored as follows: 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree. Each row (each predictor variable) is a separate univariate model. All rows (all predictors) are included in the multivariate model. ORs are interpreted as the fold increase (>1) or decrease (<1) in odds of having a higher score on the survey question outcome variable.
Discussion
HDHPs were designed with the goal to improve health care utilization and reduce total medical costs. Proponents of HDHPs argue that these policies help contain costs and make coverage more affordable by lowering premiums. 14 The classic RAND Health Insurance Experiment 15 showed that cost sharing in general had no adverse effect on participant health, except for differences seen in the sickest and poorest patients in several health domains. Since then, further research suggested that impoverished families are especially vulnerable to the effects of cost sharing.4,16 In our multivariate model, surgical decision making among families with incomes above the median was less affected by deductibles and OOP expenses. There are concerns that high-deductible policies place vulnerable populations at risk, particularly patients with chronic conditions, children, and families with medical debt.3,17,18
Increased cost sharing under HDHPs may worsen the quality of care and lead to unmet health care needs due to greater financial burden. 19 Our results suggest that high cost sharing affected surgical decision making by >2-fold for those families covered under a HDHP. Higher deductibles can lead to increased OOP expenses for common otolaryngology surgical procedures. Nearly a fourth of the respondents in our survey (23%) stated that if their family’s annual deductible had not been met, they would have waited on surgery until they could save enough money for surgery, and 16% stated that they would have waited on surgery until the deductible was met. These findings identify significant questions warranting future research. If parents decline or even delay surgery for the child due to financial reasons, how long do they delay the operation? Furthermore, what are the health outcomes and socioeconomic implications of this decision for the child and family? Waiting 3 to 4 months to proceed with tubes for a young child with hearing loss from chronic serous otitis media could lead to long-term speech delay. Likewise, delaying adenotonsillectomy for a child with severe obstructive sleep apnea poses potential adverse health risks.
Previous research showed that patients and physicians rarely discuss OOP costs during clinical visits. 20 Our survey demonstrated that 90% of respondents who were affected by high deductibles also reported that their decision making would be improved if surgeons provided the cost of the surgery, as compared with 30% of respondents not covered under a HDHP. For clinicians, it may be difficult to infer which pediatric patients are covered under a HDHP, which can create complexities in how clinicians approach counseling for patients based on insurance coverage. As cost sharing becomes more prevalent, it may be wise to discuss individual health plans and cost-sharing arrangements at the time of preoperative counseling. 4 This topic can initially be challenging and uncomfortable for physicians to address in the clinical setting but may nonetheless be an important part of the parent’s decision process. While professional fees may be easily accessible to the surgeon, facility fees and coinsurance coverage are not available. Lack of cost transparency and variation in contracting between health systems and third-party payers create significant barriers to informed decision making.
This study investigated the influence of health care policy on common otolaryngology surgical procedures, yet several questions remain to be answered. We divided families into specific income levels based on the FPL and median income in Utah. However, if families participate in a federal health insurance exchange, they are eligible for subsidies if their income is <250% of the FPL. Therefore, families with greater incomes may have higher OOP health care expenses and may be more affected by a HDHP than those receiving subsidies. Understanding how federal subsidies and individual family financial situations affect health care decision making is beyond the scope of this study but warrants further research.
An important limitation of the present study is the low survey response rate, for which there are likely several explanations. This was an email invitation sent after the child’s operation, with no incentive given for the family to complete the survey. Some respondents may not have understood the purpose of the survey and may have elected not to complete the questionnaire when asked about finances. Since the majority of respondents were Caucasian and 47% had less than a median household income for the state, there may have been a selection bias toward more affluent patients. We did not complete a demographic review of caregivers who did not respond, nor did we determine whether these children had comorbidities or special health needs. The samples were not randomized, limiting the generalizability of the findings to all populations. Last, there may have been a recall bias due to the 6 to 18 months elapsed between caregivers signing up for surgery and completing the survey. To minimize the recall period in future studies, the survey should be completed immediately before or at the time when parents make the decision to have surgery. Our data are limited to the subgroup of families in which their children had surgery, and they do not include respondents who decided to forego surgery. Therefore, our study essentially assessed the impact of HDHPs on families’ decision to proceed with surgery. We do not know how many patients did not undergo surgery because of HDHPs. Future studies should obtain a representative sample of caregivers who decided against surgery to determine why these caregivers may have declined surgery for their children.
The present study has the potential to shed light on the policy implication of increasing high cost-sharing health plans for children. The HDHP will likely continue to proliferate, and it is important to consider short- and long-term consequences on its patterns of use. A policy statement from the American Academy of Pediatrics suggested that certain essential and beneficial procedures normally provided by medical subspecialists be exempt from a HDHP, including appendectomy, reduction of fractures, and tympanostomy tubes. 1 If families are avoiding warranted procedures in the short term secondary to financial burdens under their HDHP, it is crucial to understand to what extent this phenomenon leads to long-term complications from delayed or unmet treatment.
Conclusion
This study demonstrates that a HDHP influenced parental decision making for common otolaryngology surgical procedures. Such expenditures may result in delays or avoidance of tympanostomy tube placement and adenotonsillectomy for children. Future studies are warranted to determine whether high cost-sharing policies effectively reduce health care utilization and create potential adverse health outcomes for vulnerable populations.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2017 AAO-HNSF Annual Meeting & OTO Experience; September 10-13, 2017; Chicago, Illinois.