
Abstract
Objective
There are no well-defined treatment recommendations for elderly patients with advanced head and neck squamous cell carcinoma. This study aimed to investigate whether aggressive treatment among the elderly translated into better survival outcomes.
Study Design
Retrospective cohort study.
Setting
Single tertiary institution.
Subjects and Methods
Elderly patients (≥60 years) with advanced-stage head and neck squamous cell carcinoma (stage III and IV) treated between January 1991 and May 2014 were reviewed. According to current National Comprehensive Cancer Network guidelines, they were classified to have received standard or substandard treatment. Overall survival (OS), locoregional recurrence-free survival, and distant recurrence-free survival were evaluated.
Results
A total of 355 patients were treated curatively: 194 with up-front surgery and 161 with radiotherapy or concurrent chemotherapy and radiotherapy. Median OS was higher among patients who received standard treatment (42.0 vs 16.0 months, P < .001). On multivariate analysis, standard treatment showed superior OS (P < .001). Use of substandard treatment showed a hazard ratio of 2.09 (95% CI, 1.59-2.74) for poorer OS.
Conclusion
Aggressive standard treatment protocols should be advocated for elderly patients, where comorbidities permit, as they confer better outcomes.
The majority of patients with head and neck squamous cell cancer (HNSCC) present with advanced-stage disease (stage III and IV).1,2 Despite aggressive treatment recommendations by most guidelines (eg, National Comprehensive Cancer Network [NCCN]), 3 recurrence rates remain high, with locoregional relapse among 60% of patients and distant metastasis among 30%. 4 The major paradigm shifts in treating patients with locally advanced disease with curative intent comes from the addition of chemotherapy to treatment regimes. 5 For oral cavity and other surgically managed cancers, 2 landmark studies published in 2004 demonstrated the value in adding cisplatin-based chemotherapy to adjuvant radiotherapy (RT) in high-risk cases.6,7 To date, this remains the gold standard for patients with HNSCC treated with primary surgery, although the definition of “high risk” has undergone some refinement over the years, some of which has been incorporated into the latest iteration of the American Joint Committee on Cancer’s staging system (eighth edition). 8 Similarly, for patients who receive primary radiation therapy, the addition of chemotherapy has been accepted as the treatment paradigm for locally advanced cancers of the oropharynx, larynx, and hypopharynx. Variation to these include moving from induction chemotherapy, based on the study by the Department of Veterans Affairs Laryngeal Cancer Study Group, 9 to concurrent chemoradiation therapy and to protocols incorporating both, with trials demonstrating that surgical management is the gold standard in the primary treatment of oral cavity cancers.10,11 Recent studies also examined the role of biologic agents such as cetuximab in combination with RT in this situation. 12 Several trials are still underway—RTOG 1016 (US), De-ESCALaTE (UK), and TROG 12.1 (Australia)—to determine whether the latter may be a viable option in human papillomavirus (HPV)–associated oropharyngeal cancers, which have a better prognosis to begin with. 13 However, interim analysis of RTOG 1016 reported that RT and cetuximab are associated with worse overall and progression-free survival as compared with RT and cisplatin. 14
One of the major challenges is that the global population is rapidly aging due to the longer life expectancies and lower birth rates of developed nations. 15 As a result, there has been an increase in the prevalence of malignancies among the elderly, including HNSCC, where diagnosis rates among patients >74 years have increased by >20%. 16 Despite treatment guidelines issued by organizations such as the NCCN, 3 there have been no well-defined recommendations for elderly patients. In fact, elderly patients tend to receive suboptimal treatment,17,18 and this happens for a variety of reasons—including physical factors, such as decreased organ function, poor performance status, and underlying medical comorbidities; sociopsychological factors, such as cognitive impairment, financial difficulties, or tendencies to accept death; and clinician bias, where the use of cytotoxic agents is limited among older patients based on fixed chronological cutoffs rather than physiologic status. 19 With improvements in medical care, elderly patients are fitter and healthier than in previous generations, challenging long-held views on withholding cytotoxic agents such as platinum-based chemotherapy. 20 On the contrary, the same biases exist in the very trials from which this evidence is gathered, and so the purported advantage from adding chemotherapy to RT regimes needs to be addressed for older patients specifically.
In this study, our objective was to determine, with defined guidelines, the proportion of elderly patients who received standard treatment for locally advanced HNSCC and whether this aggressive treatment translated into better outcomes.
Methods
Patients
Between January 1991 and May 2014, patients aged ≥60 years who were diagnosed with advanced-stage HNSCC (stage III and IV) at a single tertiary institution (National Cancer Centre Singapore) were retrospectively reviewed. Patients included had no prior malignancy or treatment, were treated with curative intent, and had sufficient follow-up data. All treatment decisions were made during weekly multidisciplinary tumor board meetings. Patients were divided into 2 groups according to treatment received: (1) up-front surgery with adjuvant treatment or (2) radical RT or concurrent chemotherapy and RT (CRT). Elderly patients were defined as patients aged ≥60 years, as the median age of patients in our database was 61 years. This cohort was further subdivided into 2 groups based on an age cutoff of 70 years. Cases were also divided according to tumor subsites—larynx, oral cavity, oropharynx, and hypopharynx. This study was approved by the Singhealth Centralized Institutional Review Board.
Standard and Substandard Treatment
The definition of standard versus substandard treatment was made per the NCCN guidelines for locally advanced HNSCC. 3 For the up-front surgery group, patients were classified as having standard treatment if (1) they received adjuvant RT, (2) their surgical histology showed clear margins and no extracapsular spread, or (3) they received concurrent CRT (indicated for patients with close/positive margins and extracapsular spread). Conversely, treatment was deemed substandard if they did not receive RT when indicated or if chemotherapy was omitted when the indications favored adjuvant CRT. For the primary RT/CRT group, patients with stage III/IV disease were classified as having standard treatment if they received induction chemotherapy, followed by RT or concurrent CRT. All other treatment plans, including RT without the addition of chemotherapy, were classified as substandard.
Data Processing and Analysis
Data analysis was carried out with SPSS 21 (IBM, New York, New York). Overall survival (OS), locoregional recurrence-free survival (LRFS), and distant recurrence-free survival (DRFS) rates were analyzed via the Kaplan-Meier method, and comparisons were made with the log-rank test. OS was calculated from date of diagnosis to date of death due to any cause. LRFS was calculated from date of diagnosis to date of first locoregional recurrence. DRFS was calculated from date of diagnosis to date of first distant metastatic recurrence. OS, LRFS, and DRFS were compared for patients receiving standard versus substandard treatment in the entire cohort as well as the 2 age groups: <70 and ≥70 years. OS, LRFS, and DRFS were also compared for patients receiving standard versus substandard treatment in both age groups according to 4 subsites: oropharynx, larynx, oral cavity, and hypopharynx. Predictive factors, such as site, age category, and treatment received, were analyzed by univariate and multivariate Cox regression model. P value <.05 was taken to be significant.
Results
Baseline Characteristics
Between January 1991 and May 2014, 355 elderly patients (≥60 years old) presented to our institution with advanced-stage HNSCC. The mean age was 70.0 ± 7.4 years (range, 60-95 years); 277 (78.0%) were men; and 155 (43.7%) had a significant smoking history of at least 10 pack-years. Primary sites included the larynx (n = 75, 21.1%), oral cavity (n = 146, 41.1%), oropharynx (n = 88, 24.8%), and hypopharynx (n = 46, 13.0%). A total of 194 were treated with up-front surgery, and 161 were treated with radical RT/CRT with curative intent. In the cohort treated with up-front surgery, 77 patients received adjuvant RT; 26 received adjuvant CRT; and 91 received no adjuvant treatment. In the nonsurgical cohort, 59 patients were treated with radical RT, while 102 received CRT. Between patients aged <70 years and ≥70 years, baseline characteristics were similar, except for the proportion given standard treatment. For patients aged <70 years, 67.6% were given standard treatment, as opposed to 45.9% for patients aged ≥70 years (P < .001; Table 1 and Figure 1 ).
Baseline Clinical Characteristics of Entire Cohort Comparing Proportions according to Age.
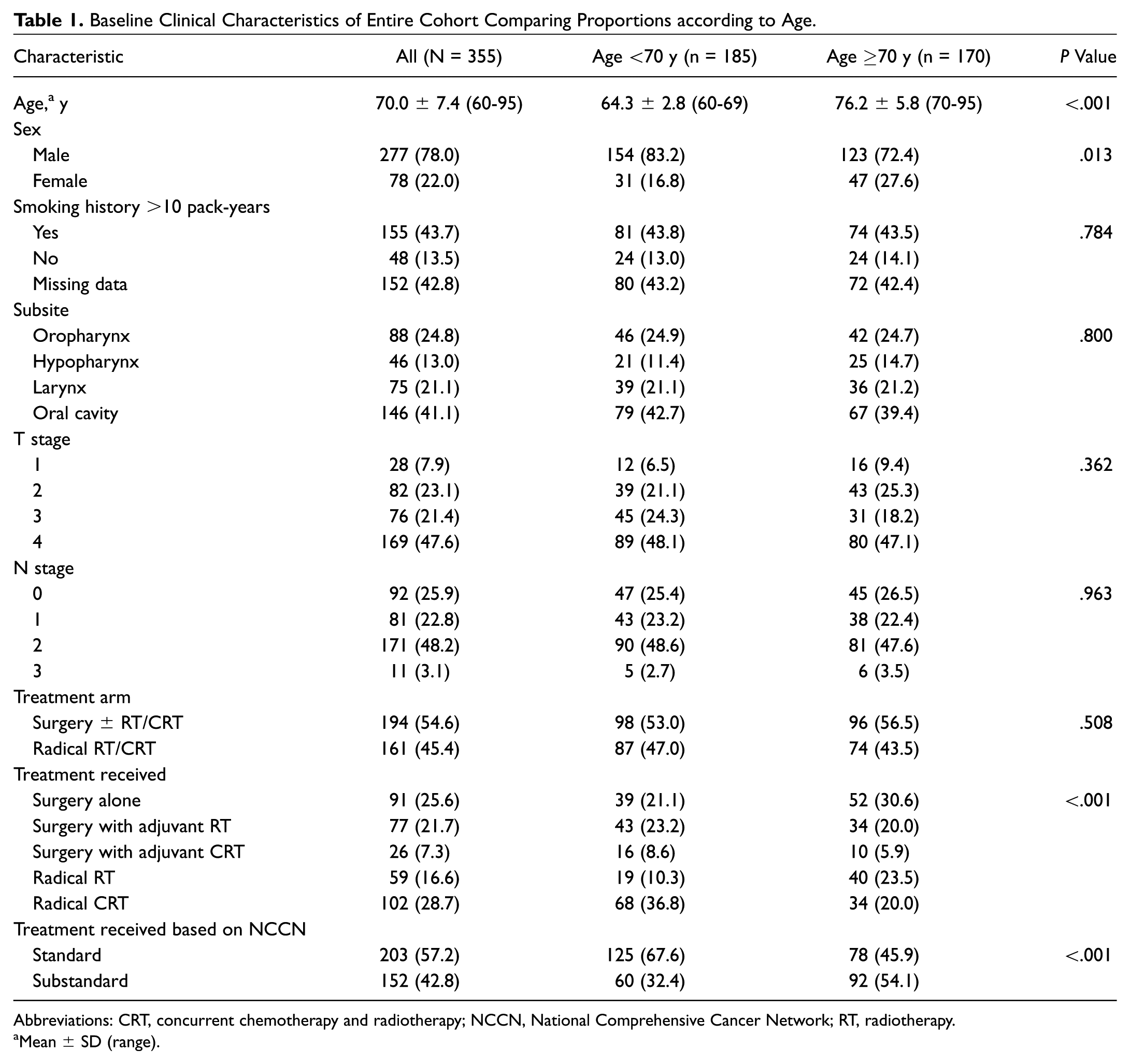
Abbreviations: CRT, concurrent chemotherapy and radiotherapy; NCCN, National Comprehensive Cancer Network; RT, radiotherapy.
Mean ± SD (range).
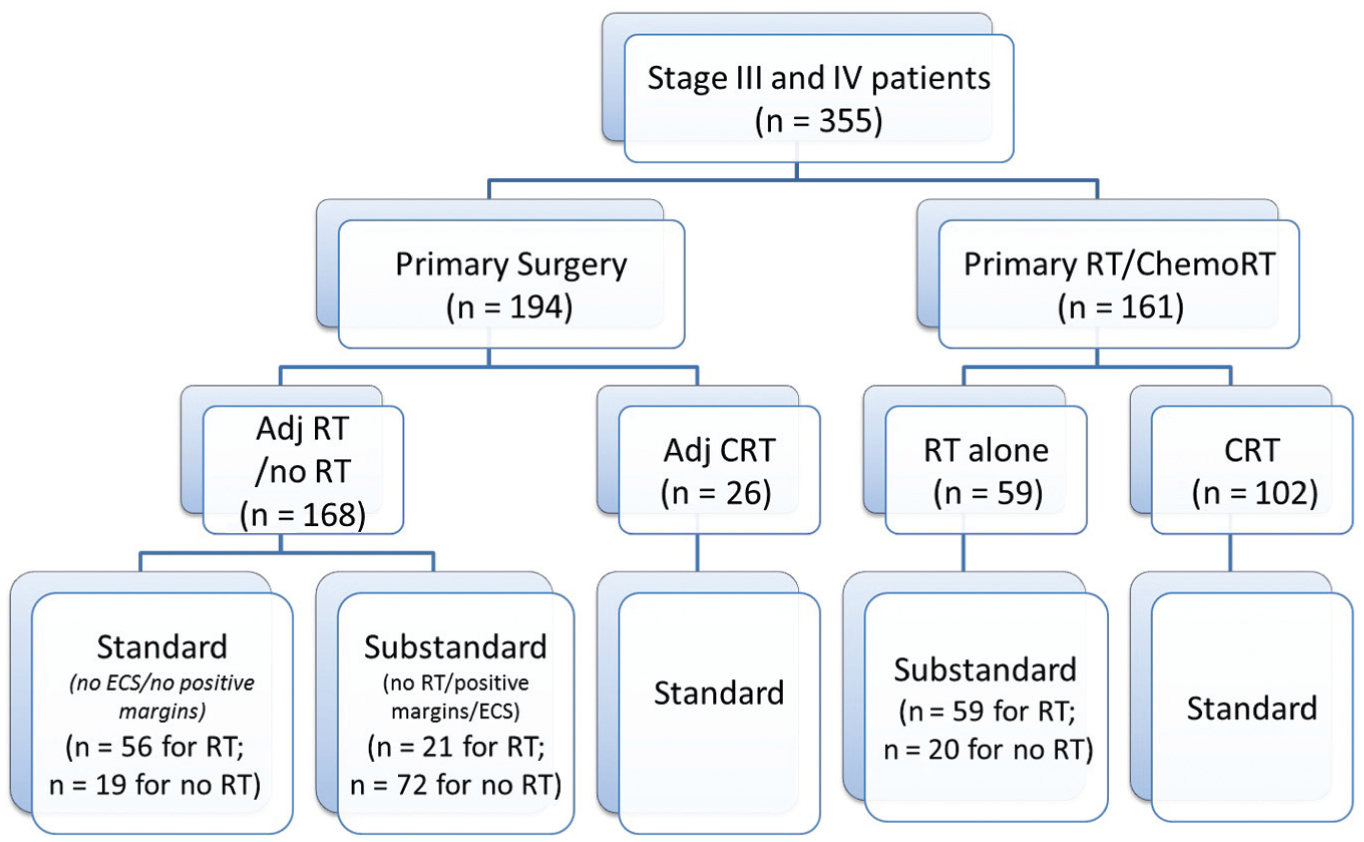
Flowchart depicting patients stratified according to respective treatment arms. Adj, adjuvant; CRT, chemotherapy and radiotherapy; ECS, extracapsular spread; RT, radiotherapy.
Comparing Standard versus Substandard Treatment
There was no significant difference in the median date of diagnosis among patients who received standard versus substandard treatment (P = .432). Patients who received substandard treatment were significantly older (72.7 ± 8.1 years vs 68.0 ± 6.2 years, P < .001). Furthermore there was a significantly greater number of patients aged ≥80 years who received substandard treatment (22.4% vs 4.0%, P < .001; Table 2 ).
Comparison of Cohort Receiving Standard Treatment versus Substandard Treatment.
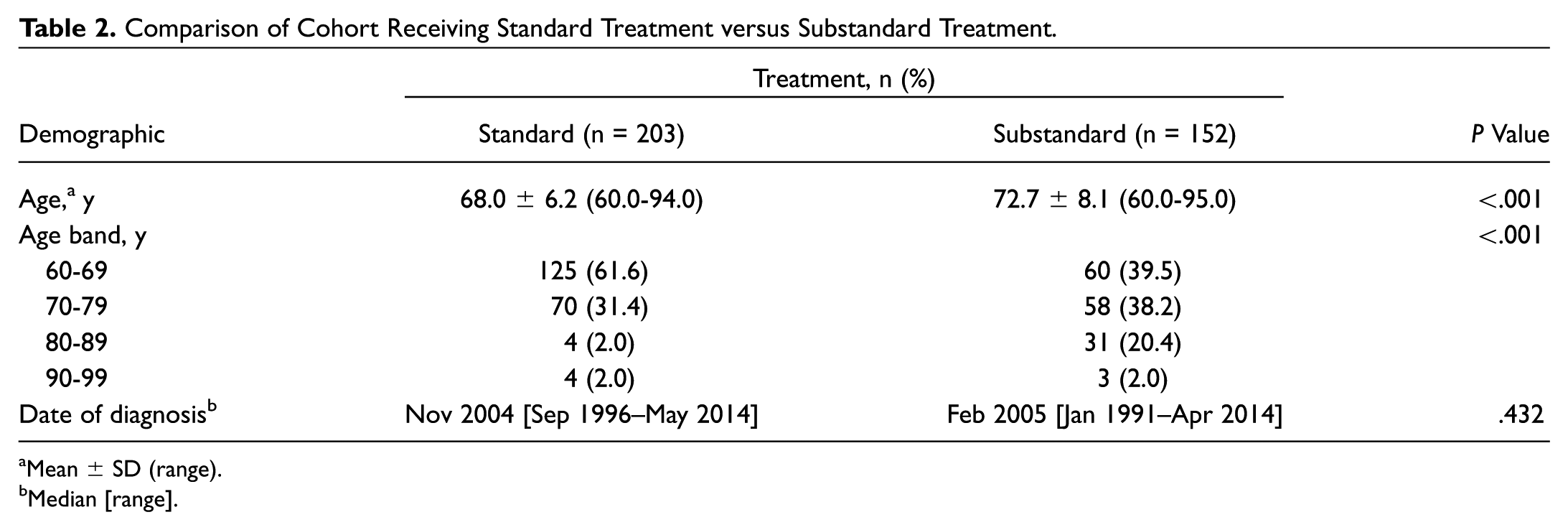
Mean ± SD (range).
Median [range].
Comparing Survival across Entire Cohort
There was no significant difference in median OS, LRFS, and DRFS when patients were stratified according to age (P = .073, P = .503, and P = .797, respectively). Among patients <70 years old, the median OS was 31.0 months (95% CI, 19.5-42.5), and for patients ≥70 years, the median OS was 28.0 months (95% CI, 15.1-40.9; P = .073). However, across the entire cohort, the median OS was higher among patients who received standard treatment (42.0 months; 95% CI, 26.9-57.1) rather than substandard treatment (16.0 months; 95% CI, 11.7-20.3; P < .001; Figure 2 ). Similarly, the LRFS was also significantly better for patients who received standard treatment (P = .002), while no difference was seen on distant metastasis rates (P = .783).
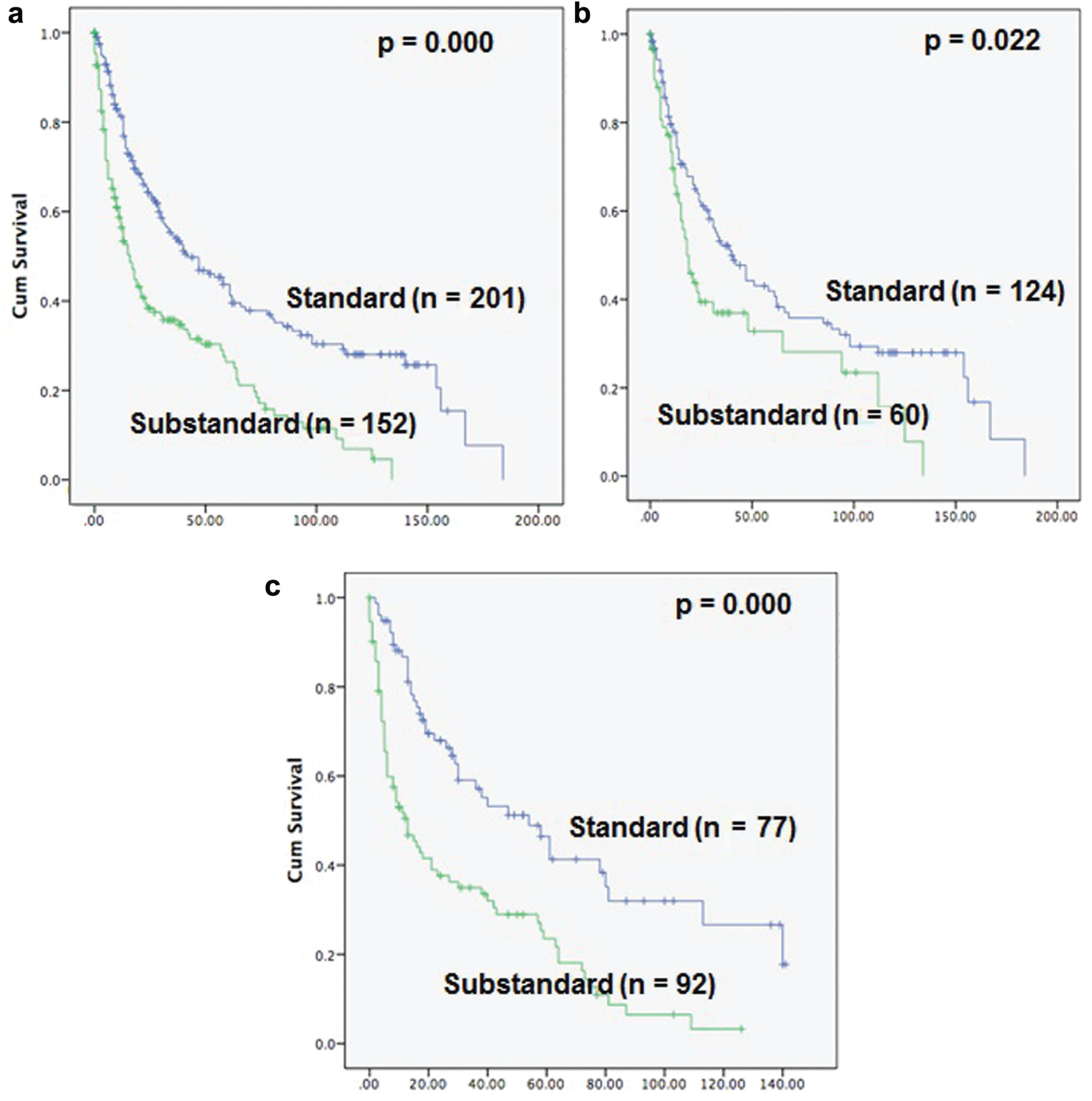
Curves showing significantly better overall survival with standard treatment for the (a) entire cohort and by subgroup: (b) <70 years and (c) ≥70 years.
Patients aged <70 years who received standard treatment had significantly better OS and LRFS (P = .022 and P = .001, respectively), but no difference in DRFS was observed (P = .950). Median OS was 40.0 months (95% CI, 27.3-52.7) with standard treatment, as opposed to 18.0 months (95% CI, 12.4-23.6) with substandard treatment. Patients aged ≥70 years who received standard treatment had significantly better OS (P < .001); however, LRFS and DRFS were not significantly different (P = .214 and P = .648, respectively). For patients ≥70 years, median OS was 54.0 months (95% CI, 32.8-75.2) with standard treatment versus 13.0 months (95% CI, 6.8-19.2) with substandard treatment.
There were no significant difference in OS, LRFS, and DRFS for patients in both treatment arms—whether they received up-front surgery or definitive radical RT/CRT (P = .162, P = .858, and P = .569, respectively).
Analyses by Subsites
In a comparison of survival among the 4 subsites (larynx, oral cavity, oropharynx, and hypopharynx), there were significant differences in OS and DRFS (P = .019 and P < .001, respectively), whereas LRFS was not significantly different (P = .053). Patients with laryngeal squamous cell cancer (SCC) had a median OS of 48.0 months (95% CI, 27.9-68.1); oral cavity SCC, 35.0 months (95% CI, 20.9-49.1); oropharyngeal SCC, 17.0 months (95% CI, 9.7-24.3); and hypopharyngeal SCC, 18.0 months (95% CI, 12.0-24.0).
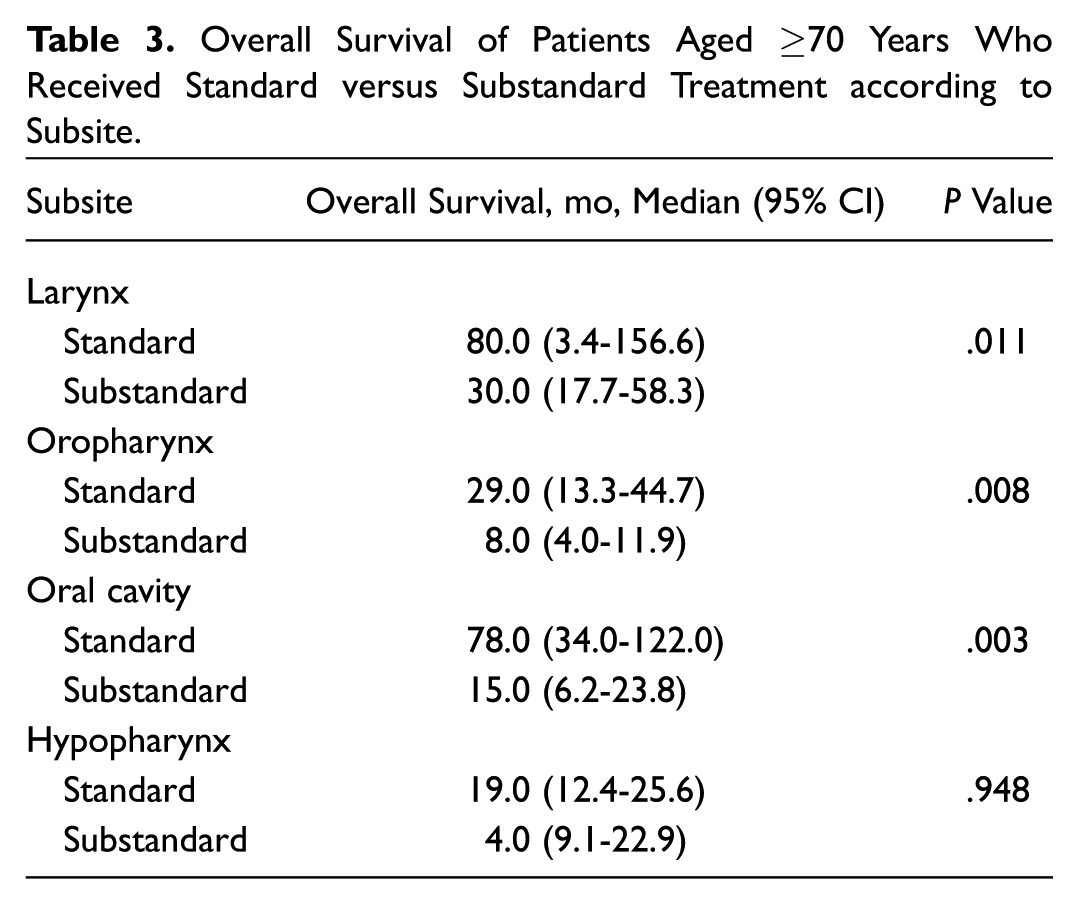
Analysis of patients aged ≥70 years based on subsite showed that standard treatment resulted in better OS for oropharyngeal, laryngeal, and oral cavity cancers but not for hypopharyngeal cancers. For oropharyngeal cancer, standard treatment resulted in significant improvement in OS (P = .008), with no difference in LRFS and DRFS (P = .609 and P = .130). The percentage of patients with oropharyngeal cancer who were smokers was 60.2%. For laryngeal SCC, patients who received standard treatment had significantly better OS and LRFS (P = .011 and P = .019), while DRFS was not different (P = .197). For oral cavity SCC, patients who received standard treatment had significantly better OS (P = .003) but no significant improvement in LRFS or DRFS (P = .320 and P = .266, respectively). For hypopharyngeal cancer, there was no significant difference in OS, LRFS, or DRFS with standard treatment (P = .948, P = .052, and P = .391, respectively; Table 3 ).
Overall Survival of Patients Aged ≥70 Years Who Received Standard versus Substandard Treatment according to Subsite.
Multivariate Analysis
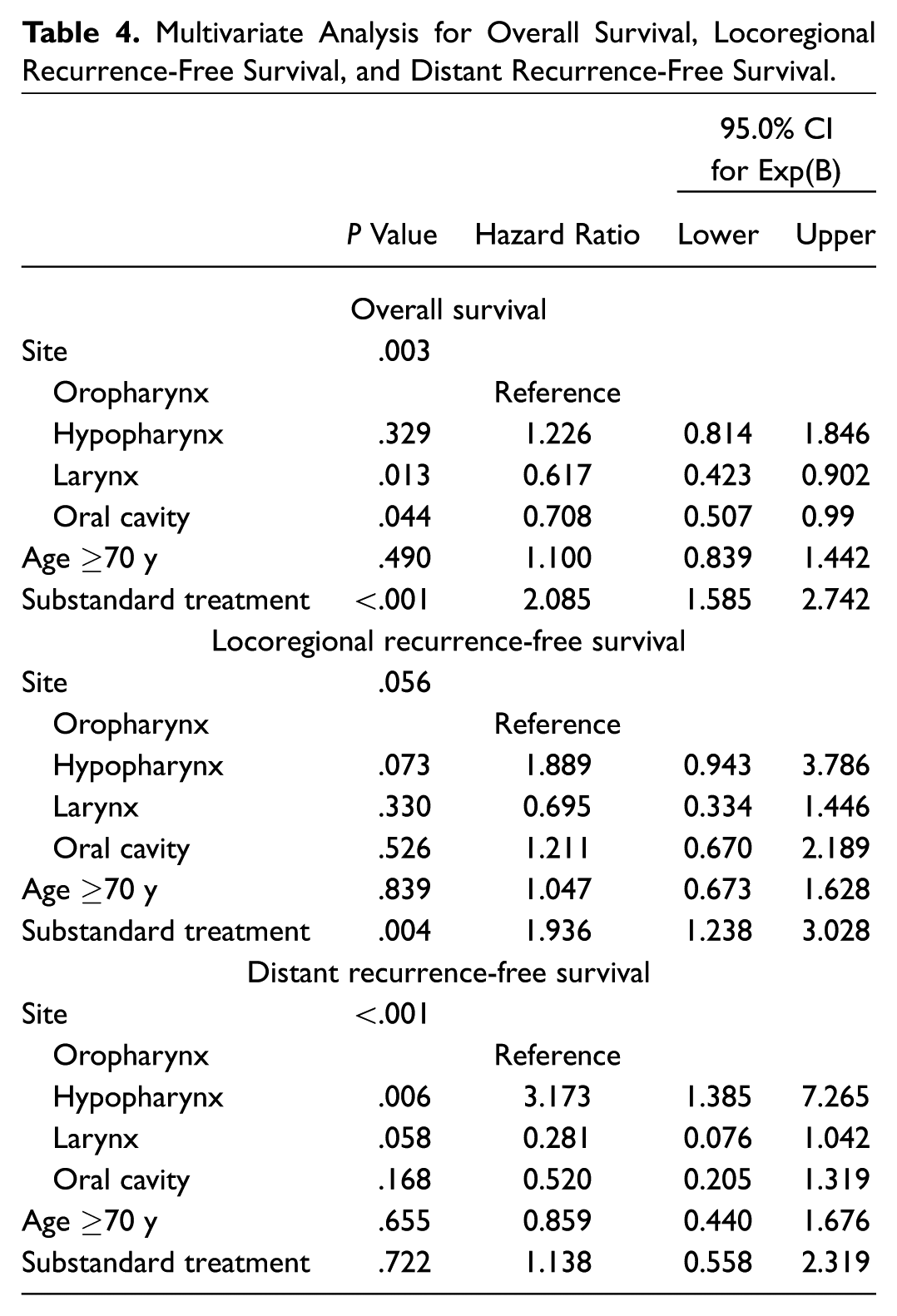
Multivariate analysis was performed with variables including standard of treatment (standard vs substandard), tumor site, and age. Standard treatment showed significantly superior OS and LRFS (P < .001 and P = .004, respectively) but no significant difference in DRFS (P = .722). The hazard ratio was 2.09 (95% CI, 1.59-2.74) for poorer OS and 1.94 (95% CI, 1.24-3.03) for poorer LRFS when patients received substandard treatment. Site of SCC showed a significant difference in OS and DRFS on multivariate analysis (P = .003 and P <.001, respectively) but no significant difference in LRFS (P = .056). Age did not have a significant effect on OS, LRFS, and DRFS (P = .490, P = .839, and P = .655, respectively; Table 4 ).
Multivariate Analysis for Overall Survival, Locoregional Recurrence-Free Survival, and Distant Recurrence-Free Survival.
Discussion
Clinical guidelines are generally derived from high-level clinical trials, which provide the level of evidence to make clinical decisions and institute standardized treatment regimes. Unfortunately, these trials are usually conducted in an “optimal” environment with extensive support networks biased toward ideal patient candidates. More importantly, their application to “real world” scenarios can be less than ideal, none more so when dealing with aging patient demographics in the oncology setting. In HNSCC, the proportion of elderly patients in many trials are significantly lower than that in routine clinical practice; hence, it is imperative to analyze data on the effect of these practices on a less studied patient population.5,21 A tendency to undertreat elderly patients has been reported—where despite similar performance status and comorbidities, patients aged ≥70 years were more commonly treated with less aggressive strategies than were their younger counterparts. 19 As such, future research should test the effect of what is deemed “standard treatment” via careful analysis of real-world databases focused on this specific population.
In this study, the patient cohort represents a busy tertiary-level center practice, where treatment regimes changed during the study period, despite the definitions of standard versus substandard care. For example, for patients who underwent primary surgery, the recommended treatment in the 1990s was adjuvant RT, which then progressed to CRT after the initial Cooper/Bernier trials6,7 for all patients with locally advanced disease, and this changed again with an understanding that the strongest risk factors in this setting were positive margins and/or extranodal extension. Furthermore, even with the knowledge of what standard treatment entailed, there was a tendency to treat elderly patients with less aggressive treatment, as demonstrated by the mean age of those receiving standard treatment (68.0 years) versus those receiving substandard treatment (72.7 years, P < .001). Hence, for patients who underwent primary surgery, 77 received adjuvant RT, while only 26 received adjuvant CRT ( Figure 1 ). These differences in management principles afforded us the different cohorts across which we could compare implementing current best practices in this context.
The most important findings in this study relate to the fact that outcomes were improved with standard recommended treatment, which often meant the inclusion of concurrent chemotherapy to radiation. Even when the elderly cohort was divided by age to <70 and ≥70 years, the difference in OS was dramatic when patients were treated aggressively with curative intent. Median OS with standard treatment was 40.0 versus 18.0 months among those <70 years (P = .022) and 54.0 versus 13.0 months among those ≥70 years (P < .001). Data supporting this approach were evident even for patients ≥70 years of age and could be extended to most subsites, including oropharynx, larynx, and oral cavity, although not as significant in hypopharyngeal cancers. In addition, multivariate analysis showed that treatment type, whether standard or substandard, had the greatest effect on OS, LRFS, and DRFS. These data support that elderly patients show significant benefit from the institution of standard treatment practices, particularly the addition of adjuvant chemotherapy, challenging the traditional belief that the latter may be detrimental to this group of patients. Certainly, this could be refined with further changes in staging, other prognostic factors (eg, HPV status), and newer treatment regimes, including the use of biologic agents such as cetuximab.22,23
The majority of patients with oropharyngeal SCC were diagnosed prior to the era wherein HPV was found to have a strong association; hence, this would unlikely change the results of the study. The prevalence of HPV-associated oropharyngeal SCC has been shown to be much lower in Asia than in the West. A recent meta-analysis by Shaikh et al indicated that the prevalence of HPV of any subtype was approximately 36% in the Asia-Pacific region. 24 This differed from the prevalence in the United States, which was approximately 71.7% from 2000 to 2004. 25 Furthermore, the percentage of patients with oropharyngeal SCC in our cohort who had significant smoking history was 60.2%. As such, the etiology of the majority of oropharyngeal SCC among our patients was less likely HPV. Finally, emerging data from RTOG 1016 suggest that replacing cisplatin with cetuximab was detrimental for patients with HPV-associated cancers and that avoiding cytotoxic chemotherapy is not an appropriate de-escalation strategy. 14
The findings of this study were supported by a large retrospective study by Amini et al, 26 who reported that CRT was associated with longer OS for patients ≤81 years who had low comorbidity scores and either T1-2/N2-3 or T3-4/N0-3 disease versus RT alone. This adds to the evidence that there may be a role for advocating standard treatment in a select group of elderly patients.
Conversely, in a meta-analysis on the effect of chemotherapy on HNSCC, Pignon et al reported a decreasing effect of chemotherapy on survival with increasing age. 5 This was attributed to older patients dying more frequently from other causes instead of HNSCC, thus making it difficult to observe survival benefit in patients. In addition, a randomized trial by Bonner et al supported this finding, which reported that the combination of RT and cetuximab was beneficial only in distinct subgroups of patients <65 years old with good performance status (Karnofsky score, 90-100). 12 For elderly patients or those who had low performance status, the effect of combined treatment was similar to RT alone. Hasegawa et al recently embarked on a retrospective study, which showed that survival for the Japanese population receiving curative treatment (surgery with RT or concurrent CRT) was significantly lower among those ≥75 years as compared with those aged 65 to 74 years. 27 The differences between these studies and our data may reflect variations in the patient cohorts with regard to comorbidities or lifestyle choices (smoking, alcohol consumption, exercise).28,29 Regardless of these differences, large combined databases among tertiary institutions would likely have the power to perform the multiple-hypothesis testing required to determine the age cutoffs and at which age should treatment escalation be tempered. 30 Other factors that are often not well defined include socioeconomic status, access to allied health/supportive care, and support rendered by family.31,32 Furthermore, the use of platinum-sparing drugs such as cetuximab may have an important role among older patients, as shown by a prospective trial by Alongi et al, 33 but may also require careful management of toxicity by clinicians. These results with our study findings suggest that there may be benefit in administration of standard treatment for elderly patients aged >70 years; however, care must be taken to ensure that supportive care is given.
The differing results in the current literature show that there is no definite treatment advocated for elderly patients with advanced-stage HNSCC. Furthermore, our study has the limitations of a retrospective study, as selection bias can occur in the recruitment process in that older patients selected to undergo aggressive treatment likely have limited comorbidities and are already selected to have better outcomes. Certain data that may affect how we view the parameter of age—such as performance status and comorbidity scoring systems—were not available retrospectively in this cohort. Future research should be based on large multicenter databases or prospective data collection, with the aims of developing more reliable recommendations that can guide clinicians in deciding the standard of care for elderly patients. Also, parameters such as allied health support, quality-of-life analyses, and presence of rehabilitation services (eg, community hospitals) should be included to address whether they aid elderly patients to undergo standard treatment.
Conclusion
In conclusion, there is significantly better survival for elderly patients who receive aggressive curative treatment regardless of subsites. Clinicians should consider giving standard-of-care treatment for elderly patients while taking into account other factors, such as performance status, quality of life, patient autonomy, and views of family members.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented as a poster (third prize) at the AHNS Ninth International Conference on Head and Neck Cancer; July 16-20, 2016; Seattle, Washington.