
Abstract
Upper airway stimulation therapy (UAS) is a new option for treatment of obstructive sleep apnea (OSA) in patients unable to tolerate continuous positive airway pressure (CPAP). We set out to evaluate the effectiveness of UAS in patients who have undergone prior palate surgery. We designed a retrospective review and evaluated patients undergoing UAS at 2 academic centers. We recorded demographic and pre- and postoperative polysomnogram (PSG) data. We compared the cohort of patients who had undergone prior palate surgery, “prior surgery,” to the cohort who had not, “no prior surgery.” A total of 164 patients were included in the study: 23 in the prior surgery and 141 in the no prior surgery groups. The mean age was significantly higher in the no prior surgery group (P = .020). There were no other significant differences when comparing demographic, quality of life, or PSG variables between cohorts. UAS therapy is an option to treat OSA in patients having undergone unsuccessful prior palate surgery.
Keywords
Obstructive sleep apnea (OSA) is characterized by recurrent upper airway obstruction, leading to a disruption in ventilation and sleep architecture. Continuous positive airway pressure (CPAP) therapy has long been accepted as the primary treatment modality for OSA. However, despite our ability to customize CPAP, 46% to 83% of patients have been shown to be noncompliant with therapy. 1 With so many unable to use CPAP, additional treatment options have developed.
Most surgical therapies either remove tissue or alter the construct of the palate and tongue base to enlarge the airway and eliminate obstruction. Upper airway stimulation (UAS) is an alternative option that does not alter anatomy or remove native tissue. We hypothesize that UAS can be successful in patients who have undergone prior anatomy-altering palate surgery for OSA, but have not seen resolution of their symptoms or polysomnogram (PSG) variables.
Methods
After institutional review board approval, a retrospective review was designed at Thomas Jefferson University (TJU) and the Technical University of Munich (TUM). We included all patients undergoing UAS implantation from November 2014 to July 2017 who had their device activated and completed their postoperative titration PSG. The goal of our study was to assess the impact of prior palate surgery on the outcomes of UAS therapy.
We recorded demographic, prior surgery, and PSG data. We also calculated the percentage of patients reaching surgical success and postoperative apnea-hypopnea index (AHI) less 5. Surgical success was defined as a decline in postoperative AHI to less than 15 and normalization of the Epworth sleepiness score (ESS) to 9 or less.
We divided the population into 2 cohorts, those undergoing prior palate surgery (prior surgery) and those not undergoing prior surgery (no prior surgery). Prior palate surgery was considered any surgical procedure performed with the goal of treating OSA. Statistical analysis was performed using SPSS software version 24 (SPSS, Inc, an IBM Company, Chicago, Illinois). Our study end points included postoperative titration AHI, postoperative O2 nadir, postoperative ESS, surgical success, and rate of postoperative AHI less than 5. We performed an analysis of variance (ANOVA) comparing age, body mass index (BMI), preoperative AHI, preoperative O2 nadir, preoperative ESS, and our study end points between the prior surgery and no prior surgery groups. Lastly, we performed a linear regression model to evaluate the impact of demographic variables, prior surgery, and preoperative PSG data points on our study end points.
Results
During the study period, 164 UAS were performed, met inclusion criteria between the 2 institutions, and were included in this study: 81 were done at TJU and 83 at TUM. Twenty-three patients had undergone prior palate surgery for OSA (11 at TJU and 12 at TUM) and 141 had not.
Baseline information of the TJU and TUM cohorts, including BMI, preoperative PSG, and preoperative ESS outcomes, is shown in Table 1 .
Baseline and Outcome Data from Thomas Jefferson University (TJU) and Technical University of Munich (TUM) Cohorts. a
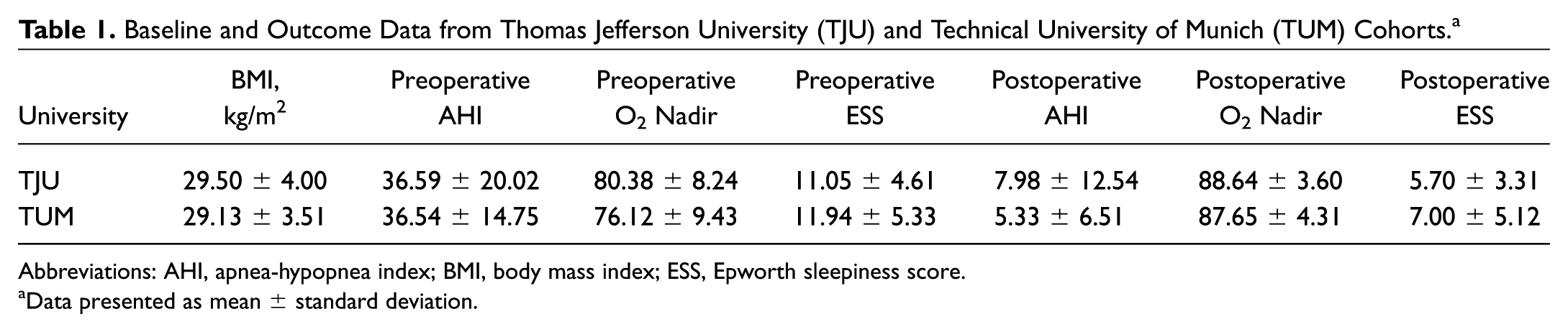
Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; ESS, Epworth sleepiness score.
Data presented as mean ± standard deviation.
Comparison of demographics, preoperative PSG data, and study end points between the 2 groups is shown in Table 2 . The mean age of the no prior surgery and prior surgery groups was 60.80 ± 11.55 years and 54.74 ± 10.17 years, respectively (P = .02). None of the other comparisons showed significant differences.
Comparison of Baseline Data Points and Study End Points between No Prior Surgery and Prior Surgery Groups Using Analysis of Variance.
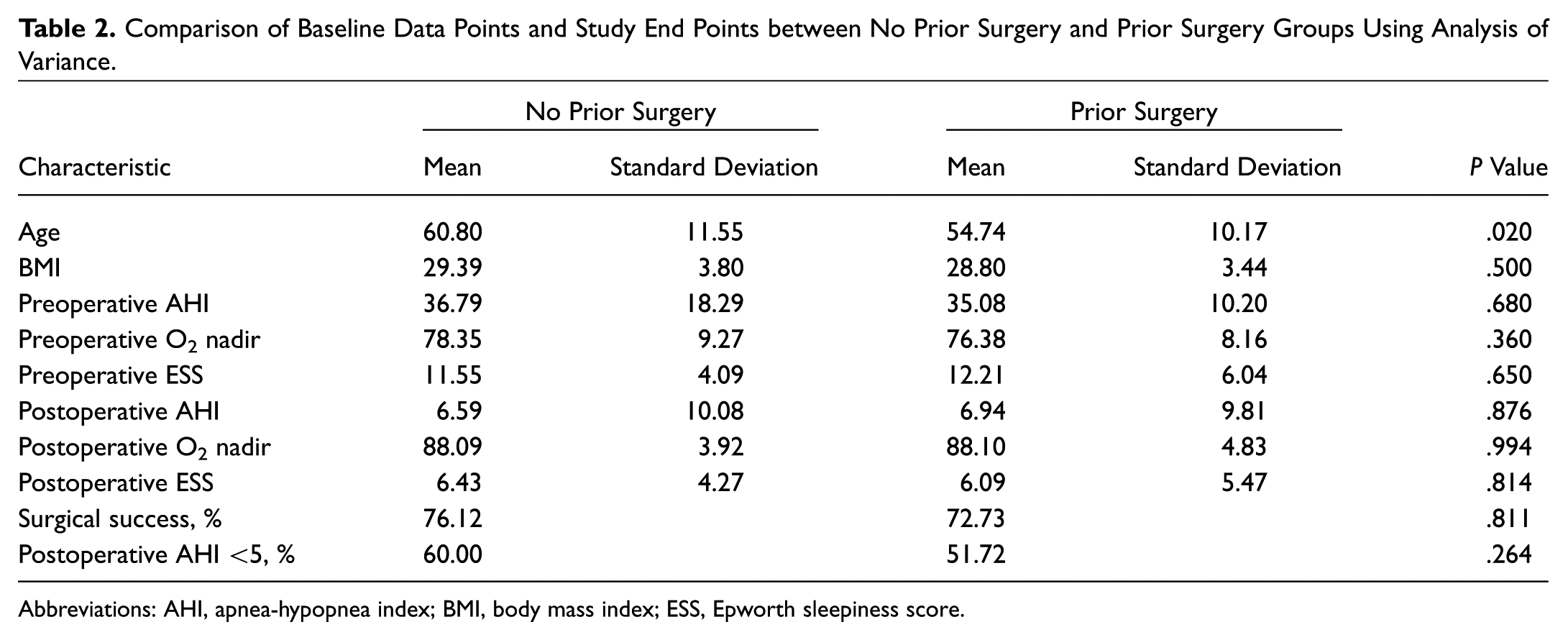
Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; ESS, Epworth sleepiness score.
The rate of surgical success and postoperative AHI less than 5 were 72.73% and 51.72%, respectively, in the prior surgery cohort. The rate of surgical success and postoperative AHI less than 5 were 76.12% and 60.28%, respectively, in the no prior surgery cohort. Neither were statistically different between groups.
We then created a linear regression model using age, BMI, prior surgery status, preoperative AHI, preoperative O2 nadir, and preoperative ESS as predictors of our study end points ( Table 3 ). None of these variables were significant predictors of our study end points.
Linear Regression Analysis Assessing Age, BMI, Prior Surgery, and Preoperative PSG Data as Predictors of Outcome Measures.
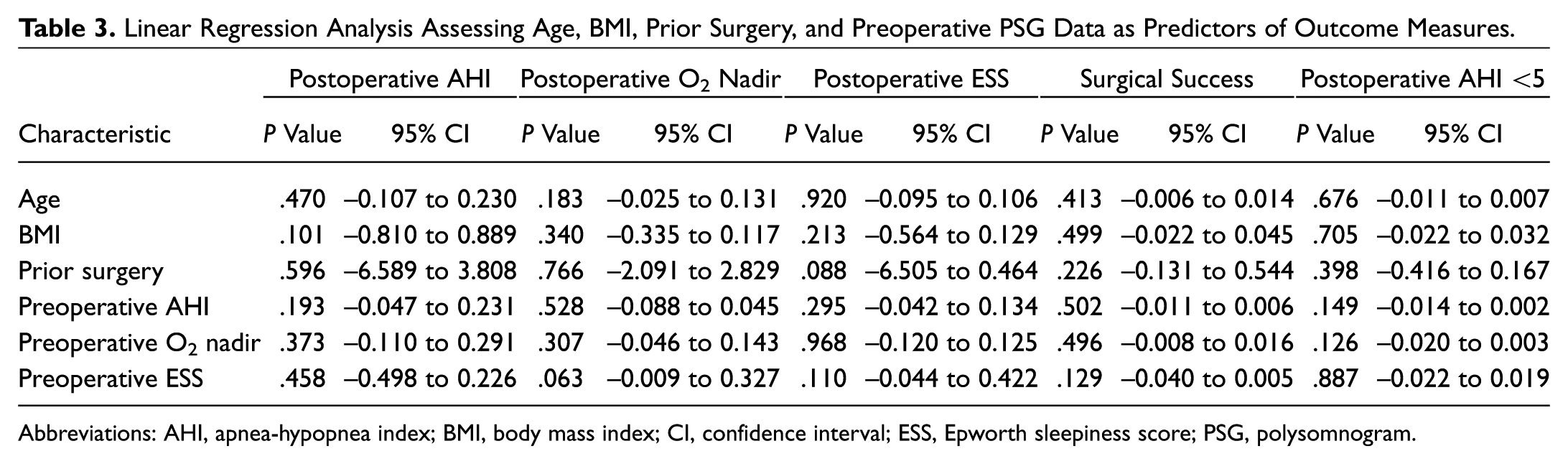
Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; CI, confidence interval; ESS, Epworth sleepiness score; PSG, polysomnogram.
Discussion
Traditional surgical alternatives to CPAP have included procedures that alter the native anatomy of the palate, tongue base, or facial skeletal framework. UAS is a novel functional surgical alternative that addresses multilevel airway collapse in OSA without altering native anatomy.2,3 For patients with moderate to severe OSA who are unable to tolerate CPAP and meet certain clinical inclusion criteria, UAS has delivered promising results. Reported surgical success rates for UAS have ranged from 66% to 96%.4-6 The stimulation therapy for apnea reduction (STAR) trial found an initial success rate of 66% at 12 months. 3 Follow-up studies at 18 and 36 months showed success rates of 64% and 74%.7,8
Patients who have undergone unsuccessful prior intervention for treatment of their OSA are seeking treatment options to alleviate their daytime symptoms and risk of comorbidity. Our multicenter study directly compares symptom and PSG measures between patients who had previously undergone palate surgery to address OSA and patients who had no prior OSA surgery prior to UAS. All postoperative outcome measures, including AHI, O2 nadir, ESS, and surgical success rates, were comparable between the 2 groups.
It is possible that postoperative changes from traditional sleep surgery, such as scarring of the palate, may have functional implications, limiting the effectiveness of UAS. However, our results support the hypothesis that UAS would perform well on patients who had received prior OSA surgery.
We recognize the limitations inherent in this study. Specifically, the study population of prior surgery patients is limited to only 23. In addition, the type and technique of prior OSA surgery vary within this group from patient to patient. This study represents an introductory, pilot analysis of this subset of patients being treated with UAS who have undergone prior palate surgery. Further analysis is required with a larger population to make a definitive conclusion.
Conclusion
Patients with persistent, moderate to severe OSA after prior OSA palate surgery can be treated with UAS provided they fit the standard inclusion criteria for the procedure.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2017 AAO-HNSF Annual Meeting and OTO Experience; September 10-13, 2017; Chicago, Illinois.