
Abstract
Objective
To examine the effect of xylitol nasal irrigation in a large sample size of patients who had undergone nasal surgery.
Study Design
Double-blinded randomized controlled crossover study.
Setting
Tertiary referral center.
Methods
The study included 100 patients with sinonasal disease who underwent endoscopic sinus surgery (ESS), septoplasty, or both concurrently. To identify patients with allergic sensitization, serum-specific immunoglobulin E levels were measured. Nasal symptoms were evaluated with the NOSE (Nasal Obstruction Symptoms Evaluation) and SNOT-20 (Sino-Nasal Outcome Test–20) and via visual analog scale (VAS) scores.
Results
In the ESS group (n = 34), the general nasal symptom score evaluated by the SNOT-20 showed significantly greater improvement in the xylitol group versus the saline group (P = .022). VAS symptom scores for sneezing (P = .003), headache (P = .02), and facial pain (P = .037) were also more improved in the xylitol group. In the septoplasty group (n = 39), the VAS score for nasal stuffiness showed a significantly greater improvement in the xylitol group when compared with the saline irrigation group (P = .001). Among the patients with allergic sensitization (n = 31), rhinorrhea symptoms improved significantly more in the xylitol group than in the saline group (P = .024). The preference survey showed that more than half of the patients in each surgical group preferred xylitol irrigation.
Conclusion
We found that xylitol nasal irrigation was useful in postoperative ESS and septoplasty care. For patients with allergic sensitization, rhinorrhea showed greater improvement in the xylitol group than in the saline group.
Nasal irrigation is commonly performed after sinonasal surgery. After endoscopic sinus surgery (ESS), nasal irrigation improves mucociliary clearance, decreases mucosal edema, dilutes inflammatory mediators, and mechanically cleanses concentrated mucous. 1 Nasal irrigation was also shown to minimize or prevent crusting, clear infective debris, ensure moistening of the mucosa, and recover mucociliary function after septoplasty. 2
Xylitol is effective for postoperative nasal irrigation due to its antibacterial characteristics, promotion of innate bactericidal mechanisms,3-5 and antiadhesive effect. 6 These effects could confer benefits for patients undergoing ESS or septoplasty. Mucosal injury can occur during surgery, and nasal symptoms may develop; there is also a risk of infection and inflammation. A pilot study was conducted in which patients with previous ESS underwent xylitol nasal irrigation. 7 However, the sample size was relatively small (n = 15), and the symptom score was slightly worse after irrigation, which conflicts with the findings of other reports.1,2,8-11 In this study, we used a larger sample size and examined the effect of xylitol nasal irrigation on patients who had undergone ESS or septoplasty (or both). We also compared the extent of nasal symptom relief between the saline and xylitol irrigation groups. The endoscopic outcomes were compared with a modified Lund-Kennedy scoring system. 12
Materials and Methods
Study Design and Patients
This study was a double-blinded randomized controlled crossover study comparing 2 methods of nasal saline irrigation. The Institutional Review Board of Seoul St Mary’s Hospital (KC16OISI0910) approved this study, which was conducted in accordance with the Declaration of Helsinki. All patients gave informed consent before they were enrolled. The study included patients with sinonasal disease who underwent ESS, septoplasty, or both concurrently at Seoul St Mary’s Hospital from November 2016 to April 2018. Patients who had previously undergone sinonasal surgery or who had immunocompromised status, cystic fibrosis, primary ciliary dyskinesia, a history of head and neck irradiation, rheumatologic diseases, or active pregnancy were excluded.
All patients underwent septoplasty with same surgical technique. Quilting suture (through-and-through suture) was conducted for approximating bilateral septal mucosa, and Merocel (Medtronic, Minneapolis, Minnesota) packing was inserted and removed 1 day postoperatively. In ESS, there were no Draf 2B/3 cases among the enrolled patients. Also, the same packing material (NasoPore; Stryker, Kalamazoo, Michigan), the same debridement schedule (postoperative days 3, 17, 24, and 38), and the same procedure by a single surgeon (S.W.K.) were conducted for both study groups. All patients in this study received topical nasal steroids postoperatively and were educated about the use of topical nasal steroids during the entire period of study.
The study included 100 patients, and the study flowchart is presented in Figure 1 . Thirteen patients withdrew from the study: 6 in group A and 5 in group B were lost to follow-up, and 1 patient in each group showed upper respiratory infection symptoms during the study. To identify patients with allergic sensitization, serum-specific immunoglobulin E levels were measured. In this analysis, a specific immunoglobulin E level >0.35 for any common airborne allergen was defined as allergic sensitization. The crossover study design is illustrated in Figure 2 . A 7-day washout period was scheduled before changing irrigation material to minimize any residual bias.
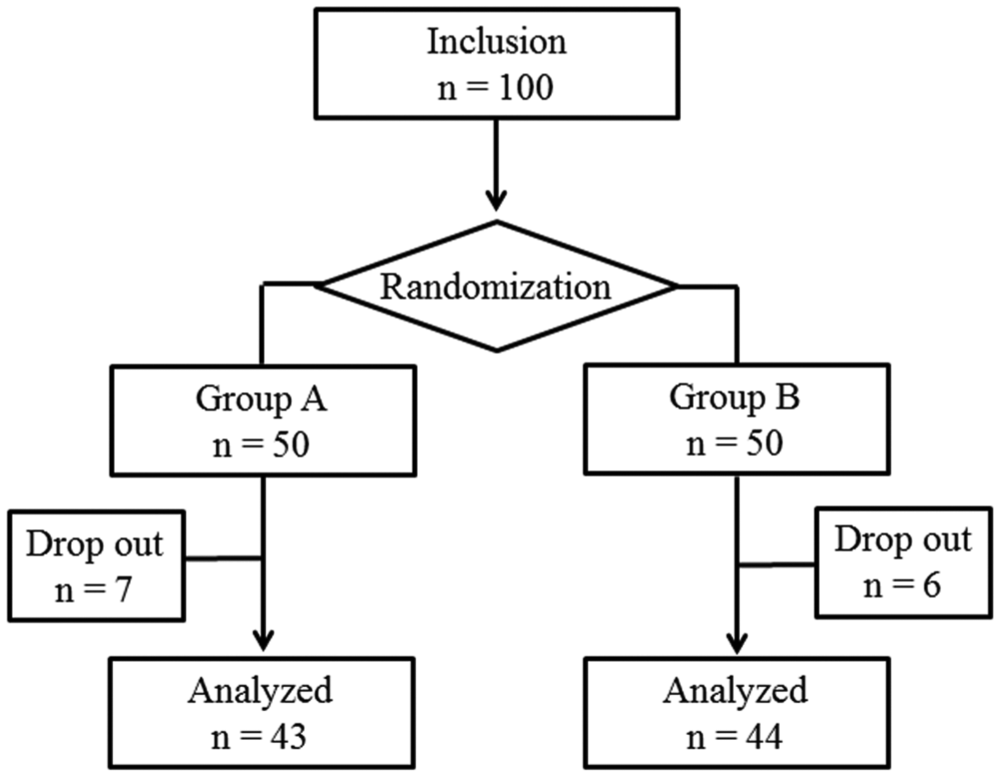
Patient flowchart.
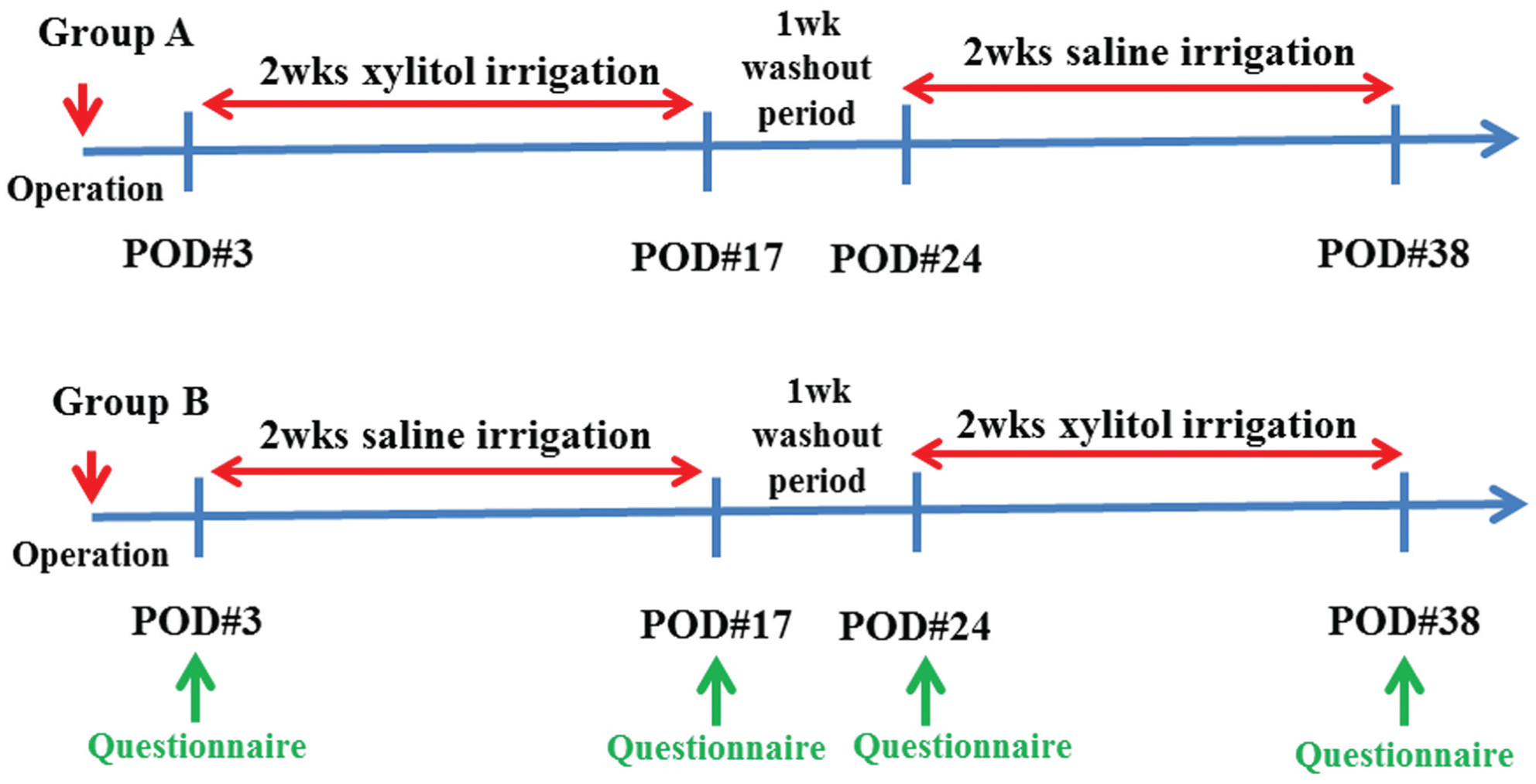
Study design. POD, postoperative day.
Materials
Xylitol
This study used unlabeled sealed packages containing 4 mg of pharmaceutical-grade xylitol (Xlear, Inc, American Fork, Utah) and 2 mg of sodium. The patients received 50 of these packages and were instructed to mix the contents of 1 package with 240 mL of distilled water in a nasal irrigation bottle, followed by bilateral nasal irrigation 3 times a day. They were instructed to use 1 envelope per day for 14 days.
Normal Saline
Standard buffered isotonic salt (NeilMed, Santa Rosa, California) was repackaged into sealed unlabeled packages. Fifty packages were given to the patients, who were instructed to mix the contents with 240 mL of distilled water in an irrigation bottle. These patients were also instructed to use 1 package per once 3 times a day for 14 days.
The sealed xylitol and salt packages were divided into 2 number-encoded envelopes. The patients were instructed to perform a nasal irrigation 3 times a day for 14 days, from postoperative day 3 onward, using the contents of the first sealed envelope. After the 7-day washout period, patients performed nasal irrigation in the same manner for 14 days with the other sealed envelope. A random-number generator was used to randomize the order of irrigation in a double-blinded fashion. Symptom questionnaires were distributed to the patients and collected by an independent coordinator throughout the study.
Outcome Measures
Nasal symptoms were evaluated with the Nasal Obstruction Symptoms Evaluation (NOSE) 13 and Sino-Nasal Outcome Test–20 (SNOT-20) 14 and via visual analog scale (VAS) scores. The VAS assessment covered nasal obstruction, sneezing, rhinorrhea, snoring, headache, facial pain, and olfactory changes. 15 The symptom questionnaires were distributed and collected at the outpatient clinic on postoperative days 3, 17, 24, and 38.
Statistical Analysis
All data are provided as mean ± SD. Student’s t test was used to compare the demographic characteristics between the groups. NOSE, SNOT-20, and VAS score changes (pre- vs posttreatment) were analyzed with a mixed effects model, 7 as were the effects of treatment. A P value <.05 was regarded as statistically significant. SAS software (version 9.4; SAS Institute, Cary, North Carolina) was used to analyze the data.
Results
The mean age of the patients in group A (n = 43) was 41.9 ± 15.6 years: 33 (76.7%) of these patients were male and 10 (23.3%) were female. The mean age in group B (n = 44) was 43.4 ± 17.3 years: 33 (75.0%) of these patients were male and 11 (25.0%) were female. There was no statistical difference between the groups in terms of demographic characteristics (age, P = .686; sex, P = .851).
In the ESS group (n = 34), the general nasal symptom score evaluated by SNOT-20 showed significantly greater improvement in the xylitol group as compared with the saline group (P = .022; Table 1 ). VAS symptom scores for sneezing (P = .003), headache (P = .02), and facial pain (P = .037) were also more improved in the xylitol group. However, the degree of change in modified Lund-Kennedy score showed no difference between the groups (P = .466). Subanalysis was carried out to evaluate the effect of preoperative existence of nasal polyp in the ESS group. Patients with chronic rhinosinusitis without nasal polyp (CRSsNP) showed results similar to those of the entire ESS group (SNOT-20, P = .012; VAS for sneezing, P = .006; VAS for headache, P = .019; VAS for facial pain, P = .005; Table 2 ). However, patients with chronic rhinosinusitis with nasal polyp (CRSwNP) showed no significant difference between groups, unlike patients with CRSsNP ( Table 3 ). In the septoplasty group (n = 39), the degree of change in general nasal symptoms (NOSE and SNOT-20 scores) showed no significant difference between groups. However, the VAS score for nasal stuffiness showed a significantly greater improvement in the xylitol group versus the saline irrigation group (P = .001; Table 4 ). Within the combined-surgery group, there was no statistically significant difference in any change score between the xylitol and saline groups ( Table 5 ). Among the patients with allergic sensitization (n = 31), rhinorrhea symptoms improved significantly more in the xylitol group than in the saline group (P = .024; Table 6 ).
Symptom Changes between the Xylitol and Saline Irrigation Treatments among Patients Who Underwent Endoscopic Sinus Surgery (n = 34).
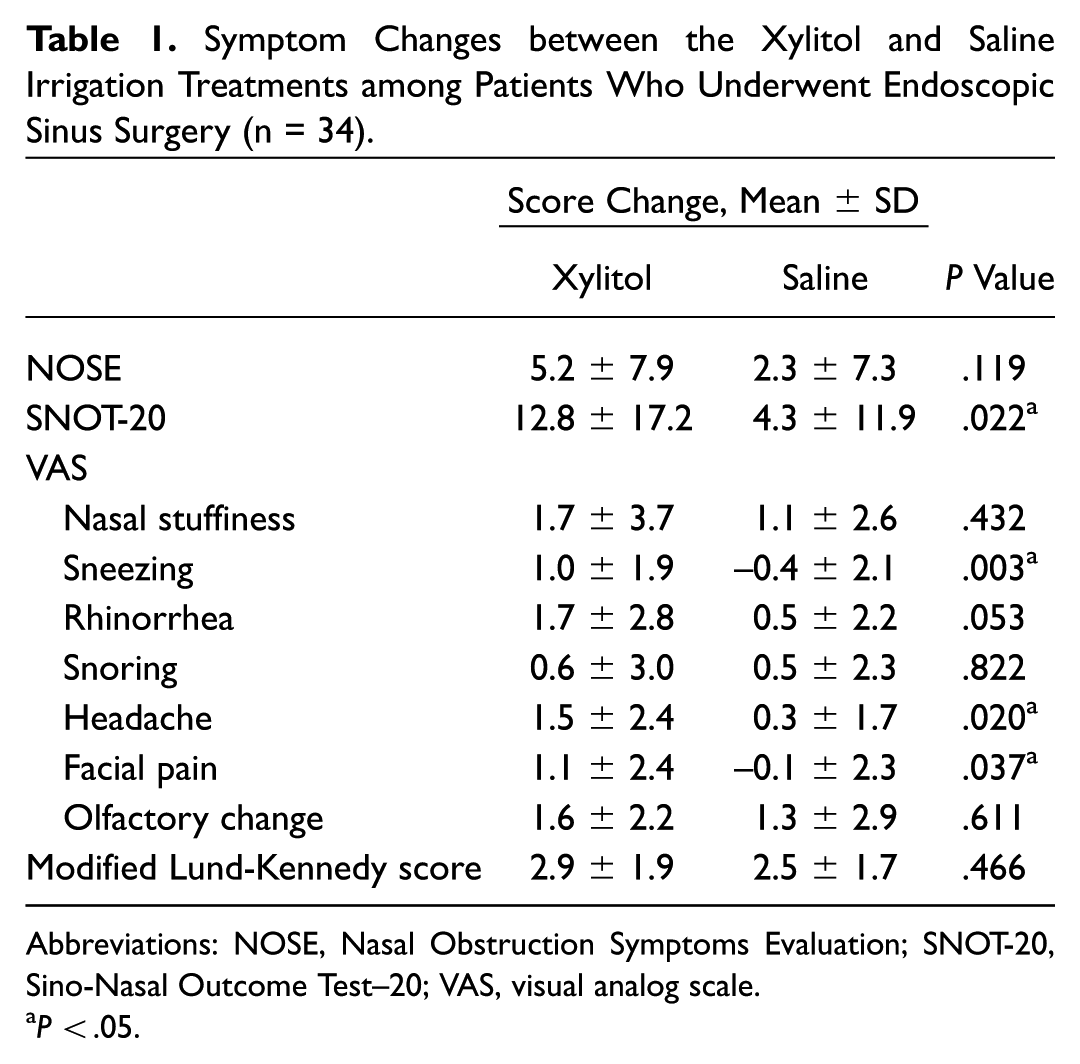
Abbreviations: NOSE, Nasal Obstruction Symptoms Evaluation; SNOT-20, Sino-Nasal Outcome Test–20; VAS, visual analog scale.
P < .05.
Symptom Changes between the Xylitol and Saline Irrigation Treatments among Patients with Chronic Rhinosinusitis without Nasal Polyp Who Underwent Endoscopic Sinus Surgery (n = 26).
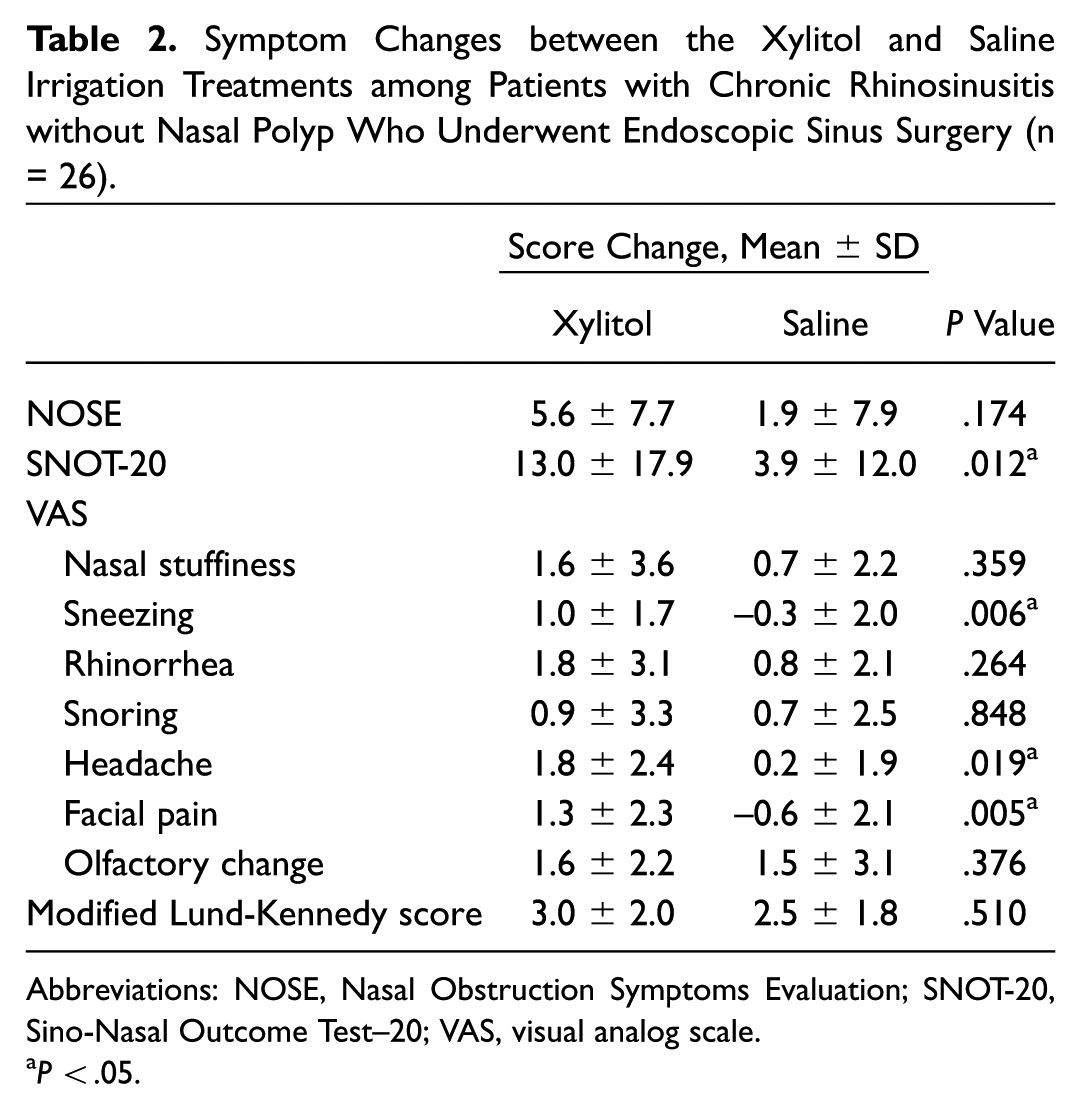
Abbreviations: NOSE, Nasal Obstruction Symptoms Evaluation; SNOT-20, Sino-Nasal Outcome Test–20; VAS, visual analog scale.
P < .05.
Symptom Changes between the Xylitol and Saline Irrigation Treatments among Patients with Chronic Rhinosinusitis without Nasal Polyp Who Underwent Endoscopic Sinus Surgery (n = 8).
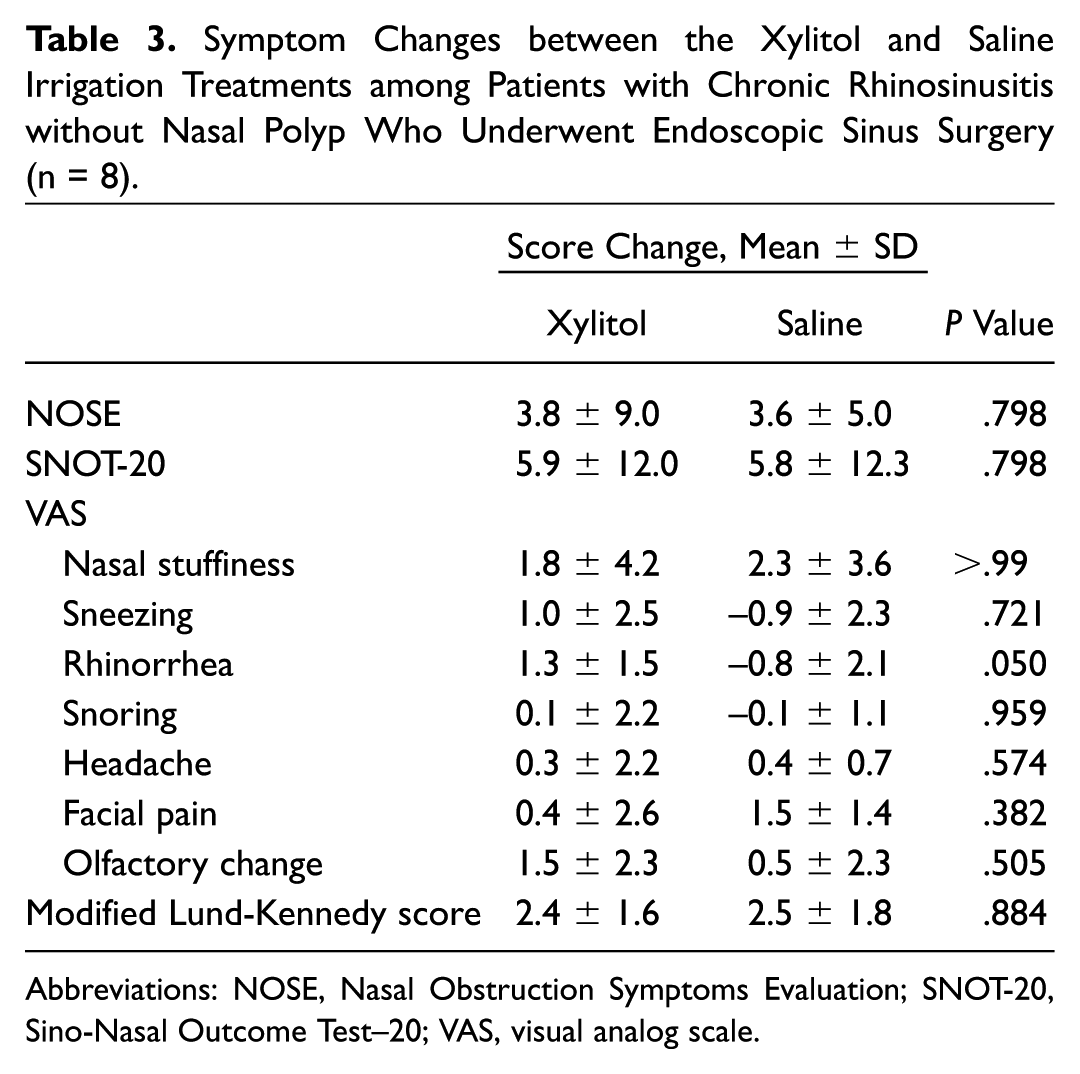
Abbreviations: NOSE, Nasal Obstruction Symptoms Evaluation; SNOT-20, Sino-Nasal Outcome Test–20; VAS, visual analog scale.
Symptom Changes between the Xylitol and Saline Irrigation Treatments among Patients Who Underwent Septoplasty (n = 39).
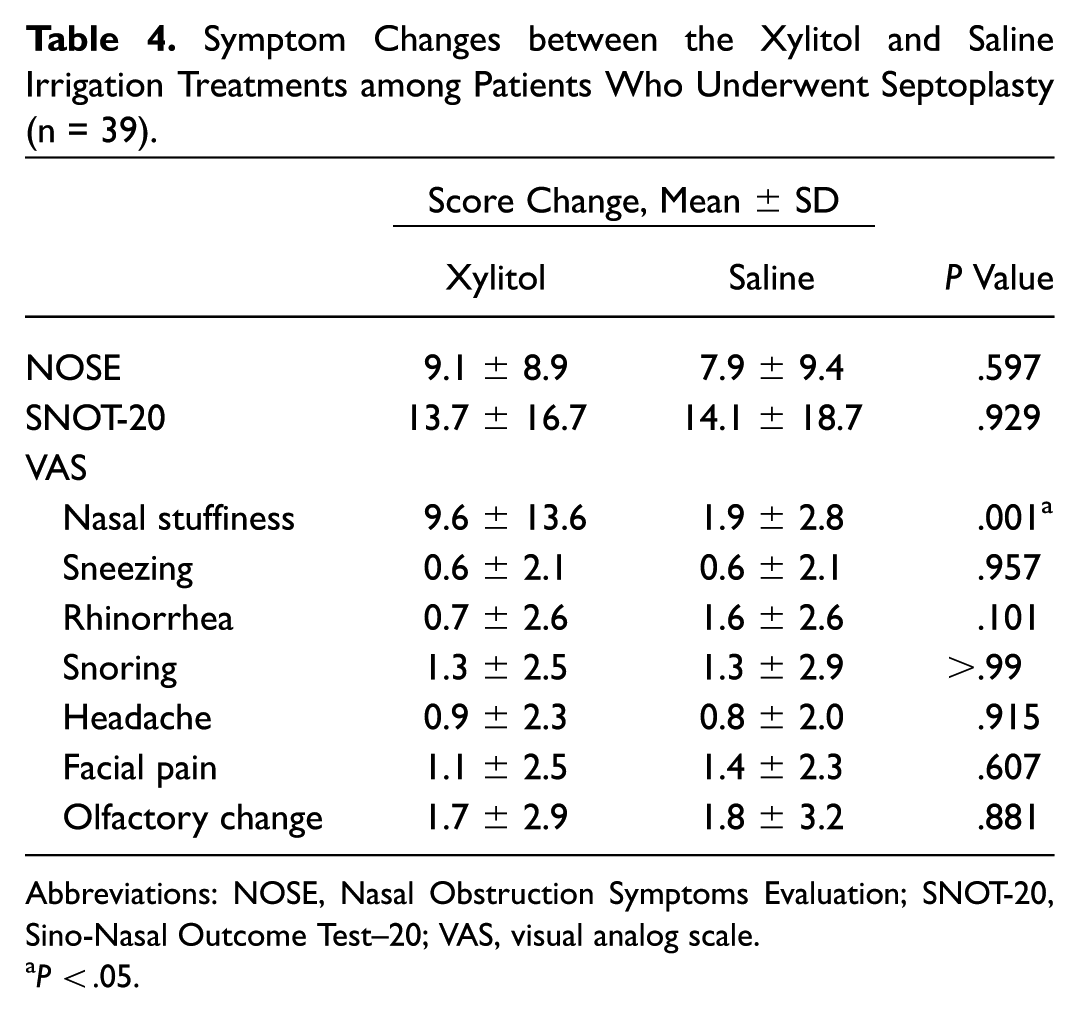
Abbreviations: NOSE, Nasal Obstruction Symptoms Evaluation; SNOT-20, Sino-Nasal Outcome Test–20; VAS, visual analog scale.
P < .05.
Symptom Changes between the Xylitol and Saline Irrigation Treatments among Patients Who Underwent Combined Surgery (n = 14).
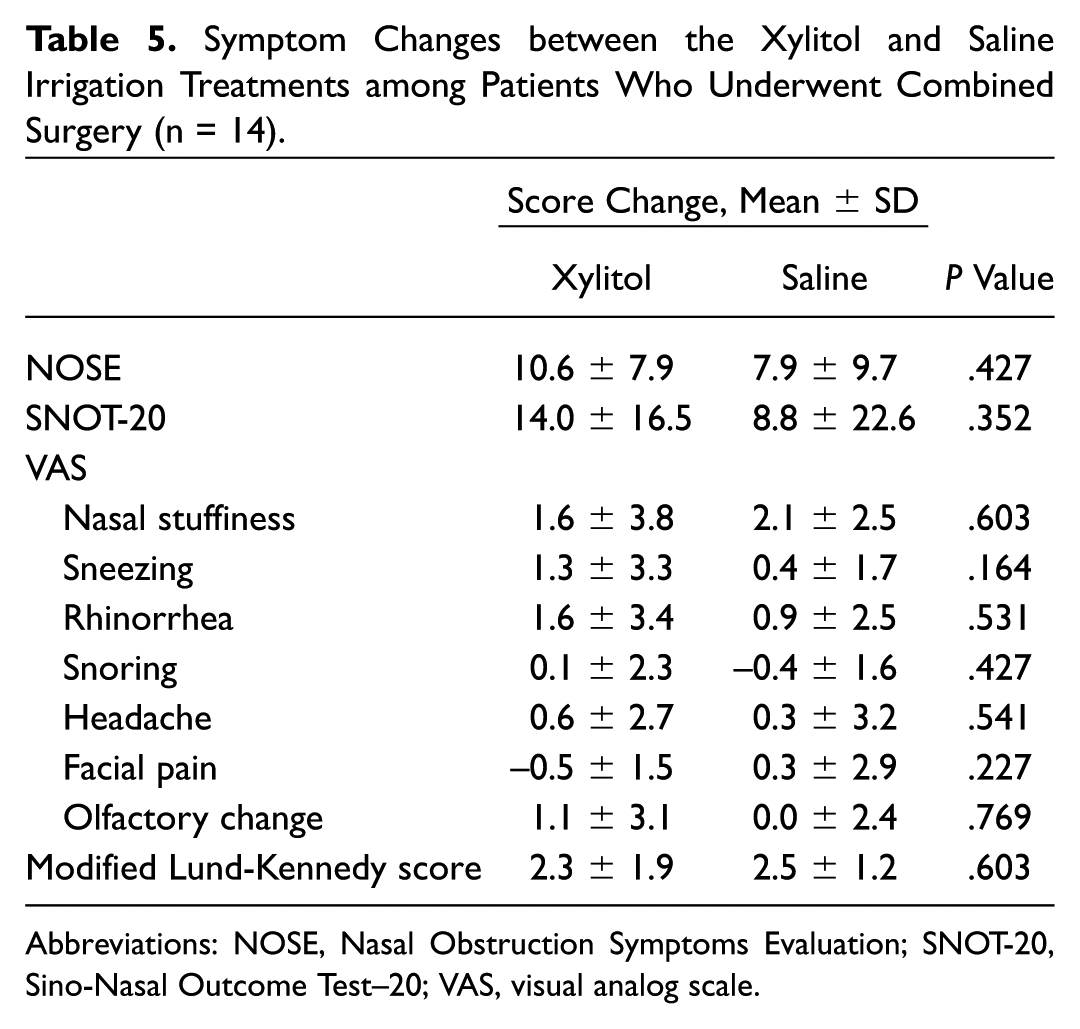
Abbreviations: NOSE, Nasal Obstruction Symptoms Evaluation; SNOT-20, Sino-Nasal Outcome Test–20; VAS, visual analog scale.
Symptom Changes between the Xylitol and Saline Irrigation Treatments among Patients with Allergic Sensitization (n = 31).
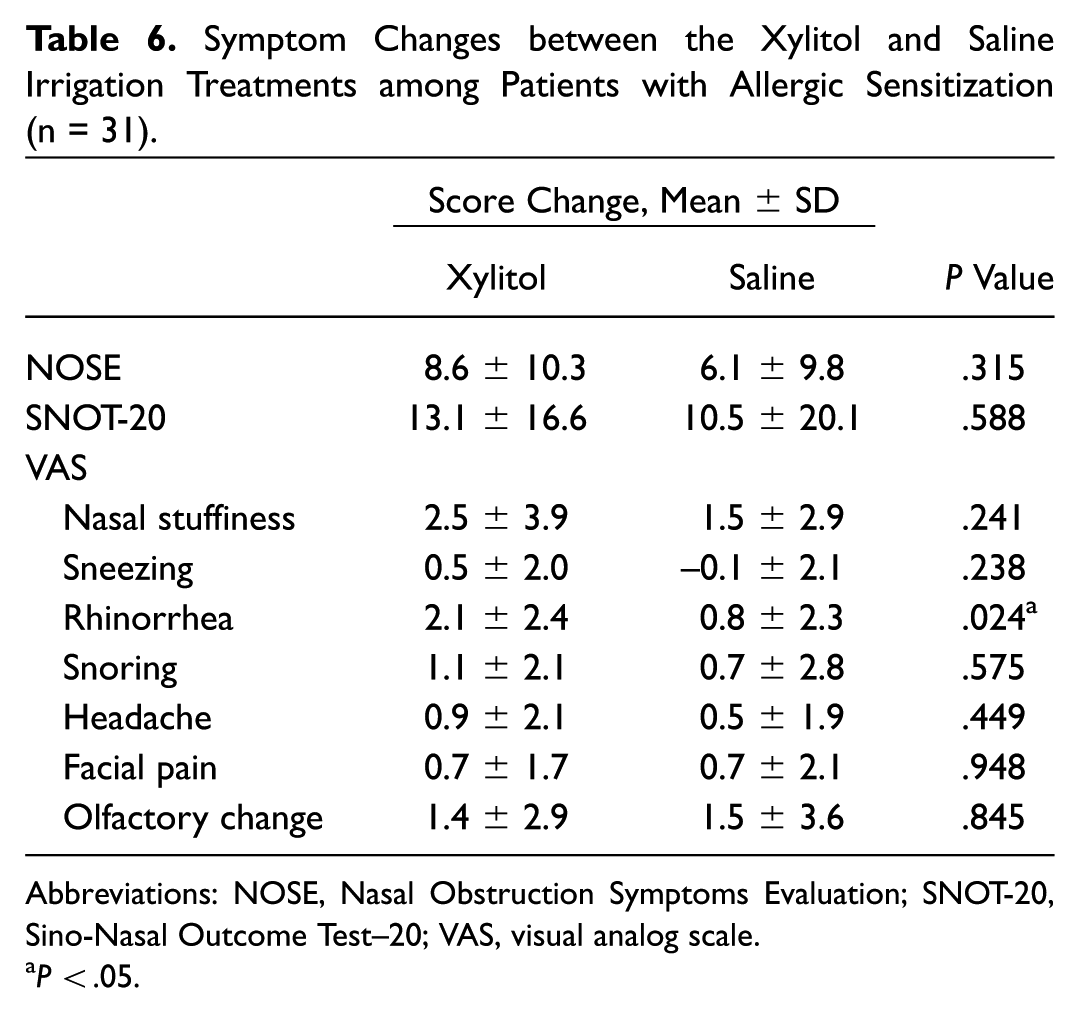
Abbreviations: NOSE, Nasal Obstruction Symptoms Evaluation; SNOT-20, Sino-Nasal Outcome Test–20; VAS, visual analog scale.
P < .05.
The preference survey showed that more than half of the patients in each surgical group preferred xylitol irrigation (septoplasty, n = 22, 56.4%; ESS, n = 22, 64.7%; combined surgery, n = 8, 57.1%; Table 7 ). Regarding safety, no adverse events were reported during or after xylitol irrigation.
Patients’ Nasal Irrigation Preference.
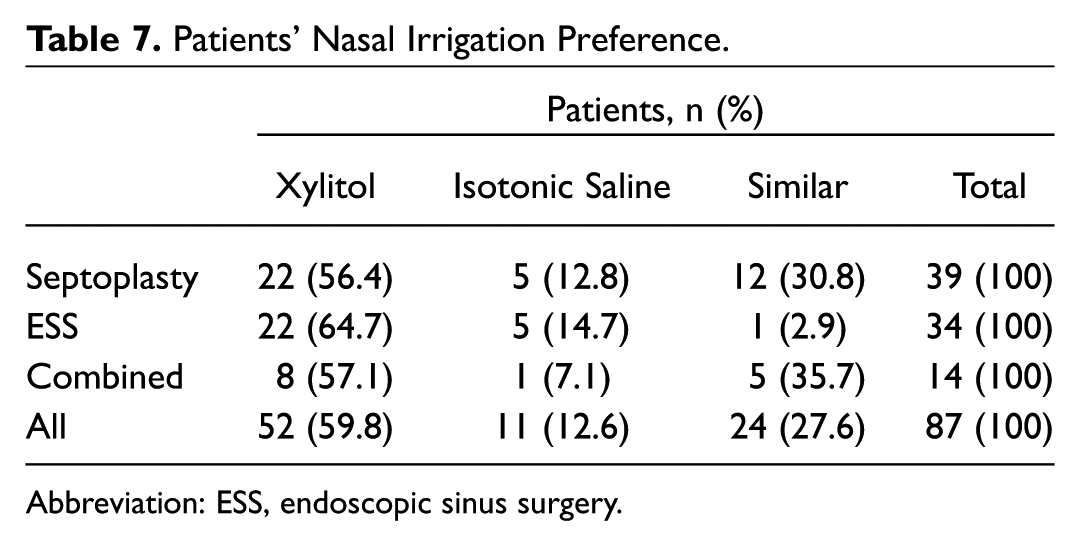
Abbreviation: ESS, endoscopic sinus surgery.
Discussion
There have been several in vitro and in vivo studies on the antibacterial properties of xylitol. Zabner et al 5 reported that the number of nasal coagulase-negative staphylococci significantly decreased after xylitol was sprayed into the nostril. Additionally, xylitol reduced the airway surface liquid salt concentration, thereby suppressing the effects of airway antimicrobial factors and augmenting the innate defense against microorganisms at the airway surface. Kontiokari et al showed that xylitol markedly reduced the growth of alpha-hemolytic streptococci, including Streptococcus pneumoniae. 4 Brown et al reported that xylitol killed bacteria in a rabbit maxillary sinus model with Pseudomonas aeruginosa inoculation. 3 Xylitol showed antiadhesive effects on epithelial cells in the context of the most common bacterial causes of rhinosinusitis (ie, S pneumoniae and Haemophilus influenzae). 6 Xylitol also showed mucolytic effects on chronic rhinosinusitis mucus. 16 A safety assessment was conducted with preclinical and clinical trials. 17 In this context, xylitol irrigation showed good results in the ESS group in this study. However, in subanalysis, xylitol irrigation did not show significant superior results among patients with CRSwNP who received ESS, unlike patients with CRSsNP. Lots of studies reported different disease characters in CRSwNP as compared with CRSsNP. The limited role of antibiotics was well known,18-20 and mucociliary function was changed in CRSwNP. 21 Therefore, the different disease characters of CRSwNP might affect the result of xylitol irrigation.
Bacterial colonization is an important factor in rhinosinusitis and allergic rhinitis. 22 A positive effect of xylitol solution on nasal congestion was demonstrated previously. 23 In this study, we further investigated the effect of xylitol irrigation of patients who had undergone septoplasty and subanalyzed a group of patients with allergic sensitization. For patients who underwent septoplasty, our study showed greater improvement in stuffiness in the xylitol irrigation group versus the saline group. Nasal stuffiness is one of the major postoperative complaints following septoplasty, so xylitol could be of overall benefit for septoplasty. Pastacaldi et al reported a close relationship among staphylococci, staphylococcal superantigens, and allergic respiratory diseases. 22 In this context, xylitol irrigation might be more effective than saline irrigation for improving the rhinorrhea symptoms of patients with allergic sensitization. This study has a limitation in not stratifying beyond type of surgery. In this study, we focused on evaluating the effect of xylitol irrigation after surgery and did not stratify by indication for surgery. Further studies focusing on allergic rhinitis or other sinonasal diseases are needed to determine the clinical utility of xylitol.
For all assessments in this study, equivalent or superior outcomes were seen in the xylitol irrigation group as compared with the saline irrigation group. Patient preference could be an important factor when choosing a nasal irrigation solution.
Conclusion
In this study, we validated a previous study on xylitol nasal irrigation for patients who underwent ESS, by including a larger cohort. Xylitol irrigation is more effective for patients with CRSsNP, and it has a limited role in CRSwNP. Also, we found that xylitol nasal irrigation was useful in postoperative septoplasty care. For patients with allergic sensitization, rhinorrhea showed greater improvement in the xylitol group than in the saline group. In fact, all measured outcomes were equivalent or superior with xylitol irrigation versus saline irrigation. Patient preference is an important factor in the choice of a nasal irrigation solution.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We thank Dr Hyeon Woo Yim (Department of Preventive Medicine, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea) for established crossover study design, calculated sample size, and statistical analysis.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.