
Abstract
Objectives
To examine trend, prevalence, and outcomes of surgical site infection (SSI) in head and neck surgery.
Study Design
Retrospective cross-sectional analysis.
Setting
The Nationwide Readmissions Database (2010-2014), which represents 56.6% of all US hospitalization.
Subjects
Adult patients (≥18 years) who underwent head and neck surgery. Patients with SSI were compared with controls.
Methods
Analysis included chi-square test and multivariate logistic and linear regression models.
Results
A total of 427 cases and 116,921 controls were identified. SSI prevalence among patients who underwent head and neck surgery was 0.37%, of which 41.0% was reported within the initial admission while the remaining 59.0% was reported on readmission within 30 days of first surgery. SSI was associated with a higher mortality risk (odds ratio, 3.95; 95% CI, 1.25-12.50; P = .019). Multivariate analysis demonstrated that a higher risk of SSI was associated with major surgery of the ear, nose and paranasal sinuses, mouth and tonsil, salivary glands and ducts, maxillofacial bones and mandible, and pharynx and larynx (P < .05 each). However, a lower risk of SSI was reported in thyroid and parathyroid and nonmajor procedures (P < .05 each). Other factors associated with a higher risk of SSI included multiple comorbidities, smoking, cancer diagnosis, concomitant neck dissection, and tracheostomy (P < .05 each). SSI was associated with a mean ± SE additional hospital stay of 8.1 ± 0.8 days per case (P < .001) and an additional cost on the health system of $20,953.00 ± $186.3 per case (P < .001).
Conclusions
SSI is associated with a significant mortality risk and burden on the health system. More than half of SSI cases were identified on readmission.
Keywords
In 1992, the Centers for Disease Control and Prevention (CDC) introduced the term surgical site infection (SSI) in its updated report on nosocomial infections. 1 The report defined SSI as an infection occurring within 30 days of surgery or within a year following an implant procedure. The report further classified SSI based on its depth: superficial incisional, deep incisional, and organ/space.
Overall, SSIs are estimated to complicate 2% to 5% of surgical procedures, which constitutes >20% of nosocomial infections, making it one of the most common hospital-acquired infections.1-5 In major head and neck surgery, superficial SSI risk is estimated at 5.5%, deep incisional SSI risk at 3.4%, and organ space SSI risk at 2.0%. 6 The source of infection is mainly attributed to autocontamination of the surgical wound.7,8 SSI was reported to be associated with a significant increase in mortality, morbidity, and burden on the health system.1,2,7,9,10
The latest CDC progress report 5 on health care–associated infections found a 19% decrease in SSI in 10 select procedures between 2008 and 2013: abdominal aortic aneurysm repair, peripheral vascular bypass surgery, coronary artery graft, cardiac surgery, colon surgery, rectal surgery, hip arthroplasty, abdominal hysterectomy, knee arthroplasty, and vaginal hysterectomy. The report urged continuing monitoring and surveillance, as SSI still represents a significant public health burden. Unfortunately and as demonstrated, the CDC report did not include any otolaryngologic procedures. As a matter of fact from the range of otolaryngologic procedures, the CDC surveillance program monitors SSI following only selected neck and thyroid/parathyroid surgical procedures.11,12
The omnipresent risk of infection compounded by emergence of microbial resistance necessitates utilization of all available resources to gather data in a timely and detailed fashion. This is especially becoming important as the number of surgical procedures continues to rise in the United States. 4 The aim of this study is to provide a new and updated perspective on SSI following otolaryngologic, and head and neck surgery in the United States. In this analysis, we investigated clinical and demographic factors association with SSI, and we examined changes in trend and burden on the health system.
Methods
This study is a retrospective cross-sectional analysis based on utilizing the Nationwide Readmissions Database (NRD) for the years 2010 to 2014. The NRD is a part of the Healthcare Cost and Utilization Project, sponsored by the Agency for Healthcare Research and Quality. The NRD is a unique and powerful database designed to support various types of analyses of national readmission rates for all payers and the uninsured. The database includes discharge data from 27 geographically dispersed states, accounting for 57.8% of the total US resident population and 56.6% of all US hospitalizations. Additionally, the database allows for weighted analysis, as utilized in this project to provide a better estimation of national outcomes. The NRD tracks patients across the sampled hospitals within a calendar year for any readmission. This database addresses a large gap in health care data: the lack of nationally representative information on hospital readmissions for all ages. The NRD consists of publicly available de-identified data that do not meet the criteria of purview by the University of Iowa Institutional Review Board. 13
The objective of the study is to examine trend, risk, and outcomes of SSI among patients who underwent otolaryngologic and head and neck surgery. The inclusion parameters of the study population were adult patients (≥18 years) who underwent head and neck surgery as a primary admission procedure (Supplemental Table S1, available in the online version of the article). The extracted sample was then surveyed for cases of SSI (ICD-9 code 998.59 [International Classification of Diseases, Ninth Revision]) during either initial admission (ie, SSI developed following surgery before discharge) or unplanned readmission (ie, SSI within 30 days after the surgery). The database includes inpatients only; thus, it reflects cases of infection that developed postoperatively while patients were still in the hospital or after discharge, requiring readmission. Cases of infection that developed following discharge and did not require admission are not captured in the database. Controls are defined as patients who underwent similar procedures with no SSI reported during the initial admission and who did not have a readmission with SSI. All admissions were checked for completeness of data. Admissions with missing values for the study parameters were excluded.
The outcomes of interest included (1) SSI risk, (2) in-hospital mortality during initial admission or readmission within postoperative 30 days, (3) length of hospital stay in days (ie, the total length of hospital stay of the first admission and readmission, if it occurred), and (4) cost of health services. The database includes hospital charges associated with each admission, as well as a cost:charge ratio determined for each hospital, which allows conversion of charge values to cost values. All cost values were adjusted for inflation to reflect the 2017 US dollar per the inflation calculator of the Bureau of Labor Statistics.13,14
Independent factors that were assessed for their association with SSI included the following: age (18-40, >40 to <61, 61 to <75, ≥75 years), sex (male, female), modified Charlson Comorbidity Index score (0, 1, ≥2), 15 body mass index (<25, ≥25), history of tobacco use, diagnosis of a head and neck cancer, history of radiotherapy, history of chemotherapy, trauma as the indication for admission, and site and class of primary procedure (site classified per ICD-9 code [Supplemental Table S1, available in the online version of the article]; class of surgery per the database [nonmajor vs major]). For database classification of major and nonmajor procedures, surgery such as ethmoidectomy, tonsillectomy, or myringotomy is classified as a major procedure, while a procedure that involves superficial excision, suturing, or epistaxis control is classified as a nonmajor procedure (for details, see Supplemental Table S2, available in the online version of the article). 13
Other independent factors included neck dissection (performed, not performed), tracheostomy (performed, not performed), blood transfusion (reported, not reported), location and type of hospital (as coded in the database: metropolitan nonteaching, metropolitan teaching, nonmetropolitan), and hospital volume (defined as the number of head and neck surgical procedures performed in each hospital per year). 13 To avoid introduction of bias, quartile classification was applied to hospital volume: low volume (<25th percentile: 1-31 surgical procedures per year), intermediate volume (25th to <75th percentile: 32-143 surgical procedures per year), and high volume (≥75th percentile: ≥144 surgical procedures per year).
Statistical analysis used weighted data to reflect national estimates. The records’ weights are available in the NRD and calculated per the stratification variables used in the sampling methodology. 13 Statistical methods used in the study included cross-tabulation and chi-square test to examine the association between each independent factor and the outcome of interest. Factors that demonstrated significant association with the outcomes were considered possible confounders and included in multivariate logistic regression models. Multivariate logistic regression models were used to calculate odds ratios (ORs) and 95% CIs. A multivariate linear regression model was used to compare mean length of stay (LOS) and cost of health services while controlling for confounders. Liner regression was also used to examine trends in SSI and associated LOS and cost. The significance level was set as α = 0.05. All data analyses were performed with SAS 9.4 for Windows (SAS Institute Inc, Cary, North Carolina).
Results
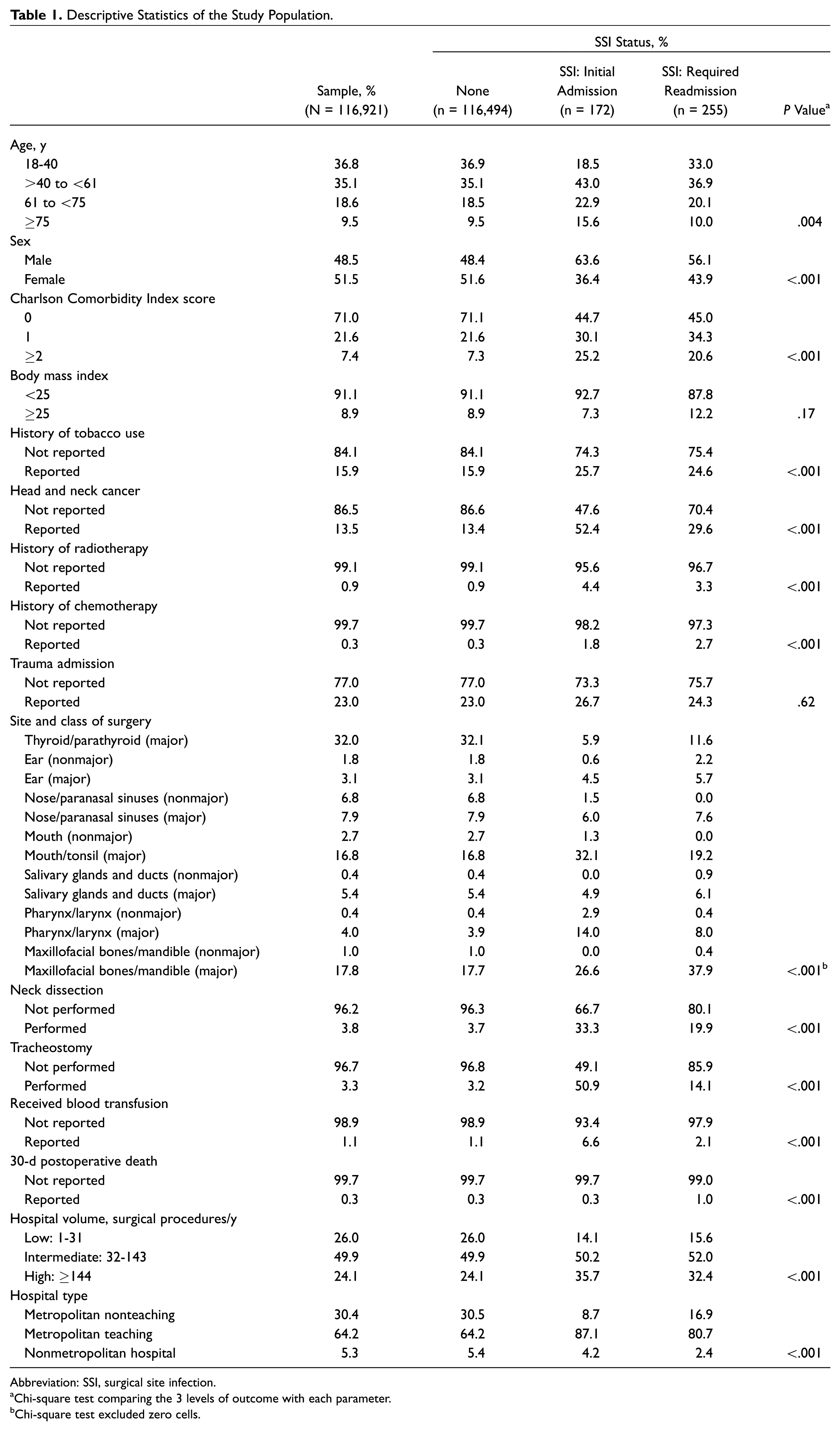
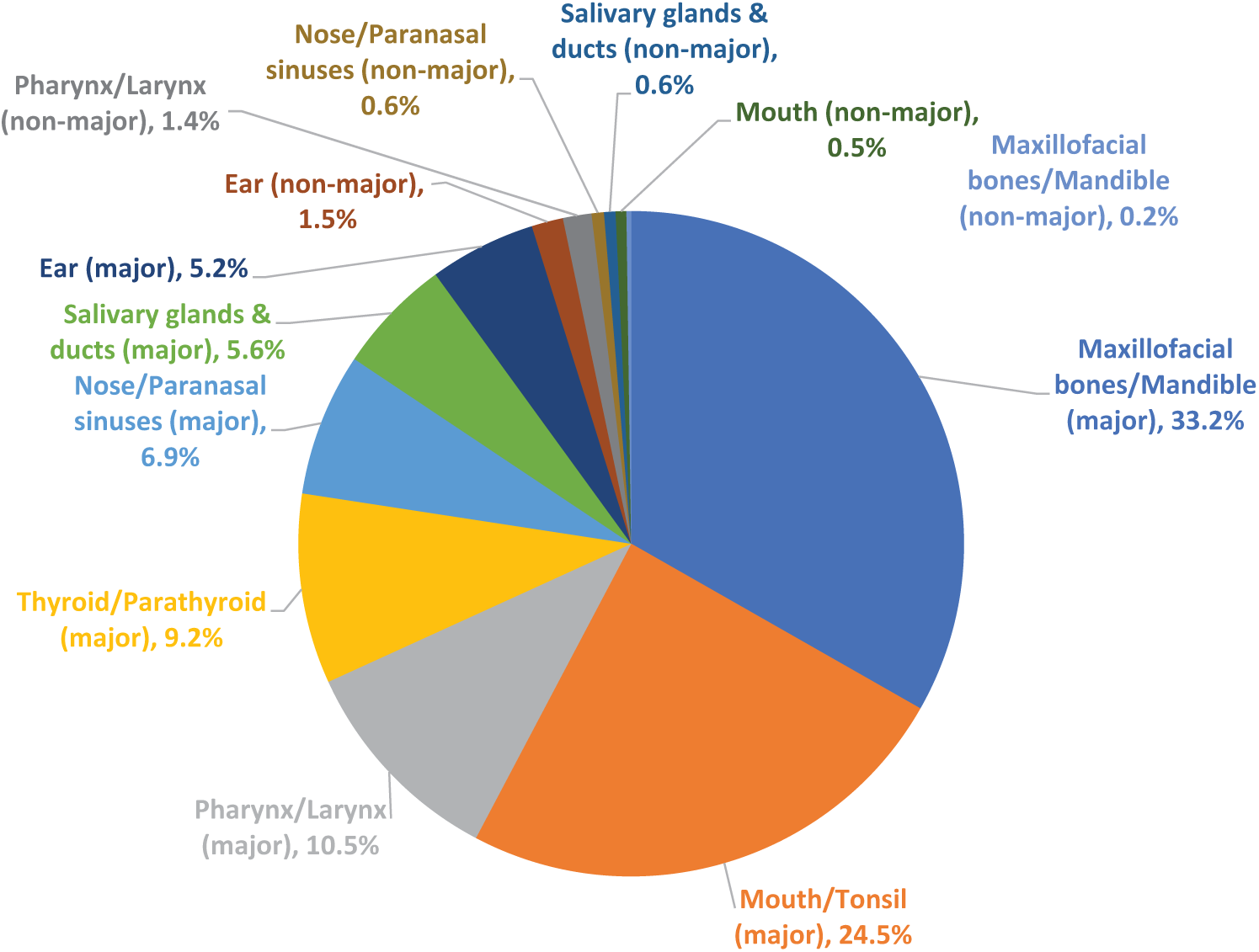
A total of 427 SSI cases and 116,921 controls were identified that underwent comparable procedures ( Table 1 ). Overall, SSI prevalence was 0.37% (95% CI, 0.32%-0.41%), of which 41.0% reported within the initial admission while the remaining 59.0% required readmission within 30 days. Figure 1 provides the mean readmission day from major otolaryngologic surgery. Admission due to trauma constituted 23.0% of all admissions, and 64.2% of patients were treated in a teaching hospital. Surgery of the thyroid, parathyroid, mouth, tonsil, maxillofacial, and mandible represented 66.6% of all head and neck procedures performed during the study period. Overall mortality risk was 0.3%.
Descriptive Statistics of the Study Population.
Abbreviation: SSI, surgical site infection.
Chi-square test comparing the 3 levels of outcome with each parameter.
Chi-square test excluded zero cells.
Mean (95% CI) readmission day counted from the day of the major otolaryngologic procedure and classified by site.
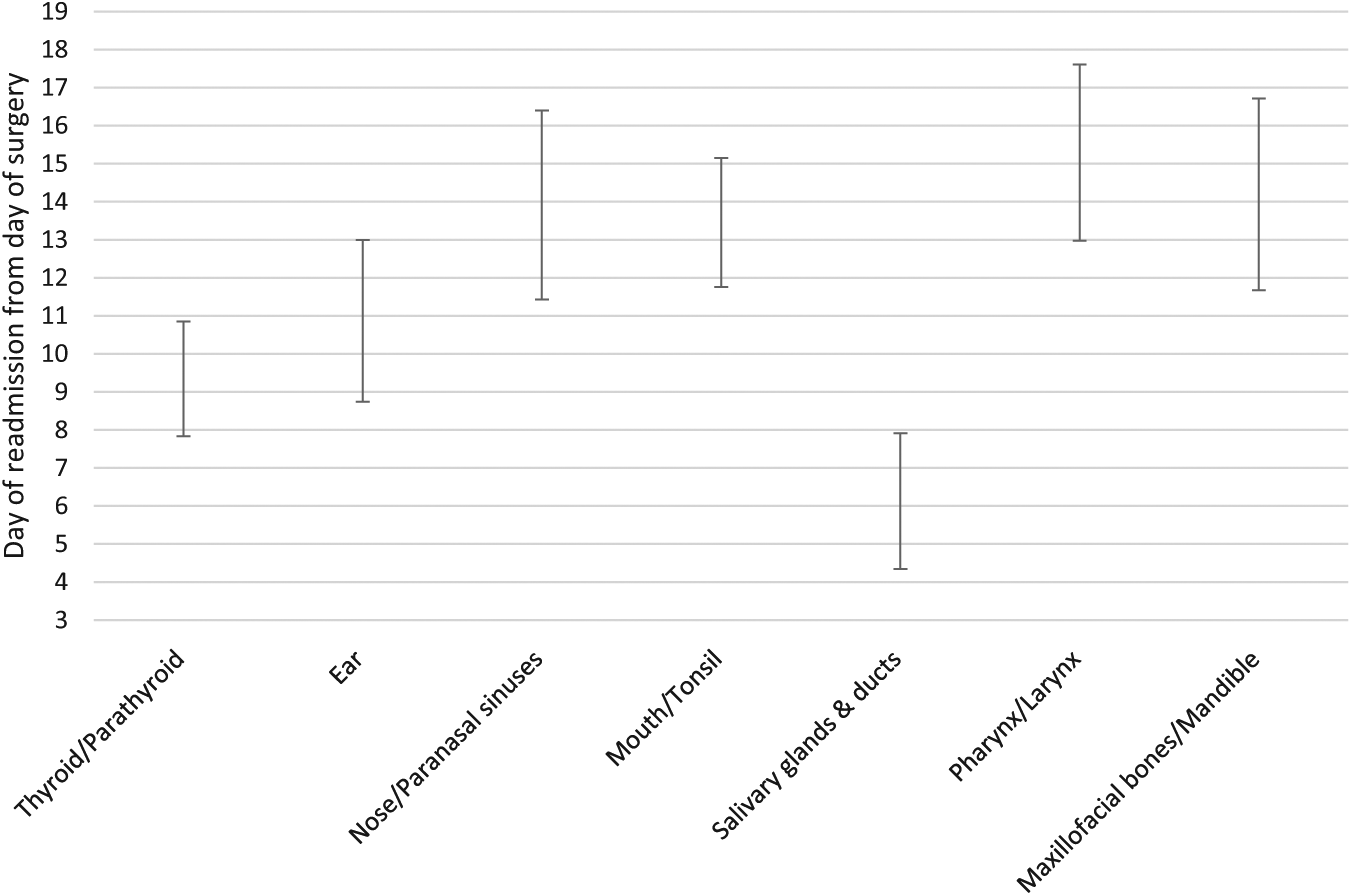
Patients who developed SSIs were more likely to have at least 1 comorbidity (P < .001; Table 2 ). Tobacco use was associated with an increased risk of infection (OR, 1.41; 95% CI, 1.05-1.90; P = .024). Patients with head and neck cancer were at a higher risk of developing SSIs (OR, 1.81; 95% CI, 1.26-2.61; P = .001). Performance of neck dissection (OR, 1.68; 95% CI, 1.12-2.51; P = .011) and/or tracheostomy (OR, 3.67; 95% CI, 2.55-5.28; P < .001) was independently associated with SSI. Patients treated in a teaching hospital were associated with an increased risk of infection (OR, 1.66; 95% CI, 1.18-2.34; P = .004).
Overall Risk of Postoperative SSI among Patients Who Underwent Head and Neck Surgery Whether the Infection Was Identified before Discharge or Required Readmission.
Abbreviations: aOR, adjusted odds ratio; CCIS, Charlson Comorbidity Index score; SSI, surgical site infection.
The model includes age, sex, Charlson Comorbidity Index score, tobacco use, history of radiotherapy, history of chemotherapy, head and neck cancer, trauma, surgery site and class, neck dissection, tracheostomy, blood transfusion, hospital volume, and hospital type.
Comparing the risk of SSI in relation to surgery site and class demonstrated 2 levels of risk: low versus high ( Table 2 , Figure 2 ; Supplemental Figure S1, available in the online version of the article). Procedures at high risk for SSI included ear (major), nose and paranasal sinuses (major), mouth and tonsil (major), salivary glands and ducts (major and nonmajor), pharynx and larynx (major), and maxillofacial bones and mandible (major). Procedures at low risk for SSI included thyroid and parathyroid, ear (nonmajor), nose and paranasal sinuses (nonmajor), mouth and tonsil (nonmajor), pharynx and larynx (nonmajor), and maxillofacial bones and mandible (nonmajor).
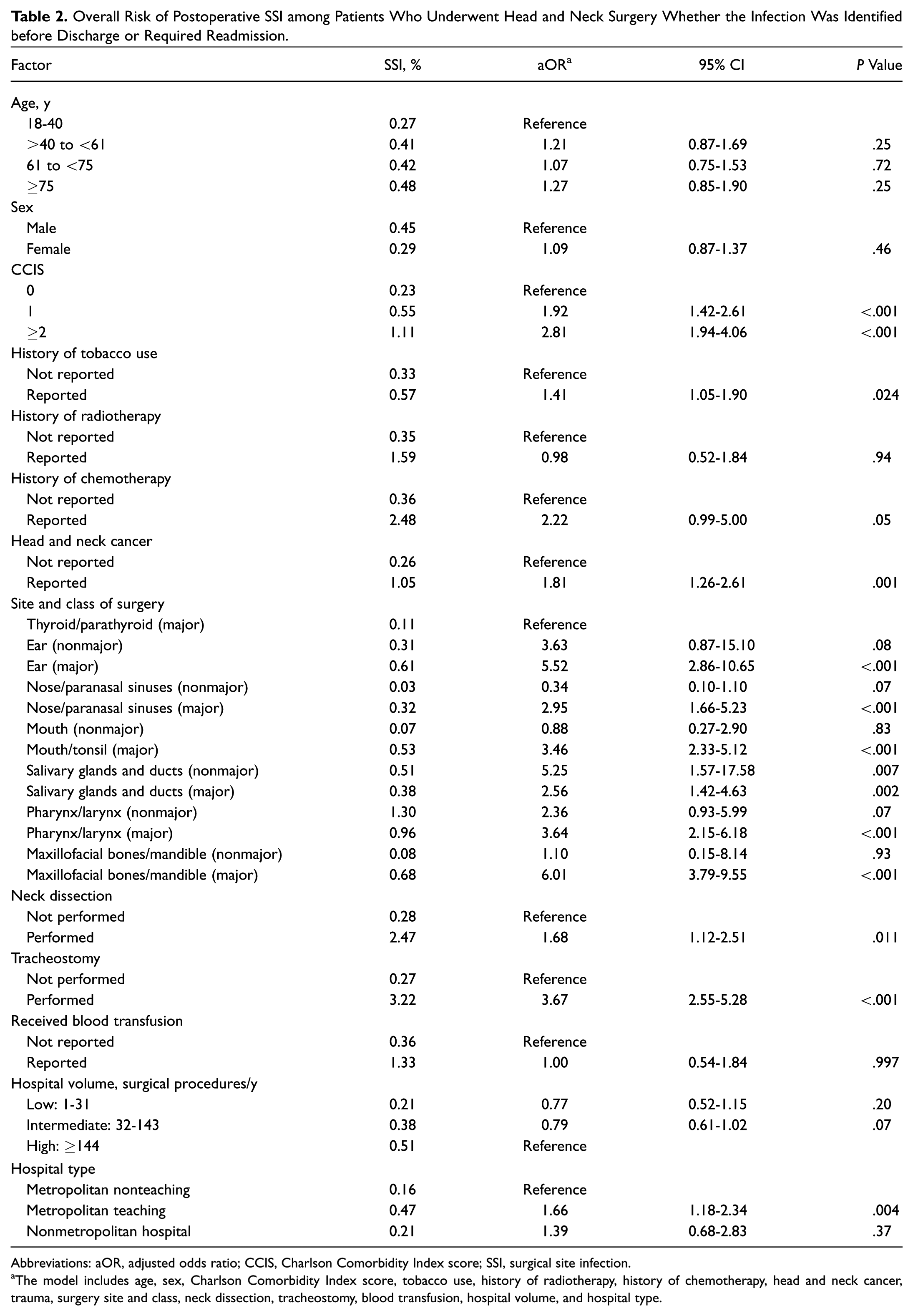
Distribution of postoperative surgical site infection by site and class of surgery.
Patients who were readmitted with SSI within 30 days after surgery were more likely to have multiple comorbidities, a history of chemotherapy, head and neck cancer, and neck dissection, as well as major surgery of the ear, nose/paranasal sinuses, mouth/tonsil, salivary glands and ducts (also nonmajor surgery), pharynx/larynx, or maxillofacial/mandible (P < .05 each; Table 3 ).
Multivariate Model of Factors That Have Significant Association with Readmission within 30 Days with Surgical Site Infection in the Univariate Models for Patients Who Had Head and Neck Surgery.
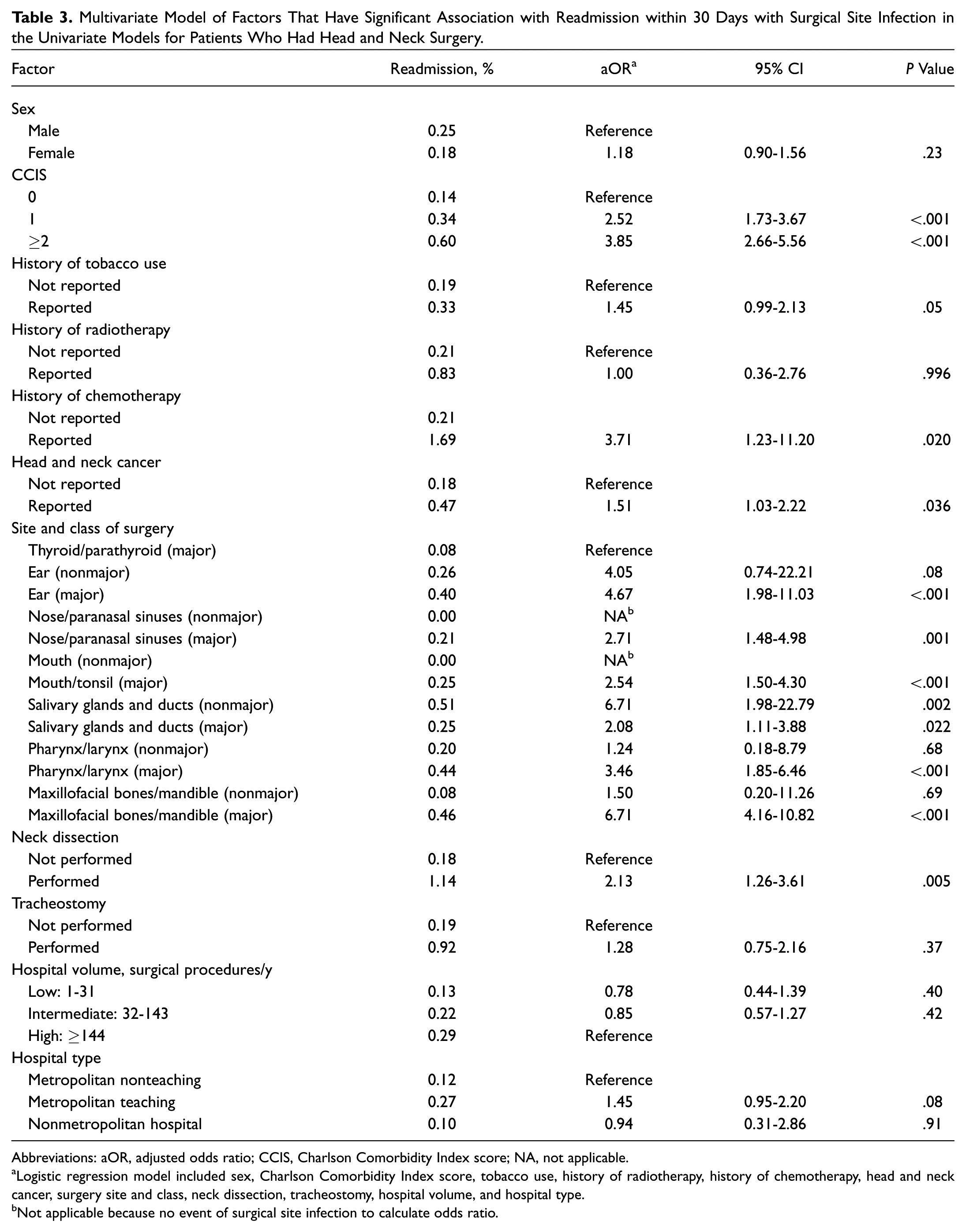
Abbreviations: aOR, adjusted odds ratio; CCIS, Charlson Comorbidity Index score; NA, not applicable.
Logistic regression model included sex, Charlson Comorbidity Index score, tobacco use, history of radiotherapy, history of chemotherapy, head and neck cancer, surgery site and class, neck dissection, tracheostomy, hospital volume, and hospital type.
Not applicable because no event of surgical site infection to calculate odds ratio.
SSIs were associated with a significant increase in mortality (2.8% vs 0.3%, P < .001; Table 4 ). Infections were also associated with a prolonged hospital stay by 8.1 ± 0.8 days (mean ± SE) per case and a higher cost of health services by $20,953.00 ± $186.31 (P < .001 each). Plotting the annual infection rate per every 10,000 head and neck procedures performed in the United States demonstrated an upward trend in SSI from 32.1 per 10,000 procedures in 2010 to 47.5 per 10,000 procedures at the end of the study period in 2014. If the risk continues to increase, the linear regression model projects that the risk could rise to 64.4 per 10,000 procedure in 2019 ( Figure 3 ). This upward trend in infection was accompanied by an increase in total additional LOS and cost, which were estimated to be 353.2 days and $ 0.65 million in 2010 for every 10,000 head and neck procedures performed in the United States. Additional LOS and cost were projected to increase to 523.5 days and $1.35 million in 2019.
Risk of Selected Outcomes for Cases That Developed Postoperative SSI vs Controls Undergoing Similar Procedures.
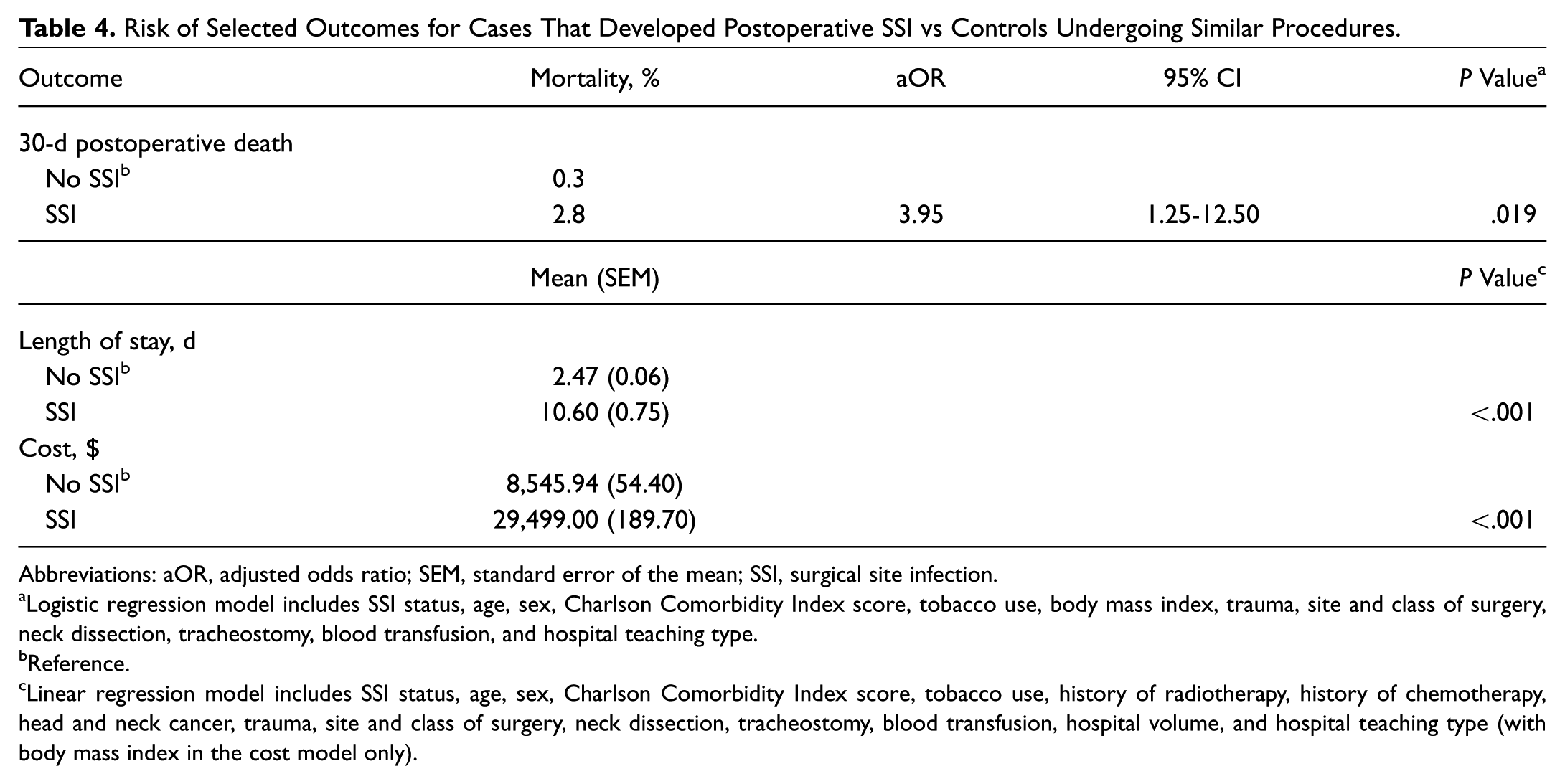
Abbreviations: aOR, adjusted odds ratio; SEM, standard error of the mean; SSI, surgical site infection.
Logistic regression model includes SSI status, age, sex, Charlson Comorbidity Index score, tobacco use, body mass index, trauma, site and class of surgery, neck dissection, tracheostomy, blood transfusion, and hospital teaching type.
Reference.
Linear regression model includes SSI status, age, sex, Charlson Comorbidity Index score, tobacco use, history of radiotherapy, history of chemotherapy, head and neck cancer, trauma, site and class of surgery, neck dissection, tracheostomy, blood transfusion, hospital volume, and hospital teaching type (with body mass index in the cost model only).
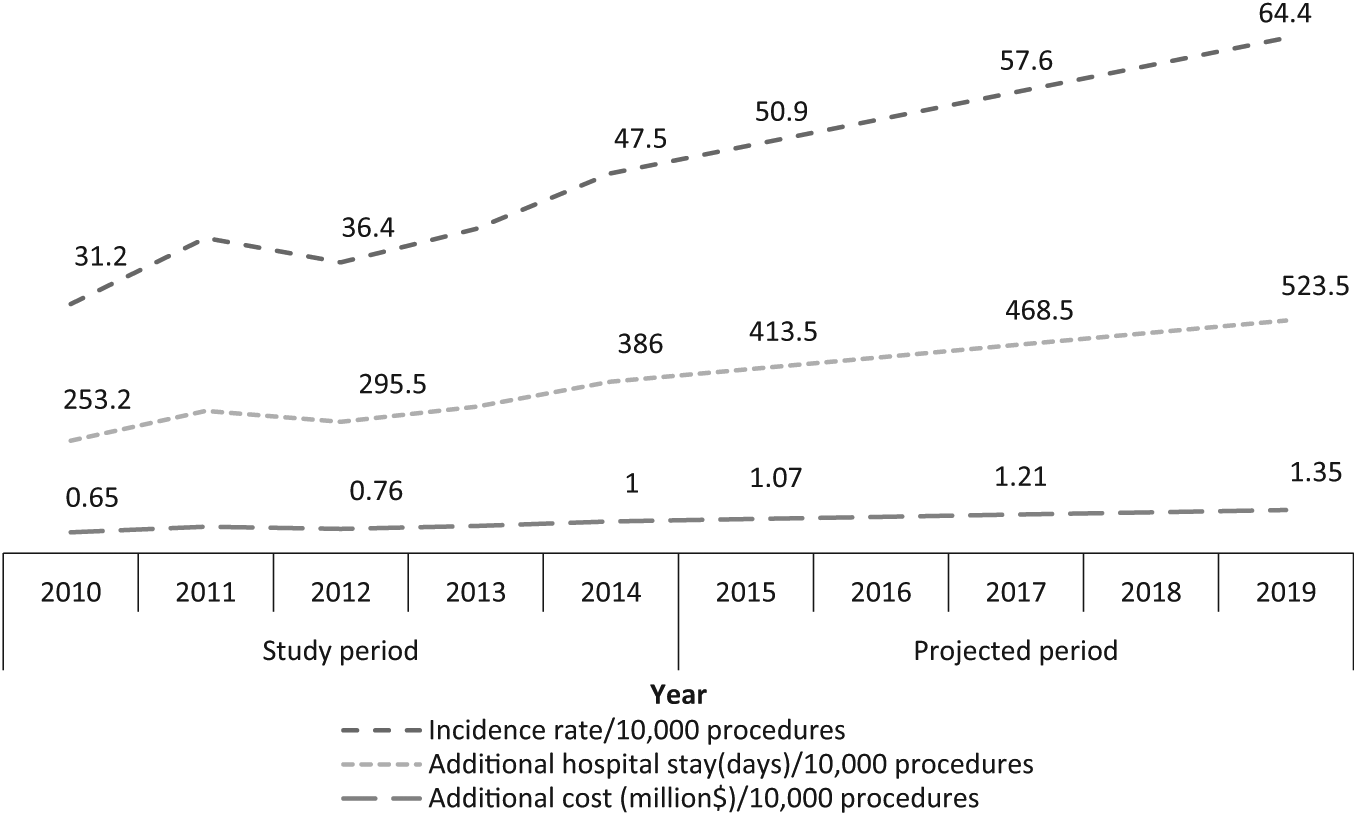
Incidence rate of surgical site infection and the associated excess length of stay and cost per 10,000 procedures.
Discussion
This study examined the prevalence and trend of SSI and related risk factors in otolaryngology in the United States. The overall prevalence of SSI was 0.37% (95% CI, 0.32%-0.41%). The trend of SSI rate was found to be increasing and projected to double from 31.2 per 10,000 procedures in 2010 to 64.4 per 10,000 procedures in 2019.
There is no national surveillance system that provides estimates of all types of health care–associated infections. 3 The CDC in 1970 sponsored the National Nosocomial Infections Surveillance System, which was then integrated into the National Healthcare Safety Network in 2005. The program obtains national data on nosocomial infections and SSI for selected procedures.11,12,16 At the inception of the program, an array of otolaryngologic procedures was included; however, this was subsequently narrowed to selected neck procedures and thyroid surgery.11,12 In the last report, for the years 2006 to 2008, the risk of SSI was 1.64% following low-risk neck surgery and 11.4% for high-risk neck surgery, while the risk following thyroid/parathyroid surgery was 0.26%. 12
Abt et al utilized the National Surgical Quality Improvement Program database to report the risk of SSI, as follows: superficial SSI, 5.5%; deep incisional, 3.4%; and organ space, 2.0%. However, their study population included only patients who underwent major head and neck oncologic surgery. 6 De Lissovoy et al surveyed the Nationwide Inpatient Sample of 2005 for SSI with the same ICD-9 code used in this study for patients who underwent neurologic, cardiovascular, colorectal, skin, breast, gastrointestinal, orthopedic, and obstetric and gynecologic procedures. 2 Among the 723,490 surgical hospitalizations included in their study, 6891 (1%) cases of SSI were identified. 2 Similar to our study, the de Lissovoy et al study reported that, on average, SSI extended LOS by 9.7 days and increased cost by $20,842 per admission. Both their study and ours included only inpatient cases of infection, explaining their comparable prevalence, which is still lower than that reported by clinical studies (discussed next).8,9,17-25 Nonetheless, the present study as compared with the de Lissovoy et al study included cases of infection that developed following discharge and required admission. The high proportion of SSI identified following discharge was also reported by Lotfi et al. 8 In their prospective study, which included 258 patients with advanced head and neck cancer, the authors found that 60% of SSI was diagnosed following discharge.
Studies that utilized single-institution clinical data demonstrated considerably variability (10%-45%)8,9,17-25—alas, a higher incidence of SSI than that found in studies based on national databases. One main reason for this variation between national and institutional databases is methodological, particularly the definition of the population at risk (ie, the denominator). In addition to the smaller sample of institutional data, which leaves more room for random error, studies that used institutional databases usually followed a more specific and narrow definition of population at risk by applying multiple clinical and surgical qualifiers. In studies based on national data, the population at risk is more broadly defined, either intentionally or as a limitation of the coding system. 5 Factors that would explain the variation in SSI incidence among institutional data include sample size, inclusion criteria, study design, year of study, and country of origin. Another confounding factor is the definition of SSI, which has been clinically inconsistent. In a survey by Lepelletier et al, in which health care professionals were presented with case vignettes for possible SSI, there was an observed disagreement in diagnosis of SSI within and between specialties. 26 Prospective studies might identify more infections, and in the case of clean-contaminated procedures, determining when an infection is clinically significant is not straightforward categorical.8,9,17-25
Risk factors of SSI identified in this study included the following: ≥1 comorbidities, tobacco use, cancer diagnosis, site and class of surgery, neck dissection, tracheostomy, blood transfusion, and treatment in teaching hospitals. In clinical practice, patients are more likely to present with >1 of the risk factors identified in this study. The higher risk in teaching hospitals is likely attributed to the fact that those hospitals likely manage more complex and severe cases. The NRD lacks specific clinical details, which could result in a residual confounding effect manifested as a higher risk of SSI in teaching hospitals. Multiple studies investigated risk factors of SSI by examining variable sets of factors for their potential association with infection; however, some those factors lacked reproducibility. Risk factors previously reported in literature include the following: the presence of comorbidities,25,27 tobacco use, 8 prior radiotherapy,9,20 prior chemotherapy, 23 type of surgery,23,25 clean-contaminated procedures,9,20 not using prophylactic antibiotic for clean-contaminated procedures,28,29 longer surgery,22,27,30 flap reconstruction, 8 neck dissection,31,32 tracheotomy,9,18,31 high American Society of Anesthesiologists score, 22 blood loss,23,27 presence of lymph node metastasis,8,25 management of a recurrent disease,18,21 oral cavity cancer as opposed to other head and neck cancers, 9 the inflammatory state of the ear at the time of surgery, 33 preoperative high liver function tests, 6 preoperative low sodium levels, 6 and early postoperative hypoalbuminemia. 34
The study also examined risk factors of readmission with SSI and identified the following independent predictors: ≥1 comorbidities, history of chemotherapy, cancer diagnosis, site and class of surgery, and neck dissection. Risk factors of readmission with SSI are particularly important for consideration by preventive programs aiming to reduce the burden of postoperative infection and the risk of readmission, because the majority of infection develops after discharge.
An estimated 55% of SSIs may be preventable with appropriate implementation of evidence-based strategies. 35 The 2017 CDC guideline for the prevention of SSI provides recommendations based on systematically evaluated evidence.4,10 The guidelines state strong recommendations for the following practices (category IA: a strong recommendation supported by high- to moderate-quality evidence suggesting net clinical benefits or harms): (1) implementation of perioperative glycemic control with blood glucose target levels <200 mg/dL, for patients with and without diabetes; (2) maintenance of perioperative normothermia; (3) administration of increased fraction of inspired oxygen intraoperatively and in the immediate postoperative period following extubation, for all patients with normal pulmonary function undergoing general anesthesia with endotracheal intubation; and (4) intraoperative skin preparation performed with an antiseptic agent containing alcohol, unless contraindicated. 10 The guidelines provide less supported recommendations for the following practices (category IB: a strong recommendation supported by low-quality evidence suggesting net clinical benefits or harms or an accepted practice supported by low- to very low-quality evidence): (1) instruction of patients to perform full body shower or bath the night before surgery, with either soap or an antiseptic agent; (2) administration of antimicrobial agents only when indicated, as based on published guidelines; and (3) timing of administration of antimicrobial agents such that bactericidal concentration is established in serum and tissues at initial incision.
The evidence regarding the type, dosage, and duration of prophylactic antibiotic in otolaryngology is still accumulating. In a thorough systematic review published in 2018, Patel et al reported a lack of evidence for routine antibiotic prophylaxis for most otolaryngologic procedures, such as tonsillectomy, simple septorhinoplasty, endoscopic sinus surgery, clean otologic surgery (tympanostomy with tube placement, tympanoplasty, stapedectomy, and mastoidectomy), and clean head and neck surgery (eg, thyroidectomy, parathyroidectomy, and salivary gland excisions). 29 Conversely, evidence supported the utilization of prophylactic antibiotic in complex septorhinoplasty, skull base surgery (anterior and lateral), clean-contaminated otologic surgery (cholesteatoma, purulent otorrhea), and clean-contaminated head and neck surgery (violation of aerodigestive tract, free flaps). Patel et al also observed that antibiotic use for 24 to 48 hours postoperatively showed equal benefit to a longer duration of prophylaxis.
The study has multiple limitations. NRD is an administrative database that lacks detailed clinical information, such as the specifics of surgery, type of infection, pathogen, and utilization of antibiotics. The database includes only inpatients and infections that required readmission; that is, it misses infections that develop after discharge and are treated in an outpatient setting. This likely explains the low prevalence identified in this study. The representation of only inpatient infection is likely to reflect early and severe infection that required readmission. Findings from this study should not be applied to infections that develop after discharge and would not require readmission, which likely to represent nonsevere infections. Additionally, the definition of the study outcomes is based on ICD-9 codes that lack specificity. The study is cross-sectional in design, which hinders establishing causality. Strength of the study is represented by the large sample size; the use of weighted analysis, which provides more accurate national estimates; and the availability of an array of factors that were controlled for their confounding effect.
Conclusions
SSI represents a major public health problem and a considerable cause of mortality and morbidity among patients undergoing otolaryngologic and head and neck surgery. The majority of SSI cases are declared after discharge. Studies are warranted to investigate whether it is safer and less burdening on the health system to consider more aggressive prophylaxis or to keep those who are at higher risk of readmission in the hospital longer following their initial surgery.
Author Contributions
Disclosures
Supplemental Material
OTO832858_suppl_mat – Supplemental material for Surgical Site Infection in Head and Neck Surgery: A National Perspective
Supplemental material, OTO832858_suppl_mat for Surgical Site Infection in Head and Neck Surgery: A National Perspective by Zaid Al-Qurayshi, Jarrett Walsh, Scott Owen and Emad Kandil in Otolaryngology–Head and Neck Surgery
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the AAO-HNSF 2018 Annual Meeting & OTO Experience; October 7-10, 2018; Atlanta, Georgia.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.