
Abstract
Objectives
Ultrasonography (US) is a reliable tool for the preoperative localization of parathyroid adenomas (PTAs). The aim of this study was to evaluate the accuracy of US for estimating both the size and the location of PTAs and the effect of operator expertise.
Study Design
Retrospective cohort study.
Setting
A single tertiary medical center.
Subjects and Methods
All patients who underwent parathyroidectomy for primary hyperparathyroidism between 1996 and 2012 were included. The estimated PTA localization and size by preoperative ultrasound were compared with the intraoperative findings and pathology report.
Results
The cohort included 410 patients. US correctly localized the adenoma in 76% of cases with a sensitivity of 76.2% and a positive predictive value of 86.8%. Measurements were least accurate for adenomas measuring <1 cm in diameter (24%). Scans made by a single senior operator specializing in the neck had a higher accuracy rate than scans made by multiple operators, with a significant difference for small adenomas (P < .001).
Conclusions
US is an accurate and sensitive tool for evaluating PTA size and location. Neck US is less accurate for small adenomas (<1 cm). In these cases particularly, the experience and expertise of the US operator may play an important role.
Parathyroidectomy is the treatment of choice for primary hyperparathyroidism (PHPT). 1 Over the past few decades, with the development of preoperative localization techniques and intraoperative parathyroid hormone monitoring, minimally invasive parathyroidectomy has gradually replaced the standard procedure with bilateral neck exploration. 2 Since most cases (85%-87%) of hyperparathyroidism are caused by a single parathyroid adenoma, accurate preoperative localization (using both ultrasonography and technetium sestamibi scintigraphy) allows the surgeon to perform a focused unilateral neck exploration.3,4 Other imaging modalities, such as computed tomography (CT) and magnetic resonance imaging (MRI), are acceptable preoperative evaluation in some medical facilities but less available in our medical center.
Ultrasonography (US) is noninvasive, relatively inexpensive, and less time-consuming than other localization tests for parathyroid adenoma (PTA). The first detection of a PTA by US was described in 1979. 5 Early studies reported variable sensitivity rates of 20% 6 to 92%7-11 for PTA localization, depending on operator skill and experience. More recent studies on the use of US as a primary screening modality in parathyroid disease reported sensitivity rates of 72% to 89%, similar to that of methoxyisobutylisonitrile (MIBI) scan.12-15 An increasing number of surgeons have also begun performing their own US evaluation prior to surgery. Studies evaluating the accuracy of a surgeon-operated US have demonstrated a sensitivity of up to 87%,16,17 independent of operator variability.
However, all the studies performed to date focused on the ability of US to correctly identify the location of PTAs, with no reference to its ability to accurately measure adenoma size. This information is valuable to the surgeon since accurate preoperative evaluation of adenoma location and size grants the surgeon a clear vision of the adenoma to assist him or her during the surgery and hence might shorten the duration of surgery and decrease the need for cervical exploration. The aim of the present study was to compare the estimated PTA size and location by preoperative US with the intraoperative findings and the final pathology report. We also evaluated the effect of US operator expertise and experience on US accuracy.
Methods
The database of a tertiary medical center was retrospectively searched for all patients with primary hyperparathyroidism treated by parathyroidectomy between 1996 and 2012. We included only patients in whom a solitary PTA was confirmed by postoperative permanent histological section. Exclusion criteria were absence of postoperative histopathological confirmation, findings of a double adenoma, multiglandular hyperplasia, and patients with recurrent or persistent disease in which double adenoma or hyperplasia was discovered during follow-up. Patients with insufficient data in the medical records, including US report or pathology documentation of adenoma size, were excluded as well. The study protocol has been approved by the Rabin Medical Center Institutional Review Board.
It is our departmental policy to perform focused surgery when parathyroid adenomas are identified preoperatively by US and MIBI. These studies are performed by specialized radiologists at various centers prior to patient referral to our medical center. If either or both modalities fail to localize the adenoma or the studies are not in concordance, intraoperative parathyroid hormone (PTH) monitoring is used. Intraoperative PTH is not used routinely when 2 modalities successfully locate an adenoma based on previous research from our institution that demonstrated only marginal benefit but a significant increase in surgery duration. 15 In all cases, intraoperative frozen-section study is performed to ensure removal of the PTA, followed by postoperative final pathology.
For the present study, patient demographics and preoperative laboratory findings were retrieved from the medical charts. Data on PTA location and size (maximal diameter) on imaging evaluation, including the operator who performed the scan, were retrieved from the computerized MIBI and US reports. US performers were independent and unaware of MIBI scan results. Data on the actual PTA location were retrieved from the surgical reports and on PTA size (maximal diameter) from the final pathology reports.
Statistical Analysis
Statistical analyses were performed using SAS software, version 9.2 (SAS Institute, Cary, North Carolina). Normally distributed variables were compared between the preoperative and postoperative assessments with the t test and nonnormally distributed variables with the Wilcoxon test. Pearson correlation and κ agreement test were used to determine the relationship in PTA size between the preoperative US and final pathology reports. A P value <.05 was considered significant.
Results
The study cohort included 410 patients with a mean ± SD age of 63.5 ± 22 years; 76% were female. As stipulated by the inclusion criteria, all underwent preoperative US and MIBI evaluation, and all were found to have a single parathyroid adenoma on the final pathology report.
US detected a suspicious PTA in 365 patients. A PTA was not detected in 45 patients. The PTA was localized intraoperatively in all patients. The most common site was the lower pole of the thyroid gland, with equal distribution between the left and right sides. Figure 1 shows the distribution of the parathyroid adenoma locations by preoperative assessment and intraoperative findings. Ectopic adenomas were located in the submandibular triangle (n = 1), carotid sheath (n = 2), mediastinal (n = 2), intrathyroidal (n = 2), and retroesophageal (n = 1). When first US exam failed to locate an adenoma, an additional test was performed by an experienced neck US specialist who localized the adenoma in the neck in 4 of 6 (75%) patients. For the other 2 patients, an MRI was performed in accordance with MIBI results, which demonstrated a mediastinal adenoma.
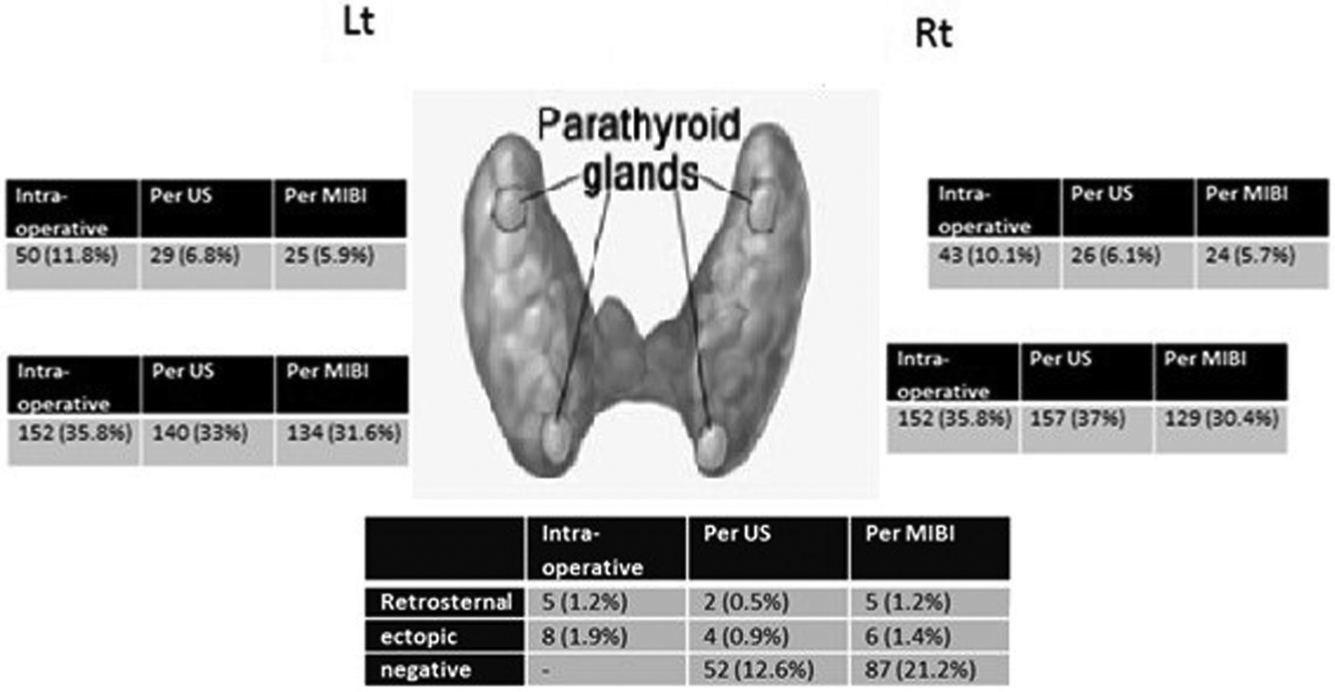
Distribution of parathyroid adenoma location by preoperative assessment and intraoperative finding. Lt, left; MIBI, methoxyisobutylisonitrile; Rt, right; US, ultrasonography.
US correctly predicted the location of the PTA (right vs left and upper vs lower) in 77% of the patients. The corresponding rate for MIBI was 76%. The sensitivity and positive predictive value of MIBI and US for PTA localization, alone and together, are shown in Table 1 .
Sensitivity and Positive Predicted Values of US and MIBI for PTA Localization.
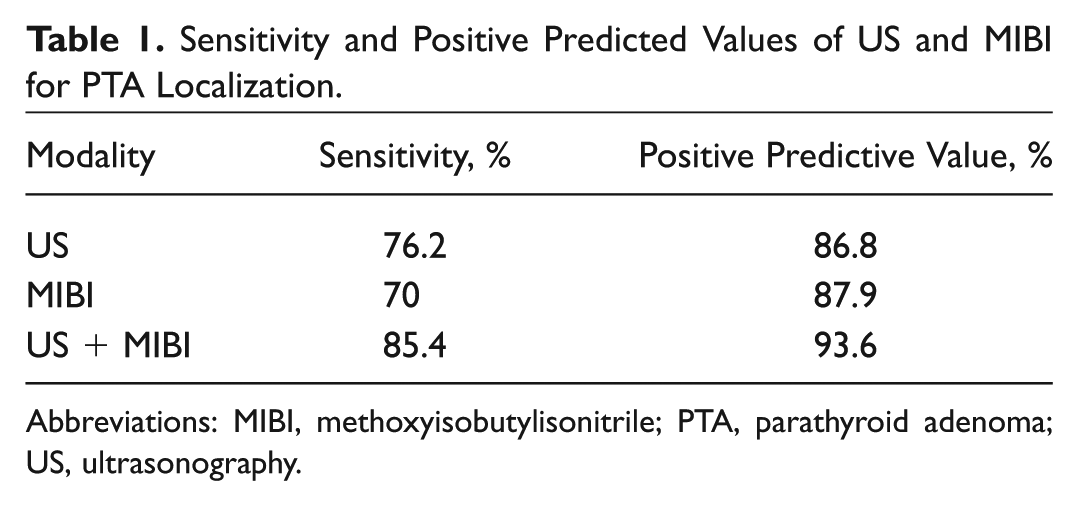
Abbreviations: MIBI, methoxyisobutylisonitrile; PTA, parathyroid adenoma; US, ultrasonography.
The US-measured adenoma size was documented for 313 patients; mean ± SD size was 1.57 ± 0.77 cm. Mean adenoma size according to the pathology reports of these 313 patients was 1.82 ± 0.9 cm. There was a positive correlation of PTA size between the preoperative US and the postoperative pathology report (r = 0.514, P < .0001), with 83% of sonographies predicting adenoma size with no more than a 10% difference.
To further evaluate the concordance between the imaging and definitive modes of measurement, we stratified the adenomas by actual size into 3 groups: <1 cm, 1 to 2 cm, and >2 cm. We found a high concordance between the US and pathology findings for the midsize adenomas (75%) and the larger adenomas (60%) and a low concordance for the smaller adenomas (24%) (P = .08). There was no significant difference in adenoma localization between US and MIBI either for adenomas measuring <1 cm (P = .258) or for adenomas measuring >1 cm (P = .233).
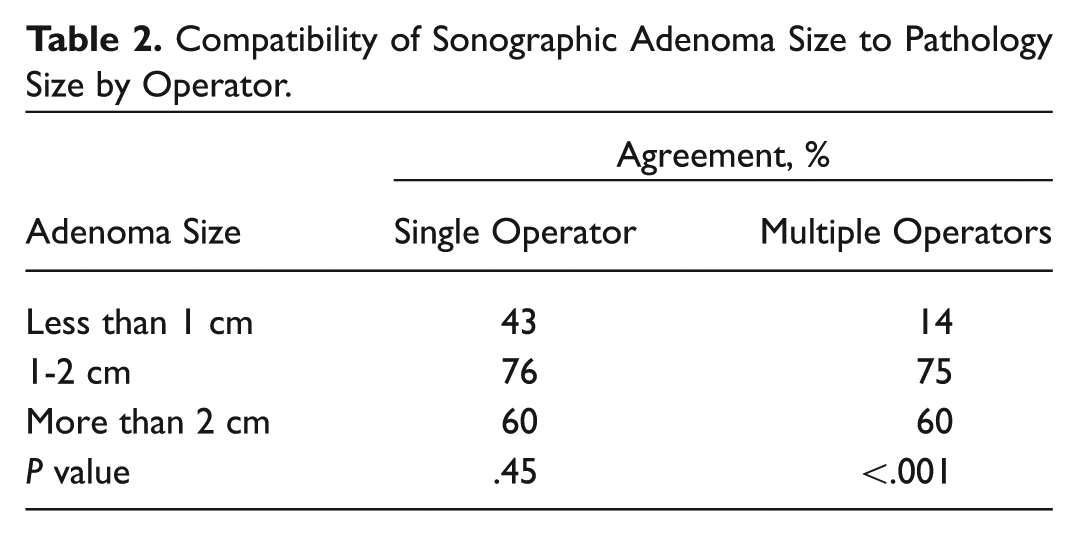
We then performed a subgroup analysis to determine the effect of a single expert radiologist as opposed to multiple radiologists on the concordance of PTA size with the postoperative pathological evaluation. Of the total 410 US studies, 168 (40.6%) were performed by the same single senior neck US specialist (M.C.), who has been practicing at a tertiary medical center for more than 3 decades, and 242 were performed by many different operators, mostly general radiologists of varying experience practicing US as well as other imaging modalities. We found that the location of the PTA was accurately predicted in 80% of patients in the first group and 75% of patients in the second group (P = .34). In terms of PTA size, there was a significant positive correlation between the preoperative and postoperative studies, but the correlation was stronger when a single neck specialist performed the preoperative evaluation (r = 0.650 vs 0.342, P < .0001). The ratio of the actual to the estimated adenoma size for the 2 groups was calculated by dividing the measurement documented in the pathology report with the measurement documented in the US report for each adenoma diagnosed. The ratio was more accurate when a single expert neck specialist operator performed the scans than when multiple operators did so (1.06 vs 0.87, P < .0001). The predictive accuracy was significantly higher for a single operator for adenomas smaller than 1 cm (43% vs 14%, P < .001); for adenomas larger than 1 cm, the difference did not reach statistical significance. Table 2 presents the concordance data between US and pathology by operator.
Compatibility of Sonographic Adenoma Size to Pathology Size by Operator.
Discussion
To our knowledge, this is one of the largest studies in the English literature addressing this accuracy of preoperative ultrasound for localizing PTA preoperatively and the first to describe the use of US for preoperative estimation of PTA size.
Our study shows that preoperative US has a high sensitivity (76.2%) and a high positive predictive value (86.8%) for localizing PTA. These values are close to the 80% reported in 2008 by Siperstein et al 18 in the largest published series to date (1158 patients). Similar to previous publications,19-21 PTA was more commonly localized to the lower parathyroid glands ( Figure 1 ).
We found a positive correlation between the preoperative size estimation and the tumor size according to the pathology report, with no more than a 10% difference from the actual size in 83% of the US studies.
US accuracy in the present study was higher for adenomas larger than 1 cm and lower for adenomas smaller than 1 cm. In an effort to explain this discrepancy, we examined the potential influence of US operator experience on size prediction by comparing US scans performed by a single highly experienced US radiologist specializing in US of the neck, including the thyroid and parathyroid gland, with scans performed by multiple different general US operators with variable experience. We found that the prediction size rate for adenomas smaller than 1 cm was significantly higher in the single-operator group. Lloyd et al 10 observed that scans done by experienced US operators had 82% sensitivity for PTA localization compared with 50% for scans done by nonexperienced operators. In the present study, in which both PTA localization and size were evaluated, the difference in performance by operator experience was more significant for size estimation than for localization. This finding emphasizes the importance of the expertise of the operator, especially in the neck region, given the contribution of an accurate preoperative estimation of PTA size to identification of the adenoma during surgery. Early and accurate identification will shorten operative time and prevent unnecessary dissection of the central compartment during neck exploration. It is especially pertinent for smaller adenomas, which are more challenging to find and require better preoperative assessment. Interestingly, larger adenomas greater than 2 cm have shown a lower concordance (60% vs 75%) compared to adenomas 1 to 2 cm. This discrepancy was also raised in a study by Bachar et al 22 regarding thyroid nodules that presented a similar discrepancy in the larger nodules. Changes in accuracy can be explained by interference of close organs such as clavicle, thyroid, and vessels in the larger adenomas. Moreover, atypical shape or margins that may not be easy to distinguish from the surrounding thyroid tissue can influence size accuracy. In locating parathyroid adenomas, there was no advantage for the experienced neck US specialist (80% vs 75%). This has several explanations. First, US is extremely reliable to locate adenomas; hence, the added value of the sonographic expertise did not reach statistical significance, only a mild trend. Second, more challenging, harder cases were referred to the US specialist. Intuitively, head and neck surgeons who specialize in US would be the best candidates to perform preoperative US because they are familiar with the cervical anatomy and different pathologies of the neck and can use the information to receive feedback during the operation itself. Previous studies have shown that surgeon-performed US is effective for localizing PTAs. 21 Soon et al, 17 in a study of 218 patients who underwent parathyroidectomy, found no statistically significant difference in sensitivity between surgeon-performed and radiologist-performed US scans (83% and 82%, respectively). Arora et al 23 reported a sensitivity of 88% and a positive predictive value of 92% in 160 patients who underwent parathyroidectomy and concluded that surgeon-performed US is the only imaging modality needed for patients with a suspected PTA. In the large study by Siperstein et al, 18 surgeon-performed US was found to be better than MIBI for the identification and localization of PTAs. However, our analysis of the performance of US for estimating both PTA location and size shows that performing sonography is challenging, especially when the parathyroid adenoma is small. Therefore, we encourage endocrine surgeons to perform preoperative US on their patients, as this is a valuable tool. As most surgeons are not highly experienced in performing US, its limitation, especially in the small-sizes adenomas, should be taken into account and therefore interpreted with caution.
Our study has several limitations. First, this is a retrospective study. Moreover, we decided to include only patients with the diagnosis of solitary parathyroid adenoma in our study to create a homogeneous study group. Patients who were diagnosed with double adenoma, multiglandular hyperplasia, or recurrent or persistent disease were not included. The decision to exclude this minority group might have caused a potential selectin bias. Further studies evaluating US accuracy regarding double adenoma and multiglandular hyperplasia are required.
In conclusion, the present study highlights the importance of preoperative US in the evaluation of both the size and the location of PTAs. In general, US is a sensitive and highly accurate tool, but its accuracy is even higher in the hands of an experienced operator who specializes in neck US. This is particularly pertinent when the adenoma is small (<1 cm).
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.