
Abstract
Objective
The present study compared the frequency of depressive disorder in patients with thyroid cancer who had undergone thyroidectomy with the frequency in control individuals.
Study Design
Retrospective population-based cohort study.
Setting
This study used data from the Korean Health Insurance Review and Assessment Service–National Sample Cohort.
Subject and Methods
A total of 3609 participants with thyroid cancer who had undergone thyroidectomy between 2003 and 2011 were enrolled in this study and matched 1:4 with 14,436 control participants by age, sex, income, and region of residence. The cumulative incidence of postoperative depressive disorder was evaluated over a period of 10 years after the thyroidectomies and compared with the incidence in controls. Depressive disorder was diagnosed by a psychiatrist.
Results
The incidence of depressive disorder was significantly higher in the thyroid cancer with thyroidectomy group than in the controls up to postoperative year 1. A subgroup analysis showed the same higher incidence of depressive disorder in the thyroid cancer group than controls for up to 1 year after operations in young adult (≤44 years old), female, urban, and low-income groups. However, the incidence was elevated only in the year of the thyroidectomies themselves in middle-aged and older, rural, and high-income groups.
Conclusion
Patients with thyroid cancer who undergo thyroidectomy have depressive disorder more frequently than normal controls. However, the frequency of depressive disorder after thyroidectomy recovers in a shorter period in middle-aged or older, high-income, and rural-dwelling patients, compared to younger, low-income, and urban-dwelling patients.
Keywords
Thyroid cancer is the most common cancer of the endocrine organs, comprising 1% of all malignancies. 1 The incidence and prevalence of thyroid cancer are increasing rapidly worldwide. 2 In Korea, the frequency of diagnosis of thyroid cancer has increased more than 10-fold in a period of about 2 decades due to the increased use of thyroid ultrasonography and screening. 3 Differentiated thyroid carcinomas, mainly papillary carcinomas, comprise the majority of thyroid malignancies and have an excellent prognosis, with a 10-year survival rate of over 90%. 4
Due to the excellent prognosis of thyroid cancer, survivors face, for many years, issues mainly related to health-related quality of life (HRQOL) besides survival. Despite the low morbidity and mortality of differentiated thyroid cancer, overall HRQOL in thyroid cancer is similar to that of cancers with poorer prognoses, such as colon cancer, gynecological cancer, and glioma, and worse than that of breast cancer. 5
Thyroid cancer survivors experience higher levels of psychological distress, including anxiety and depression, than noncancer controls. 6 Depression is a common comorbidity of cancer, and its incidence in the general cancer population was reported to range from 4% to 16% in a systemic review. 7 The incidences of depressive symptoms and definite depression are 11% and 3.7%, respectively, in the general population, with a higher rate in women than men. 8 Besides decreasing the HRQOL of patients with cancer, depression significantly interferes with treatment adherence and can lower survival rates compared with nondepressed patients. 9 Thyroid cancer survivors may benefit from psychosocial intervention over an appropriate period, and thus National Comprehensive Cancer Network Distress Management guidelines suggest that all patients with cancer should be screened for psychological distress regardless of the severity of their cancer to prevent poor recognition of depression and distress by the health care providers and patients. 10
However, depression and depressed mood are easily underdiagnosed and underestimated by examiners and patients themselves when treatment is focused on survival. The incidence of depression in thyroid cancer survivors has not been thoroughly evaluated. Previous studies have reported a significantly increased rate of depression in patients with thyroid cancer, although the studies all involved small numbers of patients in single or multiple institutions.9,11 When we reviewed PubMed and Embase databases for studies using the keywords “([thyroid cancer] OR [thyroid carcinoma] OR [thyroidectomy]) AND ([depression] or [distress] or [mood]) AND (national)” and limited the results to studies published in English before January 2018, we identified only one 1-year cross-sectional study using a national population sample and evaluating the incidence of major depressive disorder (MDD) in the 10 most common cancers. 12 The study demonstrated a 5.6% prevalence of MDD in 349 patients with thyroid cancer.
In the present work, we used data from a national cohort study to evaluate the frequency of depressive disorder in thyroid cancer survivors and to compare the frequency with controls. To our knowledge, this is the first multiyear study to evaluate depression in patients with thyroid cancer in a national population and involves the largest number of patients with thyroid cancer examined to date. In this study, we followed up the patients with thyroid cancer who underwent thyroidectomy and 1:4 matched controls for up to 10 years.
Materials and Methods
Study Population and Data Collection
The ethics committee of Hallym University (2014-I148) approved the use of these data. Written informed consent was waived by the institutional review board.
This national cohort study relied on data from the Korean Health Insurance Review and Assessment Service–National Sample Cohort (HIRA-NSC). The Korean National Health Insurance Service (NHIS) selected individuals directly from the database of the entire population to prevent nonsampling errors. Approximately 2% of the total number of individuals (1 million) were selected from the entire Korean population of 50 million. The selected data could be classified into 1476 levels (age [18 categories], sexes [2 categories], and income levels [41 categories]) using randomized stratified systematic sampling methods by proportional allocation to represent the entire population. After data selection, the appropriateness of the sample was verified by a statistician who compared data for the entire Korean population with the sample data. The detailed procedures used have been described by the National Health Insurance Sharing Service. 13 The cohort database included (1) personal information; (2) health insurance claim codes (procedures and prescriptions); (3) diagnostic codes using the International Classification of Diseases, Tenth Revision (ICD-10); (4) socioeconomic data (residence and income); and (5) medical examination data for each participant for a period ranging from 2002 to 2013.
As all Korean citizens have a 13-digit resident registration number from birth to death, exact population statistics can be determined from the database. It is mandatory for all Koreans to enroll in the NHIS. All Korean hospitals and clinics use the 13-digit resident registration numbers to register individual patients for the medical insurance system. Therefore, the risk of overlapping medical records is minimal, even if a patient transfers to another facility for further treatment. Moreover, all medical treatments in Korea can be tracked using this HIRA system. As part of the national system, death notifications are made to an administrative entity as a legal requirement prior to the funeral. The cause of death is recorded on the death certificate that is filed.
Selection of Participants
Participants who underwent thyroidectomy (claim codes: P4551, P4552, P4553, P4554, and P4561) for thyroid cancer (ICD-10: C73) from 2003 through 2011 were included from among 1,125,691 cases with 114,369,638 medical claim codes (n = 3789). Individuals younger than 15 years (n = 125) were excluded. These patients were matched 1:4 with individuals who never underwent thyroidectomies from 2002 through 2013 and who have never been diagnosed with thyroid cancer. The 2 groups were matched for age, income, region of residence, and number of histories of preoperative depression for 1 year. To prevent selection bias, the control group members were selected in random number order, from top to bottom. Participants for whom adequate matches could not be found were excluded (n = 55). Finally, 3609 patients with thyroid cancer who underwent thyroidectomies were matched with a control group of 14,436 individuals ( Figure 1 ).
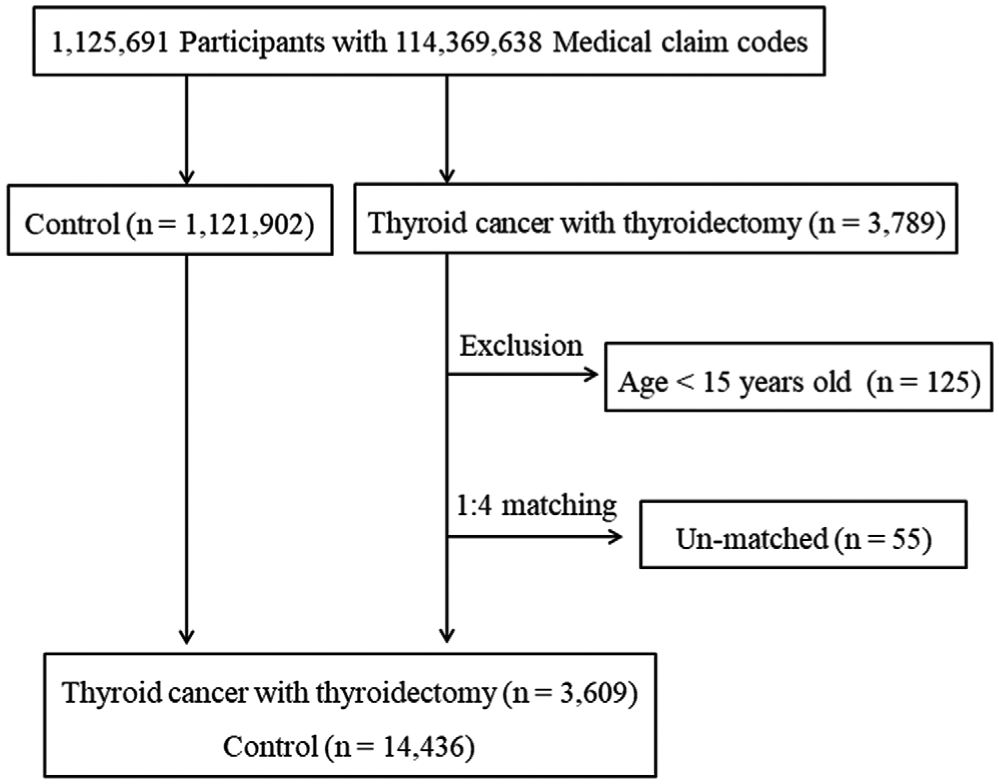
Scheme of participant selection. A total of 3789 patients with thyroid cancer who underwent thyroidectomies from 2003 through 2011 were identified among a total of 1,125,691 individuals. After removing unmatched patients and those younger than 15 years, 3609 patients were matched 1:4 with 14,436 controls.
Variables
Age was divided into 13 successive 5-year intervals: 15 to 19, 20 to 24, 25 to 29, . . . to 75+. Income was initially divided into 41 classes (1 health aid class, 20 self-employment health insurance classes, and 20 employment health insurance classes) and recategorized into 11 classes (class 1 [lowest income] to 11 [highest income]). Regions of residence were divided into 16 areas according to administrative district. They were then regrouped into urban (Seoul, Busan, Daegu, Incheon, Gwangju, Daejeon, and Ulsan) and rural areas (Gyeonggi, Gangwon, Chungcheongbuk, Chungcheongnam, Jeollabuk, Jeollanam, Gyeongsangbuk, Gyeongsangnam, and Jeju).
Depressive disorder was defined as a diagnosis made by a psychiatrist from 2002 through 2013 using ICD-10 codes F31 (bipolar affective disorder) through F39 (unspecified mood disorder). Numbers of visits to psychiatrists in clinics or hospital for depressive disorder were counted every year. Preoperative depressive disorder was counted for 1 year, and postoperative depression histories were counted each year over the entire period (1, 2, 3, . . . 10 years).
Statistical Analyses
We compared the difference in depression histories between thyroid cancer and the control group using an independent t test. Two-tailed analyses were conducted, and statistical significance was set as .05. The results were analyzed using SPSS v. 21.0 (SPSS, Inc, an IBM Company, Chicago, Illinois).
For the subgroup analysis, we stratified the participants by age, sex, region, and income: young adults (≤44 years old) vs middle-aged and older adults (≥45 years old); men vs women; urban vs rural; and low income (1-8) vs high income (9-11). The dividing point was determined around median values.
Results
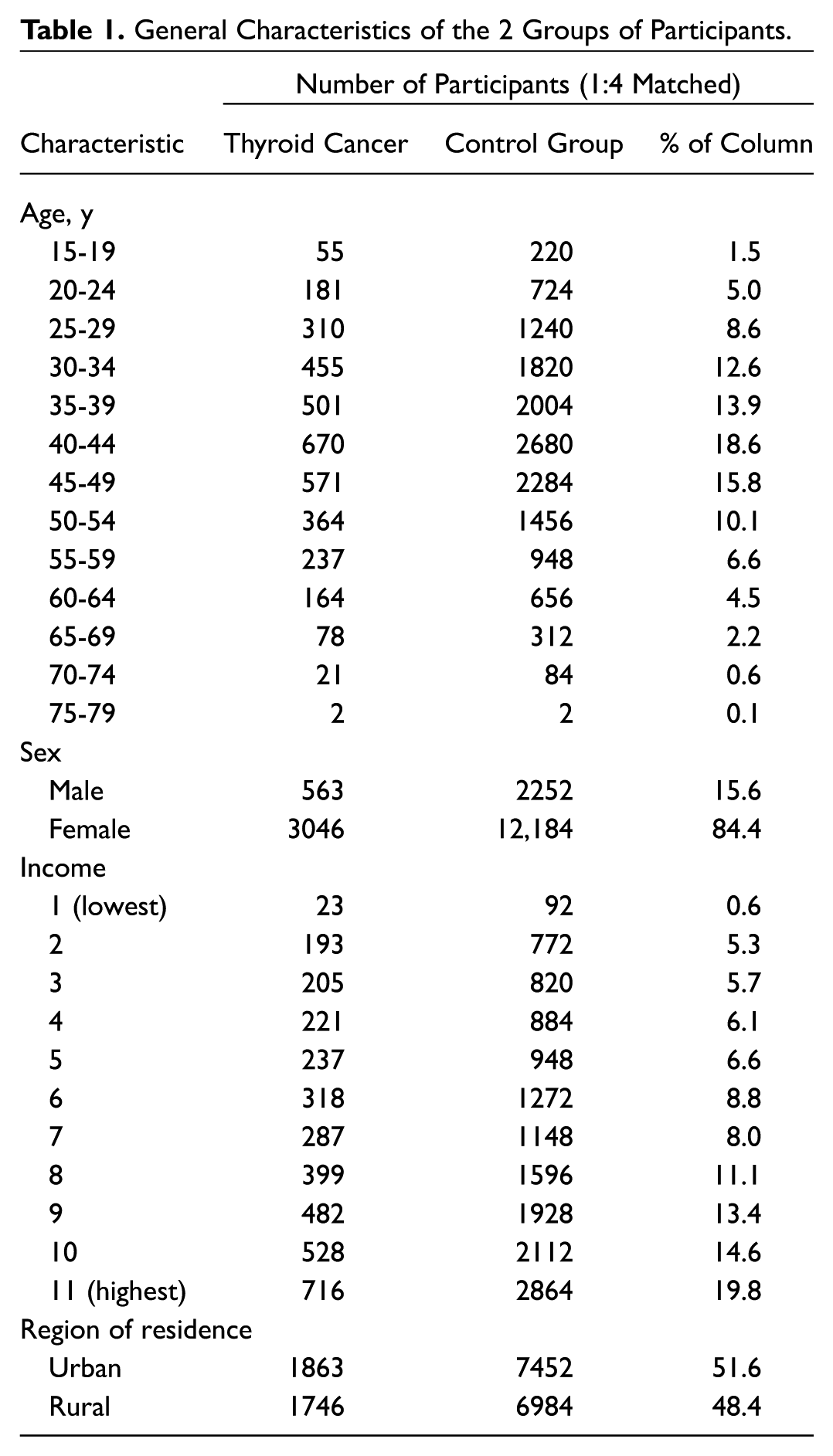
The general characteristics of the case and control groups, including age distribution, sex, level of income, and region of residence, were well matched ( Table 1 ).
General Characteristics of the 2 Groups of Participants.
The incidence of depressive disorder was the same in the cancer and control groups before the thyroidectomies because of matching ( Table 2 ). The incidence of depressive disorder was higher in the thyroid cancer group for up to 1 year after the operations (postoperative year 0 [P < .001], postoperative year 1 [P = .009]). The difference in the incidence of depressive disorder declined by 2 years after thyroidectomy.
Number of Histories of Preoperative and Postoperative Depressive Disorder in the Thyroid Cancer and Control Groups. a
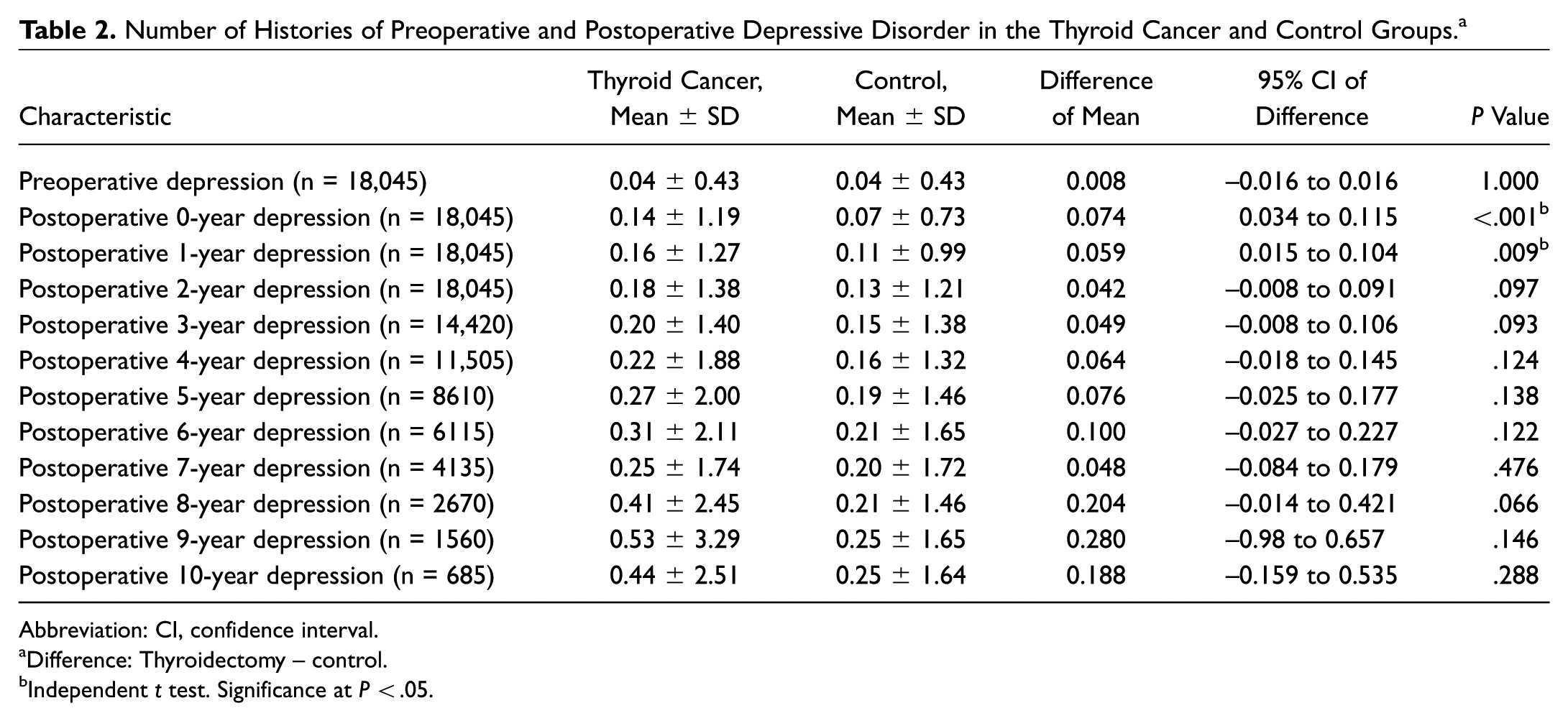
Abbreviation: CI, confidence interval.
Difference: Thyroidectomy – control.
Independent t test. Significance at P < .05.
Subgroup analysis of the frequency of depressive disorder among young adults aged ≤44 years gave similar results, with a higher frequency of depressive disorder in the thyroid cancer group after thyroidectomy for the first postoperative year ( Table 3 ). Similarly, in patients with thyroid cancer aged ≥45 years, a higher frequency of depressive disorder was observed only in the year of thyroidectomy.
Subgroup Analyses of the Number of Preoperative and Postoperative Depressive Disorder Histories in the Thyroid Cancer and Control Groups According to Age.
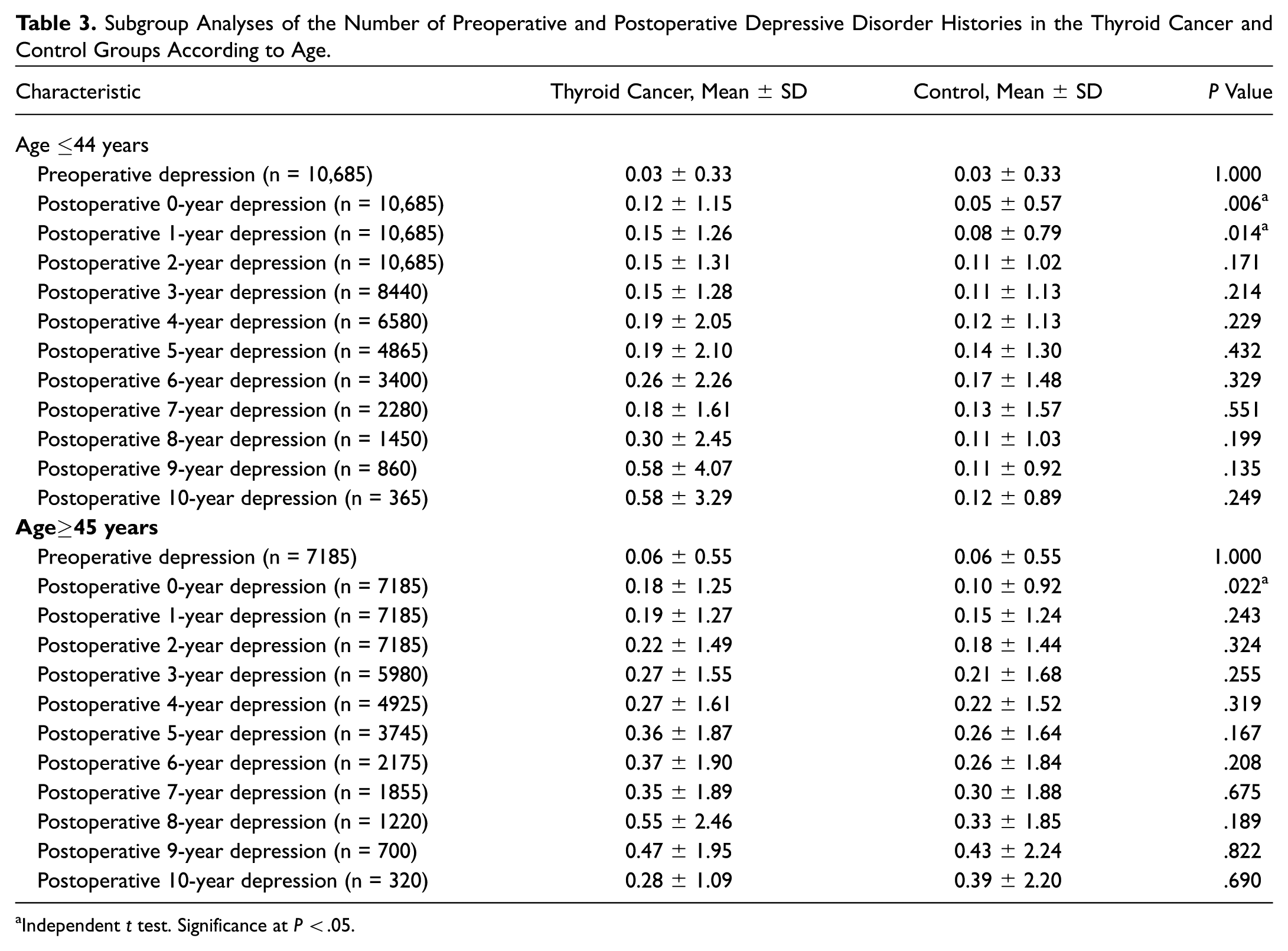
Independent t test. Significance at P < .05.
Subgroup analysis stratified by sex, region, and income showed that the incidence of depressive disorder was higher in the thyroid cancer group than in controls for up to 1 year after thyroidectomy in women, the urban group, and the low-income group. Depressive disorder was more frequent than controls only in the year of thyroidectomy in the high-income group and rural group. However, there was no difference in depressive disorder between the 2 groups in men for all periods.
Discussion
We have shown that depressive disorder was more frequent in the thyroid cancer group than in the control group in the first year after thyroidectomy and that there was no significant difference in the incidence of depressive disorder thereafter for 10 years after thyroidectomy. In addition, subgroup analysis by age showed that the frequency of depressive disorder was elevated for longer in patients who were younger than 45 years within 2 years of their thyroidectomy than in those aged 45 years or older in the year of their thyroidectomy. A subgroup analysis based on sex demonstrated that the higher incidence of depressive disorder was significant in female patients up to 1 year after thyroidectomy. However, there was no difference between patients with thyroid cancer and controls in male patients. Also, urban residents and low-income patients had a longer period of depressive disorder than rural residents and high-income patients.
Patients with cancer frequently experience psychiatric conditions, and depression and anxiety constitute 85% of such cases. 14 The prevalence of depression in patients with thyroid cancer in various publications ranges from 4.8% to 5.6%.12,15 However, it was unclear whether the incidence of depression in patients with thyroid cancer is higher than in the general population in the long term. A multicenter epidemiological study compared the prevalence of depressive symptoms in patients with cancers of various organs and controls in the general German population. 9 In that study, the odds ratio for the risk of depression in patients with thyroid cancer compared to the general population was 9.3 (95% confidence interval, 4.1-21.2; P < .001). Interestingly, patients with thyroid cancer and pancreatic cancer had the highest rates of depression, higher than those with cancers with poorer survival rates, such as brain, lung, stomach, breast, kidney, and colon. However, the size of the thyroid cancer sample (n = 25) was small, and the study design was cross-sectional with no follow-up period.
In the current study, depressive disorder was more common in the thyroid cancer group than in the controls in the short term (<2 years) but not in the long term (≥2 years). As was done in previous studies,16,17 we considered ≥2 years to be in the “long term” for cancer survivors. In a meta-analysis of 43 publications comparing rates of depression in long-term cancer survivors with those in the general population, the relative risk of depression was higher in patients in their first 2 years following diagnosis compared to those further out (2-10 years) from diagnosis. 17 The cause for the high incidence of depressive disorder in the first or second year may be because it is a period to adjust and adapt to the medical crisis and because all major treatments, including surgery, completion thyroidectomy, and radioactive iodine ablation therapy, are completed in this period in cases without recurrence. In addition to the need for a period for patients to adapt psychologically to having cancer, patients with thyroid cancer need to adapt to thyroid hormone changes in the short term. Thyroidectomy and hypothyroidism induced by radioactive iodine ablation therapy disrupt the thyroid hormone equilibrium, and many investigators have reported that hypothyroidism that developed due to treatment of thyroid disease is a major risk factor for depression.18,19 However, a systematic review of literatures evaluating an association between hypothyroidism and depression demonstrated that there was no association between thyroid function status and depression in patients without thyroid disease. 20 In contrast, for patients receiving thyroid hormone replacement, there was a significant association between thyroid status and depression. Due to the overlap of clinical symptoms between depression and hypothyroidism, thyroid dysfunction after thyroidectomy may have been misdiagnosed as depressive disorder in this study. 21 However, we assume that patients with overt thyroid dysfunction were excluded in this study because the thyroid function test is routinely performed by a psychiatrist to rule out hypothyroidism dysfunction before diagnosing depressive disorder.
Our results suggest that prompt evaluation and management of depressive disorder is important because of the increased rate of depressive disorder in the short-term period. Tagay et al 22 reported that depression is the strongest independent risk factor for impaired physical and mental HRQOL in patients with thyroid cancer, especially in the short term. Moreover, the risk of depression in patients with thyroid cancer can be reduced by active and prompt management of depressive symptoms.23,24 Wu et al 25 compared HRQOL in patients with thyroid cancer who received psychological and behavioral interventions for 1 year and those who received conventional care. After a year, patients in the intervention group had significantly fewer symptoms of depression and anxiety, as well as better overall function and HRQOL. Indeed, distress in patients with cancer should be regarded as a sixth vital sign, and routine screening for psychological distress is recommended to increase their well-being while lowering emotional and physical problems. 26 An intervention for the distress to help adjustment, even if just education, can aid in increasing quality of life and decreasing psychological distress.
One strength of this study is the large number of participants (n = 18,045) and the long follow-up period, up to 10 years. This study evaluated the frequency of depressive disorder in the largest number of patients with thyroid cancer (n = 3609) examined to date. Previous studies were based on patients with thyroid cancer from a few institutions or on a small number of patients with thyroid cancer that were part of a systematic review, including different types of cancer.4,9,11,15,22,27-29 Second, depressive disorder rates were based on visits to psychiatrists. Third, our data are representative of the entire nation, since all Korean residents have to join the national health insurance system, and its representative nature was verified by a statistician. 30
This study has some limitations. First, we did not evaluate self-reported depressive symptoms and the severity of depressive disorder. However, a diagnosis of “depressive disorder” by a psychiatrist may be more objective than “depressive mood or emotion” assessed by a questionnaire evaluating HRQOL. Second, it is hard to distinguish whether the high incidence of depressive disorder was due to thyroid cancer, thyroidectomy, or both. A comparison with cases of thyroid cancer under active surveillance or thyroidectomy cases for benign thyroid nodules may differentiate the 2 possible causes, but comparison is limited due to the small number of patients in both cases. Third, our study was confined to a single ethnicity. The prevalence of depression differs among ethnicities and in different cultures and environments. 31 Therefore, these data may not be extrapolated to general population. Fourth, we included a broad spectrum of mood disorders in this study. It may have decreased the homogeneity of depressive disorder, although narrowing the spectrum of depressive disorder may underestimate the patients with depressive mood disorders.
Conclusions
Our study suggests that patients with thyroid cancer develop depressive disorder more frequently than the healthy population for the short term (≤1 year) after thyroidectomy. In addition, the frequency of depressive disorder was elevated for longer (<2 years) in younger patients (≤44 years), females, urban residents, and low-income earners than in middle-aged and older patients (<1 year), rural residents, and high-income earners.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.