
Abstract
Objective
In advanced maxillary sinus cancers treated with surgery and radiotherapy, poor local control rates and the potential for organ preservation have prompted interest in the use of systemic therapy. Our objective was to present outcomes for induction compared to adjuvant chemotherapy in the maxillary sinus.
Study Design
Secondary database analysis.
Setting
National Cancer Database (NCDB).
Subjects and Methods
In total, 218 cases of squamous cell maxillary sinus cancer treated with surgery, radiation, and chemotherapy between 2004 and 2012 were identified from the NCDB and stratified into induction chemotherapy and adjuvant chemotherapy cohorts. Univariate Kaplan-Meier analyses were compared by log-rank test, and multivariate Cox regression was performed to evaluate overall survival when adjusting for other prognostic factors. Propensity score matching was also used for further comparison.
Results
Twenty-three patients received induction chemotherapy (10.6%) and 195 adjuvant chemotherapy (89.4%). The log-rank test comparing induction to adjuvant chemotherapy was not significant (P = .076). In multivariate Cox regression when adjusting for age, sex, race, comorbidity, grade, insurance, and T/N stage, there was a significant mortality hazard ratio of 2.305 for adjuvant relative to induction chemotherapy (confidence interval, 1.076-4.937; P = .032).
Conclusion
Induction chemotherapy was associated with improved overall survival in comparison to adjuvant chemotherapy in a relatively small cohort of patients (in whom treatment choice cannot be characterized), suggesting that this question warrants further investigation in a controlled clinical trial before any recommendations are made.
Cancers of the maxillary sinus are a difficult entity to treat given their tendency to present at advanced stages, biologic heterogeneity, close proximity to vital structures, and poor prognosis. The standard for treatment of maxillary sinus cancers is complete surgical resection with adjuvant radiotherapy with or without chemotherapy. 1 However, the local control rates continue to be relatively poor, and interest in systemic therapy has increased in recent years.2-5 One unanswered question is whether there is a role for induction chemotherapy, with some advocating the use of induction chemotherapy in advanced-stage cancers with the intent of improving organ preservation. The rarity of these cancers has limited the evidence available, although the encouraging results of preliminary single-institution studies have prompted further investigation.6-11 Our objective was to compare survival outcomes in a larger cohort for induction vs adjuvant chemotherapy among patients with maxillary sinus squamous cell cancer treated with surgery, radiotherapy, and chemotherapy.
Materials and Methods
Data Source
Data originated from the National Cancer Database (NCDB), a nationwide clinical surveillance resource data set that includes approximately 70% of all newly diagnosed malignancies in the United States from over 1500 cancer programs. Begun in 1989, the NCDB is a joint project of the American Cancer Society and the Commission on Cancer of the American College of Surgeons. Data collection is carried out under the data use agreement between Commission on Cancer–accredited hospitals and the American College of Surgeons.
Exclusion Criteria
We identified cases of cancer with a primary site in the maxillary sinus between 2004 and 2012 in the NCDB by International Classification of Disease for Oncology, 3rd Edition (ICD-O-3) topography code C31.0. Squamous cell cancers were selected by histology codes 8050 to 8089. Patients were excluded if they were younger than 18 years at the age of diagnosis, had metastatic disease, had previous cancers, had unknown treatment status, or had in situ tumors.
Treatment Definitions
All patients received surgery with adjuvant radiation and either adjuvant or induction chemotherapy. Surgery was further divided into maxillectomy without orbital exenteration and maxillectomy with orbital exenteration. Patients were considered to have radiotherapy if they received external beam radiation. Patients were considered to have received chemotherapy if they received any chemotherapy as part of their first course of therapy, regardless of the type or number of agents.
Adjuvant radiation was defined as radiation that began within 3 months of surgery. Adjuvant chemotherapy was defined as chemotherapy that began after surgery and within 45 days of the start of adjuvant radiotherapy. Induction chemotherapy was defined as chemotherapy administered within 6 months before surgery.
The covariates that were included in multivariate analysis included demographic and clinical variables. For demographic variables, age was classified into 18 to 54, 55 to 64, 65 to 74, and ≥75 years. Race was classified into white, black, and other/unknown. Insurance status was classified into private insurance, Medicare, Medicaid or other government insurance, no insurance, and unknown insurance. Comorbidity was measured by the Charlson/Deyo score, with 0 corresponding to no comorbidity; 1 to cardiovascular disease, dementia, chronic pulmonary disease, rheumatologic disease, peptic ulcer disease, mild liver disease, or diabetes; and 2 to diabetes with chronic complications, hemiplegia or paraplegia, renal disease, moderate or severe liver disease, or AIDS. For clinical variables, grade was classified into poorly differentiated or undifferentiated, moderately differentiated, well differentiated, and unknown grade. Patients were classified by tumor size (T1, T2, T3, T4a, and T4b) and nodal status (N0, N1, N2a, N2b, N2c, N3) according to seventh edition of the American Joint Committee on Cancer staging. 12
Statistical Analysis
The categorical demographic and tumor characteristics of the 2 patient cohorts were compared using Fisher’s exact test, and the continuous propensity scores were compared with a Mann-Whitney U analysis. The primary outcome was all-cause mortality. Rates of local vs radical surgery were compared by 2-sided Fisher’s exact test. Kaplan-Meier analyses and log-rank tests were used to compare overall survival. Multivariate Cox regression was performed to evaluate the association between treatment modality and overall survival when adjusting for other prognostic factors. To further control for possible confounding variables, all analyses were replicated in a 1-to-7 induction-to-adjuvant propensity score–matched cohort (bootstrapping without replacement using a caliper of .05). Statistical significance was determined for all tests at the P < .05 level. Data analysis was performed using SPSS version 25.0 (SPSS, Inc, an IBM Company, Chicago, Illinois). This study was determined to be exempt from review by the Yale Institutional Review Board.
Results
Frequencies of Adjuvant and Induction Chemotherapy
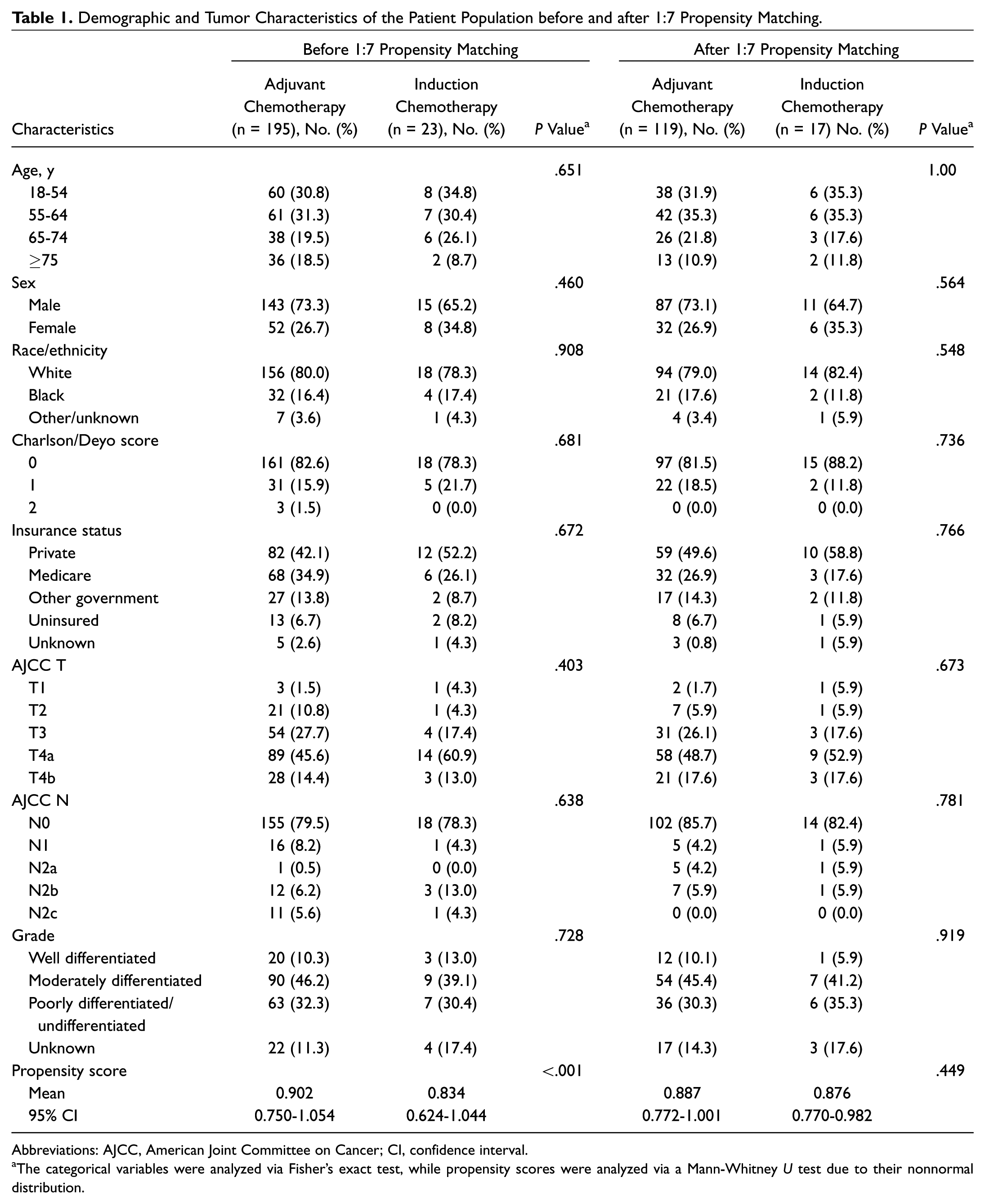
Of 1057 cases of eligible maxillary squamous cell cancer, 291 patients (23.1%) received surgery with chemoradiation. Of the 218 patients with known treatment sequence, 23 patients received induction chemotherapy (10.6%) and 195 adjuvant chemotherapy (89.4%). The demographic characteristics of these patients are described in Table 1 . The patient cohorts did not vary significantly among the demographic and tumor characteristics. Similarly, the demographic and tumor characteristics among the propensity score–matched populations did not vary significantly.
Demographic and Tumor Characteristics of the Patient Population before and after 1:7 Propensity Matching.
Abbreviations: AJCC, American Joint Committee on Cancer; CI, confidence interval.
The categorical variables were analyzed via Fisher’s exact test, while propensity scores were analyzed via a Mann-Whitney U test due to their nonnormal distribution.
Rates of Organ Preservation
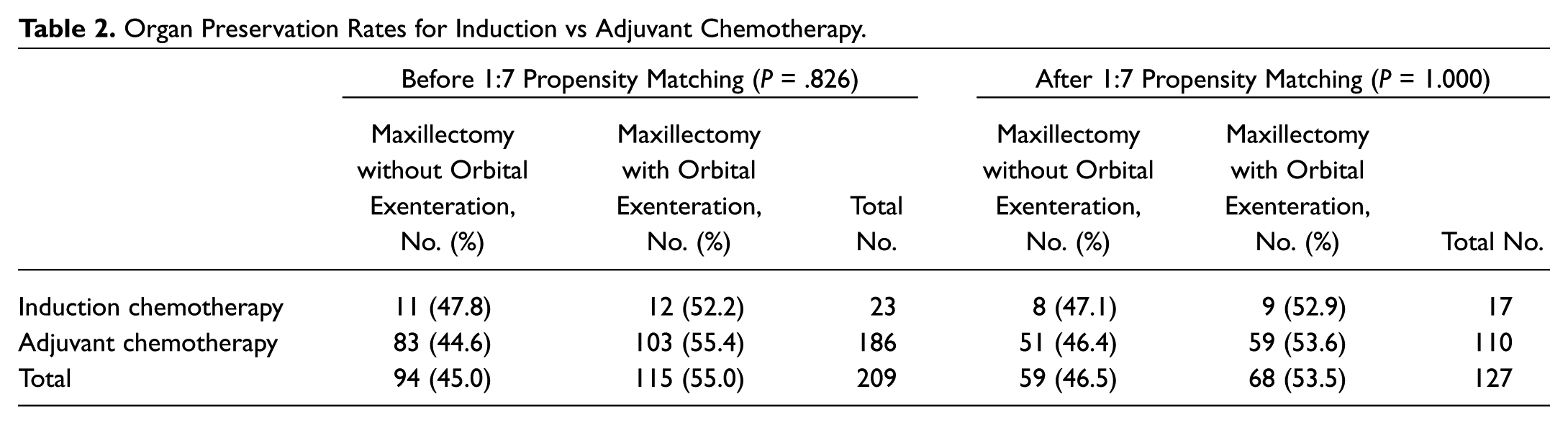
The type of surgery was unknown for 9 patients in the adjuvant chemotherapy cohort before and after 1-to-7 propensity matching. Before propensity matching, for the remaining 209 patients, there were not significant differences seen in the types of surgery received between adjuvant and induction chemotherapy ( Table 2 ). Twelve patients (52.2%) who received induction chemotherapy went on to receive maxillectomy with orbital exenteration and 11 patients (47.8%) maxillectomy without orbital exenteration. In comparison, 103 patients (55.4%) who received adjuvant chemotherapy had maxillectomy with orbital exenteration and 83 patients (44.6%) maxillectomy without orbital exenteration (P = .826). Within the propensity score–matched population, there were also no differences seen in the surgical procedure received based on chemotherapy timing (P = 1.000).
Organ Preservation Rates for Induction vs Adjuvant Chemotherapy.
Survival Outcomes
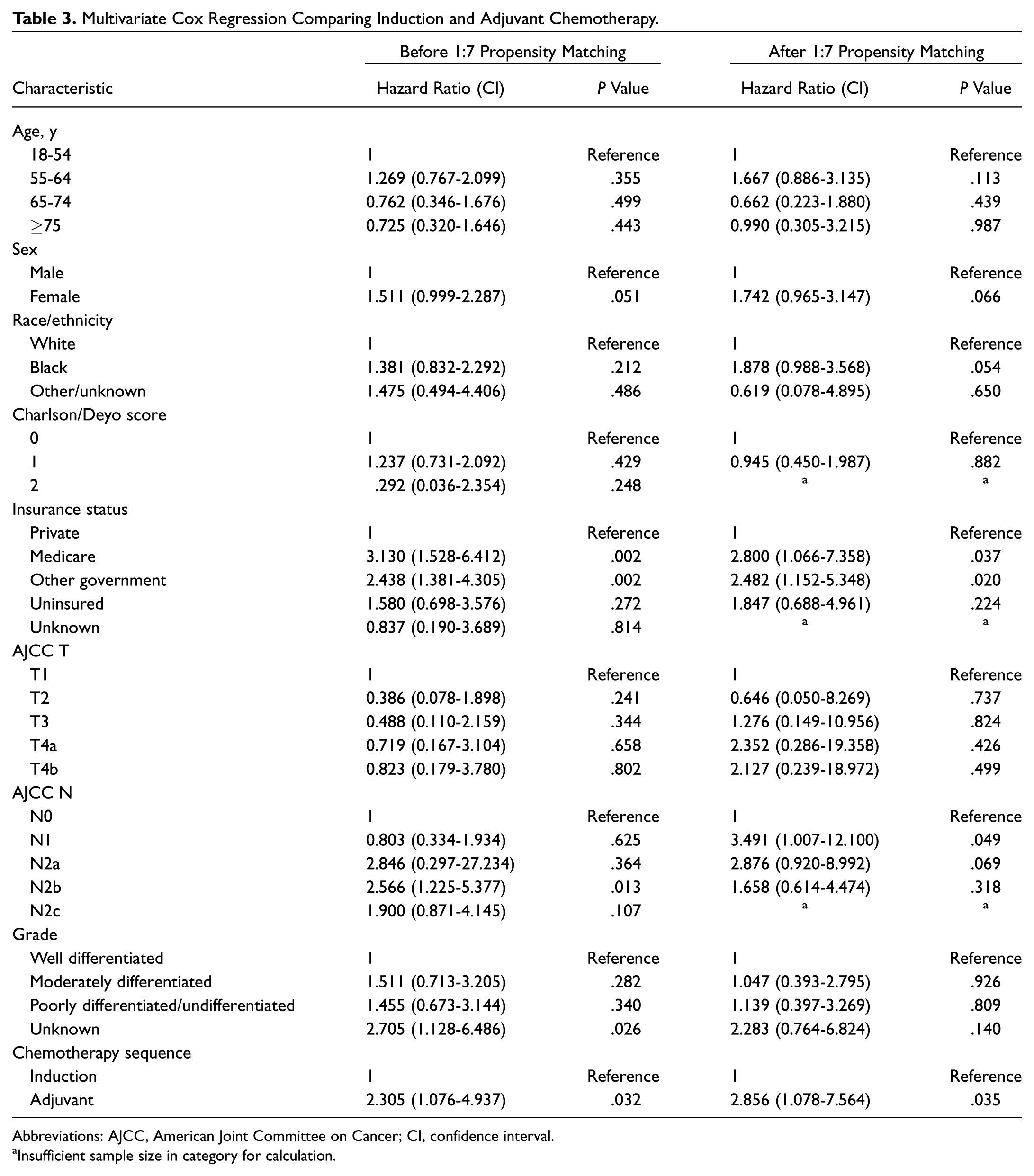
The Kaplan-Meier curves for induction vs adjuvant chemotherapy for the total and propensity score–matched populations are shown in Figure 1 . Within both populations, the log-rank test comparing induction to adjuvant chemotherapy was not significant (total population: P = .076; propensity score–matched population: P = .071). In multivariate Cox regression when adjusting for age, sex, race, comorbidity, grade, insurance, and T/N stage, there was an improved hazard ratio for induction compared to adjuvant chemotherapy (hazard ratio 2.305 for adjuvant relative to induction chemotherapy; confidence interval, 1.076-4.937; P = .032) ( Table 3 ). Similar conclusions are drawn from the propensity score–matched population multivariate Cox regression (hazard ratio 2.856 for adjuvant relative to induction chemotherapy; confidence interval, 1.078-7.564; P = .035).
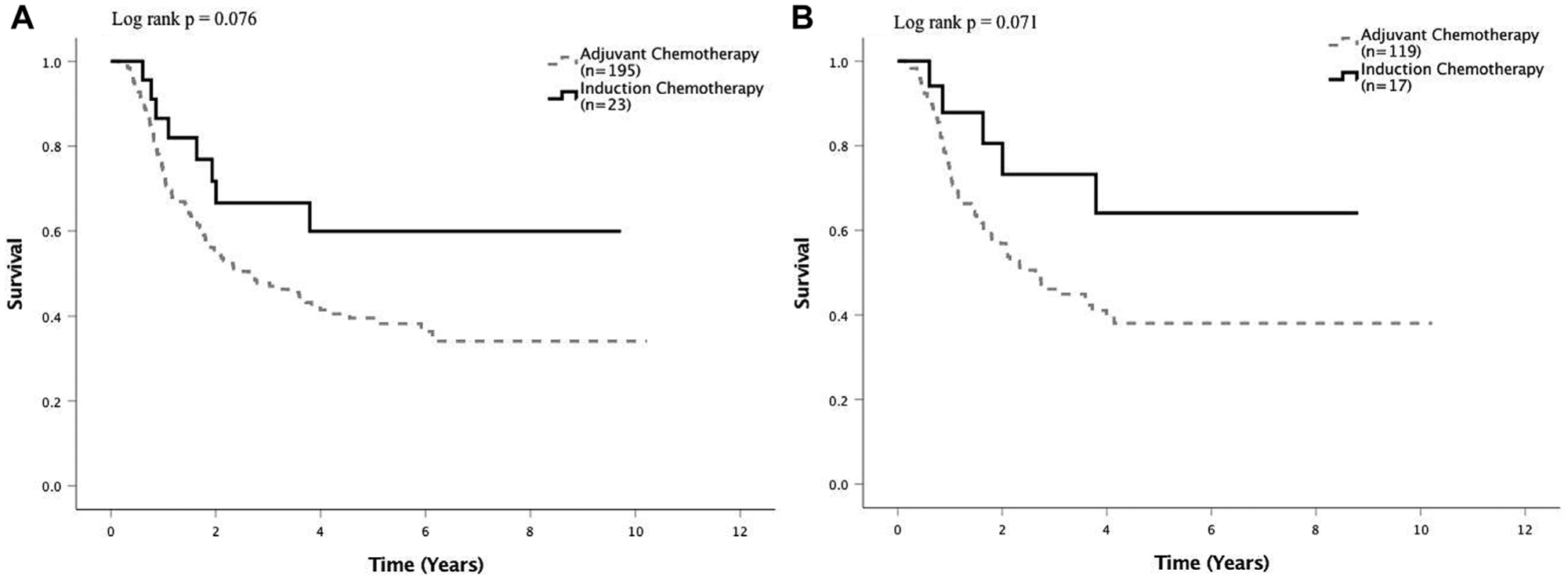
Kaplan-Meier curves for induction and adjuvant chemotherapy (A) before 1-to-7 propensity score matching and (B) after 1-to-7 propensity score matching.
Multivariate Cox Regression Comparing Induction and Adjuvant Chemotherapy.
Abbreviations: AJCC, American Joint Committee on Cancer; CI, confidence interval.
Insufficient sample size in category for calculation.
Discussion
In this study, we compare survival outcomes for 23 patients who received induction chemotherapy before surgery and radiation to 195 patients who received adjuvant chemoradiation after surgery. While limited by the small sample size of the induction chemotherapy group, our findings suggest that there may be improved overall survival associated with induction chemotherapy compared to adjuvant chemotherapy, with a hazard ratio of 2.305 for adjuvant relative to induction chemotherapy when adjusting for other prognostic factors. In addition, the findings are consistent when propensity score matching was performed, which again showed an improved overall survival associated with induction chemotherapy compared to adjuvant chemotherapy (hazard ratio of 2.856 for adjuvant relative to induction chemotherapy). However, there was no difference in frequency of maxillectomy with orbital exenteration between the induction and adjuvant chemotherapy cohorts.
In the induction chemotherapy setting, the largest studies in the maxillary sinus were published by Hanna et al 7 in 2011 and by Noronha et al 9 in 2014. Hanna et al 7 reported on 46 parasinal sinus cancers (31 cases of maxillary sinus) receiving 2- and 3-drug induction chemotherapy with 77% two-year survival and 67% response rate to chemotherapy. Noronha et al 9 reported 41% two-year survival and 39% response rate in 41 patients treated with 2- and 3-drug induction chemotherapy. There have also been other reports, but in general, the evidence has been limited to retrospective single-institution case series without a control cohort.8,10,11
Other than the limitation of the small size of the induction chemotherapy cohort, there are also limitations inherent to a study that uses secondary source data from a large database. There are many centers and physicians represented in this data set, so there is likely variation in how the surgery or chemoradiotherapy was performed. In particular, we were not able to distinguish chemotherapy by the number of agents, types of agents, or duration of treatment. In addition, the database does not indicate why certain treatment choices (ie, induction vs adjuvant chemotherapy) were chosen; although this limitation may be mitigated by propensity matching, there may still be certain patient characteristics that dictate patient care that this small sample size is unable to elucidate. Furthermore, some cases were excluded from multivariate analysis because of missing data values; the effects of these missing data are unknown. The only outcome available was overall survival and not cause-specific survival or locoregional failure rates, so patients may have succumbed to competing causes of mortality. Finally, although we adjusted for patient age, comorbidity, tumor stage, and tumor grade, bias remains a concern with retrospective studies where there may be other unmeasured confounders.
Despite these limitations, our results provide preliminary evidence that induction chemotherapy may be associated with improved survival compared to adjuvant chemotherapy. Induction chemotherapy may contribute to better survival, although we did not find a difference in likelihood of organ preservation. Ultimately, the preliminary positive results suggest that this question warrants further investigation in a controlled clinical trial before any recommendations can be made.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.