
Abstract
Objective
To determine the incidence of postoperative venous thromboembolism (VTE) in adults undergoing otologic surgery.
Study Design
Cross-sectional retrospective study.
Setting
Single tertiary academic center.
Subjects and Methods
Adults undergoing nononcologic, extracranial otologic surgery from August 2009 to December 2016. Patients with postoperative diagnosis VTE codes were identified. Imaging and clinical documents were searched for VTE evidence within the first 30 postoperative days. Methods of thromboprophylaxis were documented, and Caprini risk scores were calculated.
Results
In total, 1213 otologic surgeries were evaluated. No postoperative VTE events were identified (0/1268). Mean age was 51.0 ± 17.3 years (range, 18.1-93.4 years). Average length of surgery was 136.0 ± 79.0 minutes (range, 5-768 minutes). The average Caprini score in all patients was 4.0 ± 1.7 (range, 1-15). Eighty-five percent of patients had a Caprini score ≥3, the threshold at which chemoprophylaxis has been recommended in general surgery patients by the American College of Chest Physicians 2012 guidelines. Six patients had documented preoperative chemoprophylaxis and a Caprini score of 4.8 ± 1.7. This was not significantly different from that of patients who did not receive preoperative chemoprophylaxis (t test, P = .3). The literature would estimate a rate of 3.7% VTE in adults with similar Caprini scores undergoing general surgery procedures with no VTE prophylaxis.
Conclusion
The Caprini risk assessment model may overestimate VTE risk in patients undergoing extracranial otologic surgery. Postoperative VTE following otologic surgery is rare, even in patients traditionally considered moderate or high risk. Chemoprophylaxis guidelines in this group should be balanced against the potential risk of increased intraoperative bleeding and its associated effects on surgical visualization and morbidity.
Venous thromboembolism (VTE) is a common postoperative complication with a prevalence as high as 40% in general surgery patients without thromboprophylaxis. 1 Its risk has been shown to increase by 21-fold after surgery. 2 The Caprini risk assessment model is a widely used tool to evaluate VTE risk in surgical patients 3 that has been validated for adult otolaryngology patients undergoing inpatient procedures, 4 as well as for general, orthopedic, plastic, and otolaryngology–head and neck surgery (OHNS) patients.5-7 However, VTE rates have been found to vary among OHNS subpopulations, 8 and it is unclear whether this assessment tool with its recommendations should uniformly apply to all OHNS patients.
The evidence-based American College of Chest Physician CHEST guidelines published in 2012 for VTE prevention did not include thromboprophylaxis recommendations for OHNS or its subspecialties. 6 Since then, several studies have examined VTE risk in OHNS subspecialties such as rhinology, 9 facial plastic surgery, 10 and head and neck oncology,11-14 with few studies specifically addressing otology patients.
The aim of this study is to examine the prevalence of postoperative VTE in otology patients to elucidate the role of chemoprophylaxis in these patients.
Methods
The Stanford institutional review board approved the study protocol. Patients undergoing nononcologic otologic surgery between 2008 and 2016 at a single academic institution were retrospectively evaluated. Patients were identified using the Stanford Translational Research Integrated Database Environment (STRIDE) tool, an informatics platform that streamlines patient identification based on specific clinical characteristics. 15
Adult patients >18 years of age having undergone extracranial otologic surgery at both inpatient and outpatient settings were included. Patients were excluded if their procedure extended intracranially, surgery was performed for an oncologic diagnosis, or postoperative documentation was not available. Patients were not routinely screened for VTE using ultrasound or chest computed tomography if asymptomatic but rather at the clinical discretion of their providers typically with an extremity ultrasound or computed tomography (CT) pulmonary angiogram.
Eligible patients were identified on STRIDE with International Classification of Diseases, Ninth Revision (ICD-9) and International Classification of Diseases, Tenth Revision (ICD-10) diagnosis codes, Current Procedural Terminology (CPT) codes, and medication administration records. Patients were then screened by searching ICD-9 and ICD-10 diagnosis codes for deep venous thrombosis (DVT) or pulmonary embolism (PE) and by searching their perioperative clinical notes (including imaging records) for any mention of the words deep venous thrombosis, pulmonary embolism, DVT, or PE within the first 30 postoperative days. All patients who were screened by the aforementioned criteria then underwent additional review of their electronic medical records to verify a true VTE event. For example, a patient’s chart may have had “rule out DVT” as the indication for an ultrasound and thus screened through the algorithm as possible VTE. If the ultrasound was then negative for DVT, the patient was not counted as having a true VTE.
Data required to calculate individual Caprini risk factors were abstracted from the electronic medical records, and the Caprini score was calculated as previously described. 3 In brief, the Caprini score is a risk assessment tool for VTE in surgical patients, with points summed based on various demographic, comorbid, and perioperative risk factors. Factors are assigned a value of 1 to 5 points. Some examples include lower extremity edema, history of heart attack, congestive heart failure, or lung disease—all of which are given 1 point. Other factors include age, family history of blood clot, and prior stroke. The points are then added together to calculate the Caprini score for each patient. We also recorded whether or not patients received preoperative chemoprophylaxis. All patients had sequential compression devices (SCDs) perioperatively, as this is an institutional policy at our hospital. Data analysis was performed using Microsoft Excel (Microsoft, Redmond, Washington).
Results
A total of 1185 patients undergoing 1213 otologic surgeries met our inclusion criteria ( Table 1 ). Mean age was 51.0 ± 17.3 years (range, 18.1-93.4 years), and average length of surgery was 136.0 ± 79.0 minutes (range, 5-768 minutes). Initial screening showed DVT and PE were mentioned among perioperative notes, imaging results, or diagnosis codes in 128 and 235 surgeries, respectively. In most of these cases, “DVT” and “PE” were mentioned in clinic notes incidentally. For example, some of these cases were included initially because a clinician mentioned the risks of VTE in the preoperative notes. Other cases were screened because a clinician mentioned “PE tubes” (pressure equalizer tubes) in their notes. Those patients in whom VTE was considered based on a text search of medical records had the diagnosis excluded by lower extremity ultrasound, CT scan, or both. Upon further review of medical records of these positively screened patients, none (0/1213) were found to be true VTEs. DVT and PE were most frequently cited in the medical chart in the context of discussion of postoperative risks or ruling out DVT/PE postoperatively.
Demographics of 1213 Patients Who Underwent Otologic Surgery. a
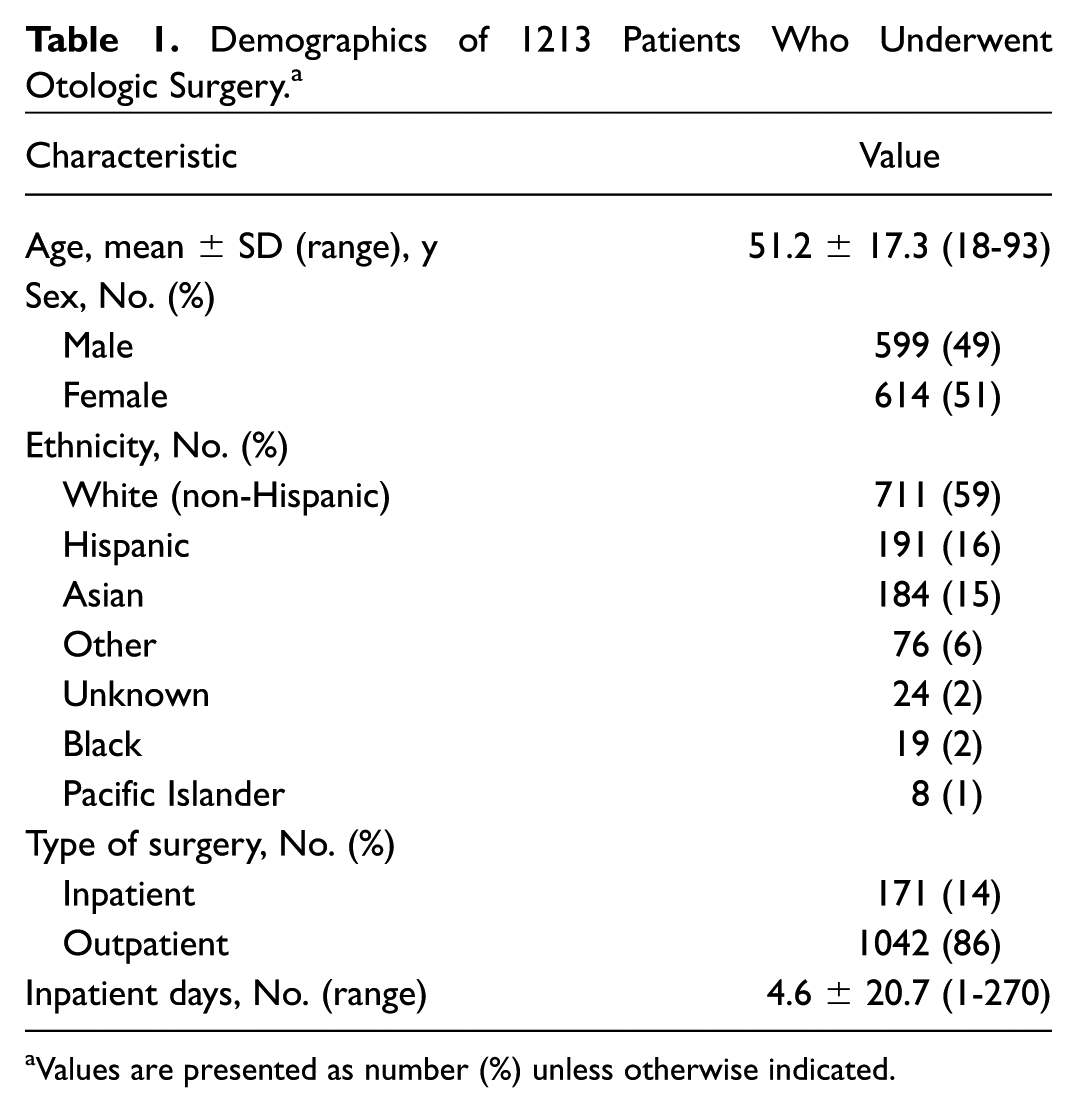
Values are presented as number (%) unless otherwise indicated.
The mean ± SD Caprini score for these cases was 4.0 ± 1.7 (range, 1-15). The distribution of patients’ Caprini risk factors is shown in Table 2 . Eighty-five percent of our cases had Caprini scores ≥3 ( Figure 1 ). Had our population been composed of general surgery patients, this would have placed them in a “moderate” risk category. 6 Similarly, 4% of our cases had Caprini scores ≥8, a score that warrants chemoprophylaxis in the plastic surgery population. 5 The absence of documented VTE in any of these patients likely illustrates a substantially reduced risk of VTE in our otologic surgical population.
Caprini Risk Factors of Patients Undergoing Otologic Surgery.
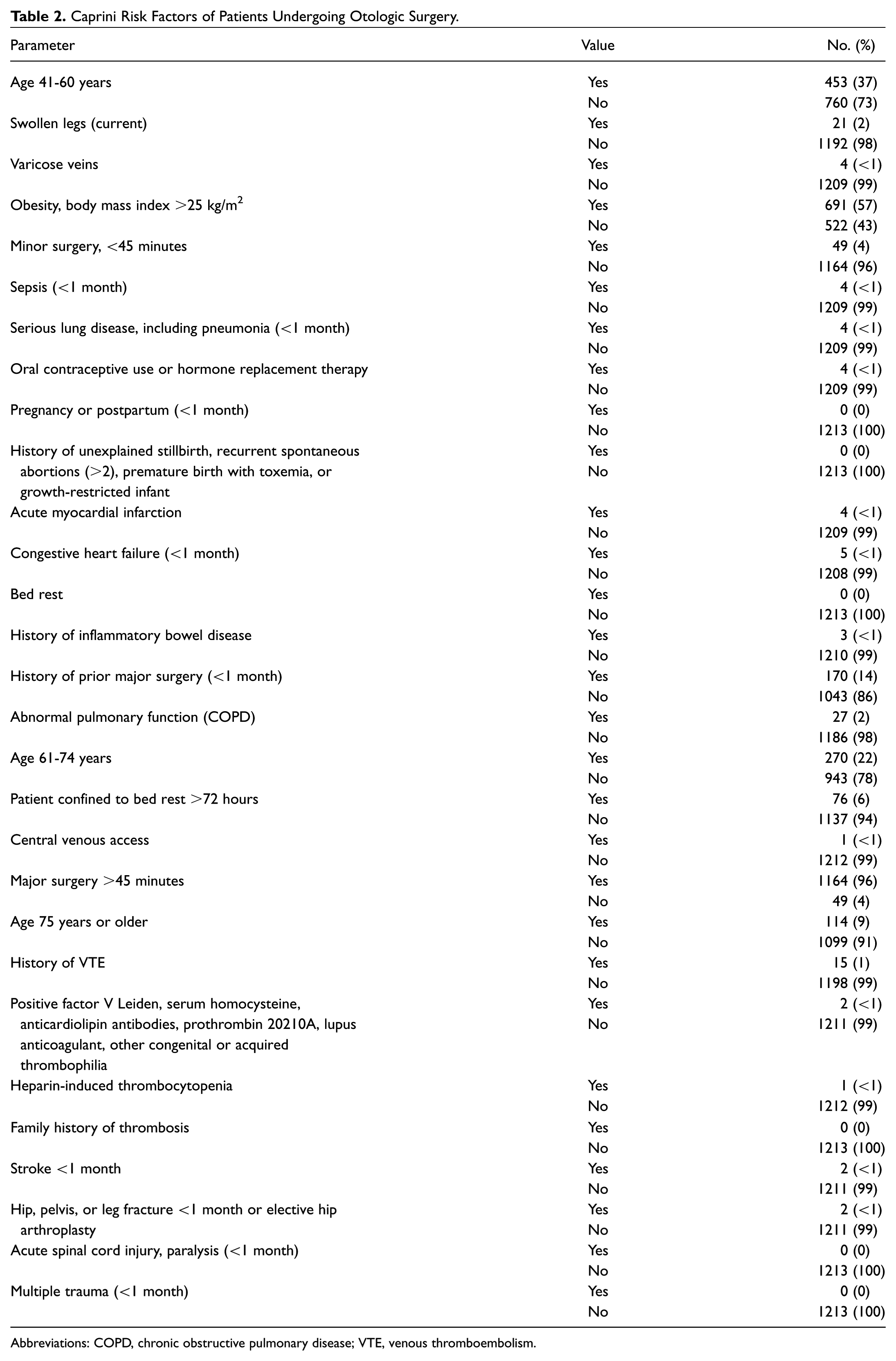
Abbreviations: COPD, chronic obstructive pulmonary disease; VTE, venous thromboembolism.
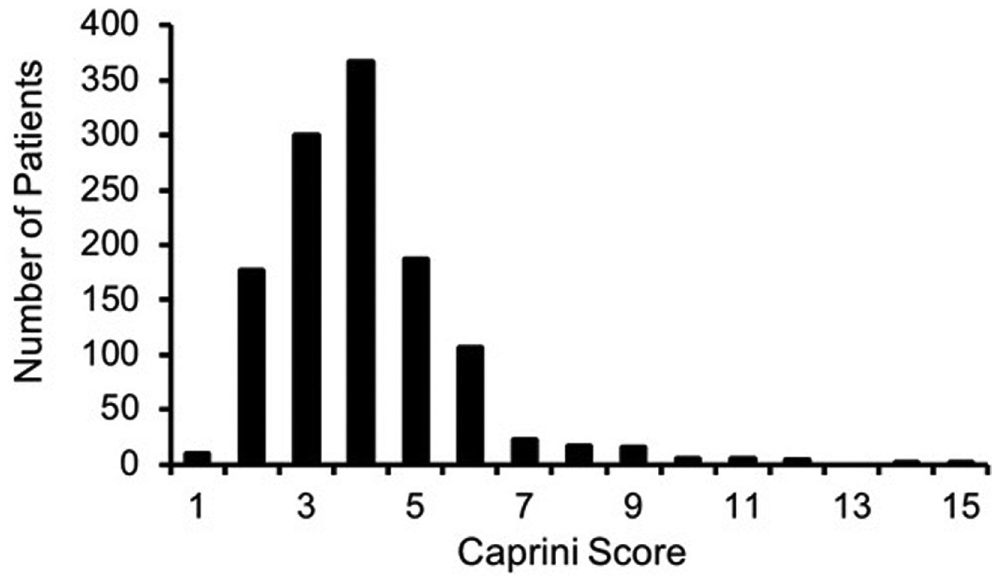
Histogram of patients as a function of Caprini score.
A review of medication administration records revealed that 6 patients received preoperative chemoprophylaxis. All of these patients had Caprini scores ≥3, averaging 4.8 ± 1.7 (range 3-8), and underwent a nononcologic combined otologic and a head and neck surgery procedure. Therefore, this subpopulation of patients who received chemoprophylaxis is unlikely to skew the results observed in patients undergoing solely extracranial otologic procedures. The Caprini scores were not significantly different between those who did and did not receive chemoprophylaxis (P = .3, t test; Figure 2 ).
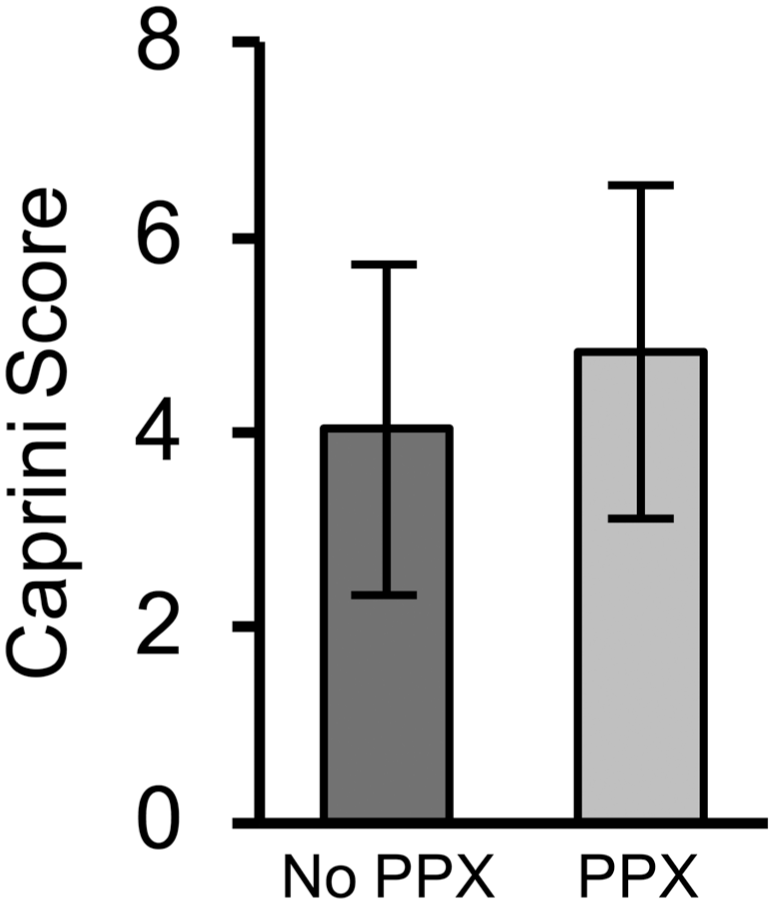
Caprini score in patients who did not receive chemoprophylaxis vs those who received chemoprophylaxis. Error bars represent standard deviation. PPX, prophylaxis.
Discussion
In this study, we found no VTE events among extracranial, nononcologic otology cases performed at a single tertiary institution during the past 8 years (1213 cases). Fewer than 0.5% of patients were given preoperative chemoprophylaxis, while all received perioperative SCDs.
Although OHNS patients as a whole have a markedly lower postoperative VTE rate (0.1%-3%)4,16-20 compared to 15% to 40% in general surgery patients without prophylaxis,1,21 certain OHNS subgroups such as patients with head and neck cancer have a disproportionately higher rate due to older age, malignancy, longer surgeries, and other comorbidities.17,20 The risk of postoperative VTE in patients with head and neck cancer is reported to be as high as 13%. 14 The differences in postoperative VTE risk among OHNS patients may reflect in part the breadth of pathology, surgeries, and types of patients treated by the specialty. Given the heterogeneity of such risk among OHNS patients, some advocate risk stratification of OHNS patients to identify those who would most benefit from appropriate chemoprophylaxis. 18
We were unable to perform risk stratification for otology patients as there were no VTE events seen in our cohort. Identifying the exact risk threshold to warrant chemoprophylaxis will require a much larger population of patients to capture a sufficient number of VTE events, which is beyond the scope of this study. We did find, however, that patients thought to be considered moderate risk for VTE as defined by the CHEST 2012 guidelines 6 did not have any recorded VTE events at our hospital postoperatively. A recent study demonstrated that current practices in VTE prophylaxis vary widely among otolaryngologists, underscoring the need for specialty-specific guidelines. 16 This study suggests that patients undergoing extracranial nononcologic otologic surgery have a low VTE risk.
Surgeries for an oncologic diagnosis, which is itself a Caprini risk factor for VTE, were excluded from this study because they often involved a second OHNS subspecialty performing additional procedures (such as neck dissection or parotidectomy) for which chemoprophylaxis is routinely administered at this institution. We sought to determine whether our institution’s practice of not routinely administering chemoprophylaxis for otologic surgery should be reevaluated to reflect conventional chemoprophylaxis guidelines, which were mostly developed with reference to general surgery procedures.
Our study had several limitations. First, our study was retrospective in nature and may be subject to various biases, including selection and information bias. Second, our study population was not powered enough to perform rigorous risk stratification analysis. Third, any VTE events treated at outside institutions that were not mentioned or recorded in our electronic medical records were not captured as a VTE event and may thus underestimate our true VTE rate. Fourth, while a robust algorithm was used to draw out Caprini risk data from the electronic medical records, it is possible that certain risk factors such as the presence of swollen legs or length of bed rest could have been inadequately captured or reported, thereby underestimating a patient’s overall Caprini score. Fifth, additional stratification of the types and lengths of otologic procedures would be quite helpful in the interpretation of these data. Although our patients all underwent extracranial otologic procedures, there is still a wide range of procedure complexity and duration. Finally, because VTE was not routinely screened for in asymptomatic patients, as per our institution’s practice, it is possible that there were patients with asymptomatic VTE who were not captured in this retrospective study.
Conclusion
The prevalence of postoperative VTE after extracranial, nononcologic, otologic surgery is rare. Chemoprophylaxis guidelines in otology patients should consider the potential risk of increased intraoperative bleeding and its associated effects on surgical visualization. Further studies elucidating the threshold at which otologic patients should receive chemoprophylaxis are warranted.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the AAO-HNSF 2018 Annual Meeting and OTO Experience; October 7-10, 2018; Atlanta, Georgia.