
Abstract
Objective
Intranasal corticosteroids (INCSs) are widely utilized for the treatment of allergic rhinitis. Epistaxis is a known adverse effect of INCSs, but it is not known if the risk of epistaxis differs among INCSs.
Data Sources
Systematic review of primary studies identified through Medline, Embase, Web of Science, PubMed Central, and Cochrane databases.
Review Methods
Systematic review was conducted according to the PRISMA standard. English-language studies were queried through February 1, 2018. The search identified randomized controlled trials of INCSs for treatment of allergic rhinitis that reported incidence of epistaxis. An itemized assessment of the risk of bias was conducted for each included study, and meta-analysis was performed of the relative risk of epistaxis for each INCS.
Results
Of 949 identified studies, 72 met the criteria for analysis. Meta-analysis demonstrated an overall relative risk of epistaxis of 1.48 (95% CI, 1.32-1.67) for all INCSs. The INCSs associated with the highest risk of epistaxis were beclomethasone hydrofluoroalkane, fluticasone furoate, mometasone furoate, and fluticasone propionate. Beclomethasone aqueous, ciclesonide hydrofluoroalkane, and ciclesonide aqueous were associated with the lowest risk of epistaxis. Conclusions about epistaxis with use of budesonide, triamcinolone, and flunisolide are limited due to the low number of studies and high heterogeneity.
Conclusions
While a differential effect on epistaxis among INCS agents is not clearly demonstrated, this meta-analysis does confirm an increased risk of epistaxis for patients using INCSs as compared with placebo for treatment of allergic rhinitis.
Allergic rhinitis (AR) is a chronic disease that affects about 20% of the US population. 1 Prevalence worldwide ranges from 10% to 20%, suggesting that >500 million people are affected globally. 2 AR is a heterogenous disorder that can vary in severity. It is characterized by nasal symptoms, including sneezing, itching, congestion, and rhinorrhea, and ocular symptoms, including redness, watering, and itching.3,4 AR can severely affect quality of life, causing headaches, fatigue, and sleep disturbances that impair cognitive and social functioning.4,5 These effects result in a large economic burden, as AR is associated with $4.5 billion a year in direct costs and about 4 million missed school and work days nationally. 6 Comorbid diseases, such as asthma, chronic sinusitis, and upper respiratory infections, exacerbate the burden of disease by increasing morbidity and medical costs for patients. 4
Intranasal corticosteroids (INCSs) represent a well-established method of AR treatment. INCSs decrease inflammation associated with AR and provide symptomatic relief of nasal and ocular symptoms.2,7,8 Current guidelines recommend INCSs as a first-line treatment for AR. 2 Although the safety of topically applied steroids is well recognized, complications (eg, dryness, crusting, and epistaxis) may result with use of these drugs. 6 Some reports suggest that newer topical steroids, such as fluticasone propionate and mometasone furoate, decrease the incidence of local and systemic side effects.6,9 Overall, the benefits of INCSs appear to outweigh the risks among patients with AR. 2
Epistaxis is one of the most commonly reported adverse effects of INCS use. 6 Epistaxis associated with INCS use occurs among 5% to 10% of patients and is usually minor and self-limited. 9 However, the reason for the increased incidence of epistaxis is unclear. Despite reports of nasal mucosal atrophy and septal perforation with INCS use, there is no convincing evidence to support the role of INCSs as a direct cause of atrophy of the sinonasal mucosa.10-12 Some authors suggested mechanical trauma of the septum caused by the sprays, 13 while others posited that direct application of corticosteroids causes chemical trauma. 14 Application of intranasal steroids to the nasal septum as compared with the lateral wall of the nose was observed to result in epistaxis more frequently, although few studies prospectively measured this. 13
Although epistaxis is a known adverse effect of INCSs as a therapeutic class, differences in rates of epistaxis for specific INCS agents have not been well studied. We performed a systematic review with meta-analysis to evaluate the relative risk of epistaxis with the use of different INCSs in the treatment of AR.
Materials and Methods
A systematic review of the English-language literature was performed with the Medline, Embase, Web of Science, PubMed Central, and Cochrane databases. Inclusion criteria for the literature search were defined with the PICOS approach (population, intervention, control, outcome, and study design). Search criteria included all occurrences of the following terms in the title or abstract: allergic rhinitis; ≥1 of epistaxis, adverse event, adverse effect, and complication; and ≥1 of fluticasone, triamcinolone, budesonide, mometasone, beclomethasone, flunisolide, and ciclesonide. Results of the systematic review were reported with the PRISMA standard (Preferred Reporting Items for Systematic Reviews and Meta-analyses; Figure 1 ).
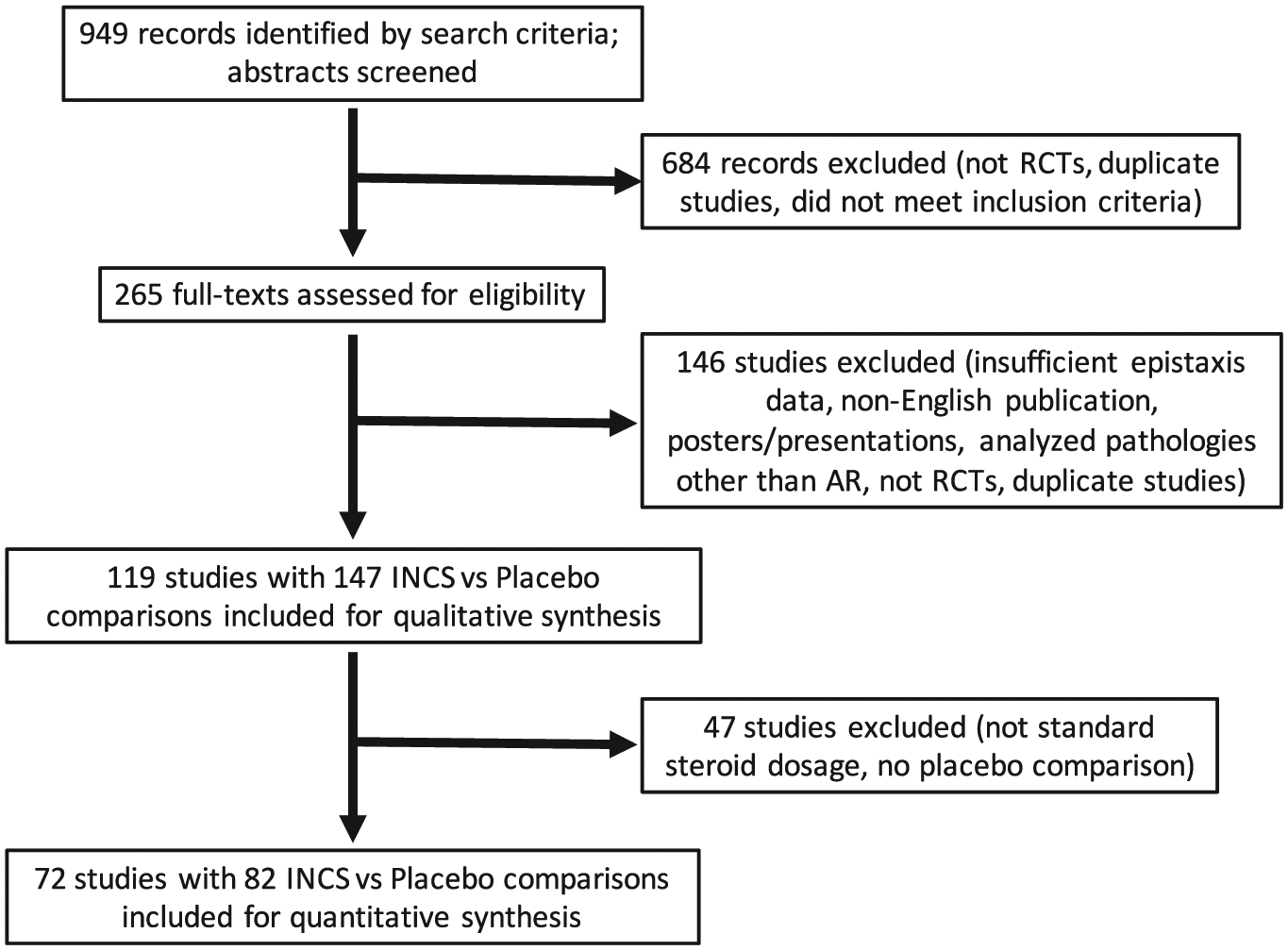
PRISMA flow diagram for the literature selection process. AR, allergic rhinitis; INCS, intranasal corticosteroid; RCT, randomized controlled trial.
Two reviewers (E.L.W., C.M.B.) independently performed the initial eligibility assessment of the identified abstracts in a standardized manner. The abstract of each citation was screened for relevance to the assessment of the use of INCSs to treat AR and the reporting of epistaxis as an adverse event. Studies were included that enrolled patients ≥2 years old who were treated with an INCS (beclomethasone, budesonide, ciclesonide, flunisolide, fluticasone furoate, fluticasone propionate, mometasone furoate, triamcinolone) in at least 1 study arm for an indication of AR and that recorded incidence of epistaxis. Only randomized controlled trials were included, and duplicate records were removed. Irrelevant citations and case reports were excluded.
The full texts of the remaining citations were then obtained and reviewed in detail by 4 reviewers (E.L.W., C.M.B., B.H.A., and W.C.H.). Studies that lacked full-text manuscripts or were non-English publications were excluded. Studies that did not provide patient demographics and quantitative epistaxis data were excluded. Studies examining pathologies other than AR were also excluded. Studies that were not randomized controlled trials or were found to be duplicate studies on full-text review were excluded. Only remaining studies were included for qualitative synthesis.
Using a standardized extraction form, 4 reviewers (E.L.W., C.M.B., B.H.A., and W.C.H.) collectively gathered the data from full-text articles, including criteria for patient selection, study design, source of individual patient data, duration of study, type of AR, age of patients, INCSs evaluated, and incidence of epistaxis. The principal summary measures were incidences of epistaxis after treatment with a specific INCS. Raw data were extracted for the number of patients treated with individual INCSs, placebo, or other medications and subsequent epistaxis incidences.
Only studies that examined standard INCS dosages were included for quantitative meta-analyses. These included beclomethasone hydrofluoroalkane (HFA; 320 or 300 mg), beclomethasone aqueous (336 or 400 µg), budesonide (128 or 256 µg), ciclesonide HFA (74 or 80 µg), ciclesonide aqueous (200 µg), fluticasone furoate (110 µg), fluticasone propionate (200 µg), mometasone furoate (200 µg), and triamcinolone (220 µg). Distinct comparisons between a specific INCS formulation/dose and a placebo were recorded. Studies that evaluated a steroid without comparison with a placebo were excluded.
Meta-analyses were performed for 9 distinct INCS formulations. A risk ratio (95% CI) for epistaxis for each INCS as compared with placebo was calculated for included studies. The incidence of epistaxis following INCS and placebo treatment were recorded or derived from each study. Forest plots depicting the cumulative risk ratios (95% CIs) of epistaxis for all INCSs were generated with a Mantel-Haenszel random-effects model. I2 values were recorded to determine study heterogeneity. The meta-analysis was performed with RevMan 5.3.5 software (Cochrane Group, London, United Kingdom).
Risk of bias was assessed at the study level by 4 reviewers (E.L.W., C.M.B., B.H.A., and W.C.H.) using the Cochrane Risk of Bias Assessment Tool to examine each study’s sequence generation, allocation concealment, performance bias, detection bias, attrition bias, reporting bias, and any other sources of biases. 15 Risk of bias was determined independently by the reviewers for each article to assess the strength of the study design.
Results
The initial literature review identified 949 articles, which were screened for relevance to the assessment of use of INCSs to treat AR and the incidence of epistaxis ( Figure 1 ). After screening of abstracts and removal of studies that were not randomized controlled trials, did not meet inclusion criteria, or were duplicate studies, a total of 265 articles were included for full-text review. Of the full texts reviewed, 146 were excluded from qualitative analysis because insufficient data were reported, manuscripts were from non-English publications, full text was not available, pathologies other than AR were analyzed, studies were not RCTs, or studies were duplicates. Forty-seven studies were excluded from quantitative review because they did not analyze a standard INCS dosage or they lacked comparison with a placebo. Ultimately, 72 articles with 82 distinct INCS-versus-placebo comparisons were included for meta-analysis.
Risk of bias was assessed for each included study ( Figure 2 ). Allocation concealment selection bias was unclear for a large number of studies (57 of 72, 79.2%) because, although test subjects were generally randomized to treatment groups, the methods did not often specifically state how randomization was performed. There was a low risk of bias for the majority of items across the included studies. Publication bias was not apparent across the 72 included studies ( Figure 3 ).
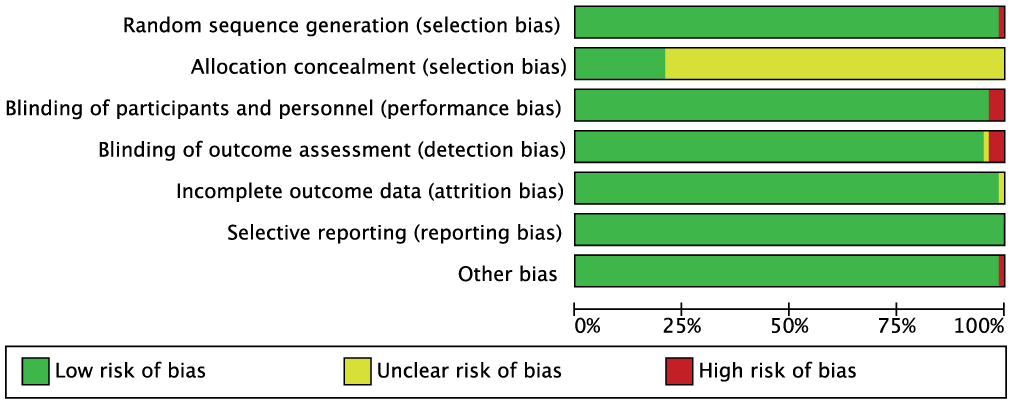
Risk of bias: review authors’ judgment about each item, presented as a percentage across all included studies.
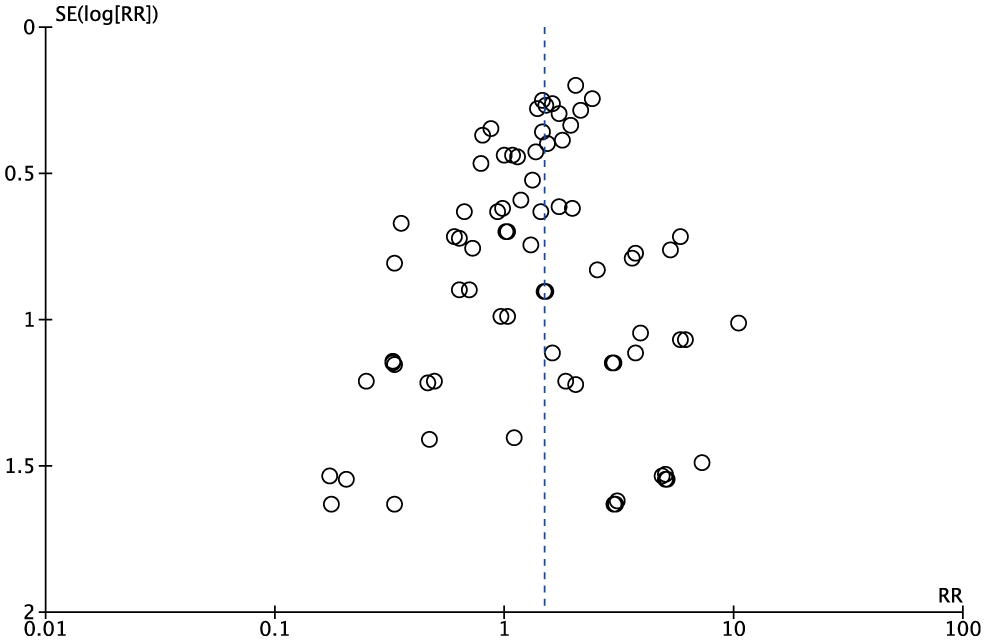
Funnel plot for included intranasal corticosteroid sprays vs placebo comparisons.
The age range of study participants among all studies was 2 to 82 years ( Table 1 ). The duration of studies ranged from 2 weeks to 12 months. For all included comparisons, meta-analysis demonstrated an overall risk ratio of 1.48 (95% CI, 1.32-1.67; I2 = 0%) for epistaxis. Patients treated with beclomethasone HFA, fluticasone furoate, and mometasone furoate had an increased risk of epistaxis as compared with those treated with placebo. The risk ratio for patients treated with beclomethasone HFA was 2.35 (95% CI, 1.06-5.20 I2 = 0%; Figure 4B ).16-21 The risk ratio for patients treated with fluticasone furoate was 1.85 (95% CI, 1.46-2.34; I2 = 0%; Figure 5 ).22-36 The risk ratio for patients treated with mometasone furoate was 1.48 (95% CI, 1.06-2.07; I2 = 3%; Figure 6 ).37-50 Fluticasone propionate was associated with an intermediate risk ratio of 1.36 (95% CI, 1.00-1.85; I2 = 0%; Figure 7 ).17,48,51-65
INCS-Related Epistaxis: Meta-analyses.
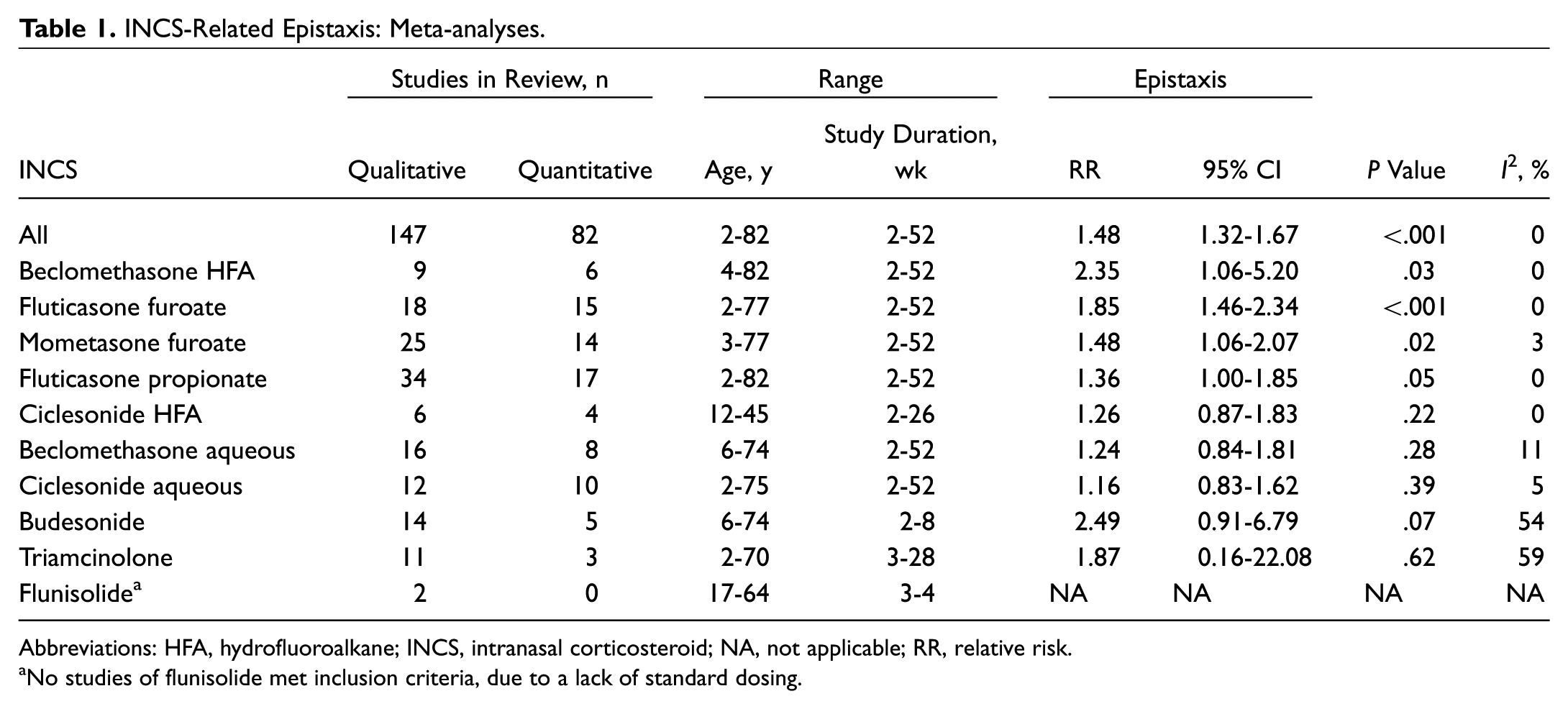
Abbreviations: HFA, hydrofluoroalkane; INCS, intranasal corticosteroid; NA, not applicable; RR, relative risk.
No studies of flunisolide met inclusion criteria, due to a lack of standard dosing.
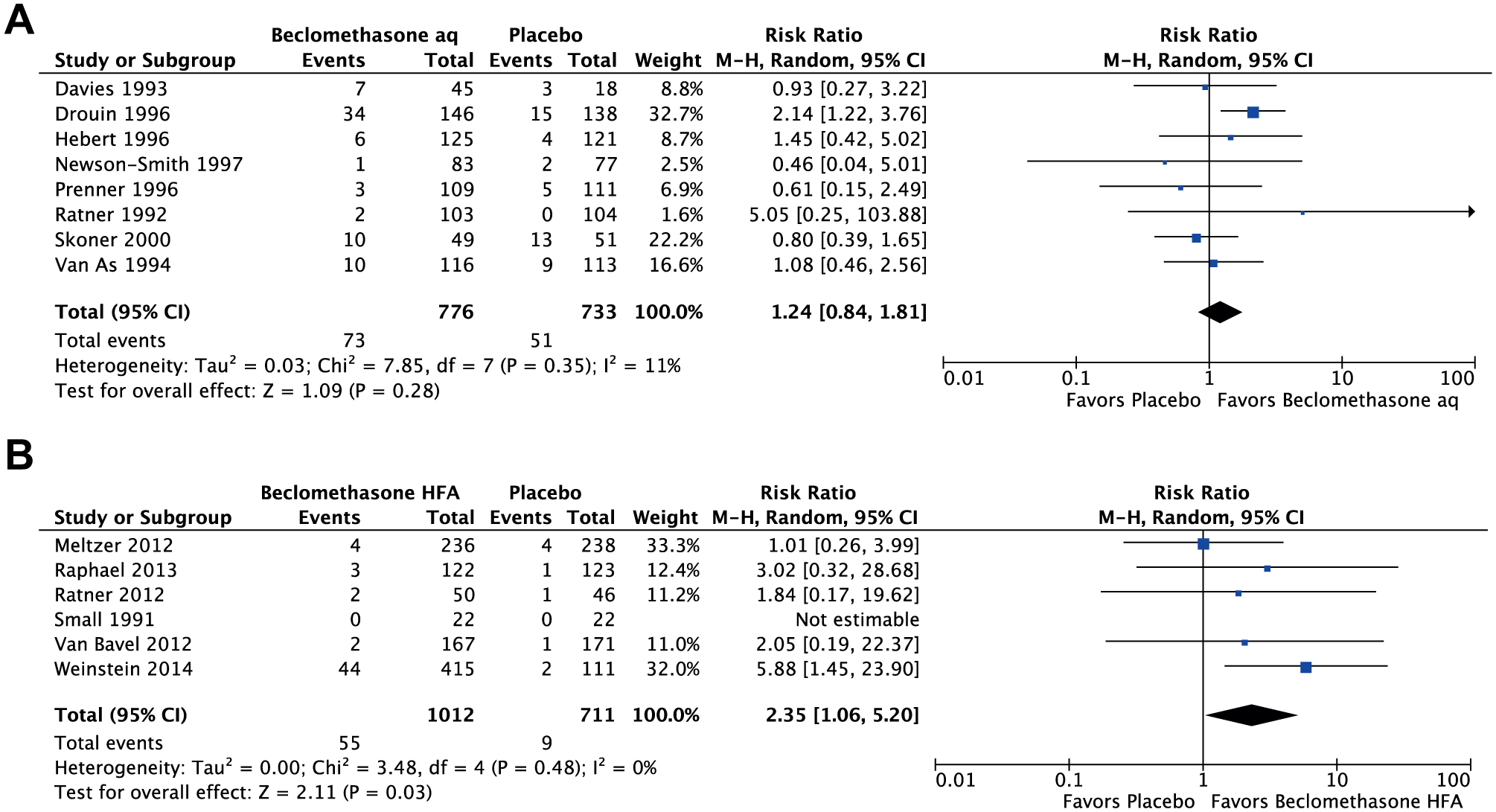
Meta-analysis of risk of epistaxis for (A) beclomethasone aqueous vs placebo and (B) beclomethasone hydrofluoroalkane vs placebo. aq, aqueous; HFA, hydrofluoroalkane; M-H, Mantel-Haenszel.
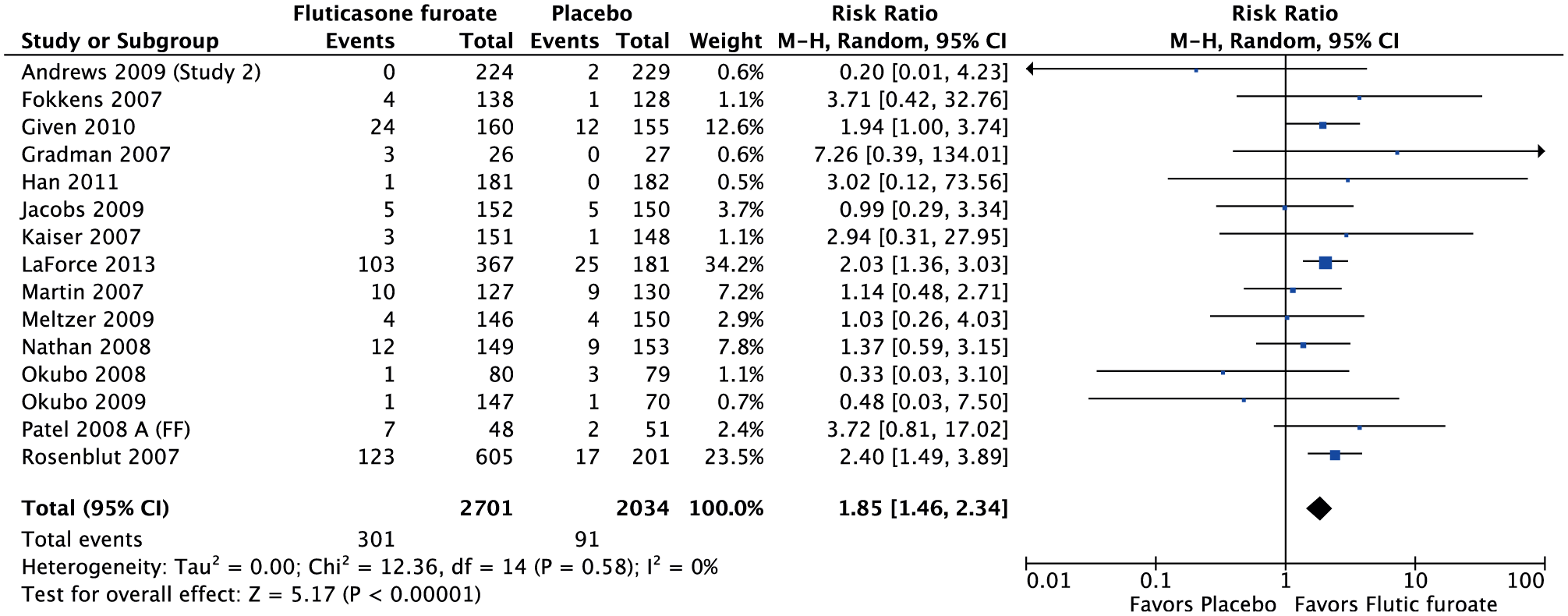
Meta-analysis of risk of epistaxis for fluticasone furoate vs placebo. M-H, Mantel-Haenszel.
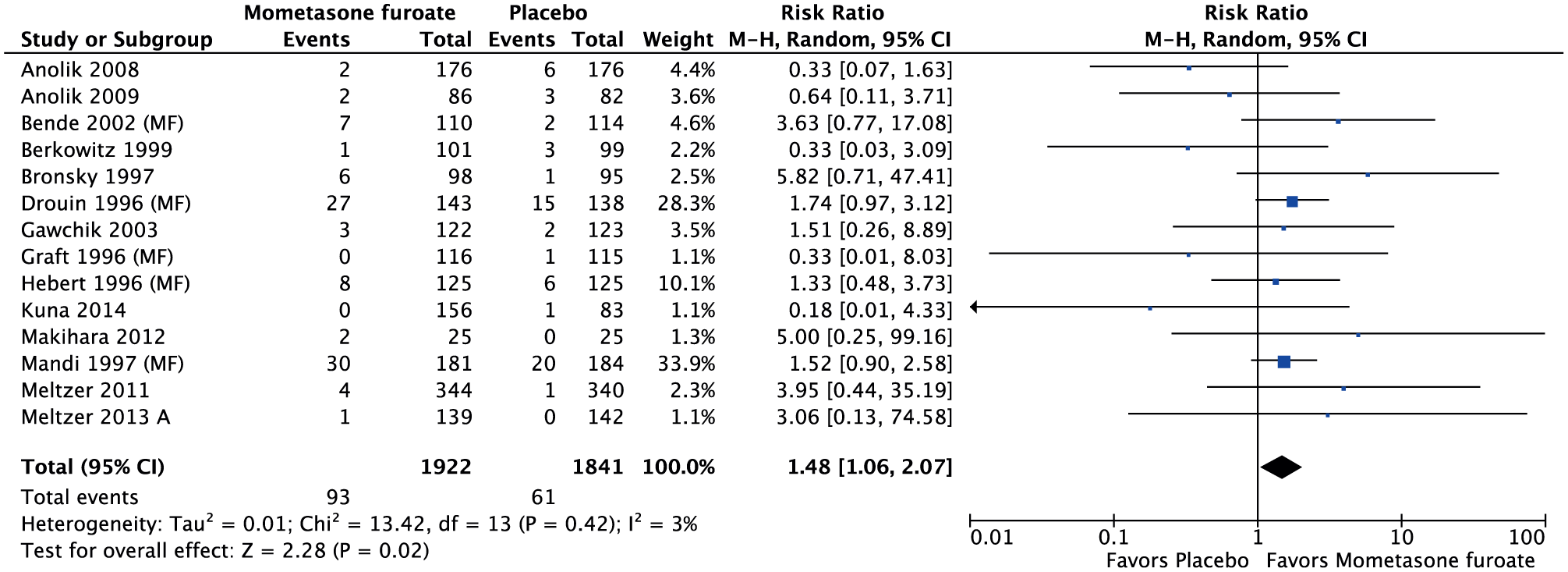
Meta-analysis of risk of epistaxis for mometasone furoate vs placebo. M-H, Mantel-Haenszel.
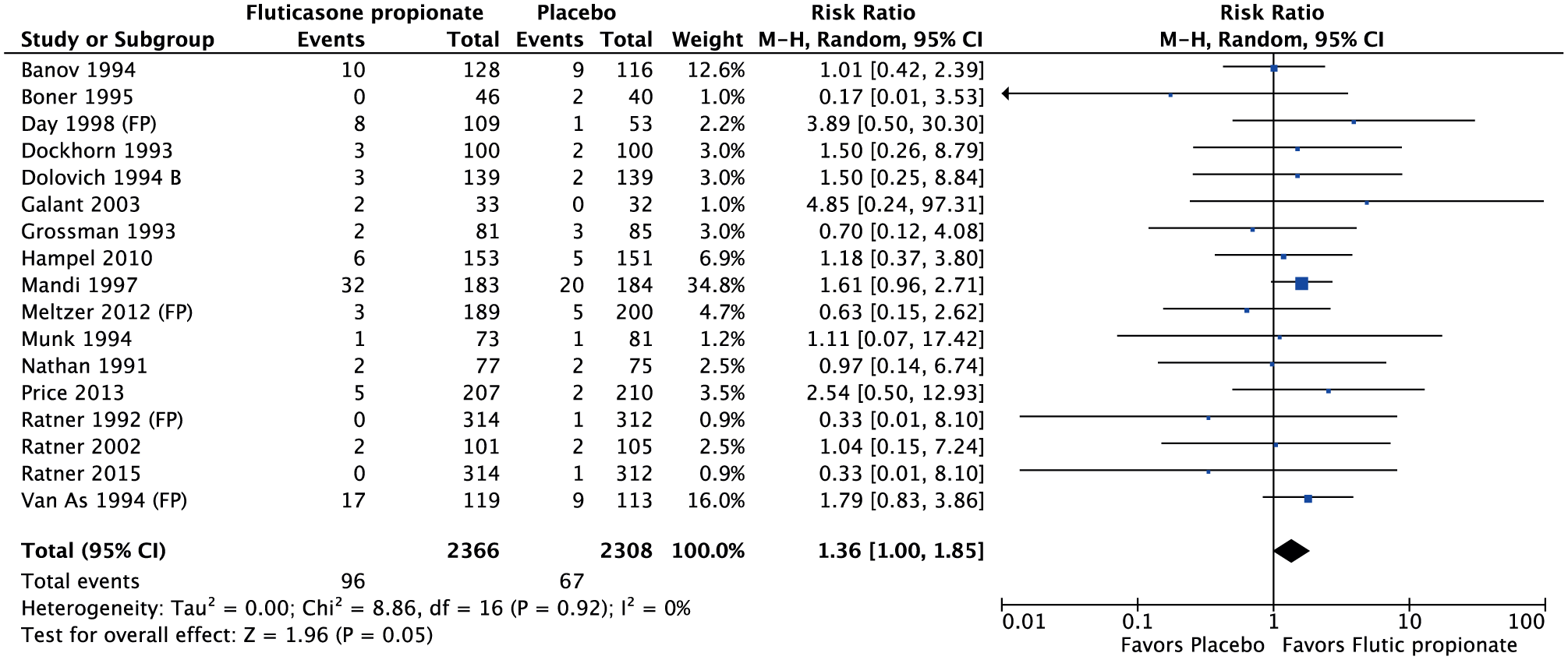
Meta-analysis of risk of epistaxis for fluticasone propionate vs placebo. M-H, Mantel-Haenszel.
Patients treated with beclomethasone aqueous, ciclesonide HFA, and ciclesonide aqueous did not have an elevated risk of epistaxis as compared with placebo. The risk ratio for patients treated with ciclesonide HFA was 1.26 (95% CI, 0.87-1.83; I2 = 0%; Figure 8B ).66-69 The risk ratio for patients treated with beclomethasone aqueous was 1.24 (95% CI, 0.84-1.81; I2 = 11%; Figure 4A ).42,45,62,65,70-73 The risk ratio for patients treated with ciclesonide aqueous was 1.16 (95% CI, 0.83-1.62; I2 = 0%; Figure 8A ).74-81
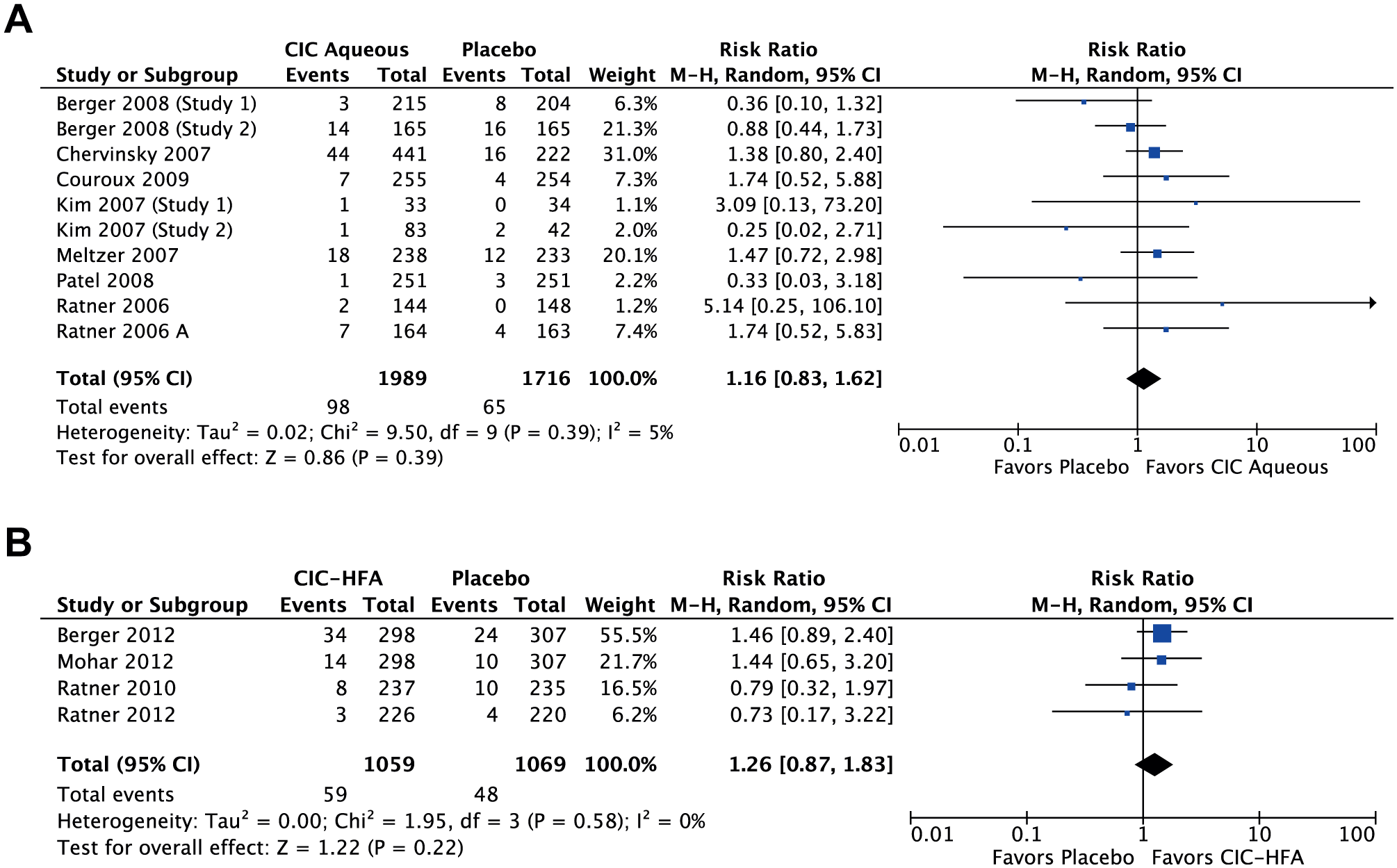
Meta-analysis of risk of epistaxis for (A) ciclesonide aqueous vs placebo and (B) ciclesonide hydrofluoroalkane vs placebo. CIC, ciclesonide; HFA, hydrofluoroalkane; M-H, Mantel-Haenszel.
The risk ratio for patients treated with budesonide was 2.49 (95% CI, 0.91-6.79; I2 = 54%; Figure 9 ); only 5 studies met inclusion criteria with moderately high heterogeneity.39,53,82,83 The risk ratio for patients treated with triamcinolone was 1.87 (95% CI, 0.16-22.08; I2 = 59%; see Supplemental Figure S1, available in the online version of the article); only 3 studies met inclusion criteria with high heterogeneity.84-86 No studies on flunisolide met inclusion criteria, due to lack of standardized dosing, and meta-analysis was not performed.
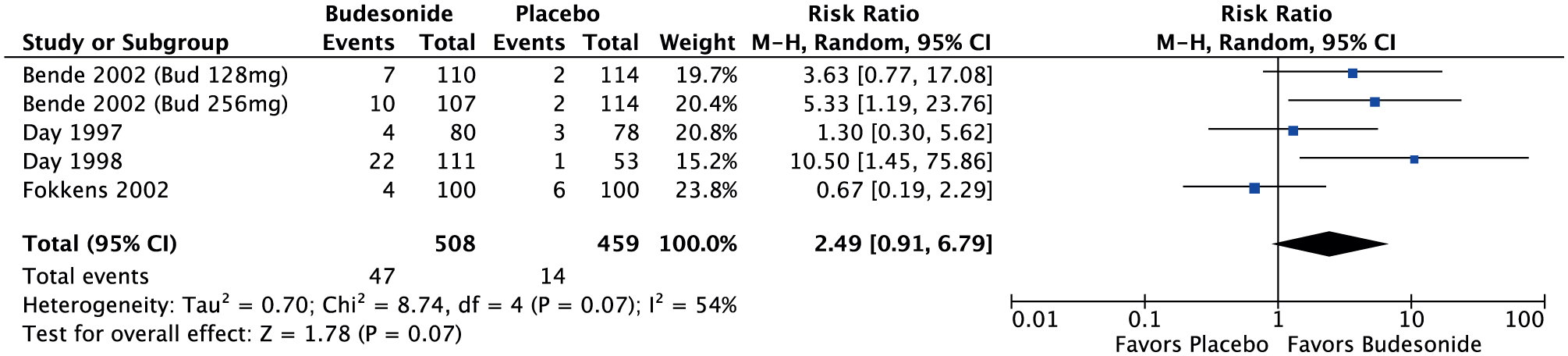
Meta-analysis of risk of epistaxis for budesonide vs placebo. M-H, Mantel-Haenszel.
Discussion
Current guidelines for AR recommend intranasal steroid sprays as a first-line treatment.87,88 Although the safety of topically applied intranasal steroids is well recognized, epistaxis is one of the most common adverse effects. 9 Newer steroid formulations were reported to have fewer systemic adverse effects, but differences in rates of epistaxis among various INCS formulations have not been well studied.6,9,89
Our findings indicate an increased relative risk of epistaxis versus placebo among several commonly prescribed INCSs for AR. The INCSs associated with an increased risk of epistaxis as compared with placebo were beclomethasone HFA, fluticasone furoate, mometasone furoate, and fluticasone propionate. There was a lower risk of epistaxis with use of beclomethasone aqueous, ciclesonide HFA, and ciclesonide aqueous. Conclusions about the risk of epistaxis associated with use of budesonide and triamcinolone are limited due to the low number of studies and high heterogeneity. Risk of epistaxis associated with the use of flunisolide was not analyzed, due to inadequate studies meeting our inclusion criteria.
A direct assessment of significant differences among INCS agents was not attempted in the present study design. While a comparable effect on epistaxis among different INCSs cannot be excluded, due to overlapping confidence intervals, this meta-analysis of randomized controlled trials is a first step in determining whether there are important clinical implications for patients with AR requiring long-term INCSs for maintenance. Epistaxis, while often minor and self-limiting, can result in lack of medication compliance, cause frustration to the patient and provider, and result in additional procedures, medications, or ineffective treatments. 90 Prescribers should be aware of which INCSs may place patients at a higher risk for epistaxis, and they should consider selecting an INCS with a lower risk of epistaxis for patients with recurrent or persistent epistaxis. Further prospective studies are needed to definitively compare the risks of epistaxis from use of specific INCSs.
Interestingly, there was an increased relative risk of epistaxis with use of the nonaqueous HFA formulation of beclomethasone but no increased risk with use of the aqueous formulation of beclomethasone. In contrast, neither the aqueous nor HFA formulation of ciclesonide was associated with an increased relative risk of epistaxis. Intranasal HFA aerosols are dry formulations that are thought to limit the postnasal drip and bitter aftertaste associated with some aqueous sprays, which potentially lead to reduced medication adherence.91,92 From our findings, it cannot be generally concluded that aqueous sprays are less likely than HFA formulations to result in an increased risk of epistaxis.
There are several limitations with our meta-analysis. For many of these studies, epistaxis was included as a secondary outcome, often as part of a larger safety evaluation of the steroid. Epistaxis was not often the primary outcome of study, and our analysis cannot account for the heterogeneity in the study designs of the included studies, such as the age of participants and the study duration. However, adverse effects were routinely collected in the randomized controlled trials included in our systematic review. While there could be minor variations in INCS dosage and/or reporting of side effects among young children included in our study, epistaxis is a common adverse effect readily reportable by patients.
Additionally, only studies that examined standard recommended doses for each steroid formulation were included for analysis. Thus, nonstandard doses or formulations were not included in these results. All studies in this meta-analysis were randomized controlled trials that investigated at least 1 intranasal steroid formulation against a placebo nasal saline spray. It did not include studies that compared one INCS with another without a placebo arm. It is also unclear whether these findings can be generalized to patients with nonallergic chronic rhinitis, which should be the subject of additional study. Furthermore, length of follow-up varied among studies.
Further prospective cohorts comparing specific INCS formulations would better elucidate comparative epistaxis risks and safety profiles. This would have utility in minimizing epistaxis among AR patients being treated with INCSs, identifying and selecting the appropriate INCSs for AR patients susceptible to epistaxis, and optimizing treatment adherence.
Conclusions
While a differential effect on epistaxis among different INCS agents is not clearly demonstrated in the present study design, this systematic review and meta-analysis of randomized controlled trials does confirm increased risk of epistaxis for patients using INCSs as compared with placebo for treatment of AR. Further prospective studies are needed to definitively compare the epistaxis risks with the use of specific INCSs.
Author Contributions
Disclosures
Supplemental Material
OTO832277_suppl_mat – Supplemental material for Epistaxis Risk Associated with Intranasal Corticosteroid Sprays: A Systematic Review and Meta-analysis
Supplemental material, OTO832277_suppl_mat for Epistaxis Risk Associated with Intranasal Corticosteroid Sprays: A Systematic Review and Meta-analysis by Eric L. Wu, William C. Harris, Casey M. Babcock, Bailin H. Alexander, Charles A. Riley and Edward D. McCoul in Otolaryngology–Head and Neck Surgery
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Supplemental Material
Additional supporting information is available in the online version of the article
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.