
Abstract
Objective
To evaluate outcomes of free flaps in low- versus high-risk American Society of Anesthesiologists (ASA) classes utilizing a standardized perioperative clinical pathway.
Study Design
Case series with chart review.
Setting
Single tertiary care academic institution.
Subjects and Methods
Data were collected from 301 patients who underwent 305 free flap reconstructions for head and neck defects from January 2012 to March 2016 by a single surgeon (M.M.). A standardized perioperative clinical pathway was utilized for all patients, aimed at abbreviating hospital stay and minimizing intensive care unit stay. Data included ASA classification, comorbidities, length of hospitalization, intensive care unit stay, 30-day mortality/readmission, discharge disposition, flap survival, and postoperative complications. Low-risk ASA classes were defined as 1 and 2 (n = 53) and high risk as 3 and 4 (n = 248).
Results
Total medical complication rates (P = .012) were mildly increased in the high-risk group, as a result of increased minor—not major—medical complication rates (P = .007). Discharge to a nursing or rehabilitation facility was found to be more common in the high-risk group (P = .024). All other outcomes were not statistically different between the cohorts.
Conclusion
The ASA classification system is a validated tool in determining perioperative risk. We found that minor medical complications and discharge to a rehabilitation/nursing facility were increased in the high-risk ASA classes; otherwise, there were no statistical differences between the groups. These findings suggest that the ASA classification may be helpful for preoperative discharge planning and counseling but should not be used for patient selection or to assess candidacy for the procedure.
Keywords
Reconstructive techniques for head and neck surgical defects have evolved over the past 2 decades, with free flap reconstruction being performed with increasing frequency and greater efficiency. The goal of reconstruction in head and neck surgery is to restore not only form but also function, and free tissue transfer (FTT) can often provide for better functional and aesthetic outcomes.1,2 The ideal reconstruction substrate provides maximum functionality while minimizing morbidity. 3 With a success rate greater than 90% to 95%,1,4-13 microvascular FTT is a consistent and effective alternative and, in many cases, considered the gold standard for reconstruction of certain head and neck defects. 9
FTT is an extensive surgical procedure that requires a patient to be under general anesthesia for a significant amount of time9,12; as such, preoperative risk assessment becomes critical for patient selection, perioperative management, and anticipation of the acuity of care needed in each case. Previous studies evaluated age as an outcome predictor for patients undergoing head and neck free flap reconstruction. They found that advanced age is consistently associated with a higher incidence of major complications, medical complications, and longer lengths of hospital stay.9,13,14 Although a patient’s age is an important factor to consider, it is widely accepted that it is not the most representative measure of a patient’s overall health status, which led to efforts in identifying other outcome predictors. Hwang et al 15 suggested using the patient’s comorbidities and American Society of Anesthesiologists (ASA) class for this purpose. The ASA classification system 16 ( Table 1 ) is used primarily by anesthesiologists to assess a patient’s global physical status prior to surgery. 17 First introduced in 1941, the ASA Physical Status Classification System was shown to be a reliable predictor of perioperative morbidity and mortality. 18 This classification system simplifies multiple factors affecting patient health into 1 measurable value, which can be interpreted and understood by other providers and which serves to adequately inform and consent patients regarding their perioperative risk. 19
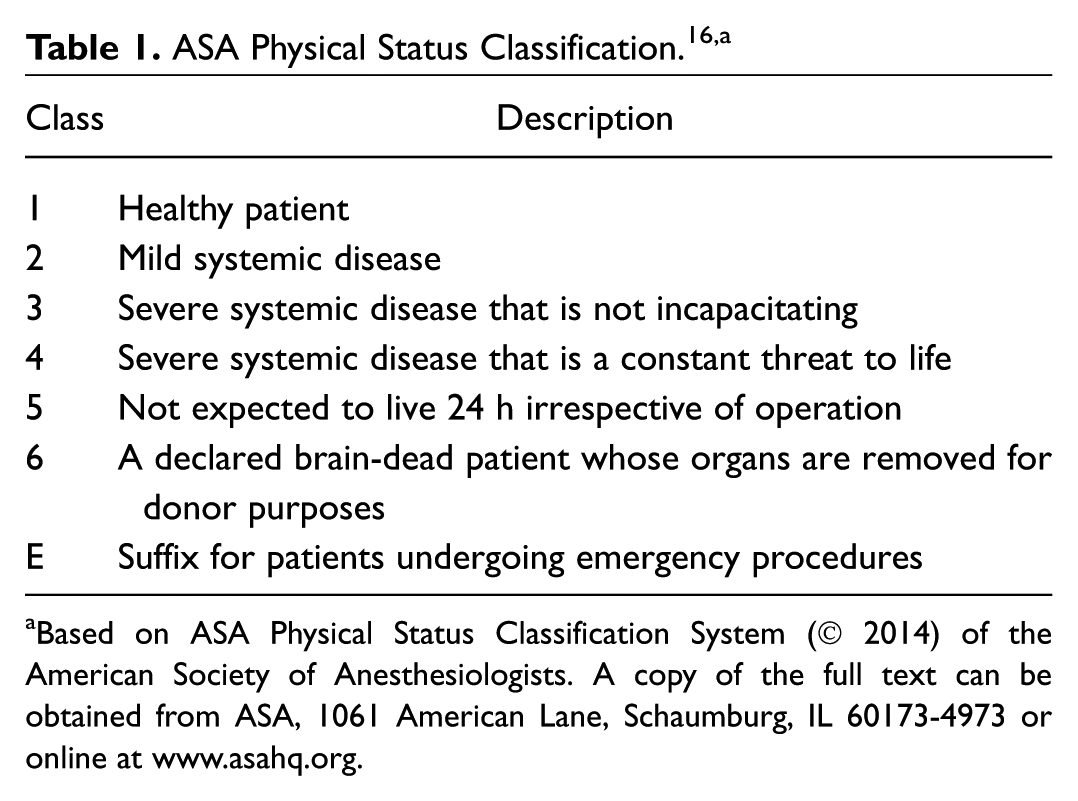
Based on ASA Physical Status Classification System (© 2014) of the American Society of Anesthesiologists. A copy of the full text can be obtained from ASA, 1061 American Lane, Schaumburg, IL 60173-4973 or online at www.asahq.org.
While several studies correlated higher ASA status with increased morbidity and mortality among patients following FTT,1,5-10,12-15,20-22 to our knowledge, no study has assessed its predictive value in the context of a perioperative clinical pathway for patients undergoing free flap. Since 2012, all patients undergoing FTT for head and neck defects at our institution are treated under a dedicated clinical pathway aimed at an abbreviated hospital stay. Under this model, patients are not scheduled to go to the intensive care unit (ICU) postoperatively, unless they are hemodynamically unstable or there are significant intraoperative complications. Similarly, planned discharge occurs at postoperative day 5 for all patients, regardless of type of flap performed, age, or comorbidities.
We sought to assess the value of preoperative ASA class as a predictor for surgical and perioperative outcomes among patients undergoing FTT under a dedicated clinical pathway.
Patients and Methods
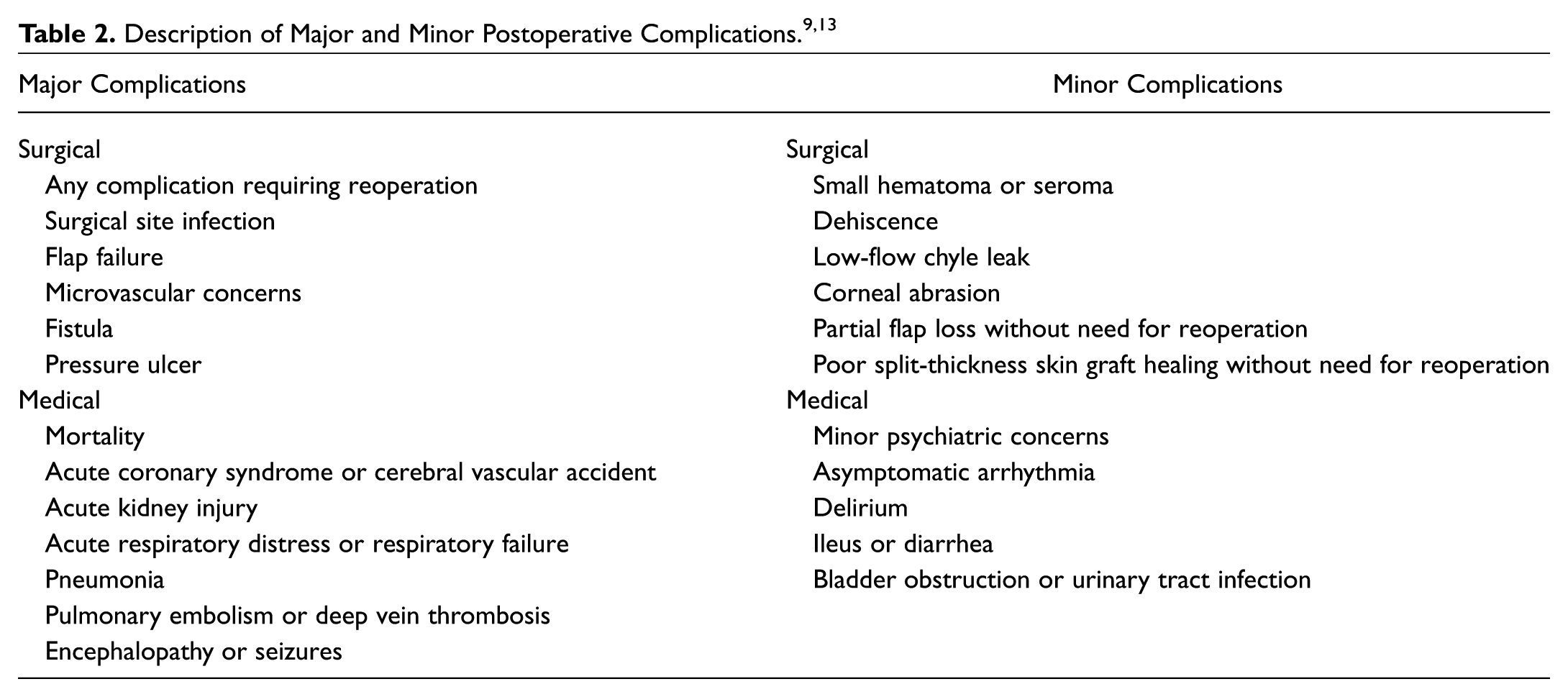
The study was approved by the University of Arkansas for Medical Sciences Institutional Review Board. We performed a retrospective chart review of 305 surgical procedures performed by the senior author (M.M.) on 301 consecutive patients who underwent FTT for head and neck defects between January 2012 and March 2016. No patients were excluded from the series. Prior to surgery, each patient was evaluated by a board-certified anesthesiologist and assigned a score based on the patient’s medical history, comorbidities, and acuity of the procedure. Information retrieved from the charts included demographic information, ASA classification per anesthesia records, preoperative comorbidities, ICU and hospital length of stay, 30-day mortality and reoperation rates, discharge disposition, flap outcomes, and postoperative complications (major and minor). Criteria for major and minor medical and surgical complications are outlined in Table 2 . The delineations of each group are consistent with prior studies by Özkan et al 9 and Clark et al 13 regarding perioperative morbidity among patients undergoing free flap.
For statistical analysis, patients were grouped into low risk (ASA class 1 and 2) and high risk (ASA class ≥3). The primary end point of the study was to compare perioperative morbidity and mortality between these groups; secondary end points were to compare length of ICU stay, hospital stay, flap outcomes, discharge disposition, and rate of readmission. Association between variables was tested with Fisher’s exact test or Student’s t test (SPSS 22; IBM, Chicago, Illinois). Statistical alpha was set at 0.05, and univariate analysis was performed in all cases.
Results
A total of 305 FTTs were included in the cohort; demographic information is presented in Table 3 . Indications for surgery, in descending order of frequency, were malignancy (n = 240, 78.7%), benign tumors (n = 25, 8.2%), osteoradionecrosis (n = 21, 6.9%), trauma (n = 10, 3.3%), and chronic wounds (n = 9, 2.9%). The mean age was 58 years, with the majority of the cohort being male (62%) and Caucasian (86%). There was no statistical difference in sex between the cohorts. A significant difference was identified in mean age between the groups: 42.1 years for the low-risk cohort versus 62.7 years for the high-risk cohort (P < .0001). Free flaps were harvested from the following sites: anterolateral thigh (n = 112), radial forearm (n = 86), fibula (n = 70), latissimus dorsi (n = 14), scapula (n = 8), vastus lateralis (n = 7), and other (n = 8).
Demographic and Clinical Characteristics by ASA Risk Group.
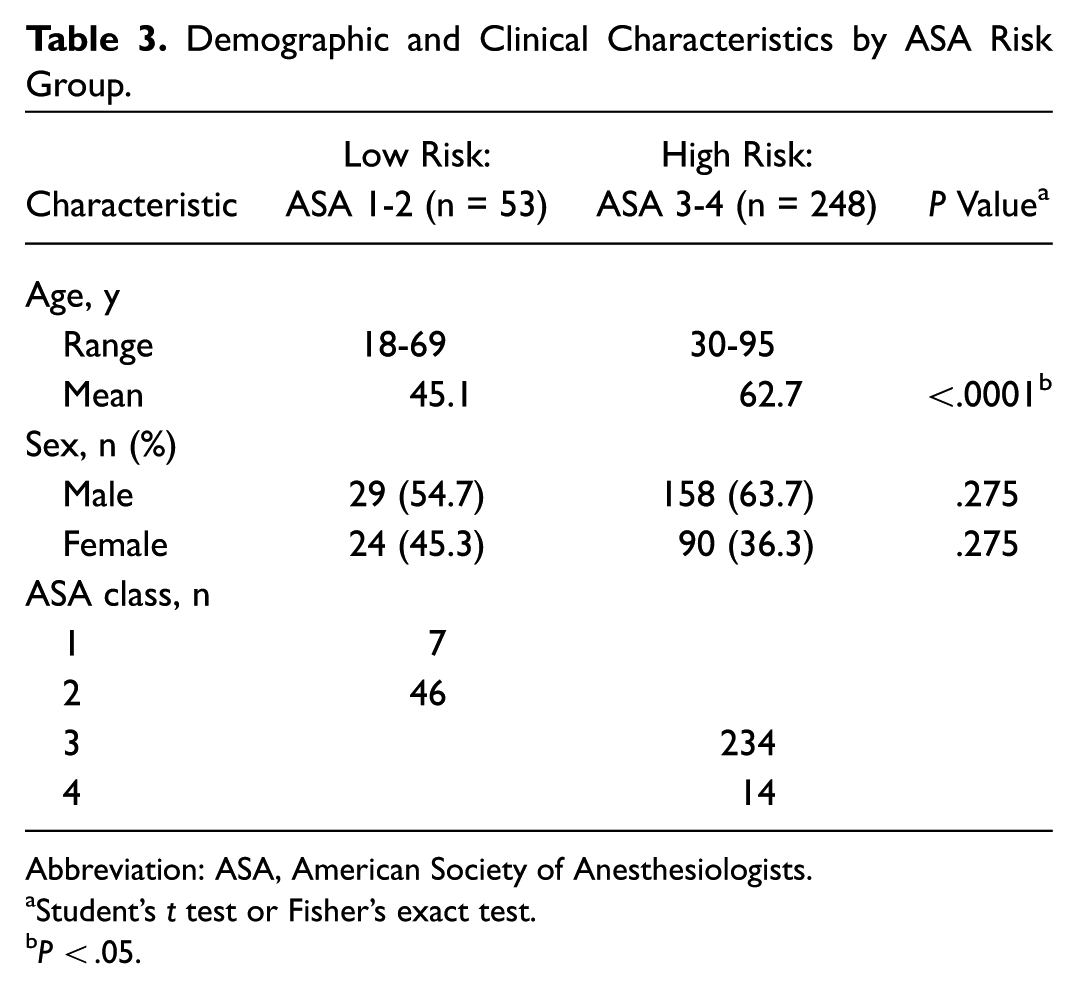
Abbreviation: ASA, American Society of Anesthesiologists.
Student’s t test or Fisher’s exact test.
P < .05.
The distribution of ASA class within the cohort was as follows: ASA 1 (n = 7), ASA 2 (n = 46), ASA 3 (n = 234), and ASA 4 (n = 14). ASA classification and frequency of preoperative comorbidities are presented in Table 4 . Perioperative variables are presented in Table 5 , including ICU and hospital length of stay, 30-day mortality and reoperation rates, discharge disposition, flap outcomes, and postoperative complications (major and minor).
Comparative Frequencies of Preoperative Comorbidities between the Low- and High-Risk ASA Groups. a
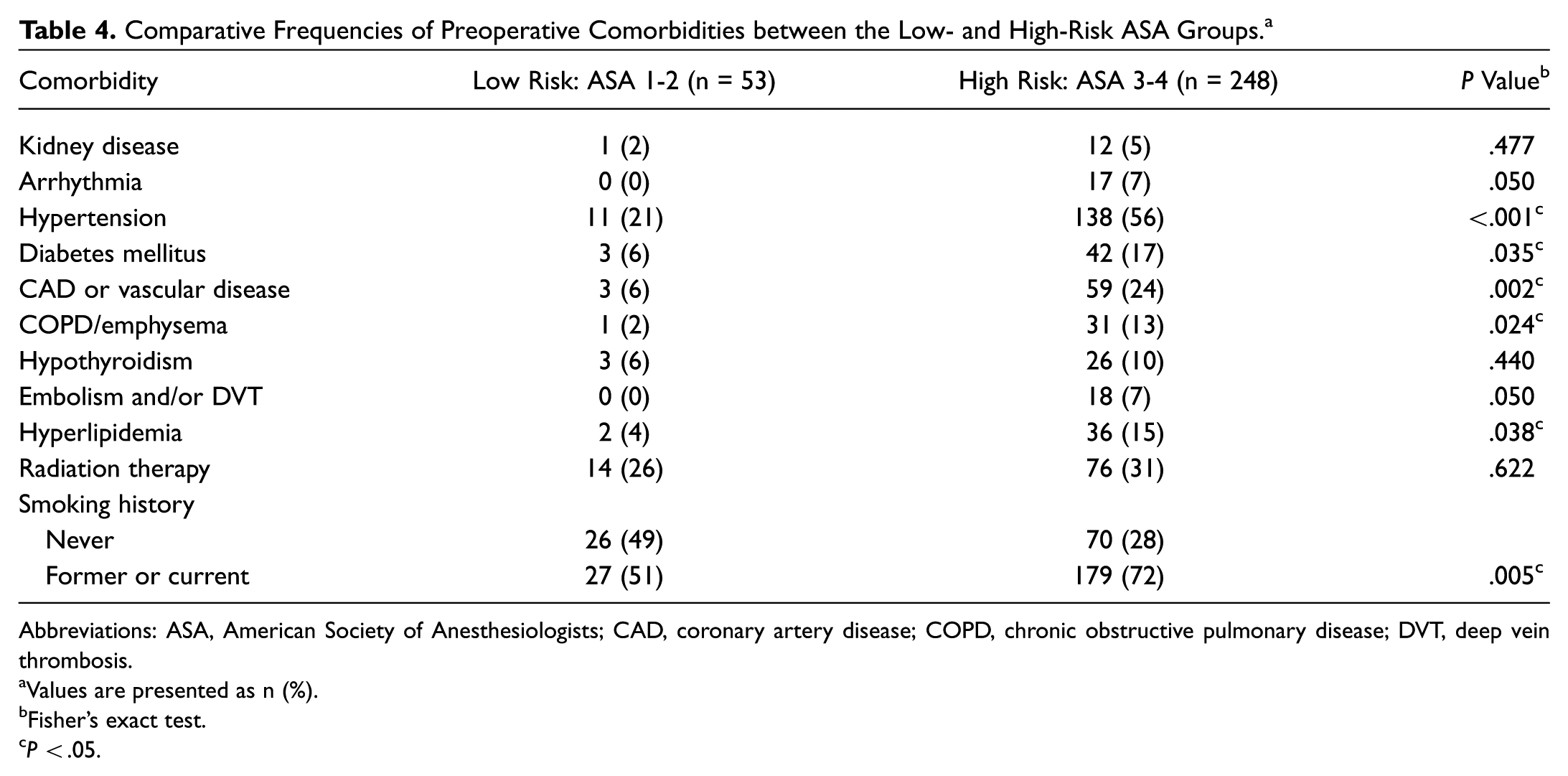
Abbreviations: ASA, American Society of Anesthesiologists; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; DVT, deep vein thrombosis.
Values are presented as n (%).
Fisher’s exact test.
P < .05.
ASA-Stratified Surgical Outcomes: Comparative Analysis between Low- and High-Risk Groups. a
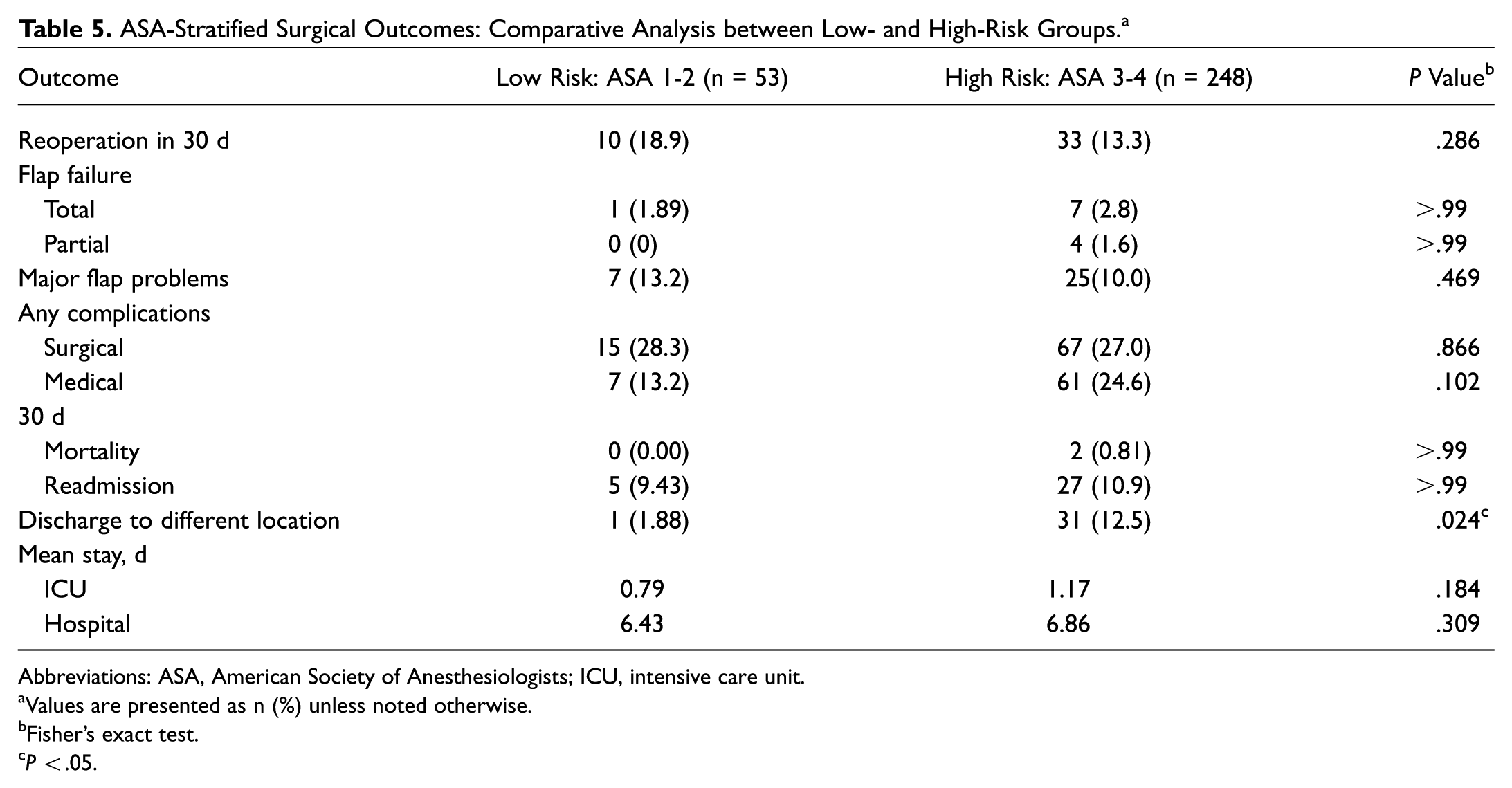
Abbreviations: ASA, American Society of Anesthesiologists; ICU, intensive care unit.
Values are presented as n (%) unless noted otherwise.
Fisher’s exact test.
P < .05.
Overall, the free flap failure rate was 2.66%, and there was no statistically significant difference between the low- and high-risk ASA groups. We found that high-risk patients were more likely to be discharged to a different location, including nursing facility or rehabilitation facility (P = .024); to have more minor medical complications per person (P = .006); and to have more total medical complications per person (P = .012).
Interestingly, we found no significant difference between the low- and high-risk groups on the following measures: total and partial flap failure rates, minor and major surgical complication rates, major medical complication rates, 30-day mortality rates, 30-day readmission rates, mean days spent in the ICU, and mean total admission days (
Patient-Adjusted Relative Risk ASA-Stratified Surgical Outcomes: Comparative Analysis between Low-and High-Risk Groups. a
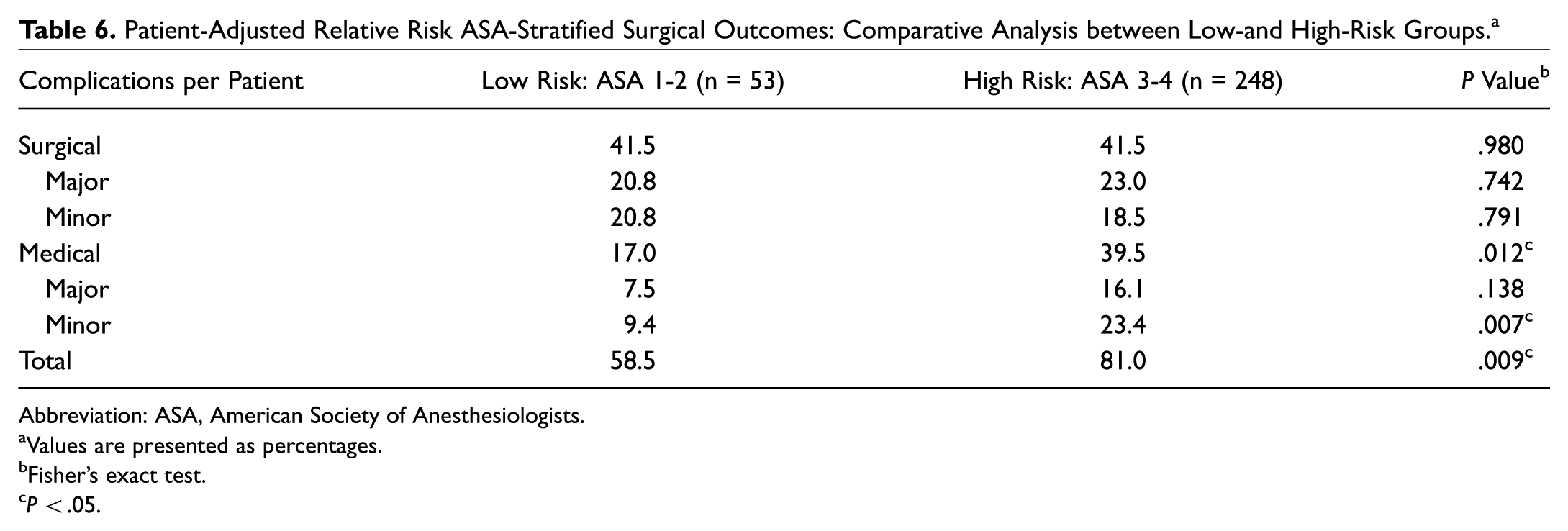
Abbreviation: ASA, American Society of Anesthesiologists.
Values are presented as percentages.
Fisher’s exact test.
P < .05.
Discussion
For patients with head and neck defects, reconstruction can provide aesthetic as well as functional improvement. 1 Microvascular FTT has become a reliable method for 1-step reconstruction, with high success rates (90%-95%).8,12,20,23 Although success rates are high, FTT continues to be a complicated and extensive procedure, with reported mean operative times ranging from 5.7 hours to almost 11 hours.9,12 Furthermore, Kwok et al 24 found that prolonged time in the operating room and head and neck cases were each an independent risk factor for flap failure.
Due to the extensive nature of FTT, it is important for clinicians to stratify patients’ risk based on their existing comorbidities to adequately advise on their operative risk and set expectations for their postoperative recovery course. Not only do risk stratification tools allow clinicians to identify patients who may require escalated perioperative care, but they also afford “meaningful comparison of surgical outcomes” among providers.25,26 This objective high-risk designation may allow for prioritization of limited resources, such as requirement for intensive care. 26 Furthermore, the use of objective risk stratification tools provide protection for the surgeon during the informed consent process, as the surgeon is providing the facts, with the patient at the center of the decision-making process.
One such risk stratification tool is the ASA physical status score. 17 This classification system is widely used by hospitals, medical boards, and lawyers and as a component of billing.17,18,26 It is a qualitative unit of measure based on an anesthesiologist’s professional opinion and experience; thus, it is possible for a patient to be assigned different ASA classes by different anesthesiologists.17,27,28
Although ASA scores may be considered subjective, studies showed high interrater reliability among anesthesiologists using the ASA classification system.22,29 Ihejirika et al 29 found a mean interrater agreement of 92%, with a range of 83.3% to 100%. Sankar et al 22 found moderate interrater reliability, with 67% of patients assigned to the same ASA class and 98.6% of paired assessments within 1 class of each other. Sankar et al also demonstrated the validity of the ASA score as a measure of preoperative physical health status, with patients in the higher ASA classes tending to be older males with more comorbidities requiring longer lengths of stay and higher risk of myocardial injury. Our study found a majority population of ASA 3 patients, which is ultimately expected given the frequent comorbidities noted in the population with head and neck cancer. A total of 33 (62.3%) patients in ASA 1-2 cohort had head and neck cancer, and this was the diagnosis for 207 (83.5%) patients of the ASA 3-4 group. ASA class 4 was limited, as patients in this population are often poor candidates for the prolonged surgery and anesthetic times required for free flap procedures.
We did note a statistically significant difference in comparing mean age between the low- and high-risk groups. Although age is not specifically taken into account as a variable by the ASA Physical Status Classification System, previous studies suggested a direct correlation between age and ASA classification. Sankar et al noted similar age distributions within a cohort of 10,864 patients and described that mean age progressively increased with higher ASA class groups. 22 Our findings mimic these results, and although age is a potentially confounding factor, we interpret the association between age and ASA class to follow a predictable pattern, as previously reported in the literature.
Length of Stay
Length of stay in the hospital is an important marker for postoperative patient health, with sicker patients often requiring longer lengths of stay. Moreover, patients who require longer hospital stays are not only accruing financial burden but are at higher risk for nosocomial infection. Several studies showed that patients in higher ASA classes tend to have longer hospital stays. Menke et al 21 found that patients in ASA class 4 had mean hospital stays almost 3 times as long as patients in ASA class 1 (27.3 vs 11.8 days), with respective mean ICU stays of 4 and 0.1 days. Wolters et al 30 reported similar findings, where patients in ASA classes 2 to 4 stayed 7 to 11 days longer than patients in ASA class 1, with mean ICU stays of 0.5 and 5.4 days in ASA classes 1 and 4, respectively. Piazza et al 8 also found that patients in the high-risk ASA group (classes 3 and 4) had significantly longer lengths of stay (23 days) than patients in the low-risk ASA group (19 days). In our study cohort, we found no significant difference between low- and high-risk ASA groups with regard to length of stay in the hospital and days in the ICU, but our data could be skewed by our small population of patients with ASA class 4: a population that may be more likely to have major complications and have longer hospitalizations. Furthermore, there was no significant difference with regard to 30-day readmission rates.
Perioperative Clinical Pathway
The short length of stay for both groups and, potentially, the equivocal outcomes can at least partially be attributed to a predefined clinical pathway. For all patients undergoing FTT, our institution utilizes a meticulous pathway that has a multidisciplinary approach to patient care. Some aspects of this pathway include progressive floor care, avoidance of ICU admission when possible, nurses specially trained in flap care, early feeding, strict flap-monitoring criteria, limiting vasoactive medications, early consultation of physical/speech/occupational therapy, limiting fluid overload, early mobilization, and universal utilization of case management assistance for disposition. The ultimate goal of the pathway is to discharge all patients on postoperative day 5 in good condition, to home if feasible. This pathway is standardized and allows for similar treatment of all patients, regardless of ASA status or comorbidities.
Complications
Although our study found no statistically significant association between ASA groups in rate of patients having ≥1 medical or surgical complications ( Table 5 ), we did find the high-risk ASA group to have more minor medical complications per person (P = .007) and more total medical complications per person (P = .012) than the low-risk ASA group ( Table 6 ). Previous studies also showed mixed findings with regard to ASA class and postoperative complications. Piazza et al 8 found that high-risk patients (ASA classes 3 and 4) had significantly more major surgical complications (20%) and minor medical complications (27.2%) than low-risk patients (ASA classes 1 and 2: 9.2% and 13.3%, respectively). For patients <75 years of age, Ferrari et al 11 found more total complications in ASA classes 3 and 4 (74.7%) than ASA classes 1 and 2 (50.4%). Özkan et al 9 found ASA class and advanced age were both significantly associated with medical complications, but interestingly, the authors found no significant association between ASA class and surgical complications. Rosenberg et al 7 found ASA class 3 and male sex to be significantly associated with postoperative medical complications. Suh et al 23 found a significant association between ASA class and both medical and reconstructive complications. The reconstructive complications cited included delayed healing of donor site, necrosis of native head and neck skin, partial or total flap necrosis, wound infection, salivary fistula, and hardware extrusion. 23 Furthermore, after multivariate analysis, the authors reported patient age and ASA status to be significant risk factors for developing postoperative medical complications. Broome et al 1 demonstrated ASA class to be an independent predictor for severe complications, with a rate of 11.8% in the low-risk group and 23.4% in high-risk group. Clark et al 13 reported a complication rate of 53% and found ASA classes 3 and 4, age ≥65 years, and current smoking status to be independent predictors of major complications.
However, Chang et al 5 found no correlation between ASA class and overall surgical complications. Furthermore, Shaari et al 6 studied several variables—age, ASA class, primary tumor site, bone versus soft tissue reconstruction—and found none to be significantly associated with postoperative complications; in fact, the only variable to approach statistical significance for developing complications was the high-risk ASA group (classes 3 and 4; P = .08). Although these findings are mixed, there appears to be a reasonable trend toward more complications, medical and surgical, among high-risk ASA class, thus alluding to the idea that high-risk patients should not undergo elective reconstructive surgery. However, instead of viewing the high-risk ASA class as a barrier to surgery, we propose using ASA class as a tool to assess a patient’s health prior to surgery, to provide adequate preoperative counseling and informed consent, and to allocate intensive care resources to high-risk patients following surgery as needed.
Morbidity and Mortality
Several studies found that patients in higher ASA classes tend to have increased morbidity and mortality following FTT. Menke et al 21 found postoperative morbidity rates of 3.9% and 33.7% for patients with ASA 1 and 4 designations, respectively, where 0% mortality rate was noted in ASA class 1 and 7.2% in ASA class 4. Wolters et al 30 found a 5- to 7-fold stepwise increase in hospital mortality per ASA class: 0.1%, 0.7%, 3.5%, and 18.3% (ASA classes 1-4, respectively). Özkan et al 9 reported 3 deaths within the 30-day postoperative period, and all were ASA class 3. On the contrary, Piazza et al 8 did not find a significant association between perioperative mortality and ASA score, and Kesting et al 10 reported no perioperative deaths within 30 days postoperatively.
Within our cohort, we found no significant difference between the high- and low-risk ASA groups on several measures of postoperative morbidity and mortality, as shown in Table 5 , although this could potentially misrepresent the high-risk category, due to the low number of ASA 4 patients in this cohort. Broome et al 1 found that “high-volume hospitals” and “high-volume surgeons” have substantially better rates of flap survival, which may account for our relatively equivocal findings between the ASA groups. Also, the level of inpatient postoperative care may vary among institutions. There are not only surgeon-specific limitations that can contribute to postoperative morbidity and mortality but also patient-specific limitations, such as lifestyle modifications, compliance, home wound care, and follow-up. 1
Flap Failure and Reoperation
Flap failure is a serious complication following FTT; fortunately, flap success rates >95% are widely reported within the literature for head and neck reconstruction.1,4-12 Our observed flap failure rate across all patients was 2.66%, and we found no statistically significant difference between low-risk (1.89%) and high-risk (2.82%) ASA groups. Our findings, as well as previous findings, demonstrated low rates of flap failure and no clear link to ASA classification. Furthermore, we found no significant difference in 30-day reoperation rate with regard to low- and high-risk ASA classes. Although no significance was demonstrated, we found higher rates of reoperation in the low-risk group (18.87%) than the high-risk group (13.31%).
Discharge Disposition
We found that 1.88% of low-risk patients (ASA classes 1 and 2) and 12.5% of high-risk patients (ASA classes 3 and 4) were discharged to a different location (P = .0244) following their hospital stay. “Different location” was defined as being placed in a skilled nursing facility, long-term acute care facility, or rehabilitation facility, when the patient was initially located within a private residence. Patient discharge disposition may be an important part of understanding why our high-risk ASA patients did not tend to have poorer outcomes as compared with their low-risk counterparts. Patients in the high-risk group may be more likely to receive higher levels of care during their postoperative course, potentially minimizing complications in this period.
Conclusion
In a single-institution, single-surgeon case series with chart review of patients undergoing FTT for head and neck defects, we conclude that a patient’s high ASA classification should not prevent one from receiving head and neck reconstructive surgery. Instead, we suggest using ASA class as a tool to predict which patients may require placement on discharge from the hospital, such as skilled nursing, long-term acute care, and rehabilitation facilities. This consideration was based on our finding that patients were much more likely to discharge to a facility if they had an ASA classification of 3 or 4. This information can be valuable during preoperative discussions with patients regarding expectations for postoperative care. Our findings suggest that higher levels of postoperative care for patients in ASA class 3 or 4 may level the playing field in regard to FTT success rates and rates of postoperative complications. We suggest that future studies further explore the use of ASA class as a tool for preoperative, goal-directed therapy for patient optimization.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the AAO-HNSF 2017 Annual Meeting & OTO Experience; September 10-13, 2017; Chicago, Illinois.