
Abstract
Objectives
Long-term effects of supracricoid laryngectomies are nowadays under discussion. The purpose of this study was to detect the prevalence of chronic aspiration and incidence of pulmonary complications, to investigate possible influencing factors, and to analyze dysphagia-related quality of life in a cohort of patients who recovered swallowing function after undergoing supracricoid laryngectomies.
Study Design
Retrospective observational study.
Setting
San Raffaele Hospital, Vita-Salute University, Milan, Italy.
Methods
A cohort of 39 patients who recovered swallowing function free of disease after a minimum 3-year follow-up period was retrospectively investigated between October and December 2017—clinically with the Pearson’s Scale and M. D. Anderson Dysphagia Inventory and instrumentally with fiberoptic endoscopic evaluation of swallowing.
Results
Chronic aspiration was demonstrated in a significant portion of patients (clinically in 33.3% and instrumentally in 35.9%). Aspiration was influenced by advanced age at surgery (P = .020). Type of surgical procedure, resection of 1 arytenoid cartilage, postoperative rehabilitation with a speech-language therapist, radiotherapy, age at consultation, and length of follow-up did not influence the prevalence of aspiration. Pulmonary complications affected 5 patients; incidence of pulmonary complications was related to aspiration and was favored by poor laryngeal sensation/cough reflex. Aspiration significantly affected quality of life.
Conclusions
Chronic aspiration is frequent and affects patients’ quality of life. However, incidence of pulmonary complications is low; therefore, oral feeding should not be contraindicated for aspirating patients. Preservation of laryngeal sensation and cough reflex is mandatory to prevent pulmonary complications.
Keywords
Supracricoid laryngectomies (SCLs) are nowadays well-accepted procedures for curative treatment of selected cases of primary or recurrent laryngeal cancer, with excellent oncologic and functional results.1-4 SCLs are classified as type II open partial horizontal laryngectomies (OPHLs) according to the nomenclature proposed in 2014 by the European Laryngological Society. 5 Type II OPHLs are further distinguished into type IIa, if the suprahyoid portion of the epiglottis is preserved and the reconstruction is provided by a cricohyoidoepiglottopexy (CHEP), 6 or type IIb, if the whole epiglottis is removed and the larynx is reconstructed with a cricohyoidopexy (CHP). 7 In OPHL type IIa and IIb, 1 arytenoid cartilage can be removed, as 1 functioning cricoarytenoid unit is sufficient to provide the effectiveness of the neolarynx.
After an appropriate rehabilitation period, respiration, deglutition. and phonation will be restored in most cases: the decannulation rate ranges between 85.7% and 100%, and a safe unrestricted oral diet is achieved by 53% to 100% of patients within the first postoperative year. 8 Focusing on swallowing function, rehabilitation is crucial, as most studies described a 100% rate of swallow dysfunction with aspiration in the first postoperative days. 9 Aspiration predisposes patients to development of pneumonia, a potentially lethal complication. Aspiration pneumonia is reported to affect 0% to 21.7% of patients. 8 However, most patients commonly achieve complete swallowing recovery within 3 months, and after completion of the rehabilitation period, the incidence of late complications is low. 9 Despite the low long-term complication rate, many authors described persistent postoperative aspiration,10-16 which seems to be tolerated by patients. Nevertheless, there are some concerns about potential sequelae of chronic aspiration after partial laryngectomy16,17: according to the literature, 1.3% of patients need a total laryngectomy because of persistent aspiration, 9 and a few cases of completion laryngectomy were reported >10 years after oncologically successful partial laryngeal surgery. 18
In the present retrospective study, we aimed to investigate the prevalence of chronic aspiration, the incidence of late pulmonary complications (LPCs), the presence of possible factors influencing swallowing outcome and LPCs, and dysphagia-related quality of life (QoL) on a cohort of patients who recovered swallowing function after SCL.
Methods
The present study was approved by the Ethics Committee of San Raffaele Hospital, Milan, Italy. Between January 2005 and September 2014, 75 patients underwent SCLs for squamous cell laryngeal carcinoma and were followed postoperatively in the Department of Otorhinolaryngology–Head and Neck Surgery of San Raffaele Hospital, Milan, Italy. Postoperative swallowing recovery was evaluated with a dedicated speech-language therapist (SLT), who assisted all of our patients with daily sessions of postural and swallowing exercises during their hospital stay. The feeding tube was removed, and the patient was discharged as soon as he or she was able to introduce daily caloric intake by mouth and no concomitant increase in inflammatory markers was observed. We always recommend domiciliary continuation of swallowing rehabilitation with an SLT until an unrestricted oral diet is reached. A minority of patients who showed greater difficulties in swallowing recovery or an increase in inflammatory markers or evidence of pneumonia were eventually discharged with the feeding tube. The possibility to remove the feeding tube was constantly reevaluated during follow-up consultations.
Inclusion criteria for this study were as follows: absence of locoregional recurrence of disease or distant metastasis, complete recovery of swallowing function without feeding tubes or tracheal cannula, and no restrictions in oral diet. Patients were investigated after a minimum 3-year follow-up period, during routine follow-up consultations. Thirty-nine patients still in follow-up were found to be eligible for this study; 2 patients were excluded because of permanent feeding tube dependency. The presence of a tracheal cannula or a feeding tube generally means that the swallowing function was not recovered; therefore, evaluation of such patients would not match the aim of the study.
Patients’ demographics are shown in Table 1 . We report sex, pT status, type of surgical procedure, age at surgery, age at follow-up consultation, duration of follow-up, rehabilitation with an SLT after hospital discharge, previous or adjuvant radiotherapy (RT), smoking status (number of cigarette pack-years), and presence of comorbidities (assessed per the Charlson Comorbidity Index 19 ).
Patients’ Demographics.
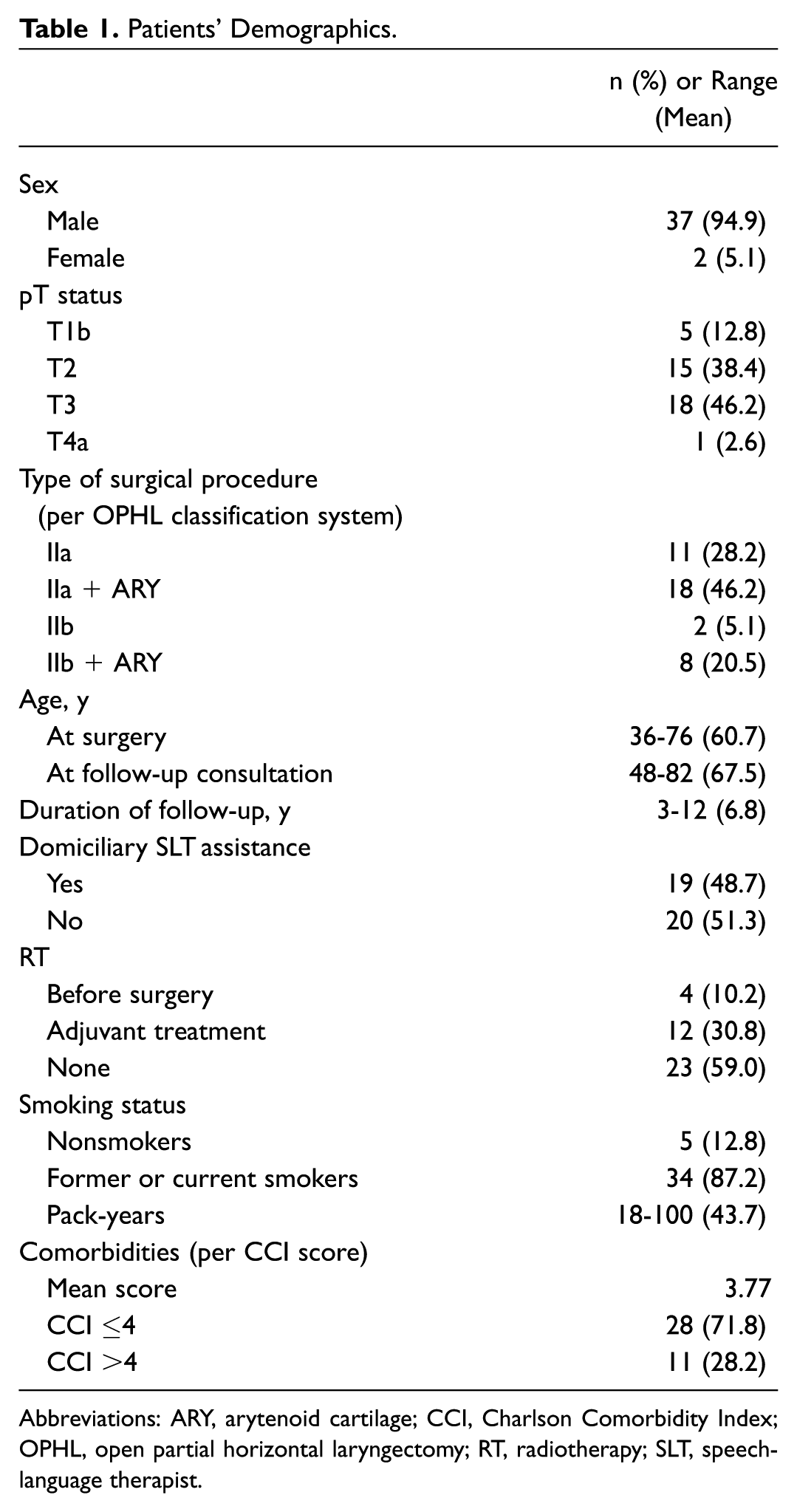
Abbreviations: ARY, arytenoid cartilage; CCI, Charlson Comorbidity Index; OPHL, open partial horizontal laryngectomy; RT, radiotherapy; SLT, speech-language therapist.
During follow-up consultation, an accurate medical history was collected to investigate frequent cough, episodes of pneumonia, or admissions to the emergency department for respiratory distress that occurred at least 6 months after treatment. A history evocative for postoperative aspiration was collected according to Pearson’s Scale (PS) 20 : 0, none; 1, occasional cough but no clinical problem; 2, constant cough worsening with meals or swallowing; 3, pulmonary complications. Swallowing assessment was performed with fiberoptic endoscopic evaluation of swallowing (FEES) with a rhinolaryngoscope (Olympus Evis Exera II CV-180; Olympus Corporation, Tokyo, Japan). During FEES, we searched for the following conditions: premature spillage, pharyngeal pooling, laryngeal penetration, poor pharyngolaryngeal sensation/absent or insufficient cough reflex, laryngeal aspiration. The first 4 parameters were globally referred to as “endoscopic risk factors for aspiration” (ERFs). Dysphagia-related QoL was assessed with the Italian version of the M. D. Anderson Dysphagia Inventory (MDADI).21,22
Statistical analysis was performed with SPSS 24 (IBM, Chicago, Illinois). The chi-square test was used to evaluate the impact of many variables of interest (ERFs, OPHL type, number of preserved arytenoids, rehabilitation with an SLT after discharge, RT, presence of comorbidities) on the prevalence of endoscopically assessed aspiration and on the incidence of LPCs; the same assessment was performed for continuous variables (age at surgery, age at follow-up consultation, length of follow-up, number of cigarette pack-years) with analysis of variance. Similarly, we used analysis of variance to investigate any possible correlation between dysphagia-related QoL (through the MDADI questionnaire) and PS, the presence of at least 1 ERF, aspiration detected at FEES, and LPCs. P < .05 was considered statistically significant.
Results
Clinical History
In our cohort of 39 patients, clinical assessment of aspiration with PS revealed no significant deglutition problems (PS = 0-1) for 26 patients (66.7%); 8 (20.5%) reported cough worsening with meals (PS = 2); and 5 (12.8%) reported LPCs (PS = 3). The latter 5 patients referred at least 1 episode of pneumonia. Cases of referred pneumonia without detailed medical documentation were considered aspiration pneumonias (2 cases). One patient reported 2 episodes of pneumonia, and another reported 3 admissions to the emergency department for acute dyspnea caused by foreign body retention in the airway. All the patients who reported pneumonia were still eating by mouth.
Fiberoptic Endoscopic Evaluation of Swallowing
The FEES study demonstrated the presence of premature spillage for 12 patients (30.8%), pharyngeal pooling for 28 (71.8%), laryngeal penetration for 19 (48.7%), and poor pharyngolaryngeal sensation/absent or insufficient cough reflex for 6 (15.4%). Globally, 28 patients (71.8%) reported at least 1 ERF, and 21 (53.8%) had >1. Interestingly, pharyngeal pooling was always present, being the most common finding in our cohort. Aspiration was detected among 14 patients (35.9%): all of them reported >1 ERF. All 6 patients affected by poor pharyngolaryngeal sensation/absent or insufficient cough reflex demonstrated aspiration at FEES.
Factors Influencing Prevalence of Chronic Aspiration at FEES
We investigated the possible correlation between evidence of chronic aspiration during FEES and type of surgical procedure (OPHL type IIa vs IIb), resection of 1 arytenoid cartilage (OPHL type II vs II + arytenoid cartilage), rehabilitation with an SLT after discharge, previous or adjuvant RT, age at surgery, age at follow-up consultation, and duration of follow-up. Results are presented in Table 2 .
Factors Influencing Prevalence of Chronic Aspiration at FEES.
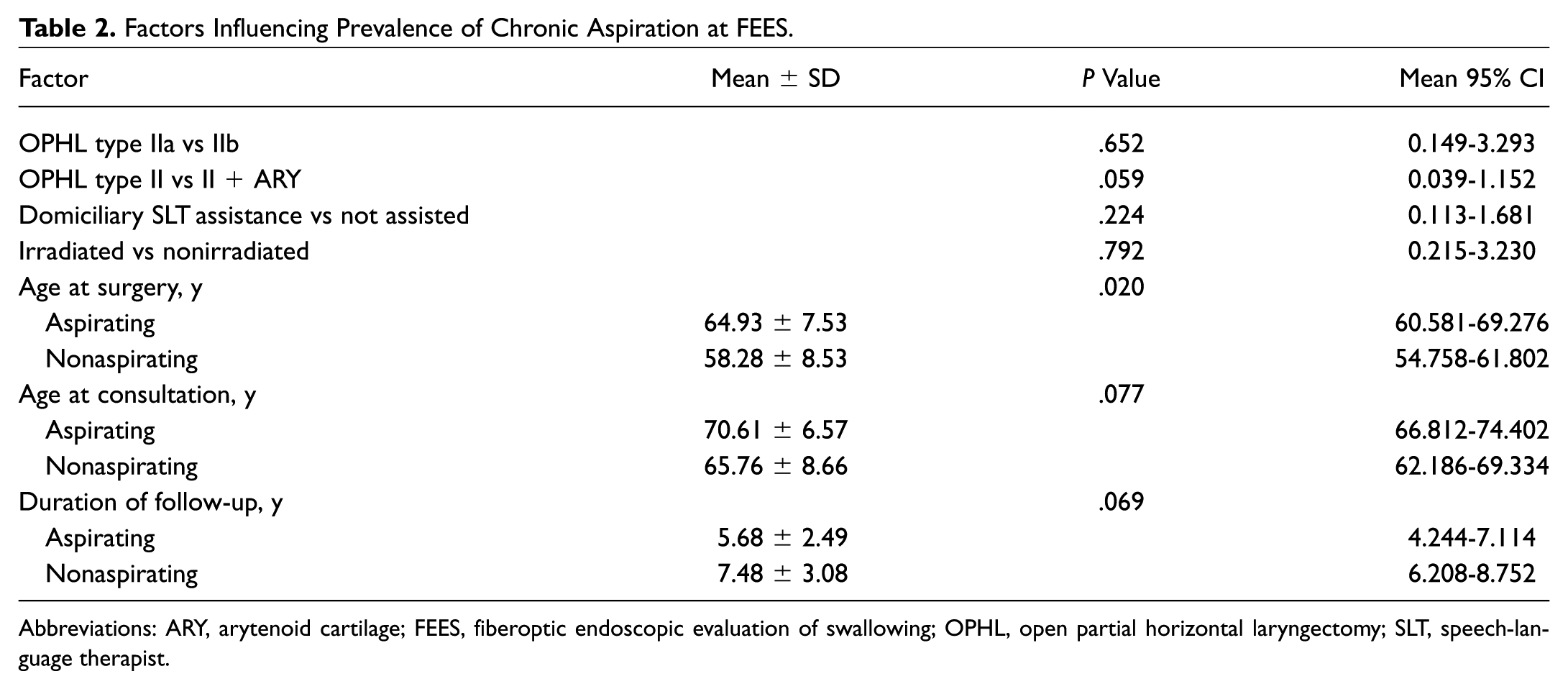
Abbreviations: ARY, arytenoid cartilage; FEES, fiberoptic endoscopic evaluation of swallowing; OPHL, open partial horizontal laryngectomy; SLT, speech-language therapist.
Younger age at surgery significantly protected patients from chronic aspiration: the mean age at surgery of nonaspirating patients was significantly lower than that of aspirating ones. Type of surgical procedure, rehabilitation with an SLT after discharge, RT, age at follow-up consultation, and length of follow-up were not related to instrumentally detected aspiration.
Resection of 1 arytenoid cartilage was not related to the prevalence of chronic aspiration. However, in a further analysis, we found a correlation between removal of 1 arytenoid and the presence of some ERFs: premature spillage (P = .003, 95% CI = .377-.769), pharyngeal pooling (P = .012, 95% CI = .034-.716), and laryngeal penetration (P = .023; 95% CI = .041-.851). There was no correlation with poor pharyngolaryngeal sensation/absent or insufficient cough reflex.
Factors Influencing Incidence of LPCs
Presence of ERFs and aspiration at FEES, age at surgery, age at follow-up consultation, smoking status, and patient comorbidities were investigated as possible factors influencing incidence of LPCs. Results are presented in Table 3 .
Factors Influencing Incidence of Late Pulmonary Complications.
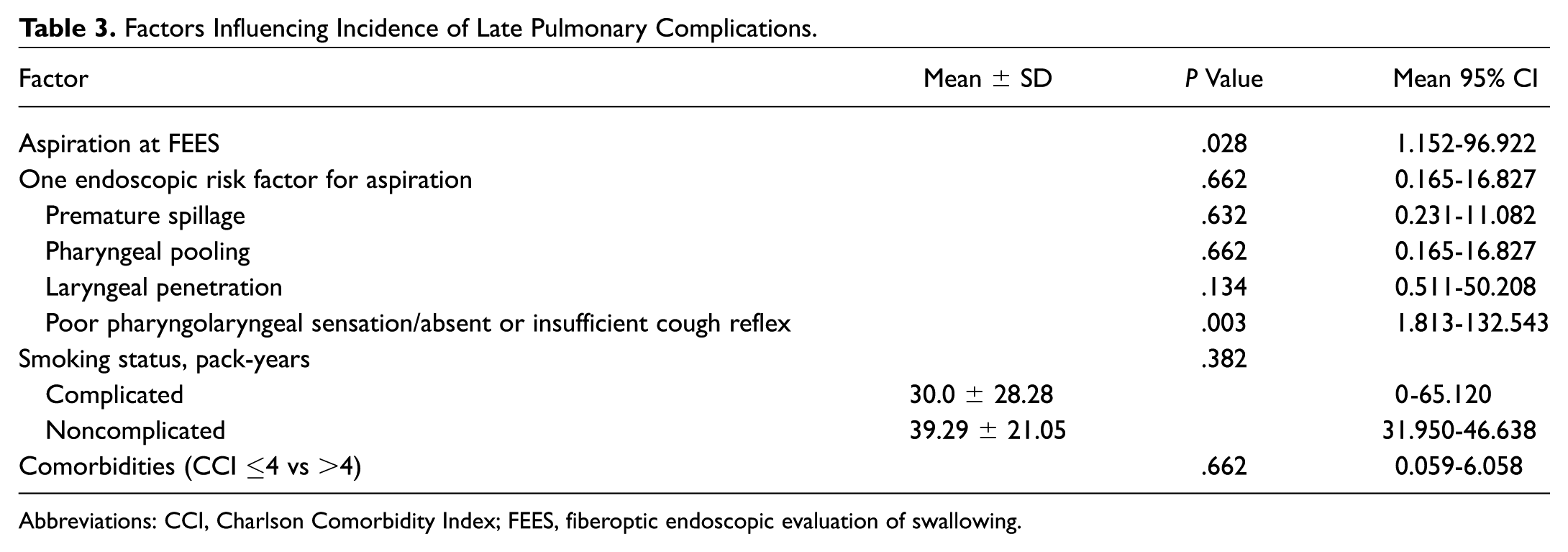
Abbreviations: CCI, Charlson Comorbidity Index; FEES, fiberoptic endoscopic evaluation of swallowing.
Not surprising, we reported a statistically significant correlation between chronic aspiration detected at FEES and incidence of LPCs. However, the presence of at least 1 or multiple ERFs was not significantly related to LPCs. Nevertheless, when ERFs were individually investigated, we found a strong correlation between poor pharyngolaryngeal sensation/absent or insufficient cough reflex and incidence of LPCs.
Age at surgery, age at follow-up consultation, number of cigarette pack-years, and patient comorbidities were not related to pulmonary events.
Dysphagia-Related QoL
The mean total MDADI score achieved by our study population was 81.5 (range, 41.25-100). The mean scores of MDADI subscales were as follows: global, 81.0 (range, 20-100); functional, 83.4 (range, 52-100); emotional, 81.6 (range, 53.3-100); physical, 79.9 (range, 42.2-100). Total MDADI score was related to PS, presence of at least 1 ERF, endoscopic evidence of aspiration, and LPCs; results are presented in Table 4 . Clinically and endoscopically detected aspiration and the presence of ERFs were associated with a lower total MDADI score. LPCs did not affect patients’ QoL.
Influence of Aspiration and Pulmonary Complications on Dysphagia-Related Quality of Life.
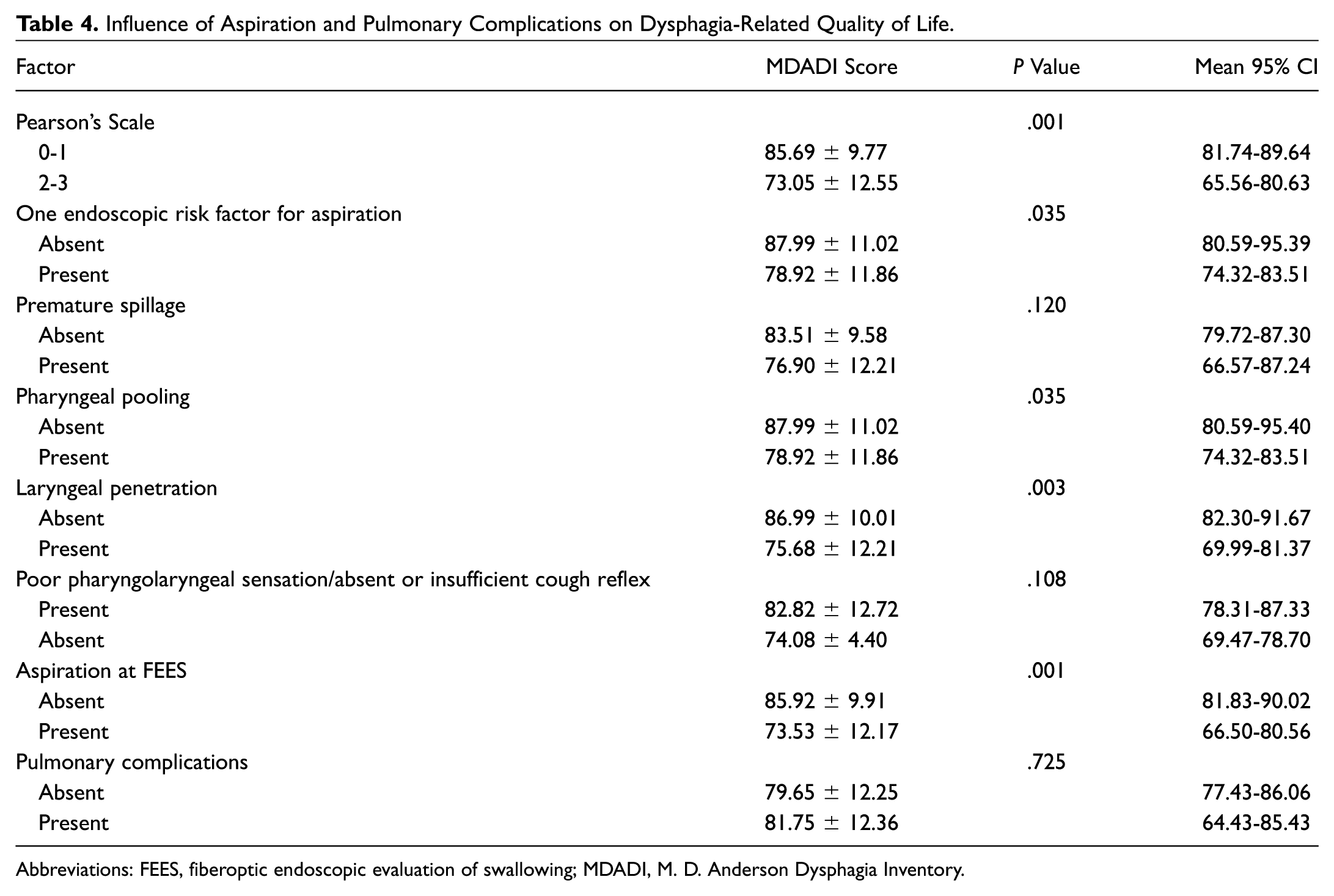
Abbreviations: FEES, fiberoptic endoscopic evaluation of swallowing; MDADI, M. D. Anderson Dysphagia Inventory.
Discussion
After an SCL, aspiration is constant in the early postoperative period. 8 Gradually, the prevalence decreases, but still a significant portion of patients (35.9% [14 of 39] in our study group, 14%-68% in the literature10-16) experiences persistent chronic aspiration, although their swallowing function recovered satisfactory.
We searched for possible factors predisposing patients to chronic aspiration. Literature on this topic is confounding, as many authors have tried to assess these factors, with conflicting results.8,10,15,16,23-25 We investigated chronic aspiration clinically and instrumentally. However, when searching for possible factors influencing prevalence of chronic aspiration, we relied on findings detected at FEES, as patients’ perceptions are not sufficient to discriminate safe swallowing in OPHL. 26
First, we looked at factors related to the surgical procedure. Laryngeal reconstruction with CHEP, sparing a portion of the epiglottis, may protect from aspiration. In a study of 457 patients, Benito et al 10 found a significant correlation between aspiration and CHP, which was not found with CHEP; a better functional outcome after CHEP, rather than after CHP, was also reported by Clayburgh et al. 25 However, in our cohort, the type of reconstruction did not affect the prevalence of chronic aspiration, in line with other authors.15,16,23 Also, preservation of both arytenoid cartilages may protect the airway. Again, some authors10,16 found a correlation between aspiration and removal of 1 arytenoid cartilage, while others did not.15,23-25 Topaloglu et al 24 found significantly higher bolus retention after removal of 1 arytenoid. Our patients with only 1 remaining arytenoid cartilage were more likely to present pharyngeal pooling, premature spillage, and laryngeal penetration but not chronic aspiration. The presence of both arytenoid cartilages may facilitate clearing of the neolarynx, therefore reducing pooling and penetration of bolus.
Second, we focused our attention on the patient. We always recommended rehabilitation with an SLT after hospital discharge, but not all patients were compliant with our recommendations. However, in our cohort, domiciliary SLT assistance was not related with reduced prevalence of aspiration, even though a possible confounding factor may come from the need for longer rehabilitation for patients with worse postoperative recovery. Further studies are needed to assess the possible role of a long period of postoperative rehabilitation with an SLT. Radiation therapy to the larynx may adversely affect swallowing function for patients who underwent SCLs. Some authors15,24,27 found worse deglutition outcomes after RT; we found no influence of RT on chronic aspiration, and other authors had similar results.10,23 We did not distinguish between patients who underwent salvage SCLs and those treated with adjuvant RT, assuming that long-term effects would depend on the sum of the 2 treatments. Further studies are needed, especially focusing on adjuvant RT, which is nowadays considered to compromise functional outcomes.
In our study group, the prevalence of chronic aspiration was significantly affected by the age at surgery, in contrast to other studies. 28 Poorer swallowing outcomes among elderly patients treated with SCLs were already reported.10,25,29 This finding may be related to poorer compliance and greater difficulties in achieving complete swallowing rehabilitation among the elderly. Unless age-related changes in swallowing mechanisms are well known, previous studies were not able to identify the effects of presbyphagia after SCLs.16,17 This is consistent with our results, as aspiration was not related to age at follow-up consultation and duration of follow-up in our series. Therefore, presbyphagia does not seem to affect long-term swallowing outcomes after SCLs. Actually, aspiration is probably more common than we think, even among healthy people. Butler et al 30 endoscopically assessed normal swallowing among healthy people and found that normal adults, especially older adults, might demonstrate trace aspiration from time to time.
Despite the rather common prevalence of chronic aspiration, incidence of LPCs after SCLs is low: in our cohort, it was at approximately 12%, but the literature reports even lower percentages. 8 This means that most patients whose chronic aspiration was clinically suspected or instrumentally demonstrated are able to tolerate aspiration without developing complications. This finding was already noticed by other authors.11,14 Furthermore, Simonelli et al 14 performed a chest CT scan of operated patients who were chronically aspirating, and they compared the results with a group of patients affected by chronic obstructive pulmonary disease (COPD), finding no significant radiologic difference. According to these findings, chronic aspiration itself should not be considered a limiting factor to normal oral alimentation after SCLs. In fact, a recent study on the natural history of patients who aspirate found no statistical association between dietary modification and development of pulmonary events. 31
An important issue would be to identify those few patients who develop LPCs. In a series of 111 SCLs, Joo et al 32 found that development of immediate postoperative pulmonary complications was associated with older age, chronic lung disease, smoking status, CHP, and removal of 1 arytenoid cartilage. Crosetti et al 17 reported that episodes of aspiration pneumonia were related to the severity of dysphagia and to more extended OPHL procedures and that incidence reduced over time. To the best of our knowledge, no study tried to assess specific factors influencing the incidence of LPCs after SCLs. In our series, evidence of chronic aspiration was related to the incidence of LPCs: this seems quite obvious, as pulmonary complications are determined by aspirated material in the airway.
A longitudinal study 33 investigating the incidence and risk factors for aspiration pneumonia among nonoperated elderly patients from different clinical settings found that dysphagia and aspiration were significantly related to pneumonia but were not significant predictors. This means that aspiration is a necessary but not sufficient condition for the development of pneumonia, and it may not be a critical risk factor for a medically stable patient. Comorbidities such as COPD, congestive heart failure, weak cough, and immunocompromised health status could impair host defenses, and the simultaneous presence of aspiration places the patient at greater risk of pneumonia. Pulmonary function is crucial for patients who are candidates for an SCL: almost all of them are current or former heavy smokers and therefore often affected by some degree of COPD; at the same time, severe COPD is a contraindication to this kind of surgery. In our series, smoking habit and patient comorbidities were not related to the incidence of LPCs, although patients who underwent SCLs were highly selected; that is, those affected by severe COPD, whose presurgical pulmonary function was most seriously compromised, were excluded.
In addition to chronic aspiration, we found a strong correlation between LPCs and poor pharyngolaryngeal sensation/absent or insufficient cough reflex. According to Simonelli et al, 14 a possible explanation for patients’ tolerance to chronic aspiration may be the efficient cough reflex and the mucociliary clearance mechanism that remove the aspirated material from the airway. Their absence would impair the clearing capacities of the airways, facilitating complications. Pharyngolaryngeal sensation and cough reflex are guaranteed by the integrity of the internal branch of the superior laryngeal nerve (ibSLN). 34 The importance of sparing this nerve during the surgical procedure was pointed out by Benito et al 10 and Yücetürk et al, 12 who found a correlation between a damaged superior laryngeal nerve and the presence of aspiration. Sparing the ibSLN is crucial, as its injury would impair pharyngolaryngeal sensation and the cough reflex; such impairment in our series was associated with not only chronic aspiration but also LPCs. During follow-up consultation, pharyngolaryngeal sensation and cough reflex should always be tested, and the evidence of chronic aspiration with reduced sensation and absent cough reflex should arouse concerns about the great likelihood of developing pulmonary events. In such cases, interruption of oral feeding may be considered.
Finally, using the MDADI questionnaire, we investigated dysphagia-related QoL after SCLs. Mean total MDADI score reported in the literature ranges between 78.4 and 92,24,28,35,36 demonstrating an overall good QoL. In a recent study, Pizzorni et al 26 investigated swallowing-related QoL after OPHLs and reported that it was significantly affected by the severity of aspiration, with mean higher scores in the functional MDADI subscale and lower scores in the physical subscale. We had similar results, with a mean total score of 81.5 and the same distribution of scores in the subscales, suggesting satisfactory long-term dysphagia-related QoL. We also confirmed that aspiration (assessed both clinically and endoscopically), pharyngeal pooling, and laryngeal penetration significantly affect QoL. This finding may be related to the worse swallowing performance of aspirating patients during their everyday social and private lives. Conversely, LPCs were not related to reduced QoL.
The small number of patients in our cohort is undoubtedly a limitation to this study, especially for the very low number of patients who reported LPCs. Confirmation of our results in a larger cohort could be useful to determine whether it is possible to identify a subset of patients at higher risk of pulmonary events among those who are chronically aspirating, to prevent them from oral feeding. Furthermore, future studies should evaluate pulmonary function among patients who are chronically aspirating after SCLs, to investigate the possible detrimental effects of chronic aspiration on pulmonary function tests.
Conclusions
After SCLs, chronic aspiration is rather common, whereas incidence of LPCs is low. We found a correlation between aspiration and age at surgery, but OPHL type, resection of 1 arytenoid cartilage, continuation of rehabilitation with an SLT after hospital discharge, RT, and increasing age did not seem to play a role. Chronic aspiration after SCL should not be considered a contraindication to oral feeding, but it seems to affect patients’ QoL. Investigation into the possible factors influencing the incidence of LPCs revealed a correlation with impaired pharyngolaryngeal sensation or weak cough reflex, underlining the importance of preservation of the ibSLN during the surgical procedure. Smoking habit and comorbidities showed no influence on incidence of LPCs, despite the highly selected cohort of patients.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the AAO-HNSF 2018 Annual Meeting & OTO Experience; October 7-10, 2018; Atlanta, Georgia.