
Abstract
Objective
To determine the effects an incentive-based physician compensation model has on safety outcomes related to outpatient otolaryngology surgical procedures.
Study Design
A retrospective analysis of a prospectively maintained database assessing the difference in outpatient surgical volume and postoperative adverse outcomes before and after the implementation of a relative value unit (RVU)–based payment structure.
Setting
Single-center academic otolaryngology practice operating at a hospital-owned ambulatory surgery center.
Subjects and Methods
Data prospectively collected from outpatient otolaryngology surgical cases performed at the surgery center from April 2013 to April 2018 were retrospectively reviewed. Equal pre-RVU and post-RVU study periods were calculated for 4 surgeons based on their chronological transition in payment structure (range, 46-56 months). Case volume and incidence rates of adverse outcomes, including postoperative infections, emergency department visits, unplanned hospital admissions, and returns to the operating room, were compared between the pre-RVU and post-RVU study periods at both the surgeon and group levels.
Results
At the group level, the post-RVU period was associated with a higher volume of surgical cases (P = .001). No significant differences were observed in the overall incidence of adverse outcomes (P = .21) or among the specific rates of postoperative hospitalizations (P = .39), infections (P = .45), unplanned returns to the operating room (P = 1.00), or emergency department visits (P = .39). Comparable results were observed at the individual surgeon level.
Conclusion
The implementation of an incentive-based salary was not associated with a change in the incidence of adverse safety outcomes in the setting of increased outpatient otolaryngology procedures.
Keywords
In the current era of value-based care, health care systems have transitioned from traditional fee-for-service models of physician compensation toward novel incentive-driven payment structures. Reimbursement models centered on relative value units (RVUs) are commonplace in today’s health care environment, attempting to measure physician performance in an objective manner by awarding productivity via clinical volume. 1 Recently, both private- and public-sector initiatives have supported clinical quality over quantity by integrating components of efficiency, satisfaction, and safety into compensation structures. This shift is best exemplified by the Centers for Medicare & Medicaid Services’ (CMS) mandated participation in the Quality Payment Program by physicians caring for Medicare-insured patients. 2 Tasked with embracing this ongoing and expansive payment reform, otolaryngologists are faced with many challenges prone to our specialty, including the absence of appropriate quality metrics and heterogeneity in practice complexion. 3
In 2014, the American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) estimated that 83% of procedures are performed in an ambulatory surgery center (ASC), hospital outpatient department, or office setting. 4 Similarly, the Agency for Healthcare Research and Quality projected that 87% of the most common operations of the ears, nose, mouth, and pharynx occur within an ASC. 5 As endorsed by the AAO-HNS, procedures performed in an outpatient setting must not be expected to pose a significant risk to patient safety and should not require medical attention overnight. 6 With an exceptionally high incidence of relatively low-risk procedures, the application of a productivity-based compensation model in otolaryngology seems worthwhile as it creates incentive without compromising patient safety.
Despite these proposed advantages and advocacy efforts from organizations such as the AAO-HNS, the systematic acceptance of innovative payment methods has not yet garnered universal acceptance. To our knowledge, there have been no published reports outlining the contemporary experiences of institutional otolaryngology practices that may aid physicians considering a transition in payment structures. With upcoming government directives, the need for institutional transparency and sharing of systems-based information has been never been greater.
In this report, we aimed to evaluate patient safety and operative outcomes of outpatient otolaryngology procedures performed at the ambulatory surgical center of our institution in relation to the implementation of an RVU-based compensation model. On a group and individual-surgeon level, we analyzed the differences in case volume and rates of various postoperative outcomes before and after the implementation of this payment structure.
Methods
The Department of Otolaryngology–Head and Neck Surgery at Cooper University Hospital began offering an RVU-based compensation program to its surgeons in 2015. The adoption of this program was mandatory upon expiration of previous contracts, with an available option to opt in early. The transition was executed by the 5 preexisting surgeons from July 2015 to July 2016. Under this new payment structure, physician compensation is calculated through a variety of metrics that incorporates personal and group clinical productivity (work RVUs), educational activities (academic RVUs), and various quality measures. This incentive-driven model replaced a primarily salary-based model in which compensation was fixed and not influenced by case volume. In both the existing and new payment structure, there was no direct financial incentive for the surgeons to operate at either the ASC or the main hospital settings.
In an effort to monitor department quality, the division prospectively collected and maintained a database recording the rates of unintended postoperative hospitalizations, visits to the emergency room, unplanned returns to the operating room, and postoperative infections for all otolaryngology surgical cases performed at the ASC of our institution. Unintended postoperative hospitalization was further classified as direct (admitted from the ASC after the operation) and indirect (admitted during the postoperative period, days 1-30). The primary end point of interest during prospective data collection was the incidence of these events, as recorded on a case-to-case basis. The occurrence of these adverse outcomes was reported for each case by both the operating physician—via required monthly evaluations—and the patient (legal guardian in pediatric cases)—via routine telephone follow-up during a 60-day postoperative period.
To determine if the new compensation program was associated with a change in the incidence of these outcomes, the prospectively collected data from April 2013 to April 2018 were retrospectively reviewed. Only data from the original 5 surgeons who participated in the existing and new contract structures were considered for review. Each surgeon in the study group is fellowship trained with practices focusing on head and neck oncology, facial plastic surgery, pediatric otolaryngology, or rhinology. All 5 surgeons operate at the ASC of our institution.
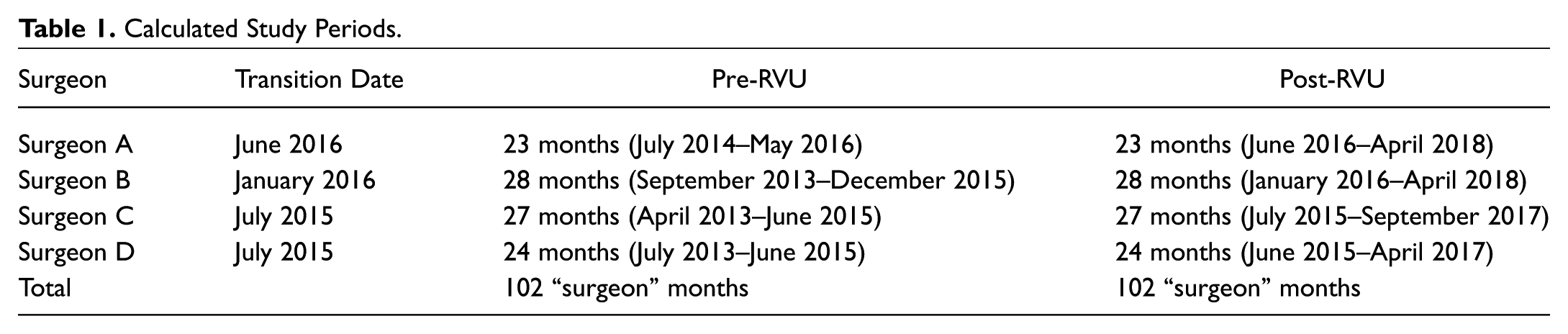
As not all of the physicians in the group transitioned to the RVU plan at a simultaneous date, individual study periods were calculated for each surgeon, which comprised equal time (months) before (pre-RVU) and after (post-RVU) the implementation of the payment structure (range, 46-56 months). Then, data from the pre-RVU and post-RVU periods were pooled together to obtain information at the group level. Note, data from 1 of the 5 surgeons were excluded as the length of the individual’s pre-RVU interval was limited secondary to early contract opt-in. Table 1 illustrates the structure of the final individual and group periods included in the study.
Calculated Study Periods.
The primary end points of interest were the differences in case volumes and rates of the aforementioned outcomes between the pre-RVU and post-RVU study periods at both the individual surgeon and group levels. Secondary end points of interest were the differences in operative times between the study periods. To assess for procedural variation, the frequencies of key indicator cases were analyzed between the 2 periods. In an effort to assess for reporting and recall bias, 150 cases (10% of total cohort) were randomly selected via a computer-generated random-number program. The authors of the study retrospectively compared the prospectively collected data to the hospital electronic medical records for any differences in reported outcomes.
Approval from the Cooper Health System Institutional Review Board was obtained prior to the beginning of the study (#18-083EX). SAS v9.4 software (SAS Institute, Cary, North Carolina) was used to perform all statistical analysis. Case volumes and the rates of the adverse safety outcomes were calculated using Poisson counts. Pearson χ2 was used to test the significance of the differences in case volumes, the rates of adverse outcomes, and the frequencies of key indicator cases between the 2 study periods. Fisher’s exact test with post hoc Bonferroni adjustment for multiple comparisons was used to calculate the level of statistical significance. A 2-sided critical value of P < .05 was used to define significance in case volume differences. Significance between rates of adverse outcomes and distribution of key indicator cases was defined using an adjusted 2-sided α of P < .007. Unadjusted odds ratios were calculated for adverse safety outcomes and reported with 95% confidence intervals. Wilcoxon rank sum was used to analyze operative times between the 2 study periods.
Results
Individual-surgeon study periods ranged from 46 to 56 months, contributing to a study group total of 204 “surgeon” months ( Table 1 ). A total of 1508 otolaryngology surgical cases performed at the ambulatory surgical center of our institution from April 2013 to April 2018 were included within this study group. In total, 685 cases were performed in the pre-RVU period and 823 in the post-RVU period (P = .001).
No significant difference was observed in the composite incidence of adverse safety outcomes between the 2 study periods (2.34% pre-RVU vs 1.46% post-RVU, P = .21). Similarly, no differences were demonstrated among any of the specific outcomes, including total hospitalizations (1.46% vs 0.97%, P = .39), direct hospitalizations (0.44% vs 0.36%, P = .39), indirect hospitalizations (1.02% to 0.61%, P = .37), or unplanned returns to the operating room (0.58% vs 0.61%, P = 1.00). The incidence of emergency room visits was 1.46% in the pre-RVU period and 0.97% in the post-RVU period (P = .39). In total, only 1 postoperative infection was reported, occurring during the pre-RVU period (0.15% vs 0%, P = .45). No intraoperative or postoperative deaths occurred in the study cohort. Table 2 summarizes these data presented with unadjusted odds ratios and 95% confidence intervals.
Incidences of Postoperative Outcomes. a
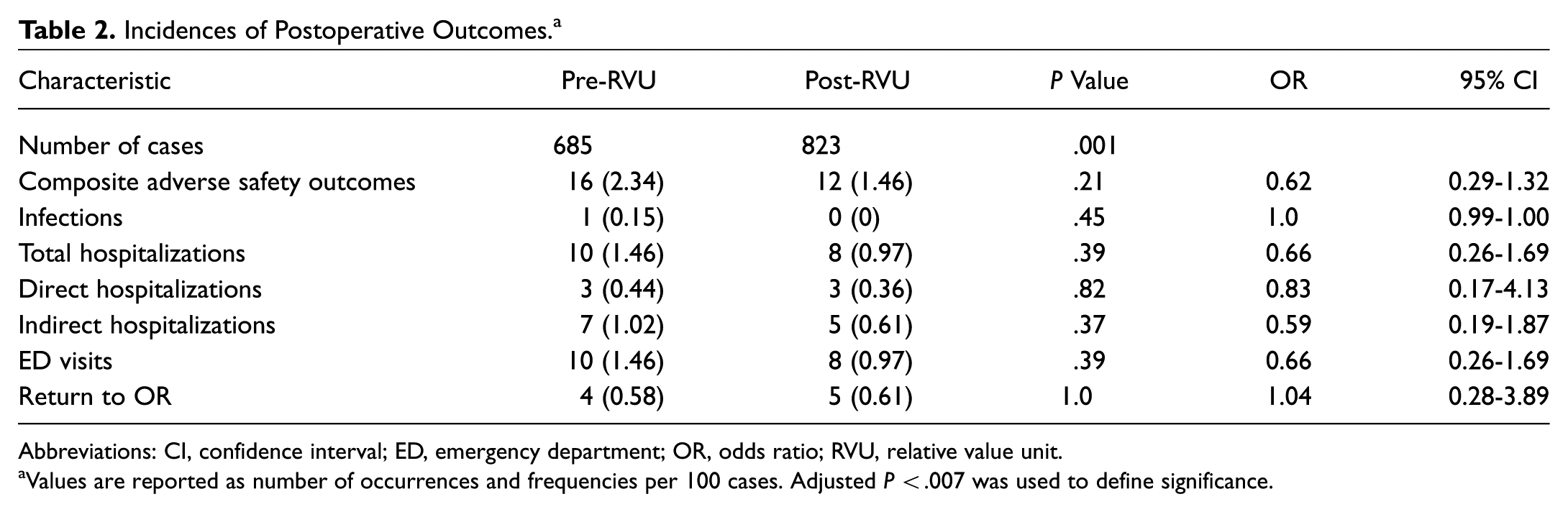
Abbreviations: CI, confidence interval; ED, emergency department; OR, odds ratio; RVU, relative value unit.
Values are reported as number of occurrences and frequencies per 100 cases. Adjusted P < .007 was used to define significance.
At the individual-surgeon level, significant differences in the case volumes between the pre-RVU and post-RVU periods were observed for 3 surgeons in the study group (P < .001 to .027). The fourth surgeon did not demonstrate a statistical difference (248 cases pre-RVU vs 320 cases post-RVU; P = .155). Analogous to the group level, no significant differences were observed in the composite and specific rates of the adverse outcomes between the pre-RVU and post-RVU study periods.
The median operative time for cases in the post-RVU period (52 minutes) was significantly less than the median operative time in the pre-RVU period (59 minutes) (P < .001). This trend held true for all but one of the surgeons in the group (P = .006-0.034, n = 3). The distribution of key index cases is summarized in Table 3 . At the group level, significant differences were observed in the frequency of parotidectomies (P < .001) between the 2 study periods. The remainder of the analyzed key indicator cases demonstrated no statistical differences. In total, 150 cases (~10% of total cohort) were randomly selected (67 pre-RVU, 83 post-RVU) for electronic medical record review. This analysis yielded no discrepancies between the incidence of the prospectively collected outcomes and retrospectively reviewed outcomes.
Key Indicator Case Distribution. a
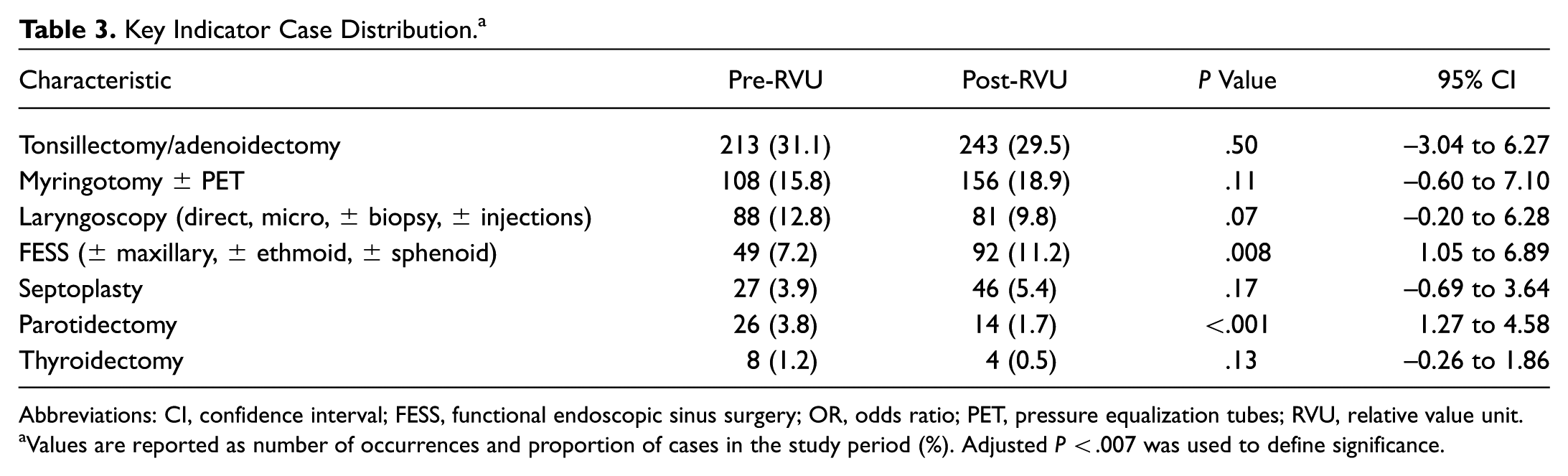
Abbreviations: CI, confidence interval; FESS, functional endoscopic sinus surgery; OR, odds ratio; PET, pressure equalization tubes; RVU, relative value unit.
Values are reported as number of occurrences and proportion of cases in the study period (%). Adjusted P < .007 was used to define significance.
Discussion
The implementation of a productivity-based compensation program in our institution’s otolaryngology practice was not associated with an increase in adverse outcomes in the setting of increased outpatient surgical volume. Specifically, this analysis demonstrated that the rates of emergency department (ED) visits, hospitalizations, and returns to the operating room following ambulatory surgery did not change after the adoption of an RVU-based compensation plan. Our experience is the first report specific to otolaryngology that contributes to the current field of evidence that suggests favorable patient safety is maintained with the incentive to increase volume. Furthermore, the post-RVU period was associated with shorter operative times than the pre-RVU period. Although limited conclusions can be made regarding the direct influence that the incentive-driven compensation held on operative times, this report demonstrates that decreased operative times were not associated with worse safety outcomes in the setting of higher outpatient volumes.
While these results potentially highlight the practicality of such compensation structures within a tertiary-center based otolaryngology practice, several limitations should be acknowledged. First, although the data were collected in a prospective manner, the risk for recall and reporting bias is inherent to the nature of the data collection process. In an effort to provide validation for our reporting system and assess for bias, our random-sample cross-analyses found no discrepancies between the prospectively reported incidences and those documented in the electronic medical records. In addition, this limitation would equally affect incidence calculations in both the pre-RVU and post-RVU periods, reducing its effects on a comparative analysis.
Second, the incidence of the studied adverse outcomes may be quite rare for otolaryngology ambulatory surgery procedures and not accurately captured in our sample. As this was an initial publication on this topic, introducing it to our field, pilot data for power calculations were not available in the planning stage of this investigation. Currently, there is a paucity of data available in our literature that details the incidence of ambulatory procedure adverse outcomes. A review of the few database studies and institutional reports reveals rates of specific adverse outcomes similar to those observed in our analysis.7-11 In our study, infections were documented by clinical finding at routine follow-up, urgent follow-up or ED visits that required unplanned antibiotics, and patient reported symptoms resembling infection via telephone survey. Although we only observed 1 postoperative infection, Owens et al 12 found comparable infection rates for all low- to moderate-risk ambulatory surgical procedures not specific to otolaryngology. Moreover, all perioperative antibiotic guidelines were followed appropriately per institutional standard.
Finally, the preexisting salary-based models were offered as new-hire contracts for the physicians at the beginning of the study period in April 2013. Although the number of clinic locations and clinic hours remained stable throughout the 5-year data collection phase, additional factors—increased patient referrals, the growth of regional institutional presence, surgeon experience, or familiarly of ancillary staff—may have influenced the observed results. Metrics such as case number per clinic patient may serve a role in the correction for these discrepancies and may be explored in future, larger scale studies. Although the theoretical incentive to overselect patients for surgery exists, we expect that the physicians in the study group upheld both standard of care and ethical practice when selecting cases. While the increased individual and group productivity was associated with increases in surgeon salary, it should be noted that there was no individual incentive to perform surgery at the ASC compared to the main hospital operating room (OR). Often, scheduling availability determines these decisions.
Data from 1 of the 5 preexisting surgeons were excluded from this analysis as the length of the individual’s pre-RVU interval was limited secondary to early contract opt-in. Nonetheless, inclusion of these data to the group cohort would not have altered the composite statistical significance and nonsignificance of the measured outcomes. At the individual level, no significant differences were measured in the individual’s safety outcomes, although the confidence of these findings is restricted by the limited sample size.
The influence of an incentive-based salary on physician productivity and safety outcomes specific to inpatient procedures should be formally investigated. A 2-year review of the vascular surgery cases performed at our tertiary care hospital exhibited no differences in the 30-day readmission, infection, or complication rates, concomitant with increased physician work-RVU generation, before and after the implementation of a similar incentive-based salary. 13 We hypothesize that comparable findings would be found with the corresponding otolaryngology cases.
The procedures performed in the study cohort were characteristically low-risk operations. The analysis of key indicator cases showed limited differences in the frequencies of such cases between the 2 study periods. At our institution, same-day otolaryngology procedures with an increased safety risk are typically assigned to be performed in the main hospital OR. Although certain preoperative factors are known predictors for adverse outcomes, such as older age at tonsillectomy and the rates of postoperative bleeding, these cases were less likely to be selected for the ASC and therefore had a lower probability of being included in our study. 14 Likewise, procedures scheduled for indications of disordered sleep breathing are mostly scheduled for the hospital setting, particularly when airway difficulties or longer postoperative monitoring are expected.
As the paradigm of payment reform continues to evolve across health care, the prominence of reimbursement linked to quality of care measures will only continue to grow. Passed in 2015, the Medicare Access and CHIP Reauthorization Act (MACRA) mandated the CMS to replace fee-for-service with value-based reimbursement models for Medicare patients. Providers must soon participate in either the Merit-based Incentive Payment System or an advanced alternative payment model, such as an accountable care organization (ACO). 15 According to a 2017 survey, 82% of practicing otolaryngologists will continue to accept established and new Medicare patients. Of those surveyed, 40% currently participate in ACOs and 50% are expected to participate in the Quality Payment Program next year. 16
Therefore, the need for accessibility and transparency of information detailing the benefits and limitations of novel compensation models is more significant than ever before. Previous studies assessing compensation programs in primacy care designed to relate reimbursement to quality of care in the setting of cost containment have demonstrated beneficial patterns of reducing spending associated with improved quality.17,18 However, no reimbursement model embodies a “one-size-fits-all” approach to otolaryngology, as heterogeneity exists amid specialty-specific and institutional-specific characteristics. For example, the contribution that otolaryngology services provide to a hospital’s overall margins needs to be well defined, as a differential exists between various surgical subspecialties. 19 Similarly, activities of teaching, research, and publication should be more heavily favored at academically oriented institutions. 20 In this new era of care, multidisciplinary clinical care and other patient-related activities also need to be considered. Generally, there is a consensus that performance-based payment systems should incorporate a variety of these factors, as illustrated by those defined by the AAO-HNS, summarized in Table 4 . 21
AAO-HNS Essential Principles for a Performance-Based Payment System.
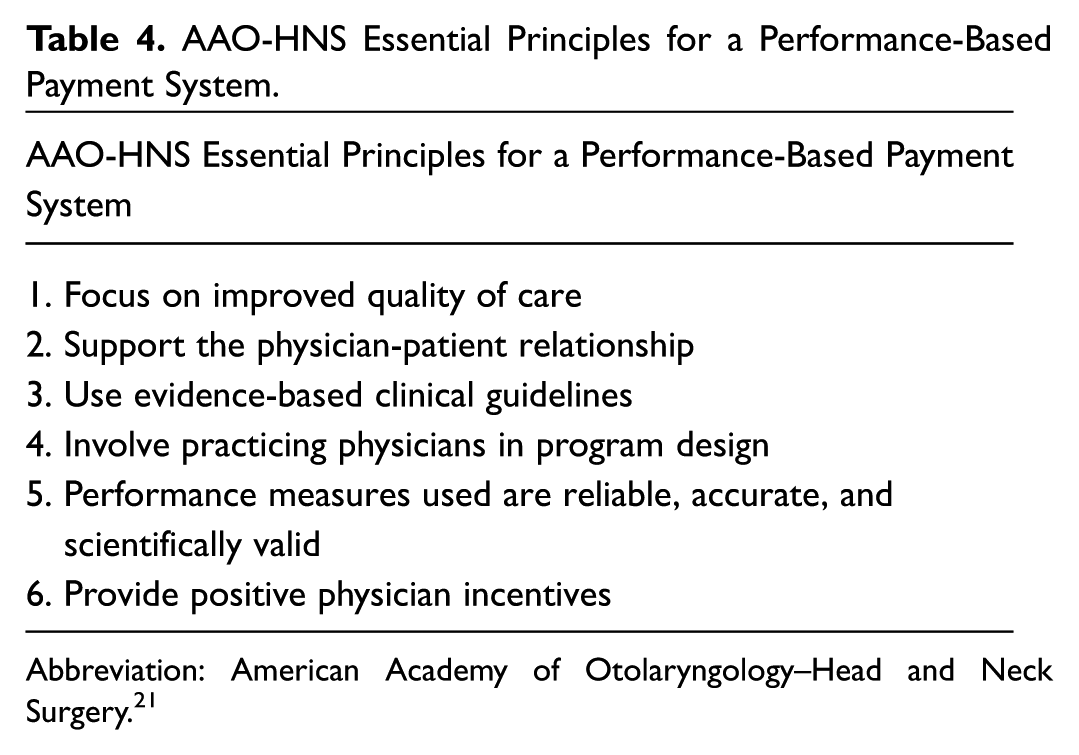
Abbreviation: American Academy of Otolaryngology–Head and Neck Surgery. 21
Additional advocacy efforts have been made to address the national-level shortcomings in the available options for physicians, illustrated by the creation of Reg-ent, position statements on appropriate use criteria, and proposed changes to ambulatory payment classification assignments.22,23 Resources have been made publicly available to physicians considering transitions (available at https://www.entnet.org/content/reimbursement). While the results disclosed in this report provide insight in the context of widespread payment reform, additional studies dedicated to practice outcomes as a consequence of the structure of compensation packages and the subsequent impact on patient access and satisfaction are currently needed.
Conclusions
Within the dynamic landscape of payment reform, the field of otolaryngology is faced with many evolving challenges inclined to the specialty. This report serves to highlight the experience of a hospital-based otolaryngology practice operating in a high-volume ASC. The implementation of a productivity-based compensation program in our institution’s otolaryngology practice was not associated with an increase in adverse outcomes in the setting of increased outpatient surgical volume. This report serves to contribute to a growing body of literature supporting novel compensation programs by providing substantial evidence in support of the advancement of incentive-driven compensation models for otolaryngology practices.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.