
Abstract
Objective
To investigate 24-hour ambulatory blood pressure changes 6 months after surgery among children with obstructive sleep apnea.
Study Design
Prospective interventional study.
Setting
Tertiary medical hospital.
Subjects and Methods
Children aged 4 to 16 years with symptoms of obstructive sleep apnea (apnea-hypopnea index >1) were recruited. All children underwent adenotonsillectomy and postoperative polysomnography overnight. The 24-hour ambulatory blood pressure was measured before and 6 months after surgery.
Results
The study cohort enrolled 124 children: mean (SD) age, 7.3 (3.1) years; 73% boys. After surgery, the apnea-hypopnea index significantly decreased from 13.3 (18.1) to 3.3 (7.2) events per hour (P < .001). Overall systolic blood pressure and diastolic blood pressure were not significantly different following surgery, while daytime systolic blood pressure was slightly increased (114.3 to 117.3 mm Hg, P < .01) postoperatively. The hypertensive group (n = 43) exhibited significantly decreased levels of overall diastolic, nighttime systolic, and nighttime diastolic blood pressure (P < .05), and 54% of hypertensive children became nonhypertensive after surgery. The nonhypertensive group (n = 81) showed slightly increased levels of nocturnal overall systolic, daytime systolic, and nighttime systolic blood pressure. A generalized linear mixed model revealed that children with hypertension had a greater decrease in systolic and diastolic ambulatory blood pressure during the daytime and nighttime (all P < .05) than those without hypertension.
Conclusions
Ambulatory blood pressure changes after adenotonsillectomy among children with obstructive sleep apnea are minimal. The decrease in ambulatory blood pressure after surgery is more prominent for hypertensive children than nonhypertensive children.
Childhood obstructive sleep apnea (OSA) is a respiratory disorder caused by upper airway collapse during sleep.1,2 The pathophysiology of childhood OSA is mainly due to tonsillar and adenoid hypertrophy obstructing the upper airway. 3 Adenotonsillectomy (T&A) is therefore widely considered the first-line therapy for treating OSA in the pediatric population.4-6
The association between elevated blood pressure (BP) and childhood OSA has received intense attention.7-13 In 1976, Guilleminault et al first stated that progressive development of hypertension could suggest the possibility of childhood OSA. 7 Since then, several hospital- and community-based studies have observed a correlation between high BP and childhood OSA.8-13 Therefore, BP monitoring for children with OSA to detect those with high BP and prevent further cardiovascular consequences is highly desired.
The effects of T&A on BP among children with OSA have garnered increased attention.14-23 As T&A offers prominent improvement of childhood OSA, it is hypothesized that the surgery may lead to improvements in BP measures as well.22,23 Teo and Mitchell conducted a review of the relevant literature and reported that T&A may have a significant role in reversing the BP and cardiovascular sequelae of childhood OSA. 22 In contrast, a review article by Vlahandonis et al identified only a small reduction or no change in BP after children with OSA underwent T&A. 23 The role of surgery on BP measures and its impact on BP changes in certain subgroups (eg, hypertensive vs nonhypertensive) remain controversial.
Office BP and 24-hour ambulatory BP (ABP) monitoring have been proposed for recording BP measures.24-26 Compared with office BP measures, ABP monitoring is better linked to preclinical organ damage in the pediatric population27,28 and is more strongly correlated with childhood OSA. 29 Moreover, BP normally decreases during the night. Absence of this phenomenon (nondipping) implies an alteration of the sympathetic nerve system and may therefore be associated with increased cardiovascular risk. 27 The nighttime dipping can also be identified with 24-hour ABP monitoring. However, the most relevant studies were based on office BP measures,14-17,19,20 and limited studies have investigated the use of ABP monitors for OSA before and after T&A.18,21 Furthermore, studies with ABP monitors are of short-term or inconsistent follow-up periods.18,21 A prospective study with a longer follow-up interval for ABP changes following T&A for children with OSA is highly needed.
This study aimed to investigate ABP changes after T&A among children with OSA. Particularly interesting is the comparison of disparities of ABP changes between hypertensive and nonhypertensive children with OSA.
Methods
Study Population
This research was approved by the Ethics Committee of National Taiwan University Hospital. Written informed consent was obtained from each child or his or her parents. Children between 4 and 16 years old with symptoms suggestive of OSA were invited to participate.30-32 Children with prior adenotonsillar surgery, pharyngeal surgery, craniofacial anomalies, genetic disorders, cognitive deficits, neuromuscular diseases, or major medical illnesses (eg, cardiac, respiratory, or renal insufficiency) were excluded.
Basic demographic data, including age, sex, and body weight, were recorded. The weight and height of each child were measured and the body mass index (BMI) calculated. The BMI of each child was converted to BMI percentile based on age- and sex-corrected standards in Taiwan. 33 Obesity was defined as a BMI >95th percentile for a child’s age and sex. 2
Polysomnography
Overnight polysomnography (PSG; Embla N7000, Medcare Flaga, Reykjavik, Iceland) was performed in our sleep laboratory according to the established protocol.34,35 Sleep stages and respiratory events were recorded per the guidelines of the American Academy of Sleep Medicine. 36 The apnea-hypopnea index (AHI) was used to define the presence and severity of OSA. OSA severity was classified as mild (5 > AHI ≥ 1), moderate (10 > AHI ≥ 5), or severe (AHI >10).34,35 Postoperative PSG studies were performed 3 to 6 months after surgery.
Adenotonsillectomy
Tonsillectomy was performed with the coblation method, and adenoidectomy was conducted with the microdebrider-assisted method.37-40 In Taiwan, parents are concerned with complications arising from general anesthesia or surgery, such as respiratory status, oral intake, and throat pain control. Moreover, Taiwan’s National Health Insurance structure allows physicians to keep children in the hospital at least overnight for observation after tonsillar surgery. 41 Therefore, all children underwent T&A under general anesthesia in a single stage and were hospitalized for 2 to 3 days. 40
24-Hour ABP
The 24-hour ABP monitoring was measured with the Oscar 2 oscillometric monitor (model 222; SunTech Medical, Morrisville, North Carolina). The Oscar 2 device was verified by the International Protocol of the European Society of Hypertension and British Hypertension Society.42,43 ABP was measured at 15-minute intervals during daytime (7
BP load is defined as the percentage of valid BP measurements >95th percentile for a child’s age and sex. 44 This study calculated the BP index to compare age and sex subgroups via the following formula: BP index = (measured BP − 95th percentile) / 95th percentile × 100.9,10,17,20,21 Hypertension was defined as mean systolic or diastolic BP values >95th percentile of the ABP norm. 44 Nocturnal dipping was obtained by determining the difference between mean daytime and nighttime BP and expressed as a percentage of total dipping. Children whose nocturnal BP dipped <10% were defined as nondippers. 44
Statistical Analysis
Data were analyzed with SPSS 22 (IBM, Armonk, New York). Comparisons of continuous variables and categorical variables before and after surgery were made with the paired-sample t test and McNemar test, respectively. The difference in pre- to postoperative changes between the nonhypertensive and hypertensive groups was estimated by a generalized linear mixed model that included the intercept, the main effects in the study group (hypertensive vs nonhypertensive) and time (post- vs preoperative), and a 2-way interaction term (group × time). The ABP parameters were deemed to change in one group more than the other when the interaction term was statistically significant. Finally, the ABP changes before and after surgery as stratified by different subgroups were analyzed with generalized linear mixed models. The subgroups included children with different age, sex, adiposity, disease severity, and preoperative hypertensive status. The intercept, main effects of subgroups, and interaction effects of subgroups × time were estimated. Pearson correlation was used to examine the relation between the changes in PSG data and selected BP parameters. A P value <.05 was considered statistically significant.
Results
Basic Data
A total of 124 children were included. Basic data are listed in Table 1 and Supplemental Table S1 (available in the online version of the article). The mean (SD) age of the study population was 7.3 (3.1) years, and 72.6% (90 of 122) were boys. In this study cohort, 52 children had mild OSA, 24 had moderate OSA, and 48 had severe OSA. The mean body weight, height, and BMI significantly increased after surgery. The mean BMI percentile significantly increased after surgery, whereas the proportion of obesity did not.
Demographic, Anthropometric, and Polysomnographic Data before and after Surgery (N = 124). a
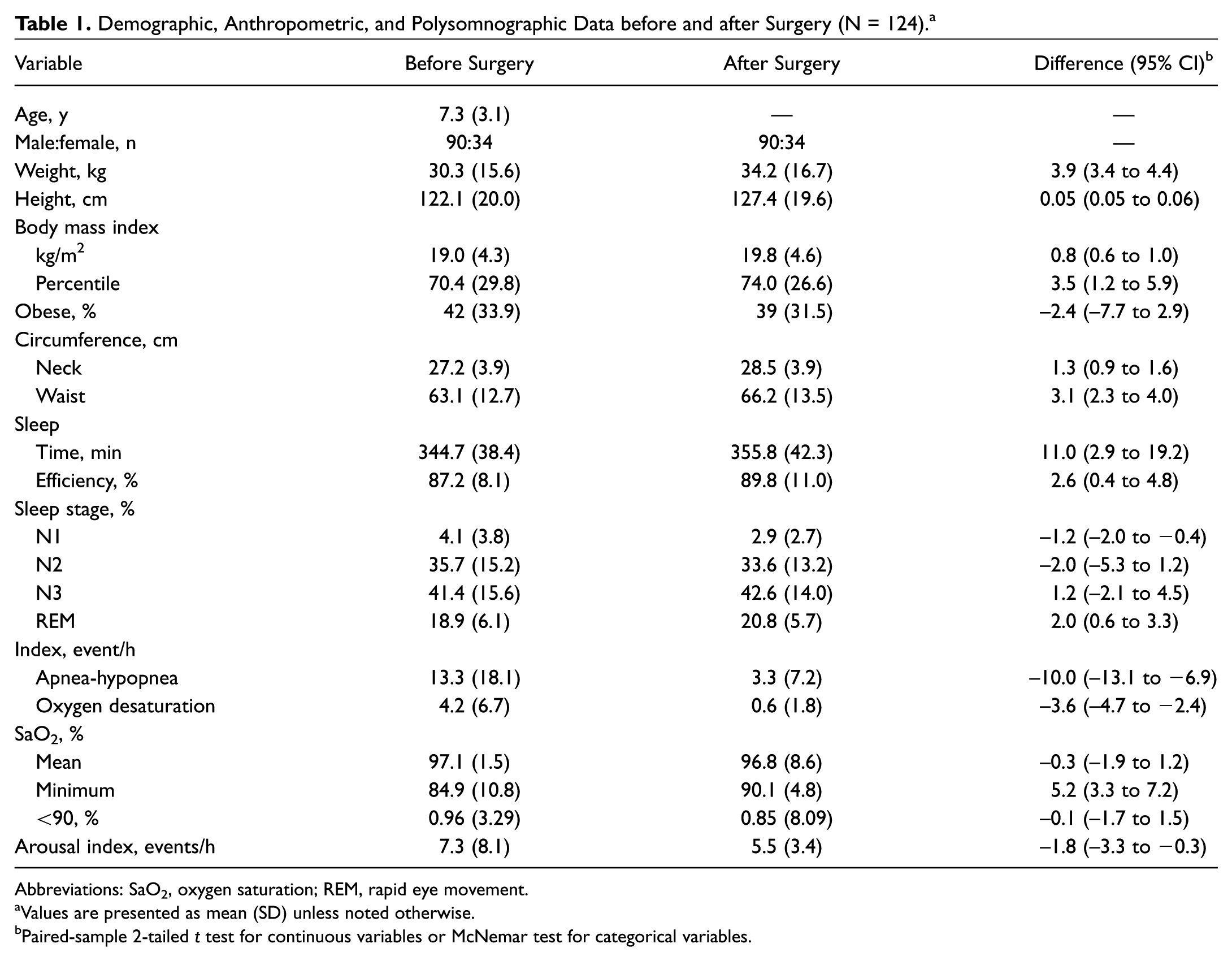
Abbreviations: SaO2, oxygen saturation; REM, rapid eye movement.
Values are presented as mean (SD) unless noted otherwise.
Paired-sample 2-tailed t test for continuous variables or McNemar test for categorical variables.
PSG Data after Surgery
After T&A, sleep architecture was altered by a significant increase in total sleep time, sleep efficiency, and rapid eye movement stage and a decrease in sleep stage 1.
After surgery, the mean AHI significantly reduced from 13.3 to 3.3 events/h (t = −6.3, P < .001) with a decrease of the oxygen desaturation index from 4.2 to 0.6 events/h (t = −6.0, P < .001). The arousal index significantly decreased from 7.3 to 5.5 events/h (t = −2.4, P = .02). The minimum oxygen saturation significantly increased from 84.9% to 90.1% after surgery (t = 5.3, P < .001).
24-Hour ABP Parameters after Surgery
The overall 24-hour ABP parameters did not change significantly after surgery ( Table 2 and Supplemental Table S2). Changes in overall systolic BP, diastolic BP, systolic BP load, and diastolic BP load were not statistically significant.
24-Hour Ambulatory Blood Pressure Parameters before and after Surgery (N = 124). a
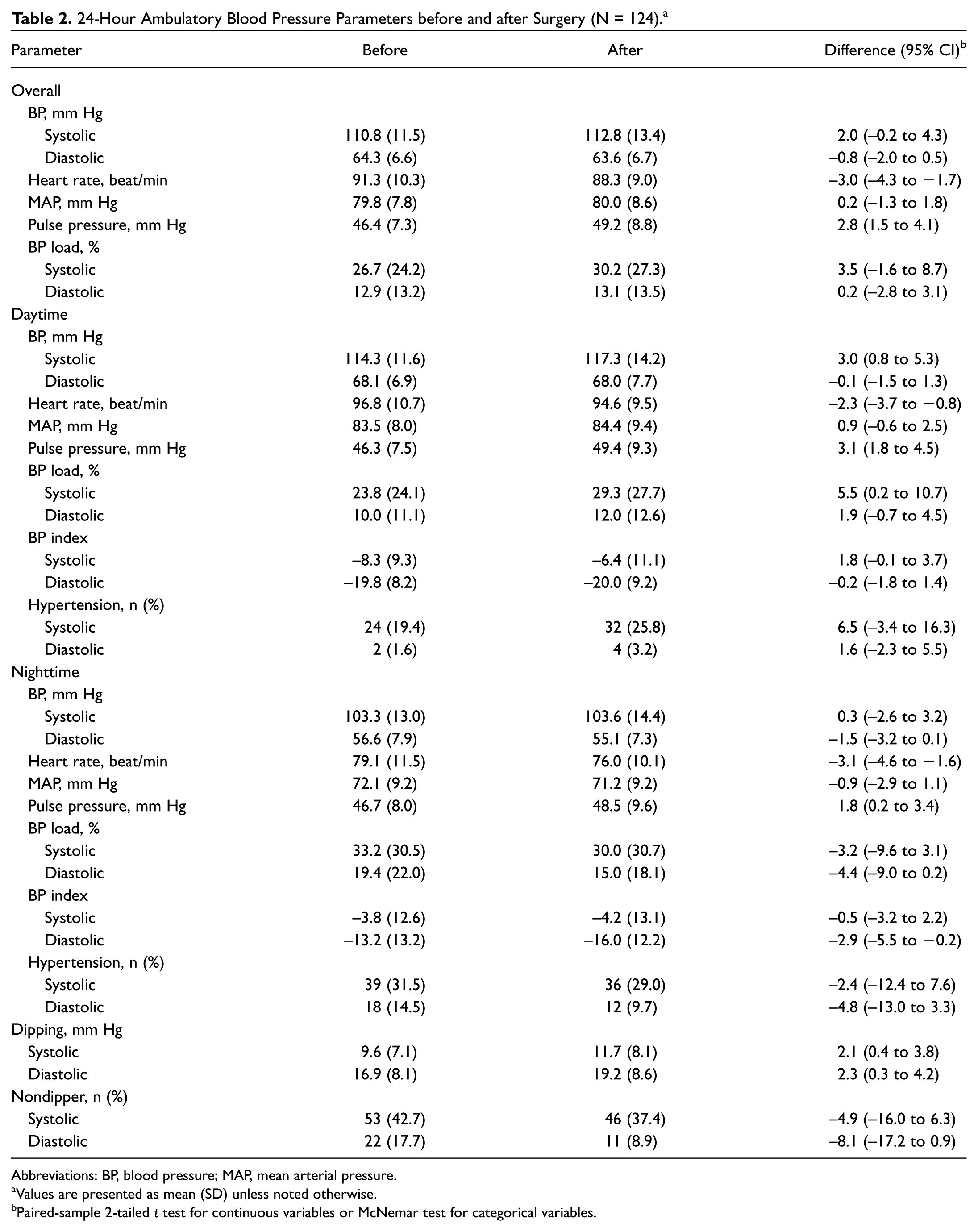
Abbreviations: BP, blood pressure; MAP, mean arterial pressure.
Values are presented as mean (SD) unless noted otherwise.
Paired-sample 2-tailed t test for continuous variables or McNemar test for categorical variables.
The daytime 24-hour ABP parameters showed a slight increase in systolic BP (114.3 to 117.3 mm Hg, t = 2.7, P < .01) and systolic BP load (23.8% to 29.3%, t = 2.1, P = .04). Daytime BP, diastolic BP load, systolic BP index, and diastolic BP index were not significantly different after surgery.
The nighttime 24-hour ABP parameters showed a slight decrease in diastolic BP index (–13.2 to −16.0, t = −2.2, P = .03). Nighttime systolic BP, diastolic BP, systolic BP load, diastolic BP load, and systolic BP index were not significantly different after surgery.
Systolic dipping (9.6 to 11.7 mm Hg, t = 2.4, P = .02) and diastolic dipping (16.9 to 19.2 mm Hg, t = 2.3, P = .02) increased slightly after surgery. However, systolic and diastolic nondippers showed no significant differences after surgery.
24-Hour ABP Changes in Hypertensive versus Nonhypertensive Groups
The hypertensive group (n = 43) showed a significant decrease in overall diastolic BP (69.8 to 65.9 mm Hg, t = −2.8, P < .01), overall systolic BP load (53.0% to 41.5%, t = −2.3, P = .03), daytime diastolic BP index (–13.5 to −16.9, t = −2.0, P = .047), nighttime systolic BP (117.0 to 109.7 mm Hg, t = −2.4, P = .02) and diastolic BP (63.2 to 57.1 mm Hg, t = −3.4, P < .01), nighttime systolic BP load (69.4% to 42.0%, t = −4.6, P < .001) and diastolic BP load (38.7 to 20.3%, t = −3.6, P < .01), nighttime systolic BP index (9.3 to 1.2, t = −2.8, P < .01) and diastolic BP index (–2.2 to −12.5, t = −3.6, P < .01), and nighttime systolic hypertension (90.7% to 46.5%, P < .001) and diastolic hypertension (41.9% to 14.0%, P = .01). The hypertensive group with OSA had a significant increase in systolic dipping (5.5 to 11.4 mm Hg, t = 3.6, P < .01) and diastolic dipping (13.5 to 19.7 mm Hg, t = 3.2, P < .01) and a decreased proportion of systolic (58.1% to 37.2%, P = .049) and diastolic (32.6% to 4.7%, P < .01) nondippers.
The nonhypertensive group demonstrated a significant increase in overall systolic BP (104.9 to 109.5 mm Hg, t = 4.0, P < .001), overall systolic BP load (12.7% to 24.3%, t = 4.5, P < .001), overall diastolic BP load (7.1% to 10.7%, t = 2.6, P = .01), daytime systolic BP (108.9 to 114.0 mm Hg, t = 4.0, P < .001), daytime systolic BP load (12.2% to 23.8%, t = 4.2, P < .001), daytime diastolic BP load (6.2% to 10.0%, t = 2.9, P < .01), daytime systolic BP index (–12.6 to −9.0, t = 3.2, P < .01), daytime systolic hypertension (0% to 21.0%, P < .001), nighttime systolic BP (96.0 to 100.3 mm Hg, t = 3.3, P < .01), nighttime systolic BP load (14.0% to 23.6%, t = 3.3, P < .01), nighttime systolic BP index (–10.7 to −7.1, t = 3.0, P < .01), and nighttime systolic hypertension (0% to 19.8%, P < .001).
Generalized Linear Mixed Model Analysis for Subgroups
This study applied a generalized linear mixed model to analyze the discrepancies of ABP changes for hypertensive groups ( Table 3 and Supplemental Table S3) and other subgroups ( Table 4 ). The most remarkable findings were the differences in ABP changes between the hypertensive and nonhypertensive groups ( Figure 1 ). Generalized linear mixed model analysis revealed that BP parameters had significant interaction terms between the groups (all P values <.05), indicating that greater improvement was exhibited by children with hypertension than those without hypertension after surgery. In addition, children with hypertension had a significant increase in systolic and diastolic dipping and decreased systolic and diastolic nondippers.
24-Hour Ambulatory Blood Pressure Parameters before and after Surgery Stratified by Hypertensive Status (N = 124). a
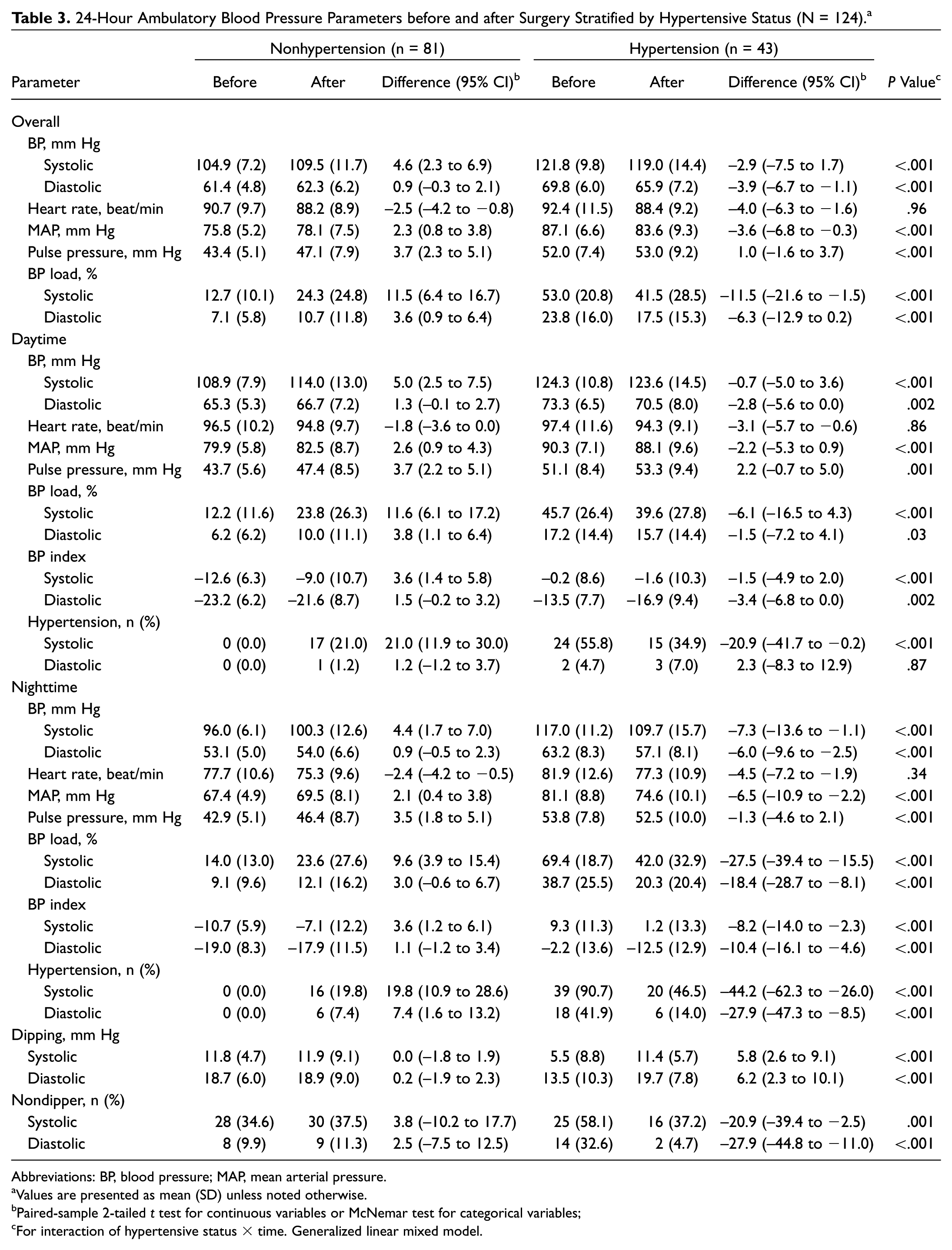
Abbreviations: BP, blood pressure; MAP, mean arterial pressure.
Values are presented as mean (SD) unless noted otherwise.
Paired-sample 2-tailed t test for continuous variables or McNemar test for categorical variables;
For interaction of hypertensive status × time. Generalized linear mixed model.
Generalized Linear Mixed Modeling of Ambulatory Blood Pressure Parameters between Subgroups.
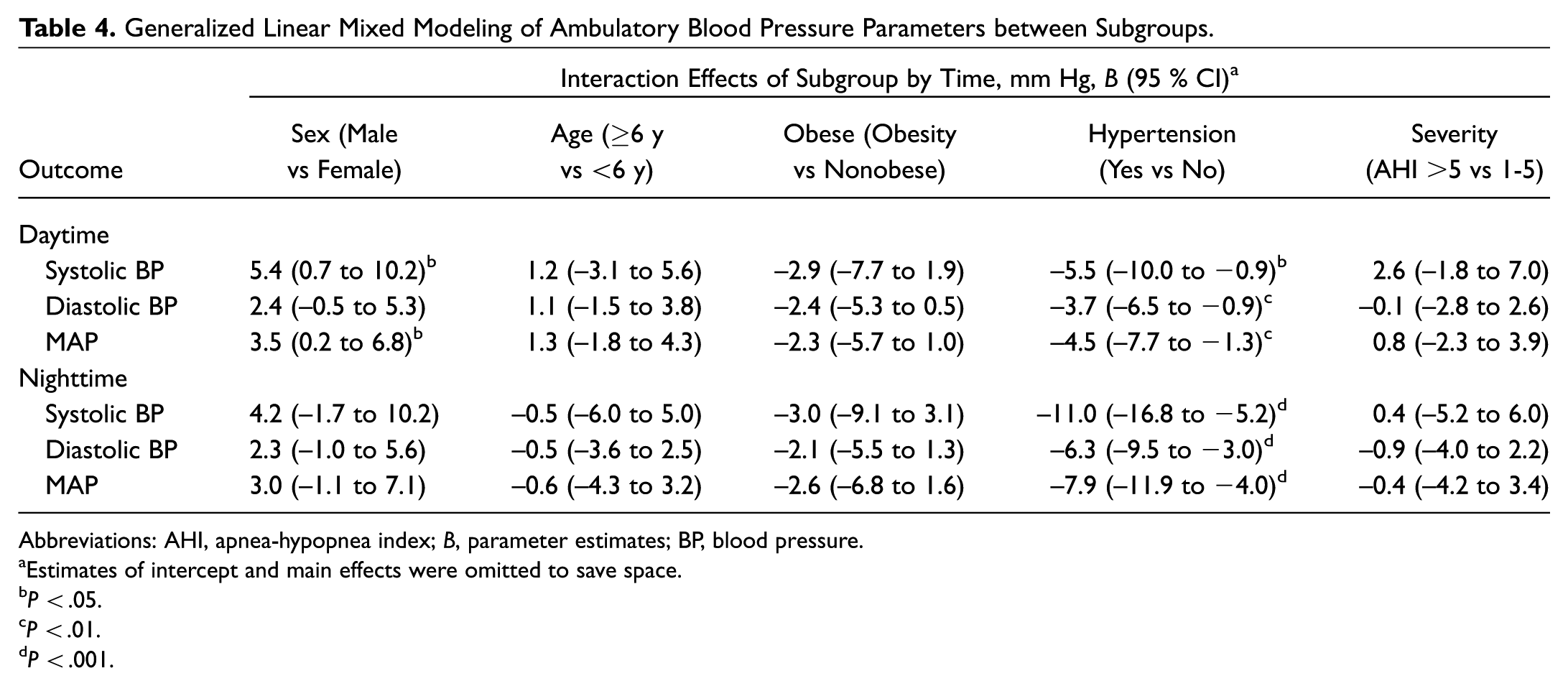
Abbreviations: AHI, apnea-hypopnea index; B, parameter estimates; BP, blood pressure.
Estimates of intercept and main effects were omitted to save space.
P < .05.
P < .01.
P < .001.
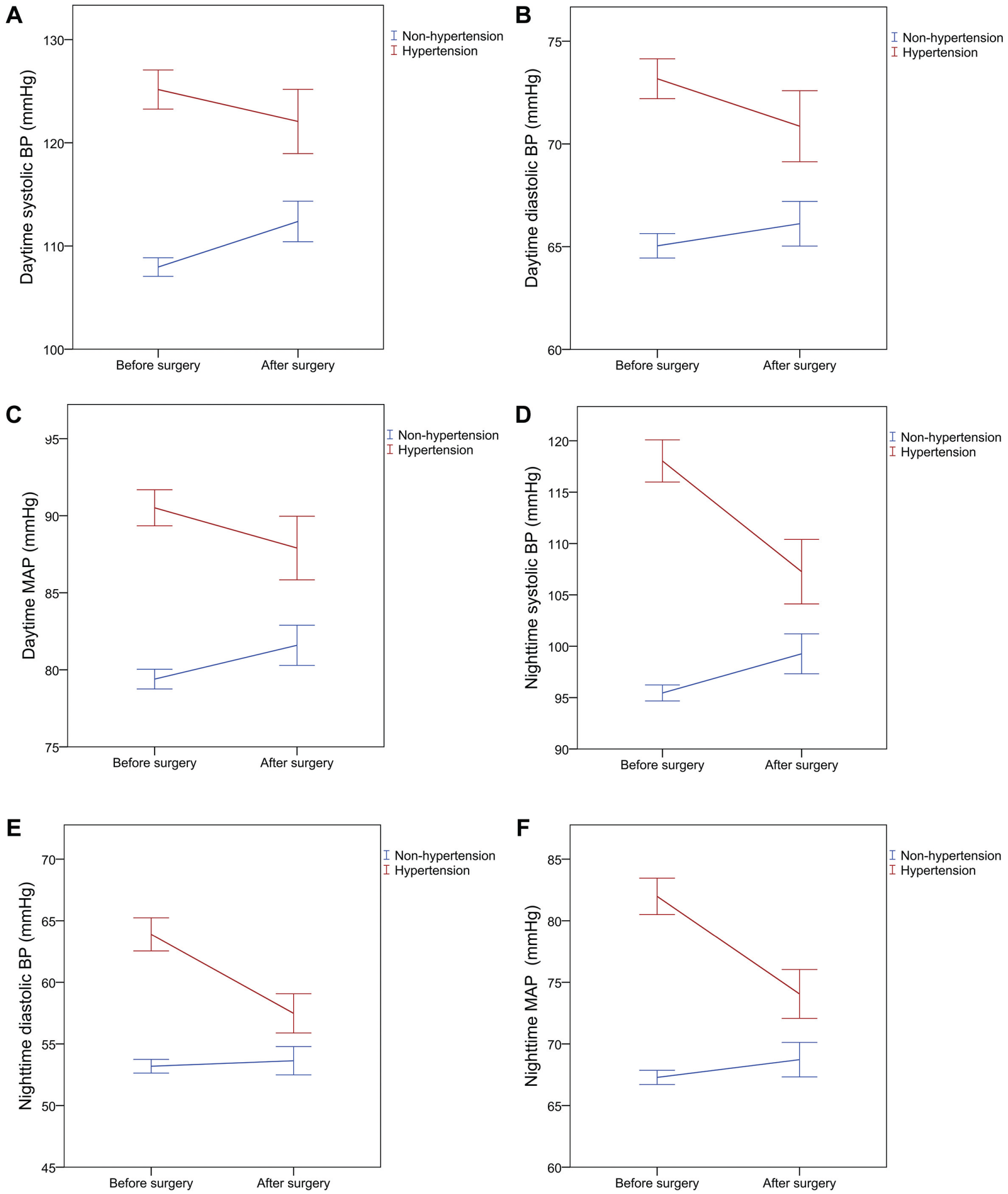
(A-C) Daytime and (D-F) nighttime systolic BP, diastolic BP, and MAP between hypertensive and nonhypertensive children after surgery. Middle horizontal line: mean. Error bars: 95% CI. BP, blood pressure; MAP, mean arterial pressure.
Table 4 demonstrates the interaction effects of all subgroups. Children with hypertension, as compared with those without hypertension, had a greater improvement in daytime systolic BP by 5.5 mm Hg (95% CI, –10.0 to −0.9 mm Hg), daytime diastolic BP by 3.7 mm Hg (95% CI, –6.5 to −0.9 mm Hg), nighttime systolic BP by 11 mm Hg (95% CI, –16.8 to −5.2 mm Hg), and nighttime diastolic BP by 6.3 mm Hg (95% CI, –9.5 to −3.0 mm Hg). In addition, as compared with girls, boys had a higher increase of daytime systolic BP by 5.4 mm Hg (95% CI, 0.7 to 10.2 mm Hg) and daytime mean arterial pressure by 3.5 mm Hg (95% CI, 0.2 to 6.8 mm Hg). However, there was no significant difference in the change before and after surgery in terms of age, obesity, or OSA severity.
Correlations between PSG and 24-Hour ABP Parameters
Correlations between preoperative PSG parameters and 24-hour ABP parameters are shown in Supplemental Table S4. Preoperative AHI and oxygen desaturation index were positively correlated with nighttime systolic and diastolic BP before surgery. However, the change of PSG parameters was not correlated with a change of 24-hour ABP parameters after surgery (Supplemental Table S5).
Shift of Hypertensive Status after Surgery
Supplemental Table S6 shows the shifts in hypertensive status after surgery. Overall, 52.4% of the children with systolic hypertension shifted to a nonhypertensive status, and 88.9% of the children with diastolic hypertension shifted to a nonhypertensive status. Furthermore, 22 (27.2%) children who were nonhypertensive before surgery became hypertensive after surgery. Despite these shifts in hypertensive status, the changes did not reach statistical significance.
Discussion
This research aimed to elaborate the effects of T&A on BP measures among children with OSA. The key finding of the study is that hypertensive children exhibit a more prominent reduction of ABP parameters than do nonhypertensive children. The major strength of this study is the application of 24-hour ABP monitoring for measuring BP. Another strength is the large sample size with a constant follow-up interval. The 24-hour ABP monitoring was conducted for all individuals at 6 months after T&A. Therefore, the results have immense clinical implications and provide data elucidating BP changes after T&A among children with OSA.
Pediatric OSA is associated with raised BP.7-13 Nisbet et al found that preschool children with OSA had a high baseline BP and suggested that elevated BP in childhood OSA may be detected as early as preschool age. 45 A longitudinal study by Li et al demonstrated that changes in OSA severity were independently associated with 24-hour ABP changes during 4-year follow-up intervals. 46 These findings imply that children with OSA may develop raised BP in their early young life and that early detection and management of OSA may lead to improvements in BP measures.
Clinicians are concerned about whether treatment of childhood OSA results in a reduction in BP measures as well.22,23,47,48 It is well recognized that T&A, the first-line treatment of childhood OSA, achieves remarkable alleviation of OSA severity.4,49 However, current literature suggests that decreased BP measures are inconsistent with a reduction in OSA severity after T&A.14-21 While Amin et al 14 and Ng et al 18 observed a significant decrease in diastolic BP profiles, Apostolidou et al, 15 Lee et al, 16 and Quante et al 19 reported no significant changes in any BP parameters after surgery. Our research group recently published 24-hour ABP data from children with OSA recorded 3 months postoperatively, which indicated a decrease in children’s overall diastolic BP. 21 In contrast, this study reported no significant change in the majority of BP parameters except a slight decrease in the nighttime diastolic BP index. Trajectories of BP changes after surgery should be considered when interpreting the data. After surgery, an increase in age and somatic growth with an increase in BP may be observed in the long term that could overcome the reduction in BP from surgery. Nevertheless, the reduction in BP measures after surgery appears to be minor, and changes in BP and the correlation to other cardiovascular outcomes after treatment among children with OSA still require future studies.50,51
This study compared the discrepancies in BP changes between hypertensive and nonhypertensive groups of children with OSA. Treating adult OSA with continuous positive airway pressure results in a greater reduction of BP for hypertensive patients than nonhypertensive patients.52,53 Similar findings were reported in the pediatric population.16,18,20,21 Ng et al observed that the preoperative hypertensive group had a significant decrease in systolic and diastolic BP after T&A. 18 Lee et al reported that the severity of childhood OSA and hypertension improved after T&A. 16 Our previous publications revealed that hypertensive children with OSA had significant improvement in office BP after T&A 20 and that children with preoperative hypertension had significant improvement in 24-hour ABP 3 months after T&A. 21 The present study had a longer follow-up period (6 months) than our previous studies 21 and confirmed the long-term beneficial effects of OSA surgery in reversing adverse cardiovascular consequences among high-risk individuals. Therefore, this study has substantial clinical implications and provides data regarding the association between OSA and cardiovascular outcomes in the pediatric population.
This study has certain limitations. First, it did not recruit a control group.19,49 The well-known Childhood Adenotonsillectomy Trial compared casual BP changes between T&A and watchful-waiting control groups.18,50 However, to our knowledge, no current study has compared the ABP changes between T&A and watchful-waiting control groups. Second, BP reference levels for children in Taiwan are lacking; hence, the normative data of the Western population were used in this study. 43 Third, this study does not link BP with other cardiovascular variables, such as carotid intima-media thickness.50,51 Future studies are required to investigate changes among other cardiovascular variables after OSA surgery among children. Fourth, there is a lack of data tracking BP and OSA from childhood to adulthood.54,55 Future studies should examine the trajectories of ABP changes and their associations with OSA changes after T&A surgery. 51
Conclusions
Children with OSA who underwent T&A have remarkable resolution of OSA. However, overall ABP parameters did not significantly decrease 6 months following surgery. Notably, hypertensive children exhibit a more prominent reduction of ABP parameters than do nonhypertensive children. This hospital-based study highlights the role of surgery in reversing cardiovascular consequences among hypertensive children with OSA.
Author Contributions
Disclosures
Supplemental Material
OTO825462_suppl_mat – Supplemental material for Effect of Adenotonsillectomy on Ambulatory Blood Pressure in Pediatric Obstructive Sleep Apnea: 6-Month Follow-up Study
Supplemental material, OTO825462_suppl_mat for Effect of Adenotonsillectomy on Ambulatory Blood Pressure in Pediatric Obstructive Sleep Apnea: 6-Month Follow-up Study by Kun-Tai Kang, Shuenn-Nan Chiu, Che-Yi Lin, Wen-Chin Weng, Pei-Lin Lee and Wei-Chung Hsu in Otolaryngology–Head and Neck Surgery
Footnotes
Acknowledgements
We thank the staff of the Center of Sleep Disorder, National Taiwan University Hospital, for their technical support. We are grateful for the cooperation and participation of all the children and their parents. We also thank the anonymous reviewers and the editors for their comments.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2018 AAO-HNSF Annual Meeting & OTO Experience; October 7-10, 2018; Atlanta, Georgia.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.